Embed Size (px)
Citation preview

CANCER
Embryonal precursors of Wilms tumorTim H. H. Coorens1, Taryn D. Treger1,2,3, Reem Al-Saadi4,5, Luiza Moore1,2, Maxine G. B. Tran6,7,Thomas J. Mitchell1,2,8, Suzanne Tugnait4, Christine Thevanesan4, Matthew D. Young1,Thomas R. W. Oliver1,2,9, Minou Oostveen4,5, Grace Collord1,2,3, Patrick S. Tarpey2, Alex Cagan1,Yvette Hooks1, Mark Brougham10, Ben C. Reynolds11, Giuseppe Barone5, John Anderson4,5,Mette Jorgensen5, G. A. Amos Burke2,3, Johannes Visser2, James C. Nicholson2,3, Naima Smeulders5,Imran Mushtaq5, Grant D. Stewart2,8, Peter J. Campbell1, David C. Wedge12,13, Iñigo Martincorena1,Dyanne Rampling5, Liz Hook2,9, Anne Y. Warren2,9, Nicholas Coleman2,9, Tanzina Chowdhury5,Neil Sebire4,5, Jarno Drost14, Kourosh Saeb-Parsy2,8, Michael R. Stratton1, Karin Straathof4,5,Kathy Pritchard-Jones4,5, Sam Behjati1,2,3*
Adult cancers often arise from premalignant clonal expansions. Whether the same is true of childhoodtumors has been unclear. To investigate whether Wilms tumor (nephroblastoma; a childhood kidneycancer) develops from a premalignant background, we examined the phylogenetic relationship betweentumors and corresponding normal tissues. In 14 of 23 cases studied (61%), we found premalignantclonal expansions in morphologically normal kidney tissues that preceded tumor development. Theseclonal expansions were defined by somatic mutations shared between tumor and normal tissues butabsent from blood cells. We also found hypermethylation of the H19 locus, a known driver of Wilmstumor development, in 58% of the expansions. Phylogenetic analyses of bilateral tumors indicated thatclonal expansions can evolve before the divergence of left and right kidney primordia. These findingsreveal embryonal precursors from which unilateral and multifocal cancers develop.
Adult cancers typically arise as a conse-quence of aging and mutagen exposure,at times through the generation of pre-cancerous clonal expansions. Examplesof these precancerous states include
Barrett’s esophagus, clonal hematopoiesis,and colonic polyps. It is unknown whetherchildhood tumors, which are thought to resultfrom aberrant fetal development, likewisearise from precancerous clonal expansions(Fig. 1A). To address this question, we studiedWilms tumor (nephroblastoma), the mostcommon kidney cancer of childhood. Wilmstumor is a prototypical embryonal malignancyof infants and young children (1). It arisesfrom abnormal fetal nephrogenesis, which itresembles morphologically (1) and transcrip-tionally (2). It occurs sporadically or in thecontext of bilateral tumors, multifocal lesions,urogenital developmental disorders, or over-growth syndromes (1).
