Embed Size (px)
Citation preview
CAN’T MISS CASES IN NEUROLOGY October 24, 2019 – Bernard S. Chang, M.D., M.M.Sc. Primary Care Internal Medicine course
DISCLOSURES
None
2 Can’t Miss Cases in Neurology | October 2019
CASES
1 Episodic spells
3 Can’t Miss Cases in Neurology | October 2019
Case 1: Episodic Spells
A 33-year-old woman has “spells” involving a feeling of déjà vu followed by a loss of awareness. During this time she stares and repetitively smacks her lips for 30 seconds, followed by a few minutes of confusion. These have occurred about once a month for the past few months.
Which of the following is an appropriate next step?
A. Watchful waiting
B. Order a brain MRI and EEG
C. Begin ethosuximide therapy
D. Begin valproic acid therapy
E. Restrict driving to daytime only
Can’t Miss Cases in Neurology | October 2019 4
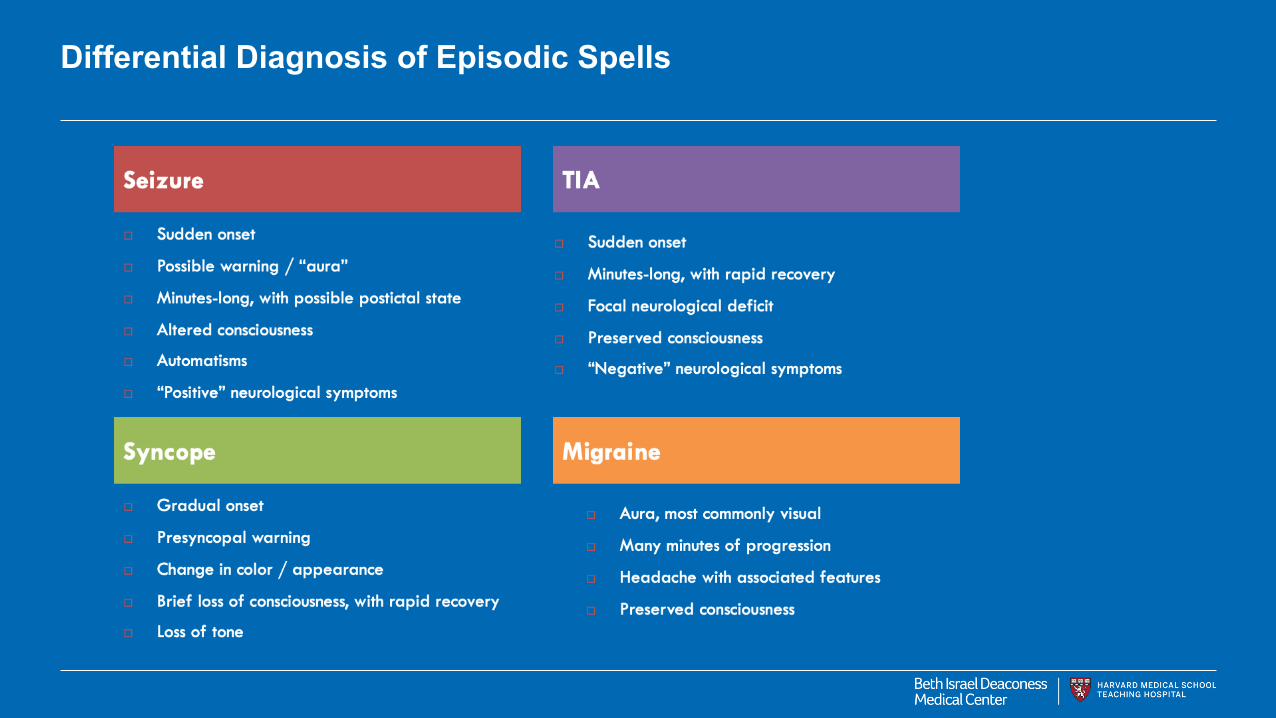
Differential Diagnosis of Episodic Spells
Episodic Spells: Focal seizures with impaired awareness
Type of seizure that can be characterized by unresponsiveness, automatisms, and postictal confusion Originate in a localized seizure focus within the brain Déjà vu and oral automatisms are suggestive of mesial temporal lobe onset
6 Can’t Miss Cases in Neurology | October 2019

Episodic Spells: Evaluation for Possible Seizures
EEG → normal EEG does not rule out seizure Laboratory → CBC, electrolyte and glucose levels, toxicology screen Brain MRI → head CT if MRI contraindicated • Mesial temporal lobe sclerosis not well visualized on
CT CSF examination → if fever, altered mental status, severe headache
7 Can’t Miss Cases in Neurology | October 2019

