Embed Size (px)
Citation preview

Cancer Immunotherapy:A Long-Awaited Reality

2

3

4

Science 26 August 1977:Vol. 197 no. 4306 pp. 893-895DOI: 10.1126/science.887927 Reports
Metastasis results from preexisting variant cells within a malignant tumorIJ Fidler, ML KripkeAbstractClones derived in vitro from a parent culture of murine malignant melanoma cells varied greatly in their ability to produce metastatic colonies in the lungs upon intravenous inoculation into syngeneic mice. This suggests that the parent tumor is heterogeneous and that highly metastatic tumor cell variants preexist in the parental population.
5

• The antigen discovery platforms of the past emphasized the use of common antigens and presently were based on the assumption of Intertumoral and Intratumoral homogeneity.
• There is now indisputable evidence from cancer genome DNA sequencing of extreme genetic diversity or heterogeneity.
• We cannot treat heterogeneous disease with homogeneous treatment.
• As immunologists we are aware of one evolutionary modality that exists to address the magnitude of cancer diversity—The Immune System.
Basic Tenets of This Presentation
6

7

Tumor Type
Codin
g m
uta
tions
per
tum
or 20 - 80
Mutation rate = ~0.5 x 10-9 mutations
/bp/generation
(Jones et al., PNAS 105: 4283, 2008)
8
Cancers Sequenced at Genome-wide Level

1. Among different patients2. Within primary tumors3. Among cells that metastasize4. Within metastatic lesions
Heterogeneity
9

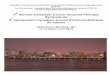
Genomic Landscape of Colorectal Cancer
A two-dimensional map of genes mutated in colorectal cancers, in which a few gene “mountains” are mutated in a large proportion of tumors while most “hills” are mutated infrequently. The mutations in two individual tumors are indicated on the lower map.
Wood, L and B. Vogelstein, Science Vol. 318, November, 2007.
10

1. Among different patients2. Within primary tumors3. Among cells that metastasize4. Within metastatic lesions
Heterogeneity
11

Heterogeneity within primary tumors
12

Nucleus Cytoplasm ExtracellularSpace
DNA RNA Protein
Inside-Out
RNA
Phosphorylated
Glycosylated SUMOylated
Ubiquitinated
Cleaved
Splice variantIsomerize
Dimerize
-PO 44OP-
-Sialyl Lewis XSia
lyl L
ewis
X -
SubcellularLocalization
CovalentPost-Translational
Modifications
Post-TranslationalProcessing
Protein
“Cancer-Specific”
13

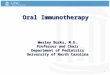
©2011 by American Society of Clinical Oncology
Wagle, N., et al., JCO 29:3085 (2011)
Treatment with PLX4032
14

Before Rx 6 months
Wagle, N., et al., JCO 29:3085 (2011)
Treatment with PLX4032
15
©2011 by American Society of Clinical Oncology


• We cannot treat heterogeneous disease with homogeneous treatment.
• As immunologists we are aware of one evolutionary modality that exists to address the magnitude of cancer diversity—The Immune System.
Basic Tenets of This Presentation
17

The Universe of Immunotherapy Players
Early Stage Occult Disease & Autologous/ Patient Specific
On-Going Development
Vaccinogen (OncoVAX®)
Late Stage & Autologous (Patient Specific)On-Going Clinical Development Argos Therapeutics (AGS-003)Bellicum Pharmaceuticals (BP-GMAX-CD1)Biovest/Accentia (BioVaxID)Dendreon (Provenge)ImmunoCellular Therapeutics (ICT-107)Northwest Biotherapeutics (DCVax)
Development CeasedAntigenics (Oncophage)AVAX (MVax)Favrille (FavID)Genitope (MyVax)Genzyme (Dendritic Tumor Cell Fusion)Genzyme (Melan-A/MART-1)IDM Pharma (UVIDEM & COLLIDEM)
Late Stage & Allogeneic/off the shelf
On-Going Clinical Development Advaxis (ADXS11-001)Apthera (NeuVax)Bavarian Nordic (PROSTVAC)BioVex (OncoVex)Celldex (CDX-110)CG Therapeutics (CG201)Cytos CYT004-MelQbG10)Eisai (Amolimogene)GSK (MAGE-A3)KAEL-GemVAX (GV1001)Medarex/BMS (MDX-1379+MDX-010)Merck KGaA/Oncothyreon (Stimuvax)New Link Genetics (HyperAcute)Nova Rx (Lucanix)Onyvax (Onyvax-P)Oxford Biomedica (TroVax)Transgene (TG 4010)
Development CeasedAphton (Insegia)AVI Biopharma (Avicine)Breakthrough Therapeutics (ABLVAX)CancerVax/Serono (Canvaxin)Cell Genesys (GVAX)Corixa (Melacine)Globelmmune (Tarmogen GI-4000)Imclone (Mitumomab)Menarini (abagovomab)Onyvax (105)Oxford Biomedica (Hi-8 Mel)Sanofi Pasteur (MEL11)Therion (PANVAC-VF)Titan Pharmaceuticals (CeaVac)
18

