Embed Size (px)
Citation preview

CÁNCER DE MAMA TRIPLE
NEGATIVO.PRESENTE Y FUTURO
Dr. Pedro Sánchez Rovira
Complejo Hospitalario de Jaén.

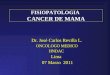
TRIPLE NEGATIVO
Ausencia de expresión de los tres receptores
C-erbB-2 (-) RP (-) RE (-)

TNBC prognosis is poor
TNBC
High risk of
early death
(between
3–5 years)2
Aggressive
biological
and clinical
features1
Large, high-grade tumours
Greater propensity to
metastasise to viscera
1. Foulkes, et al. N Engl J Med 2010; 2. Dent, et al. Clin Cancer Res 2007
Rapid rise in risk of recurrence
following diagnosis
Peak risk of recurrence at
1–3 years
Rapid progression from distant
recurrence to death







2004






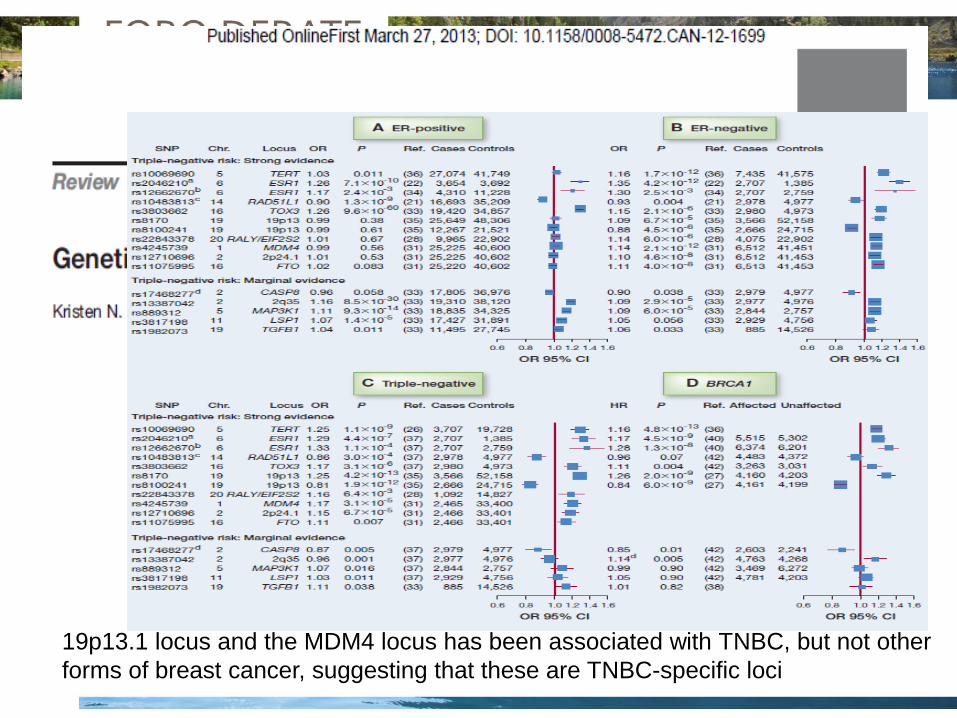
19p13.1 locus and the MDM4 locus has been associated with TNBC, but not other
forms of breast cancer, suggesting that these are TNBC-specific loci





Chemotherapy With or Without Trastuzumab After
Surgery in Treating Women With Invasive Breast Cancer
Condition Intervention Phase
Estrogen Receptor-negative Breast Cancer
Estrogen Receptor-positive Breast Cancer
HER2-positive Breast Cancer
Progesterone Receptor-negative Breast Cancer
Progesterone Receptor-positive Breast Cancer
Recurrent Breast Cancer
Stage IA Breast Cancer
Stage IB Breast Cancer
Stage II Breast Cancer
Stage IIIA Breast Cancer
Stage IIIC Breast Cancer
Drug: doxorubicin
hydrochloride
Drug: docetaxel
Drug: cyclophosphamide
Biological: trastuzumab
Drug: paclitaxel
Other: laboratory biomarker
analysis
Phase 3
ClinicalTrials.gov Identifier:
NCT01275677