Diagnostic Tests in the Evaluation of Possible Seizures
Can’t Miss Cases in Neurology | October 2019

Seizure Therapy General Rules
Risk of recurrence • After first seizure → 25% to 40% • After second seizure → 80% to 90% • Risk of recurrence ↑ with abnormal EEG, abnormal MRI,
or history of potential cause (head trauma, stroke) Chronic therapy typically started after second unprovoked seizure
9 Can’t Miss Cases in Neurology | October 2019
Seizure Therapy General Rules
Single-agent therapy • ↑ Dosage until seizures are controlled or side
effects occur • If unsuccessful, initiate a second drug as
adjunctive therapy and then try tapering first agent Drug levels
− Let clinical response guide therapy − Drug levels mostly help assess possible drug
toxicity
10 Can’t Miss Cases in Neurology | October 2019
Case 1: Episodic Spells
A 33-year-old woman has “spells” involving a feeling of déjà vu followed by a loss of awareness. During this time she stares and repetitively smacks her lips for 30 seconds, followed by a few minutes of confusion. These have occurred about once a month for the past few months.
Which of the following is an appropriate next step?
A. Watchful waiting
B. Order a brain MRI and EEG
C. Begin ethosuximide therapy
D. Begin valproic acid therapy
E. Restrict driving to daytime only
Can’t Miss Cases in Neurology | October 2019 11

CASES
1 Episodic spells 2 Facial asymmetry
12 Can’t Miss Cases in Neurology | October 2019
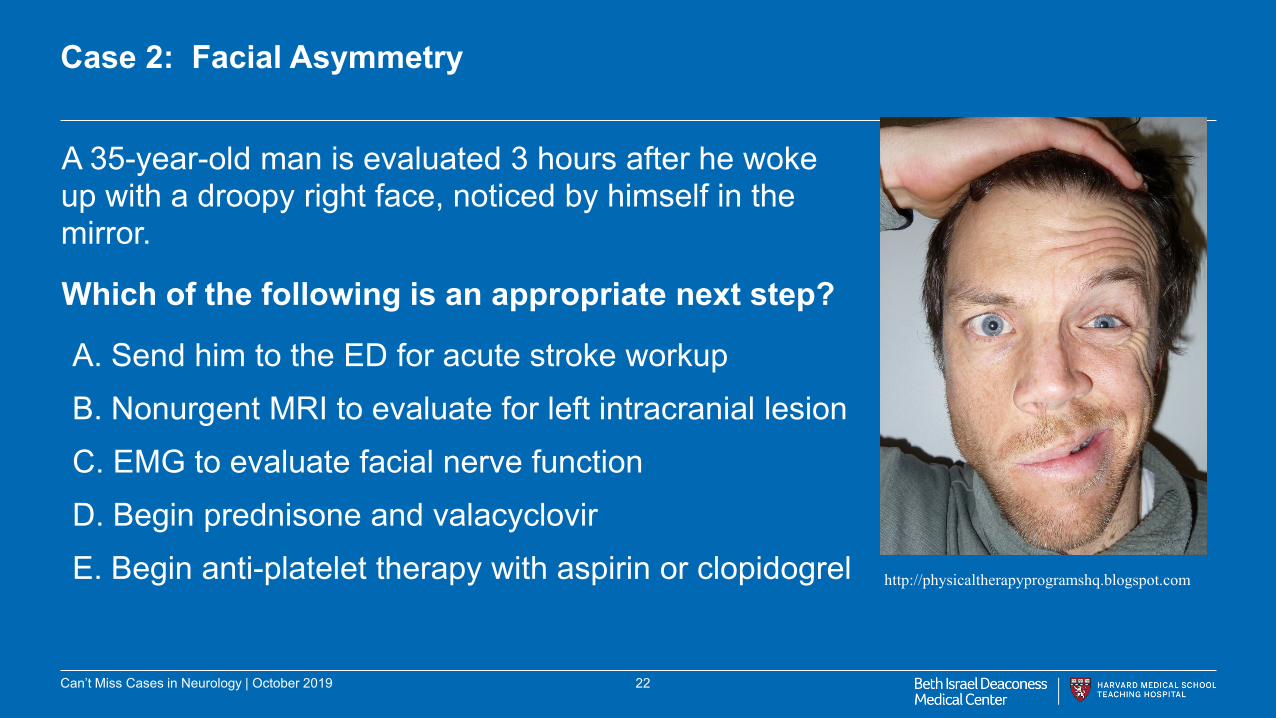
Case 2: Facial Asymmetry
A 35-year-old man is evaluated 3 hours after he woke up with a droopy right face, noticed by himself in the mirror.
Which of the following is an appropriate next step?
A. Send him to the ED for acute stroke workup B. Nonurgent MRI to evaluate for left intracranial lesion C. EMG to evaluate facial nerve function D. Begin prednisone and valacyclovir E. Begin anti-platelet therapy with aspirin or clopidogrel
13
http://physicaltherapyprogramshq.blogspot.com
Can’t Miss Cases in Neurology | October 2019

