Upload
others
View
0
Download
0
Embed Size (px)
Citation preview
Research Article
Confounding of the Association betweenRadiation Exposure from CT Scans and Risk ofLeukemia and Brain Tumors by CancerSusceptibility SyndromesJohanna M. Meulepas1, C�ecile M. Ronckers2, Johannes Merks2, Michel E.Weijerman3,Jay H. Lubin4, and Michael Hauptmann1
Abstract
Background: Recent studies linking radiation exposure frompediatric computed tomography (CT) to increased risks ofleukemia and brain tumors lacked data to control for cancersusceptibility syndromes (CSS). These syndromes might beconfounders because they are associated with an increasedcancer risk and may increase the likelihood of CT scans per-formed in children.
Methods:We identify CSS predisposing to leukemia and braintumors through a systematic literature search and summarizeprevalence and risk estimates. Because there is virtually no empir-ical evidence in published literature onpatterns ofCTuse formosttypes of CSS, we estimate confounding bias of relative risks (RR)for categories of radiation exposure based on expert opinionabout the current and previous patterns of CT scans among CSSpatients.
Results: We estimate that radiation-related RRs for leukemia arenot meaningfully confounded by Down syndrome, Noonan syn-drome, or other CSS. In contrast, RRs for brain tumors may beoverestimated due to confounding by tuberous sclerosis complex(TSC) while von Hippel–Lindau disease, neurofibromatosis type 1,or other CSS do not meaningfully confound. Empirical data on theuse of CT scans among CSS patients are urgently needed.
Conclusions: Our assessment indicates that associations withleukemia reported in previous studies are unlikely to be substan-tially confounded by unmeasured CSS, whereas brain tumor risksmight have been overestimated due to confounding by TSC.
Impact: Future studies should identify TSC patients in order toavoid overestimation of brain tumor risks due to radiation expo-sure from CT scans. Cancer Epidemiol Biomarkers Prev; 25(1); 114–26.�2015 AACR.
IntroductionFive epidemiologic studies on cancer following radiation expo-
sure from pediatric computed tomography (CT) scans haveshown elevated risks of leukemia and brain tumors (1–5) andother studies are underway (6, 7). These studies are record-linkagecohort studies on large numbers of patients collected from exist-ing databases (health insurances andhospitals)with limitedor noinformation on potential confounding factors, which may biasthe radiation-cancer association. A confounder is associated withthe exposure in the source population from which the cases arise
and with the disease under study in the non-exposed populationand is not on the causal pathway.
Concerns have been raised about a possible overestimation ofradiation-related risks in studies of pediatric CT scans and cancerdue to confounding by indication (also called reverse causation;refs. 8–13). Confounding by indication occurs if the reason for aCT scan is associated with cancer risk.
With regard to CT studies, the primary concern is about twosources of confounding by indication, namely subclinical tumorsand cancer susceptibility syndromes (CSS). Cancer in a subclinicalprodromal phase may cause symptoms that necessitate a CT scan.The CT radiation dose is solely associated with detection and notwith disease causation. This source of confounding by indicationis often amenable to evaluation through the use of an exclusionperiod. CSS, on the other side, are congenital disorders and areassociatedwith increased cancer risk at one ormore sites (14). Thepotential for confounding arises because CSS patients may haveCT scans for early symptoms of the syndrome, diagnostic pur-poses, monitoring of disease progression, or associated comor-bidities (15, 16).We focus onCSS becausewe believe that they arethe potentially most important source of confounding byindication.
In the absence of empirical data, it appears plausible that CSSpatients are more likely to have one or multiple CT scans thanchildren without CSS. Because CT scans do not cause CSS, theobserved increased risk of cancer following pediatric radiationexposure from diagnostic imaging might be partly due to
1Department of Epidemiology and Biostatistics, Netherlands CancerInstitute, Amsterdam, the Netherlands. 2Department of PaediatricOncology, Emma Children's Hospital, Academic Medical CenterAmsterdam, the Netherlands. 3Department of Paediatrics,VU Univer-sity Medical Center, Amsterdam, the Netherlands. 4National Institutesof Health, Department of Health and Human Services, Bethesda,Maryland.
Note: Supplementary data for this article are available at Cancer Epidemiology,Biomarkers & Prevention Online (http://cebp.aacrjournals.org/).
Corresponding Author: Michael Hauptmann, Department of Epidemiology andBiostatistics, Netherlands Cancer Institute, Plesmanlaan 121, 1066 CX Amster-dam, the Netherlands. Phone: 31-20-512-1047; Fax: 31-20-669-1383; [email protected]
doi: 10.1158/1055-9965.EPI-15-0636
�2015 American Association for Cancer Research.
CancerEpidemiology,Biomarkers& Prevention
Cancer Epidemiol Biomarkers Prev; 25(1) January 2016114
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/http://cebp.aacrjournals.org/http://cebp.aacrjournals.org/
confounding byCSS. The largest studies published to date did notadjust their risk estimates for CSS. Such data are likely notavailable, because most countries do not have registries or othereasily accessible resources to identify CSS patients. For CSS wherethe direction of the potential confounding is known but not itsmagnitude, we use plausible scenarios to assess the magnitude ofpossible bias in studies of radiation exposure from pediatric CTscans (17).
This report focuses on pediatric CT scans, because children aremore radiosensitive than adults. The endpoints of primary con-cern are leukemia and brain tumors. These diseases are the mostcommon radiogenic malignancies among children, adolescents,and young adults and are the primary focus of published andongoing epidemiologic studies on cancer risk following pediatricCT scan exposure (18). Nevertheless, the results of our analysesprovide guidance for all epidemiologic studies of diagnosticimaging and cancer risk.
Materials and MethodsIn short, we identify CSS predisposing to leukemia or brain
tumors and characterize: their prevalence in the general popula-tion, the strength of their association with leukemia and/or braintumors, and their life expectancy. We then calculate the magni-tude of CSS-related confounding of relative risk (RR) estimates forleukemia and brain tumors after diagnostic CT scans, undervarious assumptions for the association between CSS and thefrequency of CT scans.
Identification and characterization of CSSWe identified CSS that are associated with increased risk of
either leukemia, or brain tumors, or both, at any age based ontwo major sources of information: (i) a table of genetic syn-dromes predisposing to childhood cancer from a thoroughsystematic review of the literature by a pediatric oncologistwho specializes in these syndromes (J. Merks; ref. 14) and (ii) asystematic overview of familial cancer syndromes (15). Third,we consulted with physicians specializing in genetic syndromesat three university hospitals (see the Acknowledgments section)to identify any other rare eligible CSS. Then, the pediatriconcologist (J. Merks) assessed the likelihood of medical radi-ation exposures for screening or health care for each of the CSS.Finally, we queried the MEDLINE database for each CSS todetermine prevalence, risk of leukemia and brain tumors, lifeexpectancy, and the likelihood of diagnostic imaging (in par-ticular CT scans). We included articles regardless of studydesign, as well as book chapters and systematic reviews. Articleswere identified by name of the syndrome combined with{epidemiology OR life expectancy OR systematic review ORleukemia OR CNS tumor OR brain tumors}. We typicallyreviewed the most recent reports and focused on large studieswith adequate methodology. Because empirical data on the roleof imaging in the diagnosis and monitoring of CSS patientswere extremely sparse, we relied on expert opinion to informscenarios concerning use of CTs among CSS patients for thoseCSS with the highest potential of confounding within therelevant timeframe from 1990 to 2012.
Quantitative assessment of confounding biasMost previous and ongoing epidemiologic studies include
patients who received at least one pediatric CT scan. We assumethat all studyparticipants receive someexposure and thus evaluate
potential confounding for higher exposure compared with lowerexposure. We estimate bias of the RR of leukemia or brain tumorsby CT-related radiation exposure due to unmeasured confound-ing by a particular CSS as
Bias ¼ RROBS/RRADJ ¼ [RRCD�pHI þ (1 � pHI)]/[RRCD�pLO þ(1 � pLO)] (1)
where RROBS is the RR of cancer comparing arbitrarily definedhigh- and low-exposure groups without adjustment for CSS,RRADJ is the corresponding RR adjusted for the CSS, RRCD is theRR of cancer among CSS patients compared with others in thereference population, pHI is the CSS prevalence in the highexposed group, pLO is the CSS prevalence in the low exposedgroup. Let g ¼ pHI/pLO and f ¼ pLO/p0, where p0 is the CSSprevalence in the general population, so that the CSS prevalencein the high exposed group is amultiple of the prevalence in the lowexposed (reference) group (pHI ¼ g�pLO), while the prevalence inthe low exposed group is a multiple of that in the generalpopulation (pLO ¼ f�p0) (19). If a CSS does not increase cancerrisk (RRCD ¼ 1), or if CT use is unrelated to CSS occurrence (pLO ¼pHI), there is no bias (bias¼ 1). An evaluation of potential bias forcomparison of children with any CT scans compared with thegeneral population [standardized incidence ratio (SIR)] can becarried out by setting pLO ¼ p0, i.e., f ¼ 1.