To identify potential precursors of Wilmstumor, we used somatic mutations to infer thephylogenetic relationship between cancersand corresponding normal tissues (kidney andblood). We analyzed 229 whole-genome se-quences of 54 individuals: 23 children withWilms tumor, 16 parents of affected children,three children with other types of kidneycancer (congenital mesoblastic nephroma,malignant rhabdoid tumor), 10 adults withclear cell renal cell carcinoma (ccRCC), andtwo adults without renal tumors (one kidneytransplant patient and one kidney obtainedat autopsy; table S1). We called base sub-stitutions against the reference human ge-nome and extracted mosaic mutations fromeach set of donor-related tissues. We vali-dated the method for calling mosaic muta-tions by sequencing parental germline DNA,resequencing tissues, and inspecting rawdata (fig. S1). On the basis of the variantallele frequency (VAF) and distribution ofmutations across related tissues, we builtphylogenetic trees of tumor development.Wesupplemented DNA data with analyses ofRNA sequences and genome-wide methyl-ation patterns (table S1).Our discovery cohort consisted of three chil-
drenwith unilateralWilms tumor.We sampledtumors, blood, and histologically normal kid-ney tissues from the same individuals (table S1and fig. S2). As expected, whole-genome se-quences revealed mosaic mutations attributa-ble to the first cell divisions of the fertilized egg(fig. S3 and table S2) (3, 4). In two cases, we alsodetectedmosaicmutations in normal kidneysthat were present in the corresponding cancerbut absent from blood (Fig. 1, B to D, and table
S2), indicating that the tumors had arisen fromthat particular normal kidney tissue.Several features of these mutations showed
that they defined clonal expansions in normalkidney tissue, as illustrated by patient PD37272(Fig. 1, B to D). The VAFs of mutations in thenormal tissue of this kidney, variants 3 to 5(Fig. 1C), were as high as 44%,which suggestedthat the mutation was present in 88% of allcells in the biopsy. Mutations 3 to 5 were pre-sent in the two parenchymal biopsies (i.e., cor-tex and medulla) but were absent from bloodcell DNA, deeply sequenced to 106× genome-wide (fig. S4). Similarly, mutations 3 to 5 wereundetectable in renal pelvis, which is embry-ologically derived from a different lineagethan kidney parenchyma (5). Furthermore,the VAF of early embryonic mutations, var-iants 1 and 2, was inflated in parenchyma andin tumors (Fig. 1D). Such inflation of early em-bryonic mutations is a feature of tissues thatcontain a clonal expansion of a single cell (fig.S3). By contrast, in tissues devoid of a majorclone, such as renal pelvis and blood, the VAFsof early embryonicmutationswere not inflated(Fig. 1D). Thus, these normal tissue variants 3to 5 demonstrate the presence of clonal ex-pansions within kidney parenchyma, whichwe termed clonal nephrogenesis, accountingfor up to 88% of cells sampled in the cortex.To further study and validate our discovery
of clonal nephrogenesis as an antecedent ofWilms tumor, we studied another 20 cases:15 unilateral tumors with normal tissue biop-sies curated through a British childhoodrenal tumor study (IMPORT), four cases ofbilateral Wilms tumor, and one tumor with10 normal tissue biopsies (table S1 and fig.S5). Within the entire group of 23 children(discovery and validation cohorts), we foundevidence of clonal nephrogenesis in 10 of 19children with unilateral disease (53%) and inall four children with bilateral cancers (Fig. 2,A and B). The presence of clonal nephrogenesiswas further substantiated by the significant(P < 0.01, Wilcoxon signed-rank test) inflationof VAFs of early embryonic variants (fig. S6).There were no copy number changes detectedin normal tissues by three different methods.Conceivably these findings could be due to
tumor infiltration into normal tissue not visiblehistologically (fig. S2) or to cross-contaminationof DNAs. This explanation is implausible, ascontamination would manifest as shared var-iants at a lowVAF, rather than selectmutationsat a high VAF. We statistically excluded thepossible contribution of tumor infiltration andcontamination by using a binomial mixturemodel on the observed base counts of tumormutations in the normal samples (fig. S7).Next, we investigated whether clonal nephro-