Neuroanatomy of Facial Asymmetry
14 Can’t Miss Cases in Neurology | October 2019
Berkowitz, Clinical Neurology and Neuroanatomy: A Localization-Based Approach, 2017

Acute Ischemic Stroke Evaluation
TIA associated with ↑ risk of subsequent stroke within 48 h Hospitalize all acute TIA/stroke patients for urgent evaluation −Emergent CT scan for stroke or TIA → rule out intracranial
hemorrhage −Baseline PT and aPTT −Cardiac monitoring (evaluate for atrial fibrillation) −Echocardiography (if cardiac etiology suspected) −Carotid artery ultrasonography, head/neck MRA or CTA within
2-3 days
15 Can’t Miss Cases in Neurology | October 2019

Ischemic Stroke Acute Therapy
Intubation and mechanical ventilation if ↓ level of consciousness
Recombinant tissue plasminogen activator (rt-PA) → ischemic stroke within 3 h of onset −If unknown onset → 3 hours of the last time the
patient was seen to be well
−rt-PA may be administered up to 4.5 h if no high risk factors for hemorrhage
−Age >80 y, severe (large territory) stroke, DM with previous stroke, and any anticoagulant use
16 Can’t Miss Cases in Neurology | October 2019
Secondary Prophylaxis for Ischemic Stroke
Antiplatelets • Aspirin plus dipyridamole, clopidogrel Anticoagulation • Atrial fibrillation, left atrial thrombus, dilated
cardiomyopathy Carotid endarterectomy • Ipsilateral stenosis >70% if patient likely to live 5 years Statins • All patients regardless of cholesterol level Long-term control of hypertension • <140/90 mm Hg after acute event 17 Can’t Miss Cases in Neurology | October 2019
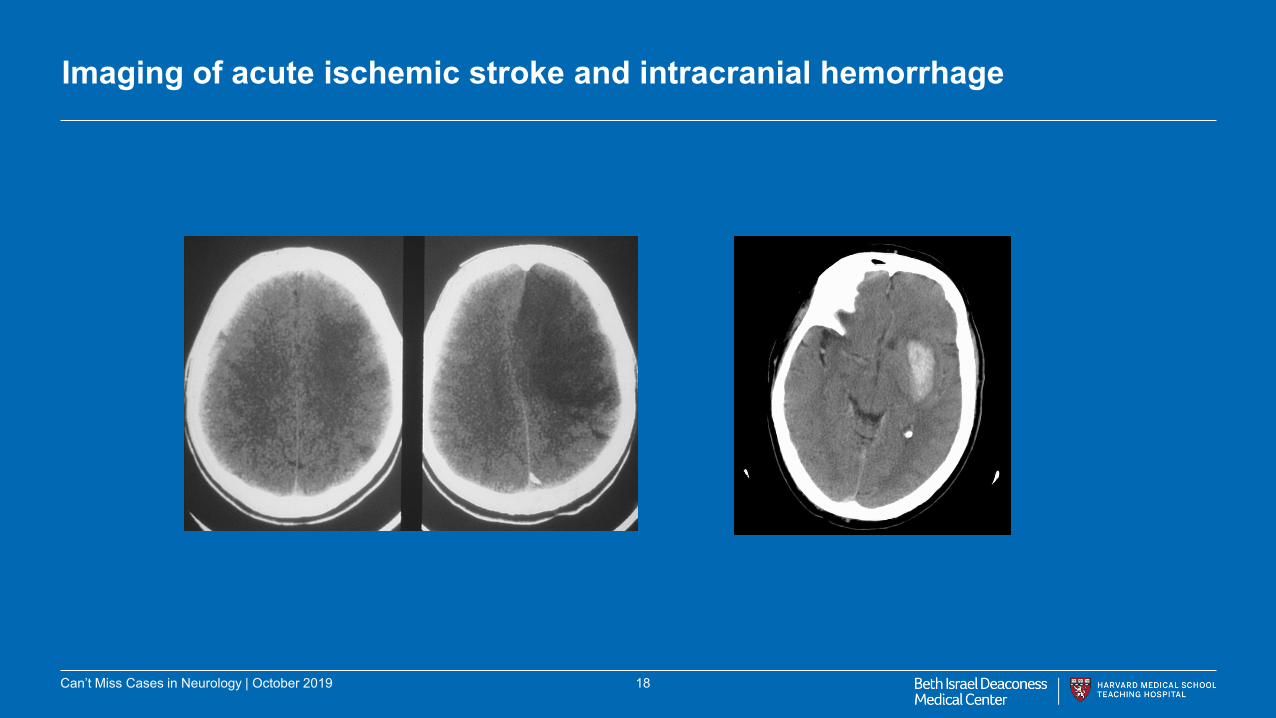
Imaging of acute ischemic stroke and intracranial hemorrhage
18 Can’t Miss Cases in Neurology | October 2019
Intracranial Hemorrhage
Most common risk factor is hypertension
Presentation − Often similar to ischemic stroke
− May not be able to be distinguished clinically
Diagnosis • Study of choice → CT without contrast
• Cerebral angiography for patients <45 years old and cocaine use
− ↑ Risk of vascular abnormalities
19 Can’t Miss Cases in Neurology | October 2019
Therapy for intracranial hemorrhage
• Reverse anticoagulation
− Use appropriate reversal agent → IV vitamin K, fresh frozen plasma, or prothrombin complex concentrates
• ↓ Intracranial pressure
− Mannitol, barbiturate coma, hyperventilation
• Maintain SBP 140-160 mm Hg (or MAP 70-130 mm Hg)
− Labetalol or nicardipine