HER2 Status and Benefit from Adjuvant
Trastuzumab in Breast Cancer
N Engl J Med 2008; 358:1409-1411

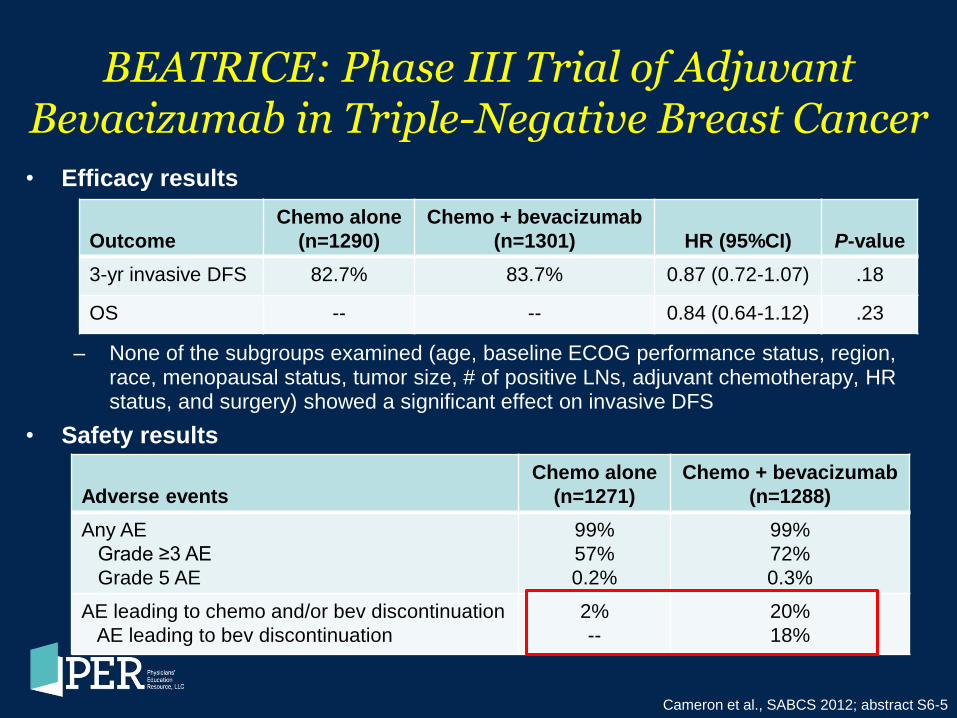
BEATRICE: Phase III Trial of Adjuvant Bevacizumab in Triple-Negative Breast Cancer
Cameron et al., SABCS 2012; abstract S6-5
• BEATRICE study design
Eligibility criteria:
• Resected triple-negative
(centrally confirmed) invasive
early breast cancer
4-8 cycles of standard chemotherapy
(investigator’s choice) R
A
N
D
O
M
I
Z
E
(N=2591)
4-8 cycles of standard chemotherapy
(investigator’s choice) + bevacizumab
5 mg/kg/wk equivalent for 1 year duration
Chemotherapy options:
• Taxane-based (≥4 cycles)
• Anthracycline-based (≥4 cycles)
• Anthracycline + taxane (3-4 cycles each)
Primary endpoint: DFS
Secondary endpoints: OS, breast
cancer-free interval, DFS, distant
DFS, safety, biomarkers
BEATRICE: Phase III Trial of Adjuvant Bevacizumab in Triple-Negative Breast Cancer
Cameron et al., SABCS 2012; abstract S6-5
• Efficacy results
– None of the subgroups examined (age, baseline ECOG performance status, region, race, menopausal status, tumor size, # of positive LNs, adjuvant chemotherapy, HR status, and surgery) showed a significant effect on invasive DFS
• Safety results
Outcome
Chemo alone
(n=1290)
Chemo + bevacizumab
(n=1301)
HR (95%CI)
P-value
3-yr invasive DFS 82.7% 83.7% 0.87 (0.72-1.07) .18
OS -- -- 0.84 (0.64-1.12) .23
Adverse events
Chemo alone
(n=1271)
Chemo + bevacizumab
(n=1288)
Any AE
Grade ≥3 AE
Grade 5 AE
99%
57%
0.2%
99%
72%
0.3%
AE leading to chemo and/or bev discontinuation
AE leading to bev discontinuation
2%
--
20%
18%