genesis represents thenormal clonal architectureof human nephrons by three approaches.First, using laser capture microscopy (LCM),
RESEARCH
Coorens et al., Science 366, 1247–1251 (2019) 6 December 2019 1 of 5
1Wellcome Sanger Institute, Hinxton CB10 1SA, UK.2Cambridge University Hospitals NHS Foundation Trust,Cambridge CB2 0QQ, UK. 3Department of Paediatrics,University of Cambridge, Cambridge CB2 0QQ, UK. 4UCLGreat Ormond Street Institute of Child Health, London WC1N1EH, UK. 5Great Ormond Street Hospital for Children NHSFoundation Trust, London WC1N 3JH, UK. 6UCL Division ofSurgery and Interventional Science, Royal Free Hospital,London NW3 2PS, UK. 7Specialist Centre for Kidney Cancer,Royal Free Hospital, London NW3 2PS, UK. 8Department ofSurgery, University of Cambridge, Cambridge CB2 0QQ, UK.9Department of Pathology, University of Cambridge,Cambridge CB2 1QP, UK. 10Department of Haematology andOncology, Royal Hospital for Sick Children, Edinburgh EH91LF, UK. 11Department of Paediatric Nephrology, RoyalHospital for Children, Glasgow G51 4TF, UK. 12Big DataInstitute, University of Oxford, Oxford OX3 7LF, UK. 13OxfordNIHR Biomedical Research Centre, John Radcliffe Hospital,Oxford OX3 9DU, UK. 14Princess Máxima Center for PediatricOncology, Oncode Institute, 3584 CS Utrecht, Netherlands.*Corresponding author. Email: [email protected]
on April 22, 2021
http://science.sciencem
ag.org/D
ownloaded from

we excised glomeruli (n = 7) and proximal anddistal tubules (n = 15) from the kidneys ofthree individuals (Fig. 2, C and D). We sub-jected these LCM cuts to whole-genome se-quencing using an established method forgenerating low-input DNA libraries (6, 7).Kidney tissues were obtained at autopsy (onecase) or from normal portions of kidneys af-fected elsewhere by ccRCC (two cases). Ouranalysis of somatic mutations across theseLCM cuts revealed a VAF distribution (Fig. 2E)that is inconsistent with the monoclonal orga-nization seen, for example, in endometrialglands or colonic crypts (6, 7). Second, we as-sessed whether mutations were commonlyshared between renal tumors and surround-ing normal kidney tissue. We studied child-hood congenital mesoblastic nephroma (twotumors and six normal kidney samples), child-hood malignant rhabdoid tumor (one cancerand one normal kidney sample), and adultccRCC (eight cancers, including one bilateralcase, and 15 normal tissues). Applying thesame analysis pipeline, we identified earlyembryonic mutations shared between tumor,normal kidney tissues, and blood (fig. S8).However, we did not find mutations sharedonly between tumor and normal tissue (Fig.
2B); this finding shows that such mutationswere specific to, and enriched in,Wilms tumor(P < 0.001, Fisher exact test). Of particular rel-evance were renal cell carcinomas, which, likeWilms tumor, are derived from nephrons. Ifnormal embryological clonal dynamics typi-cally had generated clonal expansions, wewould have expected to find clonal nephro-genesis in ccRCC cases. Third, we examinedall developmental mutations of normal kidneytissues listed thus far, supplemented by anadditional 18 biopsies obtained from bilateralkidneys that had been declined for transplan-tation (Fig. 2B).We analyzed somaticmutationspresent in kidney tissue and absent from non-renal tissue, irrespective of whether they weresharedwith tumors. Collectively, these analysesof 77 normal kidney biopsies revealed that var-iants of tissues without clonal nephrogenesishave a significantly lowerVAFdistribution thanclonal nephrogenesis mutations (P < 0.001,Wilcoxon rank-sum test; Fig. 2B). Taken to-gether, these results indicate that clonal nephro-genesis represents aberrant kidneydevelopment.A central question raised by our findings is
whether cancer-causing (driver) events under-pin clonal nephrogenesis. Notably, the clonalnephrogenesis mutations (n = 66) (table S2