• Ventricular drainage or decompression for increased ICP
• Surgical evacuation if needed
20 Can’t Miss Cases in Neurology | October 2019
Bell’s Palsy
Unexplained episode of facial muscle weakness on one side, localizable to the facial (VII) nerve Unknown cause, many associations, likely related to inflammation Acute onset, worse over a few days, better starting within two weeks but could take months Steroids, antiviral agents, supportive therapy for face and eye
21 Can’t Miss Cases in Neurology | October 2019
Case 2: Facial Asymmetry
A 35-year-old man is evaluated 3 hours after he woke up with a droopy right face, noticed by himself in the mirror.
Which of the following is an appropriate next step?
A. Send him to the ED for acute stroke workup B. Nonurgent MRI to evaluate for left intracranial lesion C. EMG to evaluate facial nerve function D. Begin prednisone and valacyclovir E. Begin anti-platelet therapy with aspirin or clopidogrel
22
http://physicaltherapyprogramshq.blogspot.com
Can’t Miss Cases in Neurology | October 2019
CASES
1 Episodic spells 2 Facial asymmetry 3 Rapidly progressive weakness
23 Can’t Miss Cases in Neurology | October 2019
Case 3: Rapidly Progressive Weakness
A 43-year-old woman has noticed progressive leg weakness over the past week. First she began having trouble getting out of automobiles, standing up from a chair, and climbing or descending stairs. The weakness progressed and by two days ago she began having difficulty raising her arms to wash her hair and turning a key in the lock of her front door. She has also noted bilateral upper and lower extremity numbness during this time period.
Which of the following is the most likely diagnosis?
A. A disorder of peripheral nerves
B. A disorder of muscles
C. A disorder of motor neurons
D. A disorder of the cerebral hemispheres
E. A disorder of the spinal cord
24 Can’t Miss Cases in Neurology | October 2019
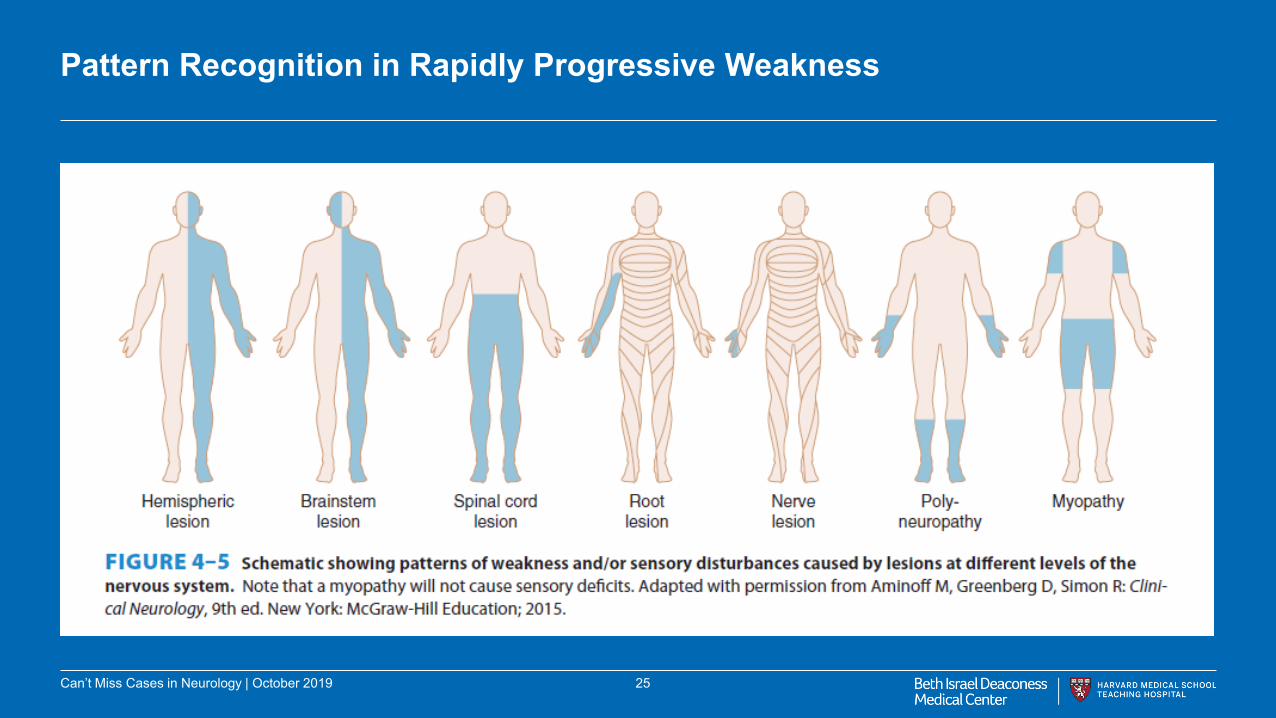
Pattern Recognition in Rapidly Progressive Weakness
25 Can’t Miss Cases in Neurology | October 2019
Peripheral Neuropathy Overview
• Typical symptoms → pain, paresthesias, weakness, or autonomic dysfunction • Small fiber axonal neuropathy → pain and paresthesias of hands and feet
without weakness • Mononeuropathies → isolated disorders of a single peripheral nerve • Mononeuropathy multiplex → multiple noncontiguous peripheral nerves