We use values of 1,. . .,5 for f and 1,. . ..,8 for g. For example,one scenario assumes that the prevalence of a particular CSSamong low exposed subjects is twice the general populationprevalence (f ¼ 2), while the CSS prevalence among highexposed subjects is 5-fold that among the low exposed (g ¼5), i.e., 10-fold the general population prevalence (pHI ¼2�5�p0). Because p0 is small, this is equivalent to CSS patientsbeing 2-fold and 10-fold more likely to be in the low and highexposed groups, respectively, compared with subjects withoutthe CSS.
We also calculated collective bias from all CSS predisposing toleukemia (and/or brain tumors) by summing their prevalencesand calculating the corresponding cancer risk as the mean of CSS-specific risks weighted by CSS prevalence. Finally, we consideredlife expectancy of all CSS. If life expectancy was severely limited,confounding would also be limited because the contribution ofperson-years from CSS patients would be very small and cancerevents would not contribute to the high exposed categories due tocommonly used lagging of exposure metrics by several years inthis type of research.
ResultsIdentification and characterization of CSS
We identified 31 CSS (Table 1), 16 of which are characterizedby population prevalence (p0) and estimated risk of leukemiaor brain tumors (Table 2). In decreasing order of prevalence,Down syndrome, fetal alcohol syndrome, Noonan syndrome,cystic fibrosis and neurofibromatosis type 1 (NF1) are the mostcommon syndromes in the general population (range, 39-160/100,000). Down syndrome, Li–Fraumeni syndrome (LFS),NF1, tuberous sclerosis complex (TSC), and von Hippel–Lindaudisease (VHL) carry the highest risks for leukemia or brain tumors.Childhood mortality from these syndromes is generally low, sothey cannot be ruled out as potential confounders based on lifeexpectancy (Table 1).
Confounding Radiation Exposure from CT Scans and Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 115
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
Table
1.Can
cersuscep
tibility
synd
romes
withan
increa
sedrisk
ofleuk
emia
orbrain
tumors
Riskofcanc
er
Syno
nym
Preva
lenc
eLife
expec
tanc
yaStud
ydesignan
dpopulation
Leuk
emia
Brain
tumors
Credibility/
valid
ity
Ataxiatelang
iectasia
AT
1–3/100,000(15)
20–4
9y(44)
Caseseries
of7
8ATpatients
(45),casereportof1
patient
(46),1p
atient
(47)
1�T-CLL
/1�
T-PLL
/5�-
ALL
1Astrocytoma
�1Med
ulloblastoma
Biallelic
Lynchsynd
rome
Mismatch
repair-
defi
cien
cy-syn
drome
Table
1.Can
cersuscep
tibility
synd
romes
withan
increa
sedrisk
ofleuk
emia
orbrain
tumors
(Cont'd)
Riskofcanc
er
Syno
nym
Preva
lenc
eLife
expec
tanc
yaStud
ydesignan
dpopulation
Leuk
emia
Brain
tumors
Credibility/
valid
ity
Gorlin
synd
rome
Nev
oid
basal-cell
carcinomasynd
rome
70y(79)
Caseseries
of173patients
(80),case
reportswith1
patient
(81–85)
3%ofthe173patients
hadmed
ulloblastoma,
case
reportsreported
5med
ulloblastoma
and1men
ingioma
�
Inco
ntinen
tiapigmen
tia
Bloch
–Sulzenb
erger
synd
rome
37
00
dea
thsofpeo
ple
(98),
multicentre
collaboration
of2108patients(99),
population-based
stud
yof135patients(100),case
reports(101,102)
15%–2
0%
ofchild
ren
withNF1d
evelopOPG
þ
1Glio
blastoma
1Med
ulloblastoma
Neu
rofibromatosistype2
NF2/multiple
inhe
rited
schw
anno
ma,
men
ingiomas
and
epen
dym
omas
synd
rome
2/100,000(87)
50–6
9y(79)
Cross
sectiona
lstudyof120
patients(103,104),clinical
spectrum
48patients
(105),6
3patients(106),
populationbased
stud
yof
406patients(107),clinical
stud
yof8
3patients(108),
retrospective
stud
yof283
patients(109,110)
Bilateralve
stibular
schw
anno
mas
90%–
95%
þ
Other
cran
ialn
erve
schw
anno
mas
24%–
51%
Intracranial
men
ingiomas
45%
–
58%
Nijm
egen
breakag
esynd
rome
NBS
1/100,000(111)
Sho
rten
edlifespan
due
tocancer
risk
and
infections
(112)
Reg
istryof55
patients(112),
case
series
of8patients
(113),case
reports(114–
116)
3T-cellp
recursor
ALL
2Med
ulloblastoma
�
1AML
1T-cellprolympho
cytic
leuk
emia
Noona
nsynd
rome
40–100/100,000(117)
Norm
al(118)
Retrospective
coho
rtof23
5patientsan
d62family
mem
bers(119),
Retrospective
coho
rtof
735patients(120
)
10%
Mye
loproliferative
disorder,3
precursor
B-A
LL,4
Juve
nile
mye
lomono
cytic
leuk
emia,3
ALL
,2CMML
þ
Rub
instein–T
aybisynd
rome
Broad
thum
b-hallux
Table
1.Can
cersuscep
tibility
synd
romes
withan
increa
sedrisk
ofleuk
emia
orbrain
tumors
(Cont'd)
Riskofcanc
er
Syno
nym
Preva
lenc
eLife
expec
tanc
yaStud
ydesignan
dpopulation
Leuk
emia
Brain
tumors
Credibility/
valid
ity
Silver–R
usselsyn
drome
1/100,000(126
)Norm
al(127
)Casereports(128
,129
)1Craniopha
ryng
ioma
�1Pilo
cyticastrocytoma
Sotossynd
rome
1/14,000(87)
Norm
alCaseseries
with22
4patients(130
)an
d27
patients(131)
3ALL
�
Sturge–
Web
ersynd
rome
SWS/encep
halofacial
angiomatosis
2–5/100,000(132
)Norm
al(133
)Retrospective
stud
ywith55
patients(134
,135
)3Ipsilateral
leptomen
ingea
lan
gioma
Trisomy8mosaicism
T8Ms/mosaic
Warkany
synd
rome
1/100,000(136
)NM
15%–20%
dev
elop
leuk
emia,syn
drome
often
detectedat
leuk
emia
diagno
sis
�
Trisomy13
Patau
synd
rome
4/100,000(137
)
1,0
00population)
withad
equa
tefollo
w-upmetho
dsan
dCCScase
ascertainm
ent.
*Ave
rage(þ
):largeco
hortstud
ieswitheither
inco
mplete
follo
w-uporinco
mplete
case
ascertainm
entmetho
dsORsm
allc
oho
rtstud
ies(<1,0
00population).
*Lo
w(�
):case
series,casereports;phy
sician
survey
s;review
sofcase
series/casereports.
Meulepas et al.
Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 Cancer Epidemiology, Biomarkers & Prevention118
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
Confounding of leukemia risk due to specific CSSDown syndrome is a genetic disorder caused by the presence
of all or part of a third copy of chromosome 21 and has aprevalence of about 160/100,000 (20). It is typically associatedwith physical growth delays, characteristic facial features, andmild-to-moderate intellectual disability. Leukemia risk amongpatients withDown syndrome is about 50-fold higher than that inthe general population (21). Ignoring confounding from Downsyndrome could maximally bias leukemia RRs about 2.0-fold(pHI/pLO ¼ 8; pLO/p0 ¼ 5; Fig. 1A).
Results for Down syndrome indicate that the potential forconfounding depends on the excess frequency of CT scans amongDown syndrome patients. Based on a recent review (22), imagingmodalities other than CT were adequate for Down syndromepatients in most clinical situations (Supplementary Table S1). Inthe absence of quantitative data from the literature, we inter-viewed a Down syndrome expert (M.E. Weijerman, pediatricianand head of the Down Center Netherlands), a pediatrician(Dr. Joost Frenkel, University Medical Center Utrecht), and anexperienced primary care physician (Dr. Bart Meijman, Amster-dam). They indicated that about 30% of children with Downsyndrome suffer lung problems, such as hyperplasia or cysts, anda fraction of those might have gotten one diagnostic chest CTsince 1990. For cardiac problems, which occur in about 44% ofDown syndrome patients (23), ultrasound is the imaging modal-ity of choice, except for a small fraction of children who need aninterventional procedure. Abdominal problems (e.g., 8% haveduodenal atresia or Hirschsprung's disease; ref. 24) are usuallyevaluated by X-ray. Experts stated that trauma does not seemto occur more often among children with Down syndromecompared with other children and that the fraction of Downsyndrome children with several CT scans due to the syndromeis considered very low. Based on a conservative quantificationof this information, if 20% of all children with Down syn-drome undergo one additional chest CT during their childhood(say, under 10 years of age) compared with other children, thiswould represent 20 CT scans per 1,000 Down syndromepatients per year attributable to Down syndrome in additionto the approximately 7 CT scans per 1,000 children per yearin the general Dutch population (25). There would then beabout (20 þ 7)/7 � 4-times as many CT scans among Downsyndrome patients than among other children, leading to less
than 20% bias of the SIR (pLO ¼ p0 and pHI ¼ 4�pLO) andno appreciable bias of the RR because the prevalenceof Down syndrome is not increasing further with exposurelevel because several CT scans due to Down syndrome are veryunlikely (Fig. 1A).