and fig. S8) were noncoding (64 of 66) or didnot generate plausible oncogenic events. Wesearched further for driver events amonggermline and somatic DNA mutations, intranscriptomes, and, where available, in meth-ylation patterns. We found hypermethylationof the H19 locus in 7 of 12 (58%) normal kidneytissues with clonal nephrogenesis. In contrast,we did not detect it in normal kidney tissueswithout clonal nephrogenesis or in blood (Fig.2, A and F), except for the blood of a child(PD40738) with Beckwith-Wiedemann syn-drome (fig. S9). H19 hypermethylation is anestablished driver event in the pathogenesisof Wilms tumor and is thought to operate bydisrupting the epigenetic regulation of growth-promoting genes that reside on chromosome11p15 (8–10). The degree of hypermethylationof H19 correlated with the VAF of clonal neph-rogenesis, indicating that hypermethylationpervaded the entire clone (Fig. 2G). In the fivewild-type samples, hypermethylation of H19may therefore have evaded detection becauseof a small clone size (Fig. 2A). We also studiedthe KvDMR1 locus on chromosome 11p15.5and determined that its methylation state wasunchanged in clonal nephrogenesis. Hypo-methylation of KvDMR1 underlies overgrowth
Coorens et al., Science 366, 1247–1251 (2019) 6 December 2019 2 of 5
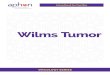
Fig. 1. Precursor clonal expansions innormal human kidneys. (A) Wilms tumorcan arise during embryogenesis on thebackground of an otherwise normal kidney(the traditional view) or from precursorlesions residing in normal tissues, as foundhere. (B) Overview of tissue sampling inthe kidney of patient PD37272. (C) Somaticmutations can be timed using their VAFacross the corresponding normal tissues,which is higher for earlier mutations. If themutation is present in tumor, kidney, andblood, it is an early embryonic mutation(mutations 1 and 2). If it is present inkidney samples and tumor only, it is clonalnephrogenic (mutations 3 to 5, markedby asterisk). If it is only in the tumor, it islabeled as such. White and black circlesindicate whether the observed VAF isinsignificant (white) or significant (black),P < 0.001 (test of presence using beta-binomial overdispersion). (D) The VAF forthe last embryonic mutation in kidneysamples and tumor compared with blood.
RESEARCH | REPORTon A
pril 22, 2021
http://science.sciencemag.org/
Dow
nloaded from

syndromes that confer only a minimal predis-position to Wilms tumor (11). We did not findany further driver events accounting for clo-nal nephrogenesis, despite re-interrogation byexome sequencing of 15 of 17 tissues with clo-nal nephrogenesis. Gene expression profiles,including fetal transcripts, did not differ be-tween normal renal tissues that displayed ordid not display clonal nephrogenesis (fig. S9).Similarly, global methylation patterns did notdiffer between these two groups (fig. S9).The timing of the emergence of clonal neph-
rogenesis during development could be definedin three children from whom we obtainedbilateral tumors. In patients PD40735 andPD36159, left and right tumors were derivedfrom the same trunk of clonal nephrogenesis(Fig. 3, A to D). In the third patient, PD40378,all five left tumors, but not the right neo-
plasms, were related to clonal nephrogenesison the left (Fig. 3E). These findings indicatethat in two children with bilateral cancers,clonal nephrogenesis must have arisen beforeleft and right kidney primordia diverged, earlyin embryogenesis (5). For unilateral tumors,the timing of the occurrence of clonal nephro-genesis remains unclear. It may have evolvedbefore the kidney was formed or thereafter,followed by a “clonal sweep” of clonal nephro-genesis replacing kidney tissue.In five cases, we sampledmultiple neoplasms
of the same kidney, which revealed two con-figurations of tumor development (Fig. 3).Tumors either were derived from a sharedtrunk that had emerged from clonal nephro-genesis (Fig. 3, A to E) or arose independentlyand successively from clonal nephrogenesis,which suggests a sustained potential for the
latter to spawn tumors (Fig. 3, F and G). Forexample, patient PD36165 presented withtwo lesions at opposing poles of the kidney:a nephrogenic rest and aWilms tumor. Cancerand the nephrogenic rest had emerged fromthe same ancestral clone at different timepoints, followed by clonal diversification with-in each (Fig. 3G).Finally, we compared the genetic alter-
ations in Wilms tumor with and without clo-nal nephrogenesis. This revealed a near–mutualexclusivity of loss of heterozygosity (LOH) ofchromosome 11p15 and clonal nephrogenesis.In tumors with clonal nephrogenesis, LOH of11p15 was mostly absent (P = 0.009, Fisherexact test) (fig. S10). This suggests that theremay be two distinct pathways for the patho-genesis of Wilms tumor that both involvedysregulation of 11p15 genes as a driver (Fig.