− Systemic disease (vasculitis, sarcoidosis)
• Polyneuropathy → diffuse, generalized, usually symmetric peripheral neuropathy − Systemic disease (diabetes), toxin (alcohol), medication
26 Can’t Miss Cases in Neurology | October 2019
Peripheral Neuropathy Syndromes
Diabetic amyotrophy • Severe leg pain, proximal weakness, atrophy Guillain-Barré syndrome • Acute ascending, areflexic paralysis, paresthesias • Therapy → plasma exchange, IV immune globulin Chronic inflammatory demyelinating polyneuropathy • Chronic progressive motor and sensory neuropathy • Therapy → prednisone, plasma exchange, IV immune
globulin
27 Can’t Miss Cases in Neurology | October 2019
Case 3: Rapidly Progressive Weakness
A 43-year-old woman has noticed progressive leg weakness over the past week. First she began having trouble getting out of automobiles, standing up from a chair, and climbing or descending stairs. The weakness progressed and by two days ago she began having difficulty raising her arms to wash her hair and turning a key in the lock of her front door. She has also noted bilateral upper and lower extremity numbness during this time period.
Which of the following is the most likely diagnosis?
A. A disorder of peripheral nerves
B. A disorder of muscles
C. A disorder of motor neurons
D. A disorder of the cerebral hemispheres
E. A disorder of the spinal cord
28 Can’t Miss Cases in Neurology | October 2019
CASES
1 Episodic spells 2 Facial asymmetry 3 Rapidly progressive weakness 4 Memory loss
29 Can’t Miss Cases in Neurology | October 2019

Case 4: Memory Loss
An 81-year-old man presents with cognitive decline over several years, according to his family. (He himself believes they are overreacting.) He has been repeating himself frequently and loses things around the house. He was formerly an active volunteer and golfer but can no longer participate in those activities. Once he got lost while driving a familiar route home.
Which of the following might be an appropriate treatment?
A. Carbidopa-levodopa
B. Gabapentin C. Riluzole D. Tetrabenazine E. Memantine 30 Can’t Miss Cases in Neurology | October 2019

31 Can’t Miss Cases in Neurology | October 2019
Evaluation for Memory Loss
Neuroimaging to look for: mass, subdural hematoma, stroke(s), pattern of atrophy suggestive of dementia Laboratory evaluation to look for potentially treatable causes of cