Embed Size (px)
Citation preview

ww
w.am
tamassage.org/m
tj1
19
COURSE DESCRIPTION: For peoplewith cancer and cancer histories, massagetherapy can be a powerful healing interven-tion. Skilled, structured touch has thepotential to reduce isolation, relieve symp-toms and help people feel cared for, whole,and empowered.
This course reviews old assumptionsabout cancer and massage therapy. It alsoincludes essential contraindications formassage for common cancer presenta-tions. It takes a detailed look at currentthought on when, where, why and how mas-sage therapy is contraindicated.
This is a two-part series of courses. Thisfirst course looks at massage contraindica-tions that arise from cancer and complica-tions as cancer develops over time. Thesecond course, which will appear in the Fall2006 mtj, looks at massage contraindica-tions that arise from cancer treatment.
by tracy walton, MS, LMTessential contraindications
CANCERMASSAGETHERAPY:
&

12
0m
tj/m
assa
ge t
hera
py jo
urna
lsu
mm
er 2
00
6
the role of massage therapyHEALING BENEFITSCancer can be an isolating experience.For people with cancer and cancer his-tories, massage therapy is often a pow-erful healing intervention. Skilled,structured touch has the potential torelieve symptoms and help people feelwhole and empowered. A well-pre-pared massage therapist offers caringtouch at an important time in some-one’s life—you can be a wonderfulcompanion on a journey that may be,by turns, deepening, strengthening,terrifying and healing. And the reas-suring company of a massage thera-pist’s touch is often welcome.
VARYING CLIENT PRESENTATIONSAs with any special population, youprovide different massage tech-niques for different clinical presenta-tions. Cancer does not define a sin-gle client presentation; instead, itencompasses a broad spectrum ofclinical possibilities:� Immediate or long-term survivor-
ship, which requires very differentmassage therapy from that given tosomeone at end of life;
� Issues facing someone duringdiagnosis are different than thosefaced later in treatment, and thesescenarios involve different massagecontraindications;
� Different types and stages of cancer
bring different signs, symptoms andcomplications, requiring individual-ized massage therapy approaches.
Because of this variability, the mas-sage therapy modifications requiredfor cancer are rarely found in a sim-ple rule or list of rules. Instead, theyflow from good clinical judgment,some basic principles in massage, andknowledge of how cancer and cancertreatment affect the body.
This first course of the two-partseries addresses essential contraindica-tions for the most common cancer pre-sentations, both early in the diseaseand as it develops over time. The sec-ond course in this series addressesessential contraindications that arisefrom the treatment of cancer, often pre-senting a separate set of issues from thecancer itself. (The second course willappear in the Fall 2006 issue of mtj.)
MASSAGE THERAPY & SYMPTOM RELIEFMassage is being recognized as asource of significant benefit for peo-ple with cancer histories and activecancer. Clients often report relieffrom the five common symptomsassociated with cancer and its treat-ment: pain, anxiety, nausea, fatigueand depression. These anecdotalreports of relief are becoming a focalpoint for massage researchers.
COURSE OBJECTIVES: A well-prepared massage therapist offers caring touch to clients with cancer at important times intheir lives. However, there are contraindications, considerations regarding site, pressure and joint movement, as well asother details you should explore before beginning massage therapy for clients with cancer.
When you have completed Part 1 of this two-part series, you will be able to:� List three problems with the traditional, absolute contraindication to massage therapy; � Describe three counterarguments to the notion that increased circulation from massage therapy promotes cancer spread;� Describe five common massage therapy contraindications for cancer and its complications;� Define deep vein thrombosis (DVT) and the concern it presents to massage therapists working with oncology clients;� List the signs and symptoms of DVT, the risk factors and the actions to take when these are present.
CONTACT HOURS: 2.5
To take the exam for this course,go to AMTA’s Online Learning site atwww.amtaonlinetraining.org.>>

Of these five symptoms, the mostsolid research support is for the reduc-tion of anxiety. But because research onmassage therapy is still in its earlystages with small numbers of patientsstudied, effects on symptom relief arenot yet definitive. Investigators contin-ue to research massage therapy ques-tions, and massage therapy for peoplewith cancer is gaining interest amongresearchers. Massage effects on thecommon symptoms and physiologicalparameters are suggested in recentsmall studies. Of particular interest inthese studies are the suggested effectsof massage on anxiety, pain and nausea.For a list of these studies, go to page 134.
the myth of the absolute contraindicationTHE CONVENTIONAL BELIEFOver the years, a myth in massagetherapy existed that all massage wascontraindicated for people with cancer.This belief was passed from therapist totherapist, taught in massage schoolsand recorded in massage literature.Unfortunately, this directive was usu-ally not specific in its guidelines andmay have drifted from its original mes-sage as it was passed through the pri-marily oral tradition of massage thera-py. In response to this severe con-traindication, therapists and studentshave asked for more specifics:� What kinds of massage are con-
traindicated? � Where shouldn’t massage be
applied? � For which kinds of cancer, and in
which stages is massage therapycontraindicated?
� Is massage therapy contraindicatedfor cancer survivors whose cancerhas resolved?
� After how many years of survivorshipis massage considered “forever safe?”
� Is massage therapy contraindicatedat the end of life or during treatment?
� Is massage therapy contraindicatedfor cancer that was removed suc-
cessfully, but the client is still inactive treatment?
Unfortunately, none of these questionswere answered, nor the nuances cap-tured, in the broad instruction, “mas-sage is contraindicated for people withcancer.” The instruction seemed basedon an underlying fear: that by increas-ing circulation, massage could pro-mote the process of cancer metastasis,the spread of cancer from its primarysite to distant tissues and organs.
Because cancer metastasis does somuch damage, and is a factor in mostcancer deaths, the massage therapyprofession was understandably cau-tious, but ill-informed. In this uncer-tain climate, countless clients wereturned away by concerned therapists.Unfortunately, because this fear wentunexamined for so long, both thera-pists and clients missed rich opportu-nities for working together to pro-mote healing.
challenges to the myth Thanks to recent thought and educa-tion, the absolute contraindication ofmassage therapy for cancer patients hasbeen examined closely and overturned.There are several major challenges to it.
TOO GENERALFirst, the contraindication was too gen-eral—a universal prohibition that didn’tnecessarily apply to individual clients,massage modalities or techniques. Withmany kinds of massage and varyingclinical pictures of cancer, it ignored allthe individual massage approaches thatmight be safe and appropriate for indi-viduals. Recognizing this, many thera-pists disregarded the contraindicationand provided modified techniques fortheir oncology clients throughout treat-ment and into recovery or end of life.
NOT SPECIFIC AS TO SITE, PRESSURE OR JOINT MOVEMENTThe contraindication as stated abovewas not specific about the site or pres-
CHALLENGES TO THEABSOLUTE MASSAGECONTRAINDICATION � It is too general as to client, massage modality or
massage technique;� It is not specific as to site, pressure or joint
movement;� It is based on a flawed assumption, that massage
increases circulation, and that increased circula-
tion promotes metastasis.
10PEOPLE LIVE WITH CANCERIN THE UNITED STATES. THIS INCLUDES ANYONEDIAGNOSED WITH CANCEROR A CANCER HISTORY. Source: American Cancer Society and theNational Cancer Institute
million

sure of the massage. It may have orig-inated as a concern about merely dis-turbing the tumor site itself, but it wasinterpreted as a rule against all mas-sage, all the time, in all places. Thiscontraindication was amplified, prop-agated and developed a life of its own.It is true that any technique is con-traindicated if it directly disturbs anactive tumor site. But for massage todo this, the tumor site would have tobe superficial enough to be in reach ofthe therapist’s hands, movements orhydrotherapy techniques.1 And oftena tumor is easy to avoid pressingupon, as it is usually limited to one orseveral readily defined areas. As sur-geon Bernie Siegel pointed out,“Massage therapy is not contraindicat-ed in cancer patients; massaging atumor is, but there is a great dealmore to a person than their tumor.”2
MASSAGE ≠ INCREASED CIRCULATION≠ INCREASED METASTASISThird, the absolute contraindication
rests on the faulty assumption thatmassage, by increasing circulation ofblood and lymph, could promote can-cer metastasis. Both parts of thisassumption are flawed. The first is theassumption that massage significantlyincreases general circulation of bloodor lymph. While this is widely believedand taught in the profession, I know ofno rigorous research, using Swedish-type massage therapy, with adequatenumbers that supports the claim of anoverall boost in systemic circulation, aswould be brought on by cardiovascularexercise. Only smatterings of smallerstudies, themselves offering conflictingresults, test effects on blood and lymphcirculation, and these are about localor regional circulation—limited to thearea of tissue worked directly by thetherapist’s hands. (For a list of somestudies on this, see page 134.)
So far, the evidence is inconclusiveabout this readily accepted assumption.
There is a second flaw in theassumption. Even if massage did signif-
icantly increase the overall flow rate ofblood or lymph, it is doubtful that thiswould result in a faster metastaticprocess. Why is this? Think about howfast circulation flows under normalconditions in the body, without mas-sage in the picture. Although figuresdiffer on the normal rate of lymph flow,it seems to take about an hour for thelymphatic system to move materialfrom out in a limb, through vessels andnodes to the subclavian veins, wherethe material joins the blood circula-tion.3 The transit time for material inthe deeper tissues in the trunk wouldseem to be, if not comparable, at leastin the same order of magnitude.
Now think about blood flow. Thetime it normally takes a cell floatingin the bloodstream to complete a cir-cuit through the entire systemic andpulmonary circuits, returning to itsstarting point), which is only a matterof a minute or a few. Under high arte-rial pressure, this cell moves quicklythrough much of the circuit. It seems
Controlled trials on massage therapy in people with cancer are still
small but are growing in size. Of particular interest is a study of
230 people in chemotherapy done at the University of Minnesota.
Researchers compared massage therapy, Healing Touch, caring
presence without touch, and usual care control (no intervention) in
outpatients. Patients were each measured during a four-week con-
trol period and were randomized to four 45-minute sessions of one
of the three interventions.
Results suggested that both massage and Healing Touch low-
ered total mood disturbance. Massage therapy lowered anxiety.
Healing Touch reduced fatigue. And massage therapy reduced the
use of analgesics over the four-week period. These are promising
findings, and if they are replicated in larger studies, present a com-
pelling case for the role of massage in helping people cope during
cancer treatment.*
More recently, investigators have undertaken studies with larger
sample sizes. Moreover, higher-level analysis of existing studies
will help determine how massage helps, when it doesn’t appear to
help and what kind of future research is needed to better answer
clinical questions.
A gold standard of higher-level analysis is a systematic, quanti-
tative review of existing studies, called a meta-analysis. So far, one
such rigorous review has not shown strong evidence for massage
therapy relieving common symptoms of cancer.** This doesn’t
mean there’s no help from massage; it just means the evidence is
not yet there to draw conclusions in either direction. It may be that
as smaller studies are added to the pool of available information,
the evidence will mount in favor of the relief massage therapy can
provide. There is even investigation into the effect of massage on
caregivers and spouses of people with cancer, a population also in
need of care.
Therapists interested in following research on massage therapy have
several resources to turn to. For example, there are online databases
of general information such as Medline (www.nlm.nih.gov), where a
search of “massage therapy” can yield good results. A list of massage
specific databases is available at www.amtaonlinelearning.org.
STUDIES GROWING IN SIZE
* Post-White J, et al. “Therapeutic massage and healing touch improve symptoms in cancer.” Integrative Cancer Therapies. 2003;2(4):332-44.
** Fellowes D, Barnes K, Wilkinson S. “Aromatherapy and massage for symptom relief in patients with cancer.” Cochrane DatabaseSystem Review. 2004;(2):CD002287.