Coorens et al., Science 366, 1247–1251 (2019) 6 December 2019 3 of 5
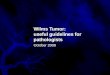
Fig. 2. Clonal nephrogenesis andH19 hypermethylation. (A) Sizes ofnephrogenic clones, as predicted by twicethe VAF of the most prominent nephro-genic mutation, alongside correspondingmethylation values of the H19 locus. Greensymbols indicate significant deviation(P < 0.05, Wilcoxon rank-sum test) fromthe background methylation distribution(gray shaded area) as obtained fromnormal kidney samples without clonalnephrogenesis. N/A, no methylation dataavailable. (B) Mutations present in samplesobtained from normal kidneys but absentin matched blood. Only in Wilms tumorwere some of these mutations shared withthe corresponding tumor. In the presenceof clonal nephrogenesis, the VAF distributionof these mutations was significantlyelevated (***P < 0.001, Wilcoxon rank-sum test). (C) Histology images showingcomponents (arrowheads) of the humannephron excised by laser capture micros-copy. Scale bar, 250 mm. (D) VAF simu-lations to derive expected distributionsdepending on clonality of a tissue: mono-clonal origin (~Bin(n~Pois(cov), P = 0.5)),oligoclonal origin (~Bin(n~Pois(cov),P = 0.3)), or polyclonal origin(~Bin(n~Pois(cov), P = 0.1)), wherecov = coverage = 40×. (E) VAF distribu-tions for 22 microdissected samples(10 proximal tubules, five distal tubules,seven glomeruli) from three patients, onerapid autopsy donor, and two ccRCCpatients. Color indicates the underlyingmaximum likelihood VAF as predicted by atruncated binomial mixturemodel. (F) Group-level methylation beta values of H19(*P < 0.05, Wilcoxon rank-sum test).(G) Relationship between predicted clonesizes from nephrogenic mutation (see Fig. 2A) and the methylation level of H19. The black dot represents patient PD40738g, who is affected by germline H19 hypermethylation(omitted from correlation and linear regression).
RESEARCH | REPORTon A
pril 22, 2021
http://science.sciencemag.org/
Dow
nloaded from

1A). Accordingly, cancers may arise either di-rectly in isolation through LOH of 11p15, orindirectly via clonal nephrogenesis with per-turbation of 11p15 by hypermethylation of H19.Our findings show that clonal expansions in
histologically normal tissue are an atypical out-come of renal development that commonly an-tedatesWilms tumor.We demonstrated a directphylogenetic link between clonal expansions,H19 hypermethylation, and the formation ofcancer, thus identifying clonal nephrogenesisas an epigenetic progenitor of cancer compris-ing “neoplasia-ready cells” (12). In contrast toprecursors of adult cancer, clonal nephrogene-sis generated histologically and functionallynormal tissues, which in themost pronouncedcases occupied the bulk of renal tissues. Iffuture work shows that the extent of clonalnephrogenesis is a marker of malignant po-tential and risk of cancer recurrence, this in-formation potentially could be used to guide
treatment and surveillance of patients withWilms tumor. Moreover, if we were able tomanipulate the neoplastic potential of clonalnephrogenesis, prevention of Wilms tumorcould become feasible. Collectively, our findingsportrayWilms tumor as an insurrection on thebackgroundof a premalignant tissue bed, ratherthana clearly demarcatedneoplasm inanother-wise normal polyclonal kidney. We speculatethat embryonal clonal expansions, perhaps alsodriven by epigenetic mechanisms, may be acommon phenomenon in childhood cancer.