For Noonan syndrome and leukemia, the unadjusted RR over-estimated the adjusted RRbymaximally 30% (Fig. 1B).Other CSSwere either less prevalent or their association with leukemia wasweaker, or both, resulting in bias of 10% or less.
Confounding of brain tumor risk due to specific CSSTSC is an autosomal-dominant neurocutaneous disorder with
a prevalence of about 8/100,000 (26). It is characterized bytumors involvingmany organ systems, including the brain, heart,kidneys, and skin, as well as other organ dysfunction and mentalretardation. Subependymal giant cell tumors (SEGA), whichdevelop in 9% to 14% of patients and almost always occur before20 to 25 years of age (27), are amajor feature specific for TSC (15).Bias can be up to 4-fold (Fig. 2A). In the past, screening for SEGAswas recommended among children with TSC using CT or mag-netic resonance imaging (MRI) of the head every 1 to 3 years (28).MRI appears to be the preferred modality in more recent years(29) and has been used almost exclusively in the Netherlandssince at least 2000 (personal communication: Drs. Bernard Zon-nenberg and Floor Janssen,UniversityMedical CenterUtrecht;Dr.Marie Claire de Wit, Erasmus Medical Center Rotterdam). Ascenario consistent with these expert opinions assumes that10% of the TSC patients in a CT study cohort were born before1990 and received, on average, 3 headCTs during an average of 25years follow-up per patient, with corresponding numbers of 30%,1 head CT, and 15 years follow-up, as well as 60%, no head CT,and 10 years of follow-up for those born in 1990–2000 and after2000, respectively. In this case, 46headCTsper 1,000TSCpatientsper year would be indicated by TSC alone, which results in (46 þ7)/7¼7.6 times asmanyheadCTs among TSCpatients comparedwith others or, equivalently, a 7.6-fold higher prevalence of TSCamong children with at least one CT scan compared with childrenin the general population. Therefore, the potential bias of the SIRis about 2-fold (pLO ¼ p0 and pHI ¼ 7.6�pLO) and bias of the RRcould be more severe because a nonnegligible fraction of TSCpatients might have received a considerable number of head CTs(Fig. 2A).
Table 2. Selected CSS by general population prevalence and relative risk of leukemia and brain tumors
General population prevalence of CSS (per 100,000)
VHL disease is an autosomal-dominant disorder that causeshemangioblastomas of the retina and the central nervous system,renal cell carcinomas, pancreatic cysts and tumors, among othermanifestations. At a prevalence of 2–3/100,000 (30), 60% to 90%of patients with VHL disease develop hemangioblastomas of thecerebellum or the brain stem (31). VHL disease biased braintumor risk by up to 6-fold (Fig. 2B).
Because VHL-associated hemangioblastomas of the cerebellumand the brain stem occur rarely during childhood, screening isrecommended to commence in the mid-teens and MRI is uni-
formly the modality of choice, although CT was mentioned inearlier versions of some guidelines (32–34). Accordingly, imagingof the head for screening purposes among young children withVHL disease was not commonly done in the Netherlands. Whenperformed, CT might have been used before 1990–1995, whileMRI is themodality of choice since then. CT also has no importantrole in the screening for other VHL-related morbidity (personalcommunication: Prof. Peter Vandertop, VU University MedicalCenter AmsterdamandAcademicMedical Center Amsterdam;Dr.Netteke Schouten–van Meeteren, Emma Children's Hospital,
pHI=2pLO
pHI=4pLO
pHI=5pLO
pHI=7pLO
pHI=3pLO
pHI=6pLO
pHI=8pLO
1.00
1.10
1.20
1.30
1.40
1.50
1.60
1.70
1.80
1.90
2.00
54321
Est
imat
ed b
ias
of
CT
-rel
ated
RR
A
pHI=2pLO
pHI=3pLO
pHI=4pLO
pHI=5pLO
pHI=6pLO
pHI=7pLO
pHI=8pLO
1.00
1.05
1.10
1.15
1.20
1.25
1.30
54321
Est
imat
ed b
ias
of
CT
-rel
ated
RR
pLO /p0
pLO /p0
B
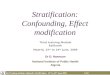
Figure 1.A, estimated potential bias of the relative risk of leukemia among high versus low exposed subjects by failure to adjust for Down syndrome. Bias ¼ RROBS/RRADJ¼ [RRCD�pHI þ (1 � pHI)]/[RRCD�pLO þ (1 � pLO)], where RROBS is the RR of leukemia comparing arbitrarily defined high and low (reference) exposure groupswithout adjustment for Down syndrome, RRADJ is the corresponding RR adjusted for Down syndrome, RRCD is the RR of leukemia due to Down syndromein the reference population, and pHI, pLO, and p0 are the prevalences of Down syndrome in the high exposed, low exposed, and general population,respectively (19). For example, under the assumption that the prevalence of Down syndrome among low exposed subjects is 5 times the general populationprevalence (pLO/p0 ¼ 5), and among the high exposed subjects is twice that in the low exposed group (pHI ¼ 2�pLO ¼ 2�5p0, i.e., 10 times the generalpopulation prevalence), the RR of leukemia not adjusted for Down syndrome overestimates the RR adjusted for Down syndrome by 13%. B, estimated potentialbias of the relative risk of leukemia among high versus low exposed subjects by failure to adjust for Noonan syndrome.
Meulepas et al.
Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 Cancer Epidemiology, Biomarkers & Prevention120
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
AcademicMedical Center Amsterdam;Dr. Theo vanOs, AcademicMedical Center Amsterdam; Prof. Thera Links, University MedicalCenter Groningen; Dr. Frederik Hes, University Medical CenterLeiden). It is therefore unlikely that a relevant number of VHLdisease patients are included in an epidemiologic study on CTscanning andmost of those would not have received several headCTs during childhood due to VHL disease.
NF1 is an autosomal-dominant disorder characterized by thedevelopment of multiple benign tumors of nerves and skin(neurofibromas) and areas of hypo- or hyperpigmentation of theskin. The most severe confounding bias caused by NF1 was about25% (Supplementary Fig. S1).
Other CSS were either less prevalent or their association withbrain tumors was weaker, or both. As a consequence, bias was10% or less.
Confounding bias due to combined CSSCombining all CSS predisposing to leukemia resulted in a
potential confounder with a prevalence of 282/100,000 and a
RR for leukemia of 14.8. This combination of prevalence and RRresulted in no additional confounding besides that from Downsyndrome (data not shown). Any CSS predisposing to braintumors were prevalent at 113/100,000 and carried a 713-foldelevated brain tumor risk, which resulted in confounding of thesame magnitude as VHL disease alone (data not shown).
DiscussionOur evaluation suggests that leukemia-predisposing CSS do
not substantially confound the association between radiationexposure from pediatric CT scans and leukemia risk because theyare too rare and/or too weakly associated with leukemia or, in thecase of Down syndrome, CT uptake is only moderately elevatedamong patients, if at all. Brain tumor risks might be substantiallyconfounded by TSC, while other brain tumor-predisposing CSSare unlikely to cause meaningful confounding. Because theseconclusions are based on assumptions about CT use among CSSpatients, robust empirical data are urgently needed.
pHI=2pLO
pHI=3pLO
pHI=4pLO
pHI=5pLO
pHI=6pLO
pHI=7pLO
pHI=8pLO
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50A
B
54321
Est
imat
ed b
ias
of
CT
-rel
ated
RR
pLO/p0
pHI=2p LO
pHI=3pLO
pHI=4pLO
pHI=5pLO
pHI=6pLO
pHI=7pLO
pHI=8pLO
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
5.50
6.00
54321
Est
imat
ed b
ias
of
CT
-rel
ated
RR
pLO/p0
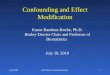
Figure 2.A, estimated potential bias of therelative risk for brain tumors amonghigh versus low exposed subjects byfailure to adjust for TSC. Bias ¼RROBS/RRADJ ¼ [RRCD�pHI þ(1 � pHI)]/[RRCD�pLO þ (1 � pLO)],where RROBS is the RR of brain tumorscomparing arbitrarily defined high andlow (reference) exposure groupswithout adjustment for TSC, RRADJ isthe corresponding RR adjusted for TSC,RRCD is the RR of brain tumors due toTSC in the reference population, andpHI, pLO, and p0 are the prevalences ofTSC in the high exposed, low exposed,and general population, respectively(19). B, estimated potential bias of therelative risk for brain tumors amonghigh versus low exposed subjects byfailure to adjust for VHL disease.