ww
w.am
tamassage.org/m
tj1
23
unlikely that massage therapy couldsignificantly increase the rate of acancer cell’s movement through thesechannels. If it did, would massagehurry the process by 15 seconds? Anhour? Would this make a differenceto the disease process of metastasis?
METASTATIC FACTORSDespite how fast a cancer cell in thelymphatic vessels or in the blood-stream can travel to other parts of thebody, the actual process of metastasiscan, in fact, take months or years.This is in part because not all cancercells, free in circulation after shed-ding from the primary tumor, go on toform metastatic tumors.
As described in Gayle MacDonald’sbook, Medicine Hands: MassageTherapy for People with Cancer,metastasis is a complex process,involving interactions of cancer cellswith the immune system, other fac-tors in the blood and the “target” tis-sues, as well as the genetic makeup ofthe cancer cell itself.4 So even thoughlymph and blood flow swiftly to carrythe cell along its course, its ability tosurvive the flow, establish a site in adistant tissue, build its own bloodsupply, and thrive as a secondarytumor site is limited by other factors.Clearly, metastasis is more than asimple mechanical movement frompoint A to point B. In fact, cancermetastasis seems to have a life of itsown, a life that is well beyond thereach of a simple, skilled 50-minutegeneral massage.
THE EXERCISE ARGUMENTGoing even further, one of the mostpowerful arguments against a generalmassage contraindication is “the exer-cise argument.” So far we’ve ques-tioned whether typical circulatorymassage—characterized by mediumand deep kneading and stroking ofthe Swedish variety or lighter, chore-ographed strokes of the lymph
drainage variety—has been thoughtto promote metastasis. But if, indeed,this were true, wouldn’t exercise orother normal activities be more dan-gerous than massage therapy? DebraCurties points out this compellingargument in an article in mtj.5
If we were truly concerned aboutthe blood and lymph flow rate andmetastasis, patients would be warnedagainst exercise and movement. Butphysicians don’t tell cancer patientsto lie still in order to keep cancer fromspreading. In fact, where possible,exercise is strongly encouraged forpeople with cancer.6 Restrictions onactivity are usually based on healingincisions, unstable bones or otherrisks, not on fear of cancer spread.Even breathing increases circulation,by encouraging venous return, asmassage is thought to do. And ofcourse, physicians don’t advise theircancer patients to breathe shallowlyto reduce the chance of metastasis.Movement, breathing and circulationare normal functions—factors inhealth and healing, not isolated fac-tors in cancer spread.
Against these physician-approvedactivities, the fear that massageincreases circulation and increasesmetastasis fades to insignificance. Ifyou place massage therapy, even the“general circulatory massage therapy”that many of us were taught, next toexercise and other equivalent activi-ties, the reasoning provides a simple,effective argument against the old
absolute massage contraindication.While there are massage contraindica-tions for patients with cancer, they arenot based on the fear of increasingblood or lymph flow. Instead, they arespecific contraindications based onspecific cancer presentations.
The reasoning about massage, cir-culation, and metastasis—along withthe exercise argument—is useful topass along to patients and health careproviders who are still affected by theconventional contraindication tomassage. This is an important educa-tional contribution massage thera-pists can make.
cancer, complications andcontraindications CATEGORIES OF CONTRAINDICATIONSTo move further away from a flat,absolute statement like “massage iscontraindicated for cancer,” it’s usefulto be more precise. What is it aboutcancer that contraindicates massagetherapy? And what is it about massagetherapy that is contraindicated ormust be modified? To manage med-ically complex information, it is usefulto group these concerns, and massagecontraindications are organized intothe following three groups:
First, contraindications for canceritself stem from how the tumor initial-ly manifests itself. Second, as cancerdevelops over time, complications canarise—cancer amplifies its effect on tis-sue and organ function, and increasesits reach to distant areas of the body.
3 TYPES OF MASSAGECONTRAINDICATIONS FOR CANCER PATIENTS� Contraindications due to the primary tumor site;� Contraindications due to the progression of the cancer;� Contraindications that arise from cancer treatment.

12
4m
tj/m
assa
ge t
hera
py jo
urna
lsu
mm
er 2
00
6
Finally, contraindications arise fromthe effects of cancer treatments, sideeffects, adverse reactions, and so on.
In general, therapists consider anyactive tumor sites—primary and sec-ondary metastatic sites—in their plan-ning. They look at whether cancerexerts stress on tissues or organs. Withchanges in the body’s internal environ-ment, you need to gauge a sensible mas-sage response. If the body is weakenedfatigued or an organ function is compro-mised, you need to provide massagetherapy techniques that are supportiverather than challenging. You shouldwork conservatively, often using gentlerpressures, less demanding protocols andsofter joint movements. You also mightwork for less time, avoid certain areas ofthe body, or schedule around good andbad times for the client.
PHYSICAL AREAS OF CONCERNSources of massage contraindicationsfor the cancer itself and the complica-tions that develop over time includetumor site or sites, bone involvement,cancer pain, vital organ involvementand deep vein thrombosis (DVT).
Of these five factors, the first fourare fairly straightforward. In contrast,a lengthy discussion is required forDVT and the need to assess whatactions are appropriate for DVT.
How cancer manifests in the body—with a tumor in a certain area, a symp-tom caused by the condition—and itscomplications or effects on organ ortissue function over time, may warrantmassage adjustments. To determinethe extent of these adjustments, youshould ask specific questions. Samplequestions are included throughout thisarticle. A complete list is also availableat www.amtaonlinelearning.org.
psychosocial challengesPeople with cancer, at the end of lifewith cancer and in survivorship facemany psychosocial challenges andoften a range of emotions and moods—
terror, sadness, anger, depression andanxiety, to name just a few. As withmany illnesses, people face isolation,stigmatization and sensation. With can-cer, the diagnosis alone can affect one’sbody image. Add that to other outwardsides of illness, surgical removal of tis-sue or loss of hair, and the relationshipwith one’s body can become fraught.
But as massage therapists, you are ina unique position to accompany peopleon the path they travel with their bodythrough diagnosis and treatment. Learnas much as you can about experiencesof cancer so that you can interview, lis-ten carefully and provide healing touchin healing ways. The connectionsbetween massage therapists and seri-ously ill clients are powerful and heal-ing. This is intuitive, but it also shows upin some concrete ways. For example,people in cancer treatment often dealwith painful touch from procedures,examinations and treatment. Massagetherapy restores pleasurable and correc-tive touch to a client’s experience, andcan help a client feel whole again.
A targeted interview question aboutmood or the emotional landscape of aclient’s experience may be too intrusivefor some clients. But open-ended ques-tions such as, “How have you been doingsince the diagnosis?” make space forthis aspect of a client’s experiences,along with the medical information youneed. Listening carefully in conversationwill help you understand clients’ experi-ences, possibly meet their concerns withmassage therapy, and certainly make ajudicious referral, which can be vital.Nearly everyone can provide solid listen-ing and empathy, but counseling is out-side the massage therapy scope. Avoidgiving advice, and refer clients to theirphysicians and nurses or to professionalcounseling for additional support.
tumor sitesOne of the most obvious issues pre-sented by a client with cancer is atumor site. Whether this is a known
for more training in cancer & massage:Tracy Walton offers an intensive training,“Caring for Clients with Cancer” with asupervised clinic, and advanced coursesaround the country. She also teaches aone-day course customized to spa andresort facilities, hospital massage pro-grams and conferences. Her coursedescriptions and teaching schedule are atwww.tracywalton.com.
Gayle MacDonald teaches “MassageTherapy for People with Cancer,” which isoffered nationally. Gayle also offers anintensive, hospital-based massage trainingand teaches for the program at theScherer Institute in Santa Fe, New Mexico.More information available at www.medi-cinehands.com.
Cheryl Chapman, an oncology nurse, certi-fied holistic nurse and massage therapist,teaches two courses: “MastectomyMassage,” and “Cancer Massage,” bothoffered nationally. More information is atwww.cherylchapman.com.
The Integrative Medicine Service atMemorial Sloan-Kettering Cancer Center,led by Wendy Miner, offers two levels of“Medical Massage for the Cancer Patient”in New York City. Visit them atwww.mskcc.org/mskcc/html/11802.cfm.
Debra Curties, the author of MassageTherapy and Cancer and Breast Massage,teaches workshops on breast massageand on massage and cancer in Canadaand the United States. More informationis available at www.curties-overzet.com/works.htm.
The Scherer Institute of Natural Healing inSanta Fe, New Mexico offers a program inOncology Massage, featuring SandyCanzone, Gayle MacDonald and otherinstructors. More information is availableat www.schererinstitute.org/ oncolcertinfo.htm.
The Colorado School of Healing Arts offersan oncology massage program, includingseveral courses at their facility inLakewood, Colorado. More information isavailable at www.csha.net/advanced/oncology.html.
The MD Anderson Cancer Center inHouston, Texas, offers “Massage for theCancer Patient: An Integrative Approach.”Reach the Complementary and IntegrativeMedicine Education and Resources(CIMER) site at www.mdanderson.org/departments/CIMER.