REFERENCES AND NOTES
1. T. D. Treger, T. Chowdhury, K. Pritchard-Jones, S. Behjati,Nat. Rev. Nephrol. 15, 240–251 (2019).
2. M. D. Young et al., Science 361, 594–599 (2018).3. S. Behjati et al., Nature 513, 422–425 (2014).4. Y. S. Ju et al., Nature 543, 714–718 (2017).5. K. M. Short, I. M. Smyth, Nat. Rev. Nephrol. 12, 754–767
(2016).6. H. Lee-Six et al., Nature 574, 532–537 (2019).
7. L. Moore et al., bioRxiv 505685 [preprint]. 24 December 2018.8. T. Moulton et al., Nat. Genet. 7, 440–447 (1994).9. K. Okamoto, I. M. Morison, T. Taniguchi, A. E. Reeve,
Proc. Natl. Acad. Sci. U.S.A. 94, 5367–5371 (1997).10. J. Charlton et al., Genome Med. 7, 11 (2015).11. W. N. Cooper et al., Eur. J. Hum. Genet. 13, 1025–1032
(2005).12. A. P. Feinberg, R. Ohlsson, S. Henikoff, Nat. Rev. Genet. 7,
21–33 (2006).
ACKNOWLEDGMENTSWe thank the research nursing staff at Cambridge UniversityHospitals, the Royal Hospital for Sick Children (Edinburgh), andthe Royal Hospital for Children (Glasgow) as well as all IMPORTinvestigators. We thank M. Gerstung and A. J. Lawson for criticalreview of the manuscript. We are indebted to our little and olderpatients and their families for participating in our research. Funding:This project was principally funded by the Little Princess Trust,the St. Baldrick’s Foundation (Robert J. Arceci International Awardto S.B.), and Wellcome (fellowship to S.B.; Sanger core funding).Additional funding was received from CRUK (IMPORT study;fellowship to T.J.M.; Cambridge Centre), NIHR (BiomedicalResearch Centre Great Ormond Street; Cambridge HumanResearch Tissue Bank; Oxford Biomedical Research Centre;fellowship to T.R.W.O.), the Royal College of Surgeons ofEngland (fellowship to T.J.M.), Wellcome (fellowship to T.H.H.C.and K.S.), Great Ormond Street Hospital Children’s Charity
Coorens et al., Science 366, 1247–1251 (2019) 6 December 2019 4 of 5
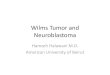
Fig. 3. Phylogenies of bilateral and multifocalWilms tumor. (A, C, E, and G) For each tumor,the phylogeny of shared mutations is shownincluding de novo germline mutations, embryonicmutations, mutations demarcating clonal neph-rogenesis, and tumor mutations. Numbers referto the number of substitutions defining eachdevelopmental trunk. Truncal driver events aredetailed. (B) Heat map showing the contributionof a mutation to the sample PD40735 shown in(A). The pattern of shared mutations reveals asplit betweenleft and right kidney, which is obeyedby both tumor and normal samples.(D) As revealed by the pattern of sharedmutations, in patient PD36159 the lefttumor is more closely related to the right branchof clonal nephrogenesis than tothe left branch. (F) Two mutations indicate theindependent emergence of tumorsat different time points from the nephrogenicclone in patient PD40641. As shown in (G),tumor and nephrogenic rest in patient PD36165both originated from clonalnephrogenesis despite being situatedat opposing kidney poles.