BEATRICE Trial: Biomarker Results
Baseline Plasma Concentration HR* P-Value
Median VEGF-A
High 0.81 .7415
Low 0.89
3rd Quartile VEGF-A
High 0.64 .3551
Low 0.92
Median VEGFR-2
High .61 .0291
Low 1.24
• Biomarker analysis performed to investigate potential predictive markers of
benefit from adjuvant bevacizumab
• Sub-study included 45% of total patient population
• Evaluated correlation of biomarkers with invasive disease-free survival
* HR <1.0 indicates CT plus Bev better than CT alone
Carmeliet et al., SABCS 2012; abstract P3-06-34


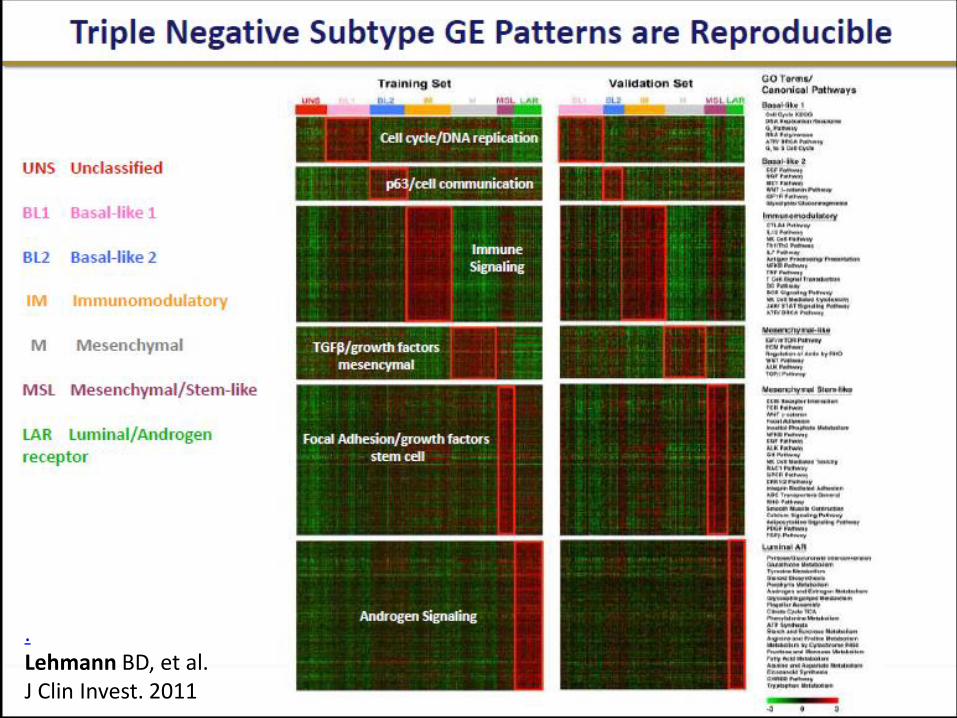
Triple-negative breast cancer subtypes and pathologic complete-response rate
to neoadjuvant chemotherapy: Results from the GEICAM/2006-2003 study.
Results: From the 94 enrolled pts, we processed 46 pre-treatment tumor
samples in a central lab and isolated high-quality RNA for microarray
analysis in 39 (42%); 7 samples are still pending to be analyzed. Tumors
were classified as follows: 4 BL1, 2 BL2, 8 IM, 5 LAR, 3 M, 3 ML with 7 pts
that couldn’t be assigned to any subtype and were not included in this
analysis. Three (75%) of the BL1 subtype pts achieved a pCR (p-
value=0.075). In contrast, IM and LAR achieved the lowest pCR rates (12%
and 20%, respectively). In the carboplatin-treated patients, 100% of BL1
patients showed pCR (p-value=0.033) in contrast with none of the IM and
LAR pts. Conclusions: Our preliminary findings suggest that TNBC
subtypes can predict tumor response to neoadjuvant CHT, supporting their
potential clinical utility in diagnosis, treatment selection and drug
development, bringing TNBC pts a step closer to personalized medicine.
Differential response of neoadjuvant chemotherapy with taxane-
carboplatin versus taxane-epirubicin in patients with locally advanced
triple-negative breast cancer.
Results: In total, 92 patients were enrolled between
January 2009 and December 2012. Of these, 43 patients
were assigned to TC group, and 49 to TE group. The pCR
rate was higher in TC group than in TE group (37.2%
versus 16.1%, p=0.032)
Abstract Number 1105