ww
w.am
tamassage.org/m
tj1
25
or suspected tumor site, or even atumor site of the past where only ascar, left by surgery, remains, mas-sage may be adapted to the site of thetumor in some way.
DIRECT PRESSURE PROHIBITIONDon’t directly massage a tumor site withpressure or move tissues in the vicinityof the tumor that may then disturb it.Most of the time this is a straightforwardcontraindication. In your initial inter-view question, you should ask some-thing like, “Where is (or was) the tumorsite,” or, more simply, “Where is (orwas) it in your body?”
There are more details about thisbasic contraindication. First of all,you need to avoid pressure or jointmovement only at the site of tumorsin reach of or mechanically affectedby hand pressure or joint movement.Using this guideline, a simple lung,liver or pancreatic tumor would pre-sumably be out of reach. If there areno other contraindications, somepressure on the back and ribs wouldlikely be fine for these cases.
On the other hand, complications ofthese conditions may lead to pressurecontraindications in those areas. Athorough interview and consultationwith a client’s physician may be neces-sary to determine whether it is a sim-ple or more complicated matter.Abdominal cancer, including coloncancer, would contraindicate abdomi-nal therapies with pressure. And can-cer in the bone contraindicates pres-sure and joint movement in the region.In fact, because massage therapists
press on the bone, bone involvement isone of the most relevant issues fortherapists and will be addressed indetail in subsequent paragraphs.
Having described the massageissues—pressure and movement—it’simportant to describe the tumorissues. First, a site where a tumor hasbeen successfully surgically removedwould not come with these con-traindications. However, if it is a heal-ing incision, massage pressure, move-ment and perhaps contact will need tobe modified depending on how newthe incision is.
Second, a suspected tumor site, notyet established by a physician usingdiagnostic tests, nevertheless getstreated like a known site, with all ofthe pressure and movement con-traindications for known sites.
Third, no matter how delicate atumor site is, neither caring contact,nor holding is necessarily contraindi-cated. If the client tolerates and wel-comes it, and there are no other con-traindications, gentle holding withsoft hands may be welcome and heal-ing. Moving the hands across the skinwith the gentlest pressure—the kindused to apply lotion, but not to rub itin—would likely be appropriatewherever the skin is intact and notirritated.
LIQUID TUMORSSome kinds of cancer are not solid.Instead, they circulate throughoutthe bloodstream. These are known asliquid tumors; a blood cancer such asleukemia is a prime example.
Sometimes DVT is clinically silent, with no signs and no symptoms or
discomfort. I know a massage therapist who worked with an individ-
ual with no symptoms or complaints, but one day the therapist felt a
strange, cord-like hardness while she used strokes with pressure on
the adductors of the client’s right thigh. Feeling that “something was
not right,” the therapist left it alone and brought it to the attention of
her client, urging him to see his physician as soon as possible.
Later the client called the therapist to say that acting on her
advice, his doctor had diagnosed a blood clot, and he was now on
medication to prevent future clot formation. His physician assured
him he was lucky the massage therapist had noticed the difference
in the tissues.
A FORTUNATE INTERVENTION
important books on cancer & massageCurties, Debra. Massage Therapy andCancer. Toronto: Curties-OverzetPublications, Inc., 1999.
MacDonald, Gayle. Medicine Hands:Massage Therapy for People with Cancer.Forres, Scotland: Findhorn Press, 1999.(2nd edition expected Fall 2006.)
MacDonald, Gayle. Massage for theHospital Patient and Medical Frail Client.Philadelphia: Lippincott Williams &Wilkins, 2004.

12
6m
tj/m
assa
ge t
hera
py jo
urna
lsu
mm
er 2
00
6
Because these are distributedthroughout the body, there is no sin-gle site-specific massage contraindi-cation to pressure or movement.There might be other more generalcontraindications to pressure orother elements of massage, but thesecan be determined after you evaluatethe client’s case for complications ofleukemia, effects on other tissues andthe effects of treatment.
bone involvement & its complications Among the most relevant issues facingyou in work with cancer patients is can-cer involving the bone, whether it is aprimary or metastatic site. Cancer canstart in the bone or it can end up there,metastasized from several other prima-ry sites such as breast, pancreas orovary. Most cancer in the bone eatsaway at the structure, making it lessstable and vulnerable to pathologic frac-ture. Pathologic fracture occurs when-ever bone is weakened by such a dis-ease process or by other diseases suchas osteoporosis. Fracture can occurwith unusually low force. Every clientwith cancer or a cancer history shouldbe asked if there is/was bone involve-ment. With bone involvement, youmust consider how stable the bones arebefore using pressure on or near themor moving involved joints. Mechanicaldisturbance in areas of bone involve-ment can damage the bone itself.
QUESTIONS TO ASKAs a massage therapist, it is not yourplace to diagnose bone involvement,but there are several questions toask clients and their physicians.Likewise, you have questions for aclient when they present with pain(see sidebar, opposite). Importantquestions include the following:� Where is the bone involvement?
(Have them describe and point tothe area(s).)
� Have you received diagnostic tests
for bone involvement? Recently?What have your doctors concludedfrom those tests?
� Have any of your physicians ornurses told you to be concernedabout the stability of your bones? Ifso, please describe their concern.
� Have any of your physicians ornurses restricted your activitiesbecause of concern about bone sta-bility? Describe.
� In general, what is your activitylevel? What kinds of activities doyou engage in daily or weekly?
These questions and physician inputabout massage will help you to deter-mine the best levels of massage pres-sure and movement to use. Examplesof how one therapist accommodatedbone involvement in practice areshown on page 128-129.
cancer painMASSAGE THERAPY TREATMENTPRIORITIES FOR CANCER PAINPain is one of the most feared cancerexperiences. Whether it’s caused by thecancer itself or by the cancer treatment,pain places emotional strains on indi-viduals and families. Pain from canceritself can be caused by the tumorthrough a variety of mechanisms, suchas pressing on organs, tissues or nerves,or by obstructing blood vessels. You canprovide therapy for pain related to mus-cle tension and various other comfort-oriented techniques. Often people findpain relief from massage. But it’s alsoimportant to ask clients about their painlevel in order to: � Find out the cause of pain;� Provide relief, where possible; � Be sure they are being treated for
their pain, and, if not, refer them totheir health care team for care.
Careful questioning about pain is impor-tant, as is proper follow-up.
If a client with cancer or a cancerhistory complains of new pain, you
PAIN CAN SIGNALBONE INVOLVEMENT When a client with cancer comes in with
pain, instead of going after the pain as
though it were muscular, wait for a physi-
cian to verify that the pain is not due to
bone metastasis. Ask the client where he
or she experiences the pain and whether
he or she has talked with a physician
about it. Have the client point to it.
Bone pain can be a symptom of bone
metastasis. Since bone metastasis usual-
ly weakens bones, an affected area could
be at risk for fracture from too much
movement or pressure. A massage thera-
pist working with a client at the site of
pain should use extremely gentle pres-
sure, with no joint movement. Positioning
should be done cautiously to avoid dis-
turbing the area.

ww
w.am
tamassage.org/m
tj1
27
should ensure that:� The client sees his or her treating
physician for evaluation and appro-priate treatment.
� Massage pressure or joint move-ment is not used at any site wherethe pain in the tissue could be dueto tumor presence.
� Massage pressure or joint movementis not used at any site where boneinvolvement could be causing thepain, bone integrity is compromisedor both. Problems with bone integri-ty make it vulnerable to fracture.
� The client’s physician providesguidelines for massage pressureand joint movement.
You are in a good position to make animportant referral and support clientsin getting their pain assessed, treatedor at least managed. Some pain goesunderreported and some people arereluctant to seek help for their pain.
vital organ involvementCENTRAL QUESTION FOR VITALORGAN INVOLVEMENTCancer that is large or advancedenough, or located in key areas, mayaffect the function of vital organs. Askeach client the following question: “Hasthe cancer affected the function of your
lungs, liver, kidney, brain or heart?”Even if a tumor is located in a tissue ororgan, it might not be large oradvanced enough to affect its function.Therefore, distinguishing between atumor’s location and its impact isimportant.
If the answer to this question is yes,follow a general guideline called “thevital organ principle.” It states: “If thefunction of a vital organ is compro-mised, provide massage with gentleelements. Adjust the massage ele-ments to pose minimal challenge tothe client’s body.”7 Think of all the ele-ments of massage—pressure, jointmovement, positioning, speed of mas-sage strokes, rhythms, length of thesession—that can be made gentler onthe body. Provide a massage at thegentle end of the continuum—one thatis supportive of healing. Don’t ask thebody to handle strong stimuli.
This principle is based on commonsense more than exact, known mecha-nisms of the effects of massage therapyon vital organs. A body working with acompromised vital organ is alreadyworking hard to maintain balance. Ashealing as a vigorous massage can be, itstill asks the body to adapt to a varietyof input with countless reflex respons-es. Someone with a vital organ com-
promise may be severely ill. His or herbody is already working hard to com-pensate for the diminished function.
ORGAN FUNCTION AND MASSAGEThe question about vital organ functionis important and the impact of it canvary from client to client. For example,a client with a slow-growing brain tumoris scheduled for surgery in a few weeks.The client may be using the time to pre-pare his or her body mentally and phys-ically by walking a couple miles eachday, doing yoga several times a weekand meditating. The client is takingminimal medications for the condition.
Another client, also with a braintumor, suffers frequent seizures, bal-ance and mobility difficulties, and evenmental status changes. It is likely thisclient is taking several strong medica-tions. This client has a very differentbody from the client mentioned in theabove example; this one requires muchmore caution. Massage will need to beshorter, gentler and scheduled aroundgood and bad times of day, and you needto be careful with positioning. Speedsare slow, rhythms are even. Joint move-ment is gentle, posing minimal chal-lenge to the client. Depending upon hisor her mental status, communicationmay need to be simplified and direct.
The following guidelines are strongly recommended for working
with cancer patients in treatment or those who have recently
received treatment for it. They help you respond appropriately
when clients report pain.
1. If clients mention pain that is new, unfamiliar, recently
increased or has not been mentioned to their physician—even if
it’s a dull pain—avoid massage pressure or joint movement in the
general area. Refer these clients to their physicians for diagnosis
and treatment. You must have assurance that there is no bone
involvement in the area compromising the bone structure in order
to use pressure or movement at that site.
2. If clients report any weakness, numbness or tingling, refer
them immediately to their physician—with or without pain.
Nervous system symptoms signal the possibility of bone pressing
on peripheral nerves, spinal cord, etc. This possible bone instabil-
ity makes this a medical emergency requiring strict immobiliza-
tion. Have the client call his or her doctor immediately to ask how
to proceed.
When to Refer to a Physician:� If clients are experiencing new, unfamiliar or recently increased
pain and have not mentioned it to their physicians;� Immediately, if the clients report nervous system symptoms
(i.e., sharp pain, numbness, tingling, weakness, etc.).
GUIDELINES FOR MASSAGE THERAPISTS: FOLLOWING UP ON CANCER PAIN
CONTINUED ON PAGE 130