RESEARCH | REPORTon A
pril 22, 2021
http://science.sciencemag.org/
Dow
nloaded from

(R.A.-S., K.P.-J.), and Li Ka Shing foundation (D.C.W.). J.D.acknowledges funding from the Alpe d’HuZes foundation/KWFDutch Cancer Society Bas Mulder Award (#10218) and theOncode Institute. Author contributions: S.B. conceived of theexperiment. T.H.H.C., T.D.T., and S.B. analyzed data. Statisticalexpertise was provided by M.D.Y., D.C.W., and I.Ma. M.D.Y.,T.J.M., G.C., P.S.T., P.J.C., M.R.S., I.Ma., and K.P.-J. contributedto discussion. L.M. and M.G.B.T. performed laser capturemicroscopy experiments. Samples were curated and/orexperiments were performed by R.A.-S., C.T., S.T., M.O., Y.H.,M.B., B.C.R., G.B., J.A., M.J., G.A.A.B., J.V., J.C.N., N.S., K.S.-P.,
G.D.S., K.S., T.C., I.Mu., J.D., and K.P.-J. Pathological expertisewas provided by L.H., T.R.W.O., D.R., A.Y.W., N.C., and N.S.A.C. created kidney illustrations. T.H.H.C., T.D.T., and S.B. wrotethe manuscript. S.B. directed the study. Competing interests:G.D.S. is a paid consultant for Pfizer, Merck, EUSA Pharma,and Cambridge Medical Robotics. All other authors declare nocompeting interests. Data and materials availability: Rawsequencing data have been deposited in the European Genome-phenome Archive (EGA) under study ID EGAD00001004774.The bespoke code used for the analyses is available on GitHub(https://github.com/TimCoorens/ClonalNephrogenesis).
SUPPLEMENTARY MATERIALS
science.sciencemag.org/content/366/6470/1247/suppl/DC1Materials and MethodsFigs. S1 to S12Tables S1 to S8References (13–30)
View/request a protocol for this paper from Bio-protocol.
25 February 2019; resubmitted 4 July 2019Accepted 6 November 201910.1126/science.aax1323
Coorens et al., Science 366, 1247–1251 (2019) 6 December 2019 5 of 5
RESEARCH | REPORTon A
pril 22, 2021
http://science.sciencemag.org/
Dow
nloaded from

Embryonal precursors of Wilms tumor
Sebire, Jarno Drost, Kourosh Saeb-Parsy, Michael R. Stratton, Karin Straathof, Kathy Pritchard-Jones and Sam BehjatiC. Wedge, Iñigo Martincorena, Dyanne Rampling, Liz Hook, Anne Y. Warren, Nicholas Coleman, Tanzina Chowdhury, NeilBurke, Johannes Visser, James C. Nicholson, Naima Smeulders, Imran Mushtaq, Grant D. Stewart, Peter J. Campbell, David Cagan, Yvette Hooks, Mark Brougham, Ben C. Reynolds, Giuseppe Barone, John Anderson, Mette Jorgensen, G. A. AmosChristine Thevanesan, Matthew D. Young, Thomas R. W. Oliver, Minou Oostveen, Grace Collord, Patrick S. Tarpey, Alex Tim H. H. Coorens, Taryn D. Treger, Reem Al-Saadi, Luiza Moore, Maxine G. B. Tran, Thomas J. Mitchell, Suzanne Tugnait,
DOI: 10.1126/science.aax1323 (6470), 1247-1251.366Science
, this issue p. 1247Sciencetumors, Wilms tumor appears to arise from a premalignant tissue bed.of mutant cells in histologically and functionally normal kidney tissue long before tumor development. Thus, like adult
studied Wilms tumor, a childhood kidney cancer. Phylogenetic analyses revealed large cloneset al.unknown. Coorens are defined by somatic mutations shared by the cancers. Whether pediatric cancers originate in a similar way is
Many adult cancers arise from clonal expansions of mutant cells in normal tissue. These premalignant expansionsfrom the beginning−−A childhood tumor
ARTICLE TOOLS http://science.sciencemag.org/content/366/6470/1247
MATERIALSSUPPLEMENTARY http://science.sciencemag.org/content/suppl/2019/12/04/366.6470.1247.DC1
REFERENCES
http://science.sciencemag.org/content/366/6470/1247#BIBLThis article cites 29 articles, 4 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
is a registered trademark of AAAS.ScienceScience, 1200 New York Avenue NW, Washington, DC 20005. The title (print ISSN 0036-8075; online ISSN 1095-9203) is published by the American Association for the Advancement ofScience
Science. No claim to original U.S. Government WorksCopyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of
on April 22, 2021
http://science.sciencem
ag.org/D
ownloaded from