Confounding Radiation Exposure from CT Scans and Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 121
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
Confounding by TSC can be controlled through adjustment forTSC or exclusion of subjects with TSC. Themost promising sourceof such data for linkage with epidemiologic cohorts might be listsof TSC patients from hospitals treating TSC patients, which areusually limited to a few highly specialized medical centers. Incontrast, hospital discharge registries or registries of congenitaldisorders might not be complete for TSC since hospitalization isoften not required and most diagnoses do not occur perinatally(35). If individuals with TSC cannot be identified, it might bepossible to identify children who developed SEGAs based oncancer incidence data from cancer registries. We are currentlyinvestigating practical aspects of linkage with TSC patient listings.Also, several cancer registries in Europe register non-malignantbrain tumors, such as SEGAs, but little information regardingcoverage/completeness by country or region and calendar periodis available. The Dutch cancer registry records SEGAs since 1999,with most of them (93%) pathologically confirmed (personalcommunication: Dr. Otto Visser, Netherlands ComprehensiveCancer Organization). Exclusion of subjects who developedSEGAs will remove confounding; however, limiting follow-up topost-1999 will substantially compromise the statistical power ofour study.
A relevant question is whether bias due to CSS can create adose–response relationship in the absence of a causal associationbetween radiation and cancer. We did not directly evaluate biasof the linear excess relative risk per Gray (ERR/Gy), the commonlyused measure of the strength of a dose-response relationshipbetween radiation exposure and cancer, because we are notaware of a published formula for the relative bias due to con-founding. However, our results show that bias due to CSS cancreate increasing RR estimates for categories of increasing radia-tion exposure in the absence of a causal association, but only invery specific circumstances. If CT scanning among patients with aparticular CSS is such that the prevalence of CSS patients increasesacross categories of increasing dose, bias of RRs comparing sub-jects exposed at different levels with the same reference level willthen also increase with exposure level, leading to a positive ERR/Gy. This does not require the cancer risk due to CSS to increasewith radiation exposure.
Two studies with some information on indication for CTscanning have recently been published. The first study included67,274 children who received at least one CT scan before age 10years between 2000 and 2010 in one of 21 French hospitals andwho were followed for, on average, 4.4 years, with cancer diag-nosed before age 15 years as the outcome of interest (5). ERRs forleukemia or brain tumors were not or onlymildly attenuated afteradjustment for Down syndrome or neurofibromatosis, respec-tively, based on hospital discharge information. More substantialattenuation of the brain tumor ERRwas observed for the group ofso-called other phakomatoses, which includes TSC. A note ofcaution in interpreting these findings is warranted, though. First,because of the small sample size and short follow-up, all confi-dence intervals were wide and included unity, and attenuation forany of the evaluated (groups of) CSS was less than about 10% ofthe confidence interval width. Second, ERRs were not attenuatedwhenpatientswith relevantCSSwere excluded fromanalysis (36–38). Third, very high prevalences were observed for several CSS,most likely owing to overrepresentation of referral centers amongparticipating hospitals, which limits the generalizability of theseresults for nation-wide samples. The second study followed44,584 children who received at least one CT scan before age
15 years in the period 1980 to 2010 inone of 20Germanhospitalsfor, on average, 3.6 years and ascertained cancers diagnosedbefore age 15 years (4). Standardized incidence ratios werenonsignificantly elevated for leukemia and brain tumors. Radi-ology reports, which were available for most of the 12 leukemiasand 7brain tumors, respectively, indicated potential confoundingby indication for one brain tumor case. Exclusion of that caseslightly attenuated the brain tumor SIR.
Our study has a number of limitations. Although patients withCSS suffer from a diverse spectrum of health complaints (15) forwhich CT scans are an appropriate diagnostic imaging modality(16), actual quantitative health care utilization data are scarce andtherefore we had to rely on subjective scenarios. For illustration,with 5% to 7% of all children in the Netherlands receiving at leastone CT before their 18th birthday, a 10-fold higher proportionamong patients with a particular CSS implies that about 50% to70% of CSS patients receive at least one CT. Second, for some ofthe CSS evaluated here, there is evidence of increased radiosen-sitivity (e.g., AT, Xeroderma pigmentosum, and LFS; ref. 15). Forthose CSS, we might have underestimated bias because the CSS-related cancer risk increases with the level of radiation exposure.However, these CSS are very rare. Also, affected families andmedical professionals arewell aware of the radiosensitivity, whichlikely implies a prevalence of CT use lower than that of the generalpopulation. Therefore, these syndromes are very unlikely to bepotent confounders. Third, expert opinions on the use of CT scansamong patients with CSS reflect clinical practice in the Nether-lands. We believe this does not limit the generalizability becauseresults are likely similar both across Western countries with acomparable number of pediatric CTs and for countries withhigher levels of pediatric CT scanning, as long as CT scanning ismore commonacross all indications.However, it should be notedthat our results are only generalizable to countries with a roughlysimilar prevalence of a CSS. Fourth, confounding by other riskfactors such as socioeconomic status, birth weight, and parentalsmoking is beyond the scope of these analyses (39, 40). Finally,although we thoroughly reviewed the literature, we were not ableto find prevalence estimates for some CSS and those we found forothers are very heterogeneous with regard to precision. Never-theless, we believe that the CSS we identified cover all relevantsituations, as evidenced by the fact that most fields in the lowerright part of Table 2 are populated.
Besides CSS, other predisposing conditions can confoundCT-related cancer risk, for instance, leukemogenic drugs or totalbody irradiation prior to stem cell transplantation for non-malig-nant diseases, such as Fanconi anemia, aplastic anemia, immunesystem deficiencies, or congenital malformations in the nervousand circulatory system (41). Confounding by these conditions,although not the objective of this report, can be easily assessed byassigning the condition to one of the cells in Table 2. For example,common variable immune deficiency has a prevalence of approx-imately 1 in 30,000 live births (42) and an increased risk ofleukemia (43), although the magnitude is not known. Based onour results, even if leukemia risk was substantially increased,confounding bias would be negligible given the low prevalence.
In conclusion, our assessment of confounding of CT-relatedcancer risks indicates that associations with leukemia reported inprevious studies (1–5) are unlikely to be substantially confound-ed by unmeasured CSS, whereas brain tumor risks might havebeen overestimated due to confounding by TSC. Robust empiricaldata on the use of CT among CSS patients are needed in order to
Meulepas et al.
Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 Cancer Epidemiology, Biomarkers & Prevention122
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
inform the interpretation of previous and future studies of thesubject.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
DisclaimerThe funders had no involvement in the study design, data collection, analysis
and interpretation, the writing of the report, or the decision to submit the paperfor publication.
Authors' ContributionsConception and design: J.M. Meulepas, C.M. Ronckers, J. Merks,M. HauptmannDevelopment of methodology: J.M. Meulepas, C.M. Ronckers, J.H. Lubin,M. HauptmannAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): J.M. Meulepas, C.M. Ronckers, M. HauptmannAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): J.M. Meulepas, C.M. Ronckers, J. Merks, J.H. Lubin,M. HauptmannWriting, review, and/or revision of the manuscript: J.M. Meulepas,C.M. Ronckers, J. Merks, M.E. Weijerman, J.H. Lubin, M. HauptmannAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): J.M. Meulepas, M. HauptmannStudy supervision: M. Hauptmann
AcknowledgmentsThe authors sincerely thank Drs. Theo van Os (Academic Medical Center
Amsterdam), Joost Frenkel, Bernard Zonnenberg and Floor Janssen (UniversityMedical Center Utrecht), Bart Meijman (Amsterdam), Marie Claire de Wit(Erasmus Medical Center Rotterdam), Frederik Hes (University Medical CenterLeiden), Otto Visser (Netherlands Comprehensive Cancer Organization), andNetteke Schouten–van Meeteren (Emma Children's Hospital, Academic Med-ical Center Amsterdam) as well as Professors Thera Links (University MedicalCenter Groningen) and Peter Vandertop (VUUniversityMedical Center Amster-dam and Academic Medical Center Amsterdam) for providing their expertise.
Grant SupportThis work was supported by the European Community Seventh Framework
Programme (grant number FP7/2007-2013) under Grant Agreement Number269912-EPI-CT: "Epidemiological study to quantify risks for paediatric com-puterized tomography and to optimize doses" and by Worldwide CancerResearch formerly known as Association for International Cancer Research(AICR; grant number 12-1155). Dr. J.H. Lubin is supported by the IntramuralResearch Program of the NCI, NIH, Department of Health andHuman Services.Dr. C.M. Ronckers is supported by the Dutch Cancer Society.
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received June22, 2015; revisedOctober 23, 2015; acceptedOctober 23, 2015;published OnlineFirst November 23, 2015.
References1. Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, et al. Radiation
exposure fromCTscans in childhoodandsubsequent riskof leukaemiaandbrain tumours: a retrospective cohort study. Lancet 2012;380:499–505.
2. Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, Byrnes GB,et al. Cancer risk in 680,000 people exposed to computed tomographyscans in childhood or adolescence: data linkage study of 11 millionAustralians. BMJ 2013;346:f2360.
3. Huang WY, Muo CH, Lin CY, Jen YM, Yang MH, Lin JC, et al. Paediatrichead CT scan and subsequent risk of malignancy and benign braintumour: a nation-wide population-based cohort study. Br J Cancer 2014;110:2354–60.
4. Krille L, Dreger S, Schindel R, Albrecht T, AsmussenM, Barkhausen J, et al.Risk of cancer incidence before the age of 15 years after exposure toionising radiation from computed tomography: results from a Germancohort study. Radiat Environ Biophys 2015;54:1–12.
5. JournyN, Rehel JL,Ducou Le PointeH, LeeC, BrisseH,Chateil JF, et al. Arethe studies on cancer risk fromCT scans biased by indication? Elements ofanswer from a large-scale cohort study in France. Br J Cancer 2015;112:185–93.
6. Bosch de BaseaM, PearceMS, Kesminiene A, Bernier M-O,Dabin J, EngelsH, et al. EPI-CT: Design, challenges and epidemiological methods of aninternational study on cancer risks after paediatric CT. J Radiol Prot2015;35:611–28.
7. Meulepas JM, Ronckers CM, Smets AMJB, Nievelstein RAJ, Jahnen A, LeeC, et al. Leukemia and brain tumors among children after radiationexposure from CT scans: design and methodological opportunities ofthe Dutch Pediatric CT Study. Eur J Epidemiol 2014;29:293–301.
8. Hauptmann M, Meulepas JM. CT scans in childhood and risk of leukae-mia and brain tumours. Lancet 2012;380:1736–37.
9. Zopf DA, Green GE. CT scans in childhood and risk of leukaemia andbrain tumours. Lancet 2012;380:1735–36.
10. National Council on Radiation Protection and Measurements (NCRP).Uncertainties in the estimation of radiation risks and probability ofdisease causation: recommendations of the National Council on Radia-tion Protection and Measurements. NCRP report no. 171, 2012.
11. Walsh L, Shore R, Auvinen A, Jung T, Wakeford R. Re: Cancer risk in680,000 people exposed to computed tomography scans in childhood oradolescence: data linkage study of 11 million Australians. Online com-ment http://www.bmj.com/content/346/bmj.f2360/rr/648506, June 4,2013.
12. Walsh L, Shore R, Auvinen A, Jung T, Wakeford R. Risks from CT scans -what do recent studies tell us? J Radiol Prot 2014;34:E1–5.
13. Boice JD Jr. Radiation epidemiology and recent paediatric computedtomography studies. Ann ICRP 2015;44:236–48.
14. Merks JHM, Brecht IB. Genetic predisposition and genetic susceptibil-ity. In: Schneider DT, Brecht IB, Olson TA, Ferrari A, editors. Raretumors in children and adolescents. Heidelberg, Germany: Springer-Verlag; 2012. p. 69–94.
15. Lindor NM, McMaster ML, Lindor CJ, Greene MH. Concise handbook offamilial cancer susceptibility syndromes—second edition. J Natl CancerInst Monogr 2008:1–93.
16. Miglioretti DL, Johnson E,Williams A,Greenlee RT,Weinmann S, SolbergLI, et al. The use of computed tomography in pediatrics and the associatedradiation exposure and estimated cancer risk. JAMA Pediatr 2013;167:700–7.
17. Lash TL, Fox MP, Fink AK. Applying quantitative bias analysis to epide-miologic data. Series: Statistics for Biology and Health. New York:Springer; 2009.
18. United Nations Scientific Committee on the Effects of Atomic RadiationUNSCEAR. Report Vol. I. Effects of ionizing radiation, report of the GeneralAssemble with Scientific Annexes. New York: United Nations; 2006.
19. Axelson O. Aspects on confounding in occupational health epidemiol-ogy. Scand J Work Environ Health 1976;4:98–102.
20. WeijermanME, van FurthAM,VonkNoordegraaf A, vanWouwe JP, BroersCJ, Gemke RJ. Prevalence, neonatal characteristics, andfirst-yearmortalityof Down syndrome: a national study. J Pediatr 2008;152:15–9.
21. Hasle H, Clemmensen IH, Mikkelsen M. Risks of leukaemia and solidtumours in individuals with Down's syndrome. Lancet 2000;355:165–69.
22. Radhakrishnan R, Towbin AJ. Imaging findings in Down syndrome.Pediatr Radiol 2014;44:506–21.
23. Freeman SB, Taft LF, Dooley KJ, Allran K, Sherman SL, Hassold TJ, et al.Population-based study of congenital heart defects in Down syndrome.Am J Med Genet 1998;80:213–17.
24. Traubici J. The double bubble sign. Radiology 2001;220:463–4.25. National Institute for Public Health and the Environment (RIVM).
Analyse van trends in de stralingsbelasting als gevolg van beeldvormendediagnostiek. Report 610003001/2013, http://www.rivm.nl/bibliotheek/rapporten/610003001.pdf. [In Dutch].
26. O'Callaghan FJ, Shiell AW,Osborne JP, Martyn CN. Prevalence of tuberoussclerosis estimated by capture-recapture analyses. Lancet 1998;351:1490.
Confounding Radiation Exposure from CT Scans and Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 123
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
27. Adriaensen ME, Schaefer-Prokop CM, Stijnen T, Duyndam DA, Zonnen-berg BA, Prokop M. Prevalence of subependymal giant cell tumors inpatients with tuberous sclerosis and a review of the literature. Eur J Neurol2009;16:691–6.
28. Roach ES, DiMario FJ, Kandt RS, Northrup H. Tuberous Sclerosis Con-sensusConference: recommendations for diagnostic evaluation.NationalTuberous Sclerosis Assocation. J Child Neurol 1999;14:401–7.
29. Roth J, Roach ES, Bartels U, J�o�zwiak S, Koenig MK, Weiner HL, et al.,Subependymal giant cell astrocytoma: diagnosis, screening, and treat-ment. Recommendations from the International Tuberous SclerosisComplex Consensus Conference 2012. Pediatr Neurol 2013;49:439–44.
30. Maher ER, Neumann HP, Richards S. von Hippel–Lindau disease: aclinical and scientific review. Eur J Hum Genet 2011;19:617–23.
31. Lonser RR, Butman JA, Huntoon K, Asthagiri AR, Wu T. Prospectivenatural history study of central nervous system hemangioblastomas invon Hippel–Lindau disease. J Neurosurg 2014;120:1055–62.
32. VHL Alliance http://www.vhl.org/wordpress/library/screening-guide-lines.pdf. Accessed December 16, 2014.
33. Choyke PL, Glenn GM, Walther MM, Patronas NJ, Linehan WM, Zbar B.von Hippel–Lindau disease: genetic, clinical, and imaging features. Radi-ology 1995;194:629–42.
34. Lonser RR, GlennGM,WaltherM, Chew EY, Libutti SK, et al. vonHippel–Lindau disease. Lancet 2003;361:2059–67.
35. Curatolo P, Bombardienri R, J�o�zwiak S. Tuberous sclerosis. Lancet2008;372:657–68.
36. Muirhead CR. Response to `Are the studies on cancer risk from CT scansbiased by indication? Elements of answer from a large-scale cohort studyin France'. Br J Cancer 2015;112:1841–2.
37. Cardis E, de Basea MB. Comment on `Are the studies on cancer risk fromCT scans biased by indication? Elements of answer from a large-scalecohort study in France'-Evidence of confounding by predisposing factorsunclear. Br J Cancer 2015;112:1842–3.
38. Journy N, Laurier D, Bernier MO. Comment on: Are the studies on cancerrisk from CT scans biased by indication? Elements of answer from a large-scale cohort study in France. Br J Cancer 2015;112:1843–4.
39. Poole C, Greenland S, Luetters C, Kelsey JL, Mezei G. Socioeconomicstatus and childhood leukaemia: a review. Int J Epidemiol 2006;35:370–84.
40. Mezei G, Sudan M, Izraeli S, Kheifets L. Epidemiology of childhoodleukemia in the presence and absence of Down syndrome. CancerEpidemiol 2014;38:479–89.
41. Sun Y, Overvad K, Olsen J. Cancer risks in children with congenitalmalformations in the nervous and circulatory system - A populationbased cohort study. Cancer Epidemiol 2014;38:393–400.
42. StiehmER, Johnston RB Jr. A history of pediatric immunology. Pediatr Res2005;57:485–67.
43. Vajdic CM, Mao L, van Leeuwen MT, Kirkpatrick P, Grulich AE,Riminton S. Are antibody deficiency disorders associated with anarrower range of cancers than other forms of immunodeficiency?Blood 2010;116:1228–34.
44. Crawford TO, Skolasky RL, Fernandez R, Rosquist KJ, Lederman HM.Survival probability in ataxia telangiectasia. Arch Dis Child 2006;91:610–1.
45. Taylor AM, Metcalfe JA, Thick J, Mak YF. Leukemia and lymphoma inataxia telangiectasia. Blood 1996;87:423–38.
46. Groot-Loonen JJ, Slater R, Taminiau J, Voûte PA. Three consecutiveprimary malignancies in one patient during childhood. Pediatr HematolOncol 1988;5:287–92.
47. Hecht F, Hecht BK. Cancer in ataxia-telangiectasia patients. Cancer GenetCytogenet 1990;46:9–19.
48. Wimmer K, Kratz CP. Constitutional mismatch repair-deficiency syn-drome. Haematologica 2010;95:699–701.
49. Wimmer K, Etzler J. Constitutional mismatch repair-deficiency syn-drome: have we so far seen only the tip of an iceberg? Hum Genet2008;124:105–22.