12
8m
tj/m
assa
ge t
hera
py jo
urna
lsu
mm
er 2
00
6
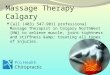
EXAMPLES OF BONE INVOLVEMENT. Bone involve-ment can be severe or mild, as shown in the followinggraphic. Bone stability can be affected to varying levels,as well, and more or less vulnerable to pathologic frac-ture. In response, the massage therapist may need toadjust the massage a little or a lot.
This graphic also shows appropriate levels of pressure
used by a therapist with six different clients, and the rea-soning used. The client descriptions demonstrate varyinglevels of risk of pathologic fracture or instability. Thesecases demonstrate the importance of receiving guidancefrom clients’ physician, getting the physician’s permissionfor massage and asking the client careful questions aboutbone involvement. >BONE METASTASIS &
These client stories illustrate the range of bone stabilities
least severe metastasis(most stable)
medium pressure
MULTIPLE BONE METASTASES,STABILIZED BY MEDICATION;VERY ACTIVE; NO ACTIVITYRESTRICTIONS.A client told me she had several sites ofbone metastasis from her primary breast can-cer. There were a couple of spots on ribs, acouple of vertebrae involved and a lesion onher hip. Medication was stabilizing her bonespretty well, and her physician encouraged herhigh level of activity. In the week before shecame in for her first session, she bicycled 40miles, cut down and hauled away small treesfrom her land, and carried wet cement to pourthe foundation for a deck. She spent hourspounding nails, building the deck.THERAPY DECISION: It seemed that this clientcould tolerate moderate pressures every-where except near the lesions; the same isapplied to joint movement. Pathologic fracturewas unlikely in this client with massageadjusted accordingly. She reported benefitfrom massage of tense muscles. The physi-cian approved the massage pressures used.
1DIFFUSE BONE METASTASES,NONE SEVERE OR UNSTABLE;VERY ACTIVE; NO ACTIVITYRESTRICTIONS.A client stated, “the cancer has spreadfrom my pancreas to everywhere in mybones,” but further communication withher and her physician revealed no concernabout bone stability. The lesions werenumerous but tiny. The doctor encouragedthe client to be quite active, so she contin-ued to workout on stairs, on a treadmill,and with weights, and did yoga severaltimes a week. She also walked brisklyeach day for 75 minutes.THERAPY DECISION: It seemed that mas-sage for this client would be safe at mod-erate pressures throughout her body, andmoderate joint movement would be fine.Pathologic fracture was unlikely in thisclient with massage adjusted accordingly.She reported that massage helped hermaintain her activity level. The physicianapproved the pressures used.
BONE METASTASES STABILIZED BY SURGERY, MODERATELY ACTIVE; NO ACTIVITY RESTRICTIONS.A client had bone metastasis in two verte-brae—C8 and T1—but had surgery to sta-bilize the area with metal hardware. Duringher course of massage therapy she wasmoderately active, walking each day. Thearea of bone involvement was somewhatstiff, but mobile.THERAPY DECISION: It seemed that I coulduse gentle to moderate pressure and jointmovement generally, but none in the areaof the affected vertebrae. In that area, Iused only gentle contact and skin stroking;I tried gentle, quiet, still holding around herneck, and the client reported relief fromstiffness and pain in the area. The physi-cian approved the pressures used.
2 3
MASSAGE PRESSURE
� This graphic is meant to provide clinical examples, not to serve as a universal practice guideline. Always include thephysician’s input on bone involvement, massage pressure, and joint movement.

ww
w.am
tamassage.org/m
tj1
29
> MASSAGE THERAPY and the therapist’s massage adjustments.
most severe metastasis(least stable)
gentle pressure
SEVERE HIP BONE METASTASIS;LOW ACTIVITY LEVEL; CAUTIOUSACTIVITY RESTRICTIONS.A long-time client came in. She hadrecently been told by her physician to moveslowly and carefully, walk with a cane andnot to step too hard off of a curb onto thestreet. The metastasis in her hip jointmade her hip unstable—a hard jolt mightfracture it. She had one other mildermetastasis site in a rib. The client receivedregular scans for bone involvement.THERAPY DECISION: This client neededcareful positioning to accommodate hervulnerable hip with absolutely no pressurein the two areas of metastasis or jointmovement at those sites. Once I deter-mined that her scans for bone involvementwere recent, it made sense to do gentlemassage and joint movement in other,unaffected areas of her body. Her hip painseemed to respond to full, gentle handcontact with no pressure, and the rest ofher body seemed to relax in response togentle muscular massage. The physicianapproved the pressures used.
MANY BONE METASTASES, EASILY FRACTURED, LIMITEDACTIVITY LEVEL; STRONG ACTIVITY RESTRICTIONS.A week prior to his massage session, aclient fractured a rib when he clipped asnug-fitting lumbar pack belt around hiswaist. Scans showed significant boneinvolvement at many sites in his body.THERAPY DECISION: This client had anextremely fragile skeleton and no pressureor joint movement was used anywhere.Instead, the gentlest holding was indicat-ed, with possible stroking of the skin only.No displacement of muscles.Repositioning this client was ill-advised;instead, I decided to work with him in theposition in which I found him. When nec-essary, I repositioned him with the help ofa medical professional. The physicianapproved the pressures used.
4 5 6MANY BONE METASTASES, EASILY FRACTURED; VERY LIMITED ACTIVITY LEVEL; STRONGACTIVITY RESTRICTIONS.A client was told by his physician that hemust drink coffee from paper cupsbecause the weight of a coffee mug couldcause fracture.THERAPY DECISION: This client had anextremely fragile skeleton. No pressure orjoint movement was used anywhere on hisbody. Instead, I used the gentlest holding,with stroking of the skin only. No displace-ment of muscles. Repositioning him formassage was ill-advised; instead, I decid-ed to work with him in the position inwhich I found him. When necessary, Irepositioned him with the help of a med-ical professional. The physician approvedthe pressures used.
BONE METASTASIS