With a median follow-up of 9 months, 1-yr DFS was similar (~76%) in both
treatment groups. BROCA identified deleterious mutations in 22/101 (22%) pts (8
BRCA 1, 12 BRCA 2, 2 BRIP1). 1-yr DFS in the 22 pts with mutations was ~85%
compared to 79% without mutations. Whole transcriptome sequencing of paired
pre vs. post preoperative chemotherapysamples will be reported separately
(Radovich et al, ASCO 2014). Conclusions: The addition of low dose rucaparib
(current phase II monotherapy dose 600 mg orally twice daily) did not impact
the toxicity of cisplatin or improve 1-yr DFS. Comparison to predicted DFS
based on residual cancer burden (RCB) is planned to investigate potential benefit
from cisplatin. Genetic testing was underutilized in this high risk population with
only 30% of BRCA1 and BRCA2 mutations identified as part of routine clinical
care. Clinical trial information: NCT01074970.

Veliparib/carboplatino más tratamiento neoadyuvante estandar para pacientes triple
negativas: I-SPY 2 TRIAL

Paclitaxel + Trastuzumab* +
New Agent A
Paclitaxel + New Agent C
Patient
is on
Study
Paclitaxel+ Trastuzumab
Paclitaxel + Trastuzumab* +
New Agent B
Paclitaxel
Paclitaxel + New Agent E
AC
AC HER 2 (+)
HER 2
(–)
Randomize
Randomize
Surgery
Surgery
Learn and adapt
from each patient
as we go along
Paclitaxel + New Agent F
Paclitaxel + Trastuzumab* +
New Agent C
Paclitaxel + New Agent D Paclitaxel +
New Agent GH
Paclitaxel + Trastuzumab* +
New Agent F
*Investigational agent may be used in place
MRI
Residual
Disease
(Pathology)
Key
I-SPY 2 TRIAL:

I-SPY 2: the first graduate Rugo et al, #S5-02, SABCS, 2013
• Primary end point: pCR • Graduate regimens have >85% Bayesian predictive
probability of success in a 300-pts biomarker-linked neoadjuvant phase III trial
• Veliparib+carbo met the 85% predictive probability criterion in HR-/HER2- and all HER2- pts
% pCR p V+Cb better p of successful phase III All HER2- 35 vs 20 97% 71% HR+/HER2- 14 vs 15 44% 16% TNBC 52 vs 24 99% 92%
• V/Cb graduated with a TNBC signature and recommended for future trial
• Biomarker study? (lesson from iniparib)

Phase III study evaluating safety and efficacy of the
addition of veliparib plus carboplatin versus the
addition of carboplatin to standard neoadjuvant
chemotherapy in subjects with early-stage triple-
negative breast cancer (TNBC).
Gunter Von Minckwitz MD
Opened in Jan 2014. NCT02032277

A phase II study of tivantinib (ARQ-197) for
metastatic triple-negative breast cancer.
(c-met)
Sara M. Tolaney MD, MPH
Conclusions: This represents the first study of tivantinib for the
treatment of metastatic triple-negative breast cancer. These results
suggest that tivantinib is well tolerated, but is largely inactive when used as monotherapy to treat metastatic triple-negative breast
cancer.
NCT01542996.


A phase Ib dose escalation, open label, multicenter study
evaluating LDE225 in combination with docetaxel in Triple
Negative (TN) Advanced Breast Cancer (ABC) patients
EDALINE Study
Sponsor: GEICAM (Spanish Breast Cancer Research Group Foundation)
Sponsor Study Code: GEICAM/2012-12 (EudraCT: 2013-001750-96)
Medication code: CLDE225XES01T
Protocol version: 2.0
Protocol version date: 15 February 2014
Coordinating Investigator: Dr. Miguel Martín, H. General Universitario Gregorio Marañón, Madrid
selective smoothened inhibitor





Mechanism of action of combined PD-1 and CTLA-4
blockade
MHC = major histocompatibility complex; TCR = T-cell receptor
Margaret K. Callahan ASCO 2014


T helper responses are maintained by basal-
like breast cancer cells and confer to immune
modulation via upregulation of PD-1 ligands.
Breast Cancer Res Treat. 2014 Jun;145(3):605-14

Phase 1/2, Open-Label Study of Nivolumab (Anti-PD-1; BMS-936558, ONO-4538) as Monotherapy or
Combined With Ipilimumab in Advanced or Metastatic Solid Tumors
Margaret K. Callahan,1 Johanna Bendell,2 Emily Chan,3 Michael Morse,4
Rathi N. Pillai,5 Petri Bono,6 Dirk Jaeger,7 T. R. Jeffry Evans,8 Ian Chau,9 Emiliano Calvo,10 Dung T. Le,11 Patrick A. Ott,12 Matthew Taylor,13
Padmanee Sharma,14 Scott Antonia,15 Brian Sharkey,16 Olaf Christensen,16 Asim Amin17
1Department of Medicine at Memorial Sloan-Kettering Cancer Center, New York, NY, USA; 2Sarah Cannon Research Institute, Nashville, TN, USA; 3Vanderbilt-Ingram Cancer Center, Nashville, TN, USA; 4Duke University Medical Center, Durham, NC, USA; 5Winship Cancer Institute at Emory University, Atlanta, GA, USA; 6Cancer Center, Helsinki University Central Hospital,
Helsinki, Finland; 7National Center for Tumor Diseases, University Medical Center Heidelberg, Heidelberg, Germany; 8Beatson West of Scotland Cancer Centre, University of Glasgow, Glasgow, UK; 9The Royal Marsden Hospital, London and Surrey, UK; 10START Madrid, Centro Integral Oncológico Clara Campal, Madrid, Spain; 11Sidney Kimmel Comprehensive Cancer Center at
Johns Hopkins University, Baltimore, MD, USA; 12Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, USA; 13Oregon Health and Science University, Portland, OR, USA; 14The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 15H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA; 16Bristol-Myers Squibb, Princeton, NJ, USA;
17Levine Cancer Institute, Charlotte, NC, USA
Email: [email protected]
Poster 179B
Margaret K. Callahan ASCO 2014

EL CÁNCER DE MAMA TRIPLE NEGATIVO CONSTITUYE UN GRUPO HETEROGENEO DE SUBTIPOS CON DISTINTOS MECANISMOS BIOMOLECULARES.
DEBEMOS PONER EN MARCHA LOS MECANISMOS NECESARIOS PARA LA IMPLEMENTACIÓN DEL DIAGNÓSTICO MOLECULAR EN ESTE SUBGRUPO DE PACIENTES.
CON ELLO, EL TRATAMIENTO BASADO EN LA COMBINACIÓN DE ANTRACICLINAS Y TAXANOS PODRÍA INDIVIDUALIZARSE (INCLUSIÓN DE PLATINOS, ANTIANGIOGÉNICOS, INHIBIDORES DE PARP…)
CONSTITUYE UNO DE LOS PRINCIPALES DESAFIOS EN CÁNCER DE MAMA QUE NOS OBLIGA A PARTICIPAR EN LAS DISTINTAS LINEAS DE INVESTIGACIÓN.
GRACIAS