DNA
Inside-Out Outside-In
RNA
Phosphorylated
Glycosylated SUMOylated
Ubiquitinated
Cleaved
Splice variantIsomerize
Dimerize
-PO 44OP-
-Sialyl Lewis XSia
lyl L
ewis
X -
CovalentPost-Translational
Modifications
__________________Post-Translational
ProcessingProtein
“Cancer-Specific”
19

The immune system plays a dual role in tumor development. It can suppress tumor growth but also select for tumor cells that are capable of surviving in an immunocompetent host. This has been termed as immunoediting. Also it may involve antigen competition.
20
Host – Tumor Interaction
Schreiber RD, et al., Cancer Immunoediting: Integrating Immunity’s Roles in Cancer Suppression and Promotion, Science 331, 6024, (2011).Hanna Jr MG, Peters LC, The Effect of Antigen Competition on both the Primary and Secondary Immune Capacity in Mice, J Immuno, 104, 166 (1970).

Most malignant cells are believed to be recognized and eliminated by the immune system. The ones that manage to evolve and escape, however, eventually grow to become detectable tumors. Source: Vesely MD, et al., Annu. Rev. Immunol (2011)
Cancer Immunoediting

Best Hope for Significant Progress with Solid Tumorsis via Treatment of Minimal Residual Disease
22

• OncoVAX® immunotherapy is a patient-specific (personalized) tumor cell vaccine using BCG as an immune stimulant
• OncoVAX® immunotherapy induces a functional anti-tumor immune response
• OncoVAX® immunotherapy delays time-to-recurrence and improves recurrence-free survival
• OncoVAX® concept is based on the recognition of tumor heterogeneity, i.e., the genetic mutations in cancer cells may vary in every patient:
– no preconception “known” or shared tumor antigens – “known” antigens not demonstrated to be functional– allogeneic vaccines may lack important antigens
• Vaccinogen’s lead indication: Stage II colon carcinoma
Vaccinogen’s proprietary lead immunotherapy product
What is OncoVAX®?
23

24
Manufacturing (6 hours) + QA release
Tumor cells + TICE BCG
Tumor cells only
Surgery 1st Injection
2nd Injection
3rd Injection
4th Injection
Day 28-35 after surgery
1 week after 1st injection
1 week after 2nd injection
6 months after surgery
OncoVAX® Treatment Schedule

OncoVAX® — Clinical Results• Induction of a DTH response following injection of autologous tumor cells
DTH response specific to tumor, not adjacent mucosa
DTH response to 3rd and 4th vaccine dose
DTH in 27 Treated Patients and 11 Controls Responses to Tumor or
Colon Mucosa
25

Survival and disease-free survival in patients grouped according to their DTH response to the third vaccine.
26

27
Manufacturing (6 hours) + QA release
Tumor cells + TICE BCG
Tumor cells only
Surgery 1st Injection
2nd Injection
3rd Injection
4th Injection
Day 28-35 after surgery
1 week after 1st injection
1 week after 2nd injection
6 months after surgery
OncoVAX® Treatment Schedule

OncoVAX® Phase IIIa Study (8701) ResultsSignificant Improvement in Recurrence-Free Survival in Stage II
Cum
ula
tive P
robabili
ty
Years
Control OncoVAX
The results were published in the British Medical Journal The Lancet January 30, 1999; 353: 345-
350
28

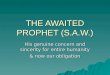
OncoVAX® Phase IIIa Study (8701) ResultsRecurrence-Free Interval (RFI) in Stage II
Cum
ula
tive P
robabili
ty
Years
Run Date: Nov. 30, 2000
Control OncoVAX
The results were published in the British Medical Journal The Lancet January 30, 1999; 353: 345-
350
Difference between treated and control: 16.1%
Greatest difference between treated and control in RFI at 18 months post-Vx
29