50. Bloom's syndrome registry http://www.weill.cornell.edu/bsr/data_-from_registry/. Accessed June 2015.
51. Roberts A, Allanson J, Jadico SK, Kavamura MI, Noonan J, Opitz JM, et al.The cardiofaciocutaneous syndrome. J Med Genet 2006;43:833–42.
52. Makita Y, Narumi Y, Yoshida M, Niihori T, Kure S, Fuijeda K, et al.Leukemia in Cardio-facio-cutaneous (CFC) syndrome: a patient with a
germline mutation in BRAF proto-oncogene. J Pediatr Hematol Oncol2007;29:287–90.
53. van Den Berg H, Hennekam RC. Acute lymphoblastic leukaemia in apatient with cardiofaciocutaneous syndrome. J Med Genet 1999;36:799–800.
54. Nelen MR, Kremer H, Konings IB, Schoute F, van Essen AJ, Koch R, et al.Novel PTENmutations in patients with Cowden disease: absence of cleargenotype-phenotype correlations. Eur J Hum Genet 1999;7:267–73.
55. Pilarski R. Cowden syndrome: a critical review of the clinical literature.J Genet Couns 2009;18:13–27.
56. Derrey S, Proust F, Debono B, Langlois O, Layet A, Layet V, et al.Association between Cowden syndrome and Lhermitte-Duclos dis-ease: report of two cases and review of the literature. Surg Neurol2004;61:447–54.
57. Lindboe CF, Helseth E, Myhr G. Lhermitte-Duclos disease and giantmeningioma as manifestations of Cowden's disease. Clin Neuropathol1995;14:327–30.
58. Vinchon M, Blond S, Lejeune JP, Krivosik I, Fossati P, Assaker R, et al.Associationof Lhermitte-Duclos andCowdendisease: report of a new caseand review of the literature. J Neurol Neurosurg Psychiatry 1994;57:699–704.
59. Eng C,Murday V, Seal S, Mohammed S, Hodgson SV, ChaudaryMA, et al.Cowden syndrome and Lhermitte-Duclos disease in a family: a singlegenetic syndrome with pleiotropy? J Med Genet 1994;31:458–61.
60. Ratjen F, Doring G. Cystic fibrosis. Lancet 2003;361:681–9.61. Proesmans M, Vermeulen F, De Boeck K. What's new in cystic fibrosis?
From treating symptoms to correction of the basic defect. Eur J Pediatr2008;167:839–49.
62. Maisonneuve P, Marshall BC, Knapp EA, Lowenfels AB. Cancer risk incystic fibrosis: a 20-year nationwide study from the United States. J NatlCancer Inst 2013;105:122–9.
63. Yang Q, Rasmussen SA, Friedman JM. Mortality associated with Down'ssyndrome in the USA from 1983 to 1997: a population-based study.Lancet 2002;359:1019–25.
64. Huber RS, Houlihan D, Filter K. Dubowitz syndrome: a review andimplications for cognitive, behavioural, and psychological features. J ClinMed Res 2011;3:147–55.
65. Tsukahara M, Opitz JM. Dubowitz syndrome: review of 141 cases includ-ing 36 previously unreported patients. Am JMed Genet 1996;63:277–89.
66. Joenje H, Patel KJ. The emerging genetic and molecular basis of Fanconianaemia. Nat Rev Genet 2001;2:446–57.
67. Alter BP. Cancer in Fanconi anemia, 1927–2001. Cancer 2003;97:425–40.
68. Kutler DI, Singh B, Satagopan J, Batish SD, Berwick M, Giampietro PF,et al. A 20-year perspective on the International Fanconi Anemia Registry(IFAR). Blood 2003;101:1249–56.
69. Suarez F, Mahlaoui N, Canioni D, Andriamanga C, Dubois d'Enghien C,BrousseN, et al. Incidence, presentation, andprognosis ofmalignancies inataxia-telangiectasia: a report from the French national registry of primaryimmune deficiencies. J Clin Oncol 2015;33:202–8.
70. Rosenberg PS, Greene MH, Alter BP. Cancer incidence in persons withFanconi anemia. Blood 2003;101:822–6.
71. Hirsch B, Shimamura A, Moreau L, Baldinger S, Hag-alshiekhM, BostromB, et al. Association of biallelic BRCA2/FANCD1 mutations with spon-taneous chromosomal instability and solid tumors of childhood. Blood2004;103:2554–9.
72. Reid S, SchindlerD,HanenbergH, Barker K,Hanks S, Kalb R, et al. Biallelicmutations in PALB2 cause Fanconi anemia subtype FA-N and predisposeto childhood cancer. Nat Genet 2007;39:162–4.
73. Burd L, Peterson L, Kobrinsky N. Fetal alcohol spectrum disorders andchildhood cancer: a concise review of case reports and future researchconsiderations. Pediatr Blood Cancer 2004;61:768–70.
74. Streissguth AP, Aase JM, Clarren SK, Randels SP, LaDue RA, Smith DF.Fetal alcohol syndrome in adolescents and adults. JAMA 1991;265:1961–7.
75. Kiess W, LinderkampO,HadornHB, Haas R. Fetal alcohol syndrome andmalignant disease. Eur J Pediatr 1984;143:160–1.
76. Evans DG, Howard E, Giblin C, Clancy T, Spencer H, Huson SM, et al.Birth incidence and prevalence of tumor-prone syndromes: estimatesfrom a UK family genetic register service. Am J Med Genet Part A2010;152A:327–332.
Meulepas et al.
Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 Cancer Epidemiology, Biomarkers & Prevention124
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
77. Vasen HF, van Duijvendijk P, Buskens E, Bulow C, Bjork J, Jarvinen HJ,et al. Decision analysis in the surgical treatment of patients with familialadenomatous polyposis: a Dutch-Scandinavian collaborative studyincluding 659 patients. Gut 2001;49:231–5.
78. Attard TM, Giglio P, Koppula S, Snyder C, Lynch HT. Brain tumors inindividuals with familial adenomatous polyposis: a cancer registry expe-rience and pooled case report analysis. Cancer 2007;109:761–6.
79. Wilding A, Ingham SL, Lalloo F, Clancy T, Huson SM, Moran A, et al. Lifeexpectancy in hereditary cancer predisposing diseases: an observationalstudy. J Med Genet 2012;49:264–9.
80. Cowan R, Hoban P, Kelsey A, Birch JM, Gattamaneni R, Evans DG. Thegene for the naevoid basal cell carcinoma syndrome acts as a tumour-suppressor gene in medulloblastoma. Br J Cancer 1997;76:141–5.
81. Fukushima Y, Oka H, Utsuki S, Iwamoto K, Fuji K. Nevoid Basal cellcarcinoma syndrome with medulloblastoma and meningioma-casereport. Neurol Med Chir 2004;44:665–8.
82. Atahan IL, Yildiz F, Ozyar E, Uzal D, Zorlu F. Basal cell carcinomasdeveloping in a case of medulloblastoma associated with Gorlin's syn-drome. Pediatr Hematol Oncol 1998;15:187–91.
83. Korczak JF, Brahim JS, DiGiovanna JJ, Kase RG,Wexler LH, Goldstein AM.Nevoid basal cell carcinoma syndrome with medulloblastoma in anAfrican-American boy: a rare case illustrating gene-environment interac-tion. Am J Med Genet 1997;69:309–14.
84. Smucker PS, Smith JL. Multifocal desmoplastic medulloblastoma in anafrican-american child with nevoid basal cell carcinoma(gorlin) syn-drome. Case report. J Neurosurg 2006;105:315–20.
85. LacombeD,Chateil JF, FontanD, Battin J.Medulloblastoma in the nevoidbasal-cell carcinoma syndrome: case reports and review of the literature.Genet Couns 1990;1:273–7.
86. Berlin AL, Paller AS, Chan LS. Incontinentia pigmentia: a review andupdate on the molecular basis of pathophysiology. J Am Acad Dermatol2002;47:169–87.
87. Pagon RA, Adam MP, Ardinger HH, Bird TD, Dolan CR, et al., Gen-eReviewsTM[Internet]. Seattle: University of Washington; 1993–2014.
88. Minic S, Trpinac D, Obradovic M, Novotny GE, Gabriel HD, Kuhn M.Incontinentia pigmentiwithultrastructurally disordered leucocytes. J ClinPathol 2010;63:657–9.
89. Rivera R, Cangir A, Strong L. Incontinentia pigmenti (Bloch-Sulzbergersyndrome) associated with acute granulocytic leukemia. South Med J1975;68:1391–4.
90. Gonzalez KD, Noltner KA, Buzin CH, Gu D, Wen-Fong CY, Nguyen VQ,et al. Beyond Li–Fraumeni Syndrome: clinical characteristics of familieswith p53 germline mutations. J Clin Oncol 2009;27:1250–6.
91. McBride KA, Ballinger ML, Killick E, Kirk J, Tattersall MH, Eeles RA, et al.Li–Fraumeni syndrome: cancer risk assessment and clinical management.Nat Rev Clin Oncol 2014;11:260–71.
92. RuijsMW, Verhoef S, RookusMA, Pruntel R, van derHout AH,HogervorstFB, et al. TP53 germline mutation testing in 180 families suspected of Li–Fraumeni syndrome: mutation detection rate and relative frequency ofcancers in different familial phenotypes. J Med Genet 2010;47:421–8.
93. Birch JM,AlstonRD,McNally RJ, EvansDG,KelseyAM.Relative frequencyand morphology of cancers in carriers of germline TP53 mutations.Oncogene 2001;20:4621–8.
94. Garber JE, Goldstein AM, Katon AF, Dreyfus MG, Fraumeni JF Jr. Follow-up study of twenty-four families with Li–Fraumeni syndrome. Cancer Res1991;51:6094–7.
95. Rodriguez FJ, Perry A, Gutmann DH, O'Neill BP, Leonard J. Gliomas inneurofibromatosis type 1: a clinicopathologic study of 100 patients.J Neuropathol Exp Neurol 2008;67:240–9.
96. Listernick R, Charrow J, Greenwald M, Mets M. Natural history of opticpathway tumors in childrenwithneurofibromatosis type 1: a longitudinalstudy. J Pediatr 1994;125:63–6.
97. Guillamo JS, Cr�eange A, Kalifa C, Grill J, Rodriquez D, Doz F, et al.Prognostic factors of CNS tumors in Neurofibromatosis 1 (NF1): aretrospective study of 104 patients. Brain 2003;126:152–60.
98. Rasmussen SA, Yang Q, Friedman JM. Mortality in neurofibromatosis1: an analysis using U.S. death certificates. Am J Hum Genet 2001;68:1110–8.
99. Gutmann DH, Rasmussen SA, Wolkenstein P, MacCollin MM, Guha A,Inskip PD, et al. Gliomas presenting after age 10 in individulas withneurofibromatosis type 1 (NF1). Neurology 2002;59:759–61.
100. Huson SM, Compston DA, Clark P, Harper PS. A genetic study of vonRecklinghausen neurofibromatosis in South East Wales. I. Prevalence,fitness, mutation rate, and effect of parental transmission on severity.J Med Genet 1989;26:704–11.
101. Jeong TS, Yee GT. Glioblastoma in a patient with neurofibromatosis type1: a case report and review of the literature. Brain Tumor Res Treat2014;2:36–8.
102. Pascual-Castroviejo I, Pascual-Pascual SI, Viano J, Carceller F, Gutierrez-Molina M, et al. Posterior fossa tumors in children with neurofibroma-tosis type 1 (NF1). Childs Nerv Syst 2010;26:1599–603.
103. EvansDG,Maher ER, BaserME.Age related shift in themutation spectra ofgermline and somatic NF2 mutations: hypothetical role of DNA repairmechanisms. J Med Genet 2005;42:630–2.
104. EvansDG,Huson SM,DonnaiD,NearyW, Blair V. A clinical study of type2 neurofibromatosis. Q J Med 1992;84:603–18.
105. Mautner VF. Spinal tumors in patients with neurofibromatosis type 2:MRimaging studyof frequency,multiplicity and variety. AJRAm JRoentgenol1996;166:1231.
106. Parry DM, Eldridge R, Kaiser-Kupfer MI, Bouzas EA, Pikus A, Patronas N.Neurofibromatosis 2 (NF2): clinical characteristics of 63 affected indivi-duals and clinical evidence for heterogeneity. Am J Med Genet1994;52:450–61.
107. Baser ME, Kuramoto L, Joe H, Friedman JM, Wallace AJ. Genotype-phenotype correlations for nervous system tumors in neurofibroma-tosis 2: a population-based study. Am J Hum Genet 2004;75:231–9.
108. Fisher LM, Doherty JK, Lev MH, Slattery WH 3rd. Distribution of non-vestibular cranial nerve schwannomas in neurofibromatosis 2. Oto Neu-rotol 2007;28:1083–90.
109. Otsuka G, Saito K, Nagatani T, Yoshida J. Age at symptomonset and long-term survival in patients with neurofibromatosis type 2. J Neurosurg2003;99:480–3.
110. Asthagiri AR, ParryDM,Butman JA, KimHJ, TsilouET.Neurofibromatosistype 2. Lancet 2009;373:1974–86.
111. ChrzanowskaKH,GregorekH,Dembowska-Baginska B.Nijmegen break-age syndrome (NBS). Orphanet J Rare Dis 2012;28:7–13.
112. The International Nijmegen Breakage Syndrome Study Group. Nijmegenbreakage syndrome. Arch Dis Child 2000;82:400–6.
113. Resnick IB, Kondratenko I, Togoev O, Vasserman N, Shagina I, EvgrafovO, et al. Nijmegen breakage syndrome: clinical characteristics and muta-tion analysis in eight unrelated Russian families. J Pediatr 2002;140:355–61.
114. Michallet AS, Lesca G, Radford-Weiss I, Delarue R, Varet B, Buzyn A. T-cellprolymphocytic leukemia with autoimmune manifestation in Nijmegenbreakage syndrome. Ann Hematol 2003;82:517–7.
115. Distel L, Neubauer S, Varon R, Holter W, Grabenbauer G. Fatal toxicityfollowing radio- and chemotherapy of medulloblastoma in a child withunrecognized Nijmegen breakage syndrome. Med Pediatr Oncol 2003;41:44–8.
116. Bakshi S, Cerosaletti KM, Concannon P, Bawle EV, Fontanesi J, GattiRA, et al. Medulloblastoma with adverse reaction to radiation therapyin Nijmegen breakage syndrome. J Pediatr Hematol Oncol 2003;25:248–51.
117. Sharland M, Burch M, McKenna WM, Paton MA. A clinical study ofNoonan syndrome. Arch Dis Child 1992;67:178–83.
118. Shaw AC, Kalidas K, Crosby AH, Jeffery S, Patton MA. The natural historyof Noonan syndrome: a long-term follow-up study. Arch Dis Child2007;92:128–32.
119. Jongmans MC, van der Burgt I, Hoogerbrugge PM, Noordam K,Yntema HG, Nillesen WM, et al. Cancer risk in patients with Noonansyndrome carrying a PTPN11 mutation. Eur J Hum Genet 2011;19:870–874.
120. Kratz CP, Franke L, Peters H, Kohlschmidt N, Kazmierczak B, Finckh U,et al. Cancer spectrum and frequency among children with Noonan,Costello, and cardio-facio-cutaneous syndromes. Br J Cancer 2015;112:1392–7.
121. Hennekam RC, Van Den Boogaard MJ, Sibbles BJ, Van Spijker HG.Rubinstein-Taybi syndrome in The Netherlands. Am J Med Genet Suppl1990;6:17–29.
122. Hennekam RC. Rubinstein-Taybi syndrome. Eur J Hum Genet 2006;14:981–5.
Confounding Radiation Exposure from CT Scans and Cancer Risk
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 125
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
123. Bilir BM, Bilir N, Wilson GN. Intracranial angioblastic meningioma andan aged appearance in a woman with Rubinstein-Taybi syndrome. Am JMed Genet Suppl 1990;6:69–72.
124. Jonas DM, Heillbron DC, Ablin AR. Rubinstein-Taybi syndrome andacute leukemia. J Pediatr 1978;92:851–2.
125. Rosenberg PS, Alter BP, Link DC, Stein S, Rodger E, Bolyard AA, et al.Neutrophil elastase mutations and risk of leukaemia in severe congenitalneutropenia. Br J Haematol 2008;140:210–3.
126. Christoforidis A, Maniadaki I, Stanhope R. Managing children withRussel-Silver syndrome: more than just growth hormone treatement?J Pediatr Endocrinol Metab 2005;18:651–2.
127. Abu-Amero S,MonkD, Frost J, PreeceM, Stanier P,MooreGE. The geneticaetiology of Silver–Russell syndrome. J Med Genet 2008;45:193–9.
128. Draznin MB, Stelling MW, Johanson AJ. Silver–Russell syndrome andcraniopharyngioma. J Pediatr 1980;96:887–9.
129. Fenton E, Refai D, See W, Rawluk DJ. Supratentorial juvenile pilocyticastrocytoma in a young adult with Silver–Russell syndrome. Br J Neuro-surg 2008;22:776–7.
130. Hersh JH, Cole TR, Bloom AS, Bertolone SJ, Highes HE. Risk of malig-nancy in Sotos syndrome. J Pediatr 1992;120:572–4.
131. Fickie MR, Lapunzina P, Gentile JK, Tolkoff-Rubin N, Kroshinsky D,Galan E, et al. Adults with Sotos syndrome: review of 21 adults withmolecularly confirmedNSD1 alterations, including a detailed case reportof the oldest person. Am J Med Genet A 2011;155A:2105–11.
132. Comi AM. Update on Sturge-Weber syndrome: diagnosis, treatment,quantitative measures and controversies. Lymphat Res Biol 2007;5:257–64.
133. Thomas-SohlKA, VaslowDF,Maria BL. Sturge-Weber syndrome: a review.Pediatr Neurol 2004;30:303–10.
134. Pascual-Castroviejo L, Pascual-Pascual SI, Velazquez-Fragua R, Via~no J.Sturge-Weber syndrome: study of 55 patients. Can J Neurol Sci 2008;35:301–7.