13
0m
tj/m
assa
ge t
hera
py jo
urna
lsu
mm
er 2
00
6
The first client has a tumor in a vitalorgan with minimal changes in func-tion. The second scenario requires amuch more modified massage inresponse to vital organ involvement, asthe client’s function is impaired. Theseare very different scenarios, suggestinga wide range in brain function. Bothcases show that there is no one mas-sage response to a brain tumor.Instead, get a sense of vital organ func-tion and modify massage accordingly.In both these cases, approval for mas-sage from the client’s physician withguidance about any adjustments inmassage therapy focus, pressure andmovement is essential.
Because cancer treatment, as well ascancer itself, can affect some vitalorgan functions, it is worthwhile toexpand the interview question to, “Hascancer or its treatment affected thefunction of any of the following…?”Then list the vital organs.
deep vein thrombosisDEEP VEIN THROMBOSIS IN CLIENTS WITH CANCERMassage therapists need to learn allthey can about the risk of DVT in mas-sage therapy practice, how to assessrisk and how to get help from a client’sphysician. Some aspects of cancer orits treatment can increase a client’srisk of DVT— a blood clot. In particu-lar, advanced cancer—and even somespecific cancers such as lung, pancreasand gut (stomach, small intestine,colon, rectum and anus)—raise therisk of DVT above normal levels.
The danger of DVT lies in a clot, orthrombus, that detaches from thewalls of the veins and floats free in thevenous circulation. Here it is called anembolus. A blood clot formed in theveins of the extremities—especiallythe legs, where they are most likely toform—can do considerable damage ifit is dislodged. Traveling from theseveins, a process known as emboliza-tion, the clot can continue through
the right side of the heart to the pul-monary circulation. There, the embo-lus can lodge on the arterial side of thelungs, blocking further blood flow andinhibiting necessary oxygenation ofthe blood. This situation, called pul-monary embolism, can cause short-ness of breath, chest pain, rapid heartrate or cough (with bloody phlegm). Itis life threatening, and is treated as amedical emergency.
DVT is of particular interest tomassage therapists, because it’simportant to avoid any pressure ormovement that could detach a clotfrom the veins of the extremities,initiating an embolism. But a bloodclot can be clinically silent. It doesnot always produce signs or symp-toms. A blood clot can be difficult forphysicians to diagnose.
One response to this uncertaintywould be to avoid all massage of theextremities in cancer patients, but thatwould be an overly conservativeapproach. Instead, to manage theuncertainty and risk of DVT in practice,along with the therapeutic need formassage of the extremities, hone yourinterview skills to get specific informa-tion from the client. To work safely withthis population, you need to distinguishbetween two client scenarios: � A client who you suspect has devel-
oped DVT (because he or sheshows signs or symptoms);
� A client at risk for DVT (because heor she has one or more risk factors).
These two scenarios require very dif-ferent follow-up on your part.
SUSPECTED DVT—RECOGNIZINGSIGNS OR SYMPTOMS DVT can occur in upper or lowerextremity; however, the most commonscenario is a thrombus in the lowerextremity, which will be discussed inthis article. Usually it occurs unilater-ally, although it can occur in both legs.About half the time, DVT occurs with-
WHO IS AT RISKFOR DVT?Recognizing the risk of DVT is more diffi-
cult than recognizing the symptoms that
lead you to suspect DVT. DVT risk increas-
es above the normal level for a number of
reasons—cancer is only one of them.
Risk factors for DVT include:� Some cancer treatments.� Immobility (72+ hours of bed rest, long
plane or car ride, etc.).� Trauma.� Recent surgery (especially abdominal
and pelvic surgery such as for cancer,
orthopedic hip and knee surgery and
neurosurgical procedures).� Increasing age. � Obesity.� Pregnancy and the postpartum period.� Cardiac diseases.� Oral contraceptives.� Smoking.� Diabetes.� Previous occurrence of DVT or pul-
monary embolism.� Cancer, although different sources list
different types increasing the risk.
Included on some lists are lung,
pancreas, gastrointestinal, prostate,
ovarian, endometrial and breast.

ww
w.am
tamassage.org/m
tj1
31
out any signs or symptoms. Signs orsymptoms of DVT are a red flag andany one of these signs or symptomsputs the situation in the “suspectedDVT” category:� Pain or tenderness (can be nonspe-
cific, non-local and feel like a deepache).
� Blue coloration in skin, nail beds orboth.
� Redness.� Warmth.� Swelling.� A “cord-like” feeling in the leg
(could be an enlarged vein). � Enlargement of the superficial
veins (they look wider).
You need to be cautious if you workwith clients with cancer, or anyonecurrently or recently in cancer treat-ment. Be especially alert for possibleDVT. Any one of the above symptomsor signs is a red flag. While it is outsideof your scope of practice to diagnose,you can still recognize the signs orsymptoms of DVT and refer clients totheir physicians immediately.
ACTIONS TO TAKE FOR SUSPECTED DVTDVT is a medical emergency. If yoususpect a client might have DVT, wasteno time considering massage con-traindications; no massage is providedin these cases. Instead, in a firm, non-alarmist fashion, you should suggestthat the client call his or her physicianto see how he or she should proceed. Ifthe physician or the physician’s nursecannot be reached quickly, a visit tothe emergency room is necessary.
Some therapists might recoil at thisscenario—what if you’re wrong in sus-pecting DVT? Why alarm the clientunnecessarily? There is no crime insuspecting a problem and acting on it;it’s up to the client’s physician todetermine whether or not the problemis serious. Massage therapists don’tpossess the skill to assess or treat this
situation on their own. That’s why it’simportant to get physician assistanceas soon as possible.
RECOGNIZING DVT RISKSLow levels of activity (or immobility)have some influence on DVT risk.Immobility, by creating an environ-ment for venous stasis or blood pool-ing adds greatly to the risk of DVT.One familiar version of this is “econo-my class syndrome”—the develop-ment of blood clot after long airplaneflights. People sitting in cramped quar-ters, discouraged from movement, runan additional risk of clot formation.
Various scoring systems help peo-ple assess DVT risk. On one website,the client’s age and various risk fac-tors are used to calculate DVT risk.8
Other scoring systems, such as onefor emergency physicians, have beendeveloped that combine risk factorswith signs and symptoms to helpphysicians diagnose DVT.9
One thing that can help you recog-nize DVT risk and make an appropri-ate decision is to consider yourclient’s recent and ongoing activity. Aclient who is more active—exercisesregularly, walks to work every day oris generally up and about—is less atrisk of DVT than a client with rough-ly the same diagnosis and treatment,but whose fatigue keeps him or heron the couch or in bed much of the
day. Someone who has been in bedfor more than three days is also atgreater risk.
ACTIONS TO TAKE FOR CLIENTS AT RISK FOR DVT Not all risk factors are equal; somehave more weight than others.Different sources list different risk fac-tors, with different statistics. In thissea of conflicting information, what isa massage therapist to do? Most mas-sage therapy training doesn’t includeassessment of the likelihood of DVT.While the diagnosis should be left tothe physician, when working with apopulation with elevated risk, such ascancer patients, there are some basicguidelines you can follow: 1. Never massage a person showingsymptoms of DVT. If you observe signsof DVT, or the client reports symptoms,do not initiate or continue the mas-sage. The situation is now “suspectedDVT” and you should treat it as a med-ical emergency as described above.2. Be alert for the risks of DVT in peo-ple with cancer or other risk factors.3. Before using any massage pressure orjoint movement techniques on thelower extremities in any of the followingscenarios, (and many of the scenarioson the “risk list”) it is imperative to con-sult with the client’s physician for:� People with active cancer;� Anyone in cancer treatment, or
THE HOMAN’S SIGNSome medical and massage literature mention using Homan’s Sign tocheck for DVT. A test is considered positive for DVT if passive dorsiflexionproduces pain in the calf, a positive “Homan’s sign.” Although it persists insome of the literature, it is not considered a reliable indicator of DVT, and isill-advised. In fact, manipulating the area during this test could even beunsafe if it disturbs an existing thrombus. If you are concerned enough touse this test for DVT, you are concerned enough to consult the client’sphysician. Suspected DVT is a medical emergency. Contact the physician.