OncoVAX® Phase IIIa Study (8701) Results15-Year Follow Up (RFI) in Stage 2 Patients
Perc
ent
Su
rviv
al
Time (Years)
• Kaplan-Meier curves, comparing ASI with the control group in the original study population (n=254), show a significantly better prognosis for patients who received adjuvant ASI therapy
• ASI versus control at 15-year follow up
• HR=0.62 (95% CI: 0.34-0.96) log rank
• p-value 0.033
de Weger, Vincent A, et al., Clinical effects of Adjuvant Active Specific Immunotherapy differ between Patients
with Microsatellite Stable and Microsatellite Instable Colon Cancer, Clin Cancer Res 2012Feb1; 18(3):882-9.
30

Clinical Highlights
• Completed Phase IIIa trial with demonstrated efficacy– Statistically significant survival benefit in Stage II colon
cancer– 89.3% 5-year Recurrence-free survival rate
• Safe and well-tolerated– Over 350 patients have received 3-4 OncoVAX®
injections with no significant side effects– Major therapeutic index benefit over all chemotherapies
• First and only sterile and aseptically manufactured patient-specific autologous vaccine
31

8701 Phase III inProspectively
StratifiedStage II and IIIColon Cancer
8701 Phase III inProspectively
StratifiedStage II and IIIColon Cancer
ASI 2005-4,Phase III In Stage II(T3, T4 a&b) NOMO
ASI 2005-4,Phase III In Stage II(T3, T4 a&b) NOMO
Interim Analysis2018 (66% of
Expected Events)
Interim Analysis2018 (66% of
Expected Events)
Final PrimaryEndpoint Analysis
2020
Final PrimaryEndpoint Analysis
2020
ASI 2004 OLFPhase I in Stage III
Colon Cancer
ASI 2004 OLFPhase I in Stage III
Colon Cancer
DTH EvaluationFor Immune StatusASI + FolFOX 2017
DTH EvaluationFor Immune StatusASI + FolFOX 2017
Phase III inStage III
2020
Phase III inStage III
2020
Clinical Strategy for OncoVAX® in Colon Cancer 2015-2020
Completed & CMC ApprovedWith SPA and Fast Track
BLASubmission
+ ClinicalReportable
Event
BLASubmission
32

Forward-Looking Statements
This presentation and related commentary may contain forward-looking statements within the meaning of the Securities Act of 1933 (the “Securities Act”) and the Securities Exchange Act of 1934 (the “Exchange Act”) and are subject to the safe harbor created by the Private Securities Litigation Reform Act of 1995. Vaccinogen has based these forward-looking statements largely on our expectations and projections about future events and financial trends affecting the financial condition and/or operating results of its business. Forward-looking statements involve risks and uncertainties; particularly those risks and uncertainties inherent in the process of discovering, developing and commercializing drugs that are safe and effective for use as human therapeutics. There are important factors that could cause actual results to be substantially different from the results expressed or implied by these forward-looking statements.
In addition, in this presentation and related commentary, the words “believe,” “may,” “will,” “estimate,” “continue,” “anticipate,” “intend,” “plan,” “expect,” “potential,” or “opportunity,” the negative of these words or similar expressions, as they relate to Vaccinogen, its business, future financial or operating performance or Vaccinogen’s management, are intended to identify forward-looking statements. Past financial or operating performance is not necessarily a reliable indicator of future performance and you should not use Vaccinogen’s historical performance to anticipate results or future period trends.
Because such statements involve risks and uncertainties, many of which are outside of Vaccinogen’s control, Vaccinogen's actual results and performance may differ materially from the results expressed or implied by such forward-looking statements. Given these risks and uncertainties, readers are cautioned not to place undue reliance on such forward-looking statements. Other important risk factors that may affect Vaccinogen's business, results of operations and financial position are discussed in its most recently filed Registration Statement on Form 10 and in other Securities and Exchange Commission filings. Unless otherwise required by law, Vaccinogen also disclaims any obligation to update its view of any such risks or uncertainties or to announce publicly the result of any revisions to the forward-looking statements made here. However, readers should review carefully reports and documents that Vaccinogen files periodically with the Securities and Exchange Commission.
33