135. Tseng BS, Haas-Kogan D. Neurocutaneous syndromes and associatedCNS tumors. In:Gupta N, Banerjee A, Haas-Kogan D, eds. Pediatric CNStumors. Berlin: Springer; 2004:183–203.
136. Hale NE, Kean JF Jr. Piecing together a picture of trisomy 8 mosaicismsyndrome. J Am Osteopath Assoc 2010;110:21–3.
137. Springett AL,Morris JK. Antenatal detection of Edwards (Trisomy 18) andPatau (Trisomy 13) syndrome: England and Wales 2005–2012. J MedScreen 2014;21:113–9.
138. Peroos S, Forsythe E, Pugh JH, Arthur-Farraj P, Hodes D. Longevityand Patau syndrome: what determines survival? BMJ Case Rep2012;2012.
139. Omar AO, Ahmad AE, El Bashir H, Al JaberMJ. Trisomy 13 in a 7-year-oldgirl with cerebellar tumor, eye abnormalities, and autistic features. Am JMed Genet A 2009;149A:1056–7.
140. Shepherd CW, Gomez MR, Lie JT, Crowson CS. Causes of death inpatients with tuberous sclerosis. Mayo Clin Proc 1991;66:792–6.
141. OstromQT, Bauchet L, Davis FG, Deltour I, Fisher JL, Langer CE, et al. Theepidemiology of glioma in adults: a "state of the science" review. NeuroOncol 2014;16:896–913.
142. Hamilton SR, Liu B, Parsons RE, Papadopoulos N, Jen J, Powell SM,et al. The molecular basis of Turcot's syndrome. N Engl J Med1995;332:839–47.
143. Schoemaker MJ, Swerdlow AJ, Higgins CD, Wright AF, Jacobs PA. Cancerincidence in women with Turner syndrome in Great Britain: a nationalcohort study. Lancet Oncol 2008;9:239–46.
144. Pier DB, Nunes FP, Plotkin SR, Stemmer-Rachamimov AO, Kim JC.Turner syndrome and meningioma: support for a possible increased riskof neoplasia in Turner syndrome. Eur J Med Genet 2014;57:269–74.
145. Lauper JM, Krause A, Vaughan TL, Monnat RJ Jr. Spectrum and risk ofneoplasia in Werner syndrome: a systematic review. PLoS One 2013;8:e59709.
146. Kleijer WJ, Laugel V, Berneburg M, Nordo T, Fawcett H, Gratchev A, et al.Incidence of DNA repair deficiency disorders in western Europe: Xero-derma pigmentosum, Cockayne syndrome and trichothiodystrophy.DNA Repair (AMST) 2008;7:744–50.
147. Lehmann AR, McGibbon D, Stefanini M. Xeroderma pigmentosum.Orphanet J Rare Dis 2011;1:6–70.
148. Kraemer KH, Lee MM, Scotto J. Xeroderma pigmentosum. Cutaneous,ocular, and neurologic abnormalities in 830 published cases. ArchDermatol 1987;123:241–50.
149. Lai JP, Liu YC, Alimchandani M, Liu Q, Aung PP, Matsuda K, et al. Theinfluence of DNA repair on neurological degeneration, cachexia, skincancer and internal neoplasms: autopsy report of four xeroderma pig-mentosum patients (XP-A, XP-C and XP-D). Acta Neuropathol Commun2013;1:4.
150. Kraemer KH, LeeMM, Andrews AD, LambertWC. The role of sunlight andDNA repair inmelanoma and nonmelanoma skin cancer. The xerodermapigmentosum paradigm. Arch Dermatol 1994;130:1018–21.
Cancer Epidemiol Biomarkers Prev; 25(1) January 2016 Cancer Epidemiology, Biomarkers & Prevention126
Meulepas et al.
RETR
ACTE
D Ju
ly 1,
2016
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/
Retraction
Retraction: Confounding of the Associationbetween Radiation Exposure from CT Scansand Risk of Leukemia and Brain Tumors byCancer Susceptibility Syndromes
The article titled, "Confounding of the association between radiation exposure fromCT scans and risk of leukemia and brain tumors by cancer susceptibility syndromes,"which was published in the January 2016 issue of Cancer Epidemiology, Biomarkers &Prevention (1), is being retracted at the request of the authors.
The authors recently reported analytical errors that drastically change the publishedarticle conclusions. The error is explained in detail below.
The authors calculated, separately for a series of cancer susceptibility syndromes(CSS), the bias of radiation risks for leukemia and brain tumors from computedtomography (CT) scanning in children due to confounding by CSS, based onAxelson's formula. Values of the factors in the formula were chosen based onliterature when available and based on assumptions otherwise. The erroroccurred in the calculation of bias for syndromes tuberous sclerosis complex(TSC) and von Hippel–Lindau (VHL) and brain tumor risk. More specifically,the error occurred in the calculation of the relative risk of brain tumors amongpatients with TSC or VHL disease compared with the general population (RR_CDin the formula). Because of the error, the estimates for these two relative riskswere too high, 2,500 and 28,000, respectively, when they should have been 125and 142. Because of the large (and incorrect) relative risks used, bias of TSC andVHL disease was substantial for several scenarios. As a result, the authorsconcluded that TSC is a potentially important confounder for brain tumorrisks in CT studies. The authors originally concluded that, "associations withleukemia reported in previous studies are unlikely to be substantially con-founded by unmeasured CSS, whereas brain tumor risks might havebeen overestimated due to confounding by TSC" (1). In light of the analyticalerror, the reassessment indicates that associations with leukemia and braintumors reported in previous studies are unlikely to be substantially confoundedby unmeasured CSS.
The authors regret the error and seek, in good faith, to update the scientific record byissuing this retraction.
Reference1. Meulepas JM, Ronckers CM,Merks J, WeijermanME, Lubin JH, HauptmannM. Confounding of the
association between radiation exposure from CT scans and risk of leukemia and brain tumors bycancer susceptibility syndromes. Cancer Epidemiol Biomarkers Prev 2016;25:114–26.
Published online July 1, 2016.doi: 10.1158/1055-9965.EPI-16-0300�2016 American Association for Cancer Research.
CancerEpidemiology,Biomarkers& Prevention
Cancer Epidemiol Biomarkers Prev; 25(7) July 20161192
2016;25:114-126. Published OnlineFirst November 23, 2015.Cancer Epidemiol Biomarkers Prev Johanna M. Meulepas, Cécile M. Ronckers, Johannes Merks, et al. Susceptibility SyndromesCT Scans and Risk of Leukemia and Brain Tumors by Cancer Confounding of the Association between Radiation Exposure from
Updated version
10.1158/1055-9965.EPI-15-0636doi:
Access the most recent version of this article at:
Material
Supplementary
http://cebp.aacrjournals.org/content/suppl/2015/11/21/1055-9965.EPI-15-0636.DC1
Access the most recent supplemental material at:
Cited articles
http://cebp.aacrjournals.org/content/25/1/114.full#ref-list-1
This article cites 139 articles, 25 of which you can access for free at:
Citing articles
http://cebp.aacrjournals.org/content/25/1/114.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/25/1/114To request permission to re-use all or part of this article, use this link
on June 28, 2021. © 2016 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2015; DOI: 10.1158/1055-9965.EPI-15-0636
http://cebp.aacrjournals.org/lookup/doi/10.1158/1055-9965.EPI-15-0636http://cebp.aacrjournals.org/content/suppl/2015/11/21/1055-9965.EPI-15-0636.DC1http://cebp.aacrjournals.org/content/25/1/114.full#ref-list-1http://cebp.aacrjournals.org/content/25/1/114.full#related-urlshttp://cebp.aacrjournals.org/cgi/alertsmailto:[email protected]://cebp.aacrjournals.org/content/25/1/114http://cebp.aacrjournals.org/
/ColorImageDict > /JPEG2000ColorACSImageDict > /JPEG2000ColorImageDict > /AntiAliasGrayImages false /CropGrayImages false /GrayImageMinResolution 200 /GrayImageMinResolutionPolicy /Warning /DownsampleGrayImages false /GrayImageDownsampleType /None /GrayImageResolution 300 /GrayImageDepth 8 /GrayImageMinDownsampleDepth 2 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /FlateEncode /AutoFilterGrayImages false /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict > /GrayImageDict > /JPEG2000GrayACSImageDict > /JPEG2000GrayImageDict > /AntiAliasMonoImages false /CropMonoImages false /MonoImageMinResolution 600 /MonoImageMinResolutionPolicy /Warning /DownsampleMonoImages false /MonoImageDownsampleType /None /MonoImageResolution 1200 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None ] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (None) /PDFXOutputConditionIdentifier () /PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped /False
/CreateJDFFile false /Description > /Namespace [ (Adobe) (Common) (1.0) ] /OtherNamespaces [ > /FormElements false /GenerateStructure false /IncludeBookmarks false /IncludeHyperlinks false /IncludeInteractive false /IncludeLayers false /IncludeProfiles false /MarksOffset 18 /MarksWeight 0.250000 /MultimediaHandling /UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /NA /PageMarksFile /RomanDefault /PreserveEditing true /UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling /LeaveUntagged /UseDocumentBleed false >> > ]>> setdistillerparams> setpagedevice