13
2m
tj/m
assa
ge t
hera
py jo
urna
lsu
mm
er 2
00
6
between treatments;� People whose cancer treatment
ended less than one year ago;� Anyone taking a medication that
increases DVT risk, including somedrugs that prevent cancer recurrence.
4. A note from the physician, sayingsimply, “massage is fine for this per-son” does not specifically address theDVT risk and role of massage. It is toogeneral. It does not substitute for afocused discussion, nor does it clearthe way for massage or movement ofthe legs with pressure. In the bestinterests of the client, the therapistshould be direct and specific with thephysician about DVT. Be sure to:� Inform the physician that you and
the client are discussing joint move-ment and massage of the lowerextremities with pressure.
� List the DVT risk factors that youknow about, ask if there are anyadditional risk factors, and explainthe interface of massage and DVTrisk.
� Be sure the physician speaksdirectly to the client’s DVT risk andunderstands that massage caninclude joint movement and rangeof pressures on the legs and feet.
5. If the massage setting or timingdoesn’t allow for involving the client’sphysician for the currently scheduledmassage, leave the lower extremitiesout of the session and focus on therest of the body. Leave the physiciancommunication for later in prepara-tion for the next session.
Remember that not just cancer, butcancer treatment such as surgery andsome medications can increase DVTrisk. This is why it’s good to ask aclient, and ultimately the client’sphysician: “Is there anything aboutthe cancer or cancer treatment thatmight increase your risk of bloodclots?” and “Did your doctor or nursetalk with you about any increasedrisk of blood clots during this time?”
DVT REVIEW The information about DVT may seemoverwhelming. Just remember, DVT isa medical problem that is diagnosed,treated and followed by physiciansand nurses. If a client is by definitionat higher risk of DVT, always ask thehealth care provider to consider theclient’s risk level before massaging thelower extremities with pressure. Makesure the physician understands thatyou use pressure on the legs. Also listthe risk factors that you know about;ask the physician to address thoserisk factors in the light of massage.
the role of the interviewMany interview questions are suggestedby the information above: questionsabout tumor sites, bone involvement,pain and DVT risk factors are just a few.These and other interview questionsprovide a good starting point for thera-pists looking for possible massage con-traindications. Asking so many ques-tions might seem overwhelming, and thelength of the interview might take up thewhole session! Most therapists are morecomfortable providing the hands-on ses-sion than conducting a lengthy inter-view, and may need time to get used tothese lines of questioning. And some ofyou work in high-volume, heavily sched-uled settings like on-site massage andspas, which may not allow for manymedical questions. In those settings, youmay be working without documentation,and getting only verbal informationabout a client’s cancer and cancer histo-ry before the session. Abridged inter-view strategies need to be used for man-aging clients in such settings, withoutsacrificing the flow of information need-ed to assess massage contraindications.
In reality, not every question needsto be asked of every client—somequestions are follow-ups to others. Andsome information, such as a client’spositioning needs, will emerge in thehands-on session, or as part of everylead-in to the massage. Some questions
For more information about cancer, go tothe American Cancer Society’s website atwww.cancer.org.>>

ww
w.am
tamassage.org/m
tj1
33
can be grouped or handled more effi-ciently under “umbrella” questionssuch as “How is the treatment affectingyou?” And with practice, many of thequestions can easily be worked into anatural conversation with the client.
No matter how streamlined or drawnout the interview becomes, it is an impor-tant, fundamental exchange. It goes farbeyond establishing contraindications.Each interview question says to clientsthat you are curious about how it is to bethem, in this time, in this situation, inthis body. These questions provide smallways for you to establish a connection.They can reduce the isolation a personfeels, and make small parts of the cancerjourney, where possible, a shared experi-ence. This sharing can happen in themoment—or later that day, when a ther-apist—curious about the client’s condi-tion, searches the web for more informa-tion about the client’s cancer treatment.This learning can inform future sessionswith the client or just make the therapistmore prepared for the next relevant situ-ation—with a different client, on a differ-ent day. The effort to gather informa-tion—from the client, from the massageliterature or from medical resources—isnever wasted.
Information on cancer, its complica-tions and the effects of cancer treat-ments is vast. No one can know it all,but bits of it stand out. This is useful ifyou are considering the best way to pro-vide massage. These factors help thera-pists consider the best pressure to use,possible positions, whether or not tomove a joint, or the appropriate lengthof a session for a client with cancer.
concluding thoughts Remember that not all cancer presen-tations are addressed in this course.Instead, it includes some of the com-mon issues encountered in massagetherapy practice. If you see somethingfurther in your practice, outside thescope of this article, you will need to doadditional homework to incorporate it
into your session design. Look to themany resources on massage and can-cer—books, articles, research andadditional training—for more informa-tion and guidance on working effective-ly and safely. Study patient educationliterature on the client’s condition andtreatment to learn more about how itaffects the body. And, of course,include the client’s physician in yourdecisions about contraindications.
Together with caring, skilled touch,information about a client’s experiencecan lead to a profoundly healingexchange. That is a compelling force inmassage therapy; it is no wonder thatclients and therapists alike are drawnto it. �
�See Part 2 of this course aboutcontraindications due to cancertreatment in the Fall issue of mtj.
REFERENCES1. Curties D. “Could Massage Therapy
Promote Cancer Metastasis?” MassageTherapy Journal. 2000; 39(3):83-88.
2. Siegel B. “Clarifications” (letter to theeditor). Massage Therapy Journal,1996; 35(2):12.
3. Howarth DM, Southee AE, Whyte IM.“Lymphatic flow rates and first-aid insimulated peripheral snake or spiderenvenomation.” Med J Aust, 1994 Dec5-19;161(11-12):700-1.
4. MacDonald G. “How Cancer Spreads.”Massage Therapy Journal, 2001;39(4):74-78.
5. Curties D. “ Could Massage TherapyPromote Cancer Metastasis?” MassageTherapy Journal, 2000; 39(3):83-88.
6. Kaelin CM. Living through breast can-cer. New York: McGraw-Hill, 2005.
7. Walton T, Medical Conditions inMassage Therapy. Philadelphia:Lippincott Williams & Wilkins, (manu-script in preparation).
8. Sanofi-Aventis group. “DVT PreventionCenter; DVT Risk Assessor.” Availableat http://dvt.net/riskAssessorForm.do;accessed January 2006.
9. Stephen A. Colucciello, MD. DeepVenous Thrombosis: Risk FactorAssessment and Diagnosis. Available atwww.hypertension-consult.com/Secure/textbookarticles/Textbook/68_DVT.htm.Accessed January 2006.
For sample questions you should askyour clients with cancer, go towww.amtaonlinetraining.org.
>>
2THE NUMBER OF AMERICANS WHO EXPERIENCE DVT EACHYEAR.Source: American Heart Association
million
ADDITIONAL RESOURCES ON FOLLOWING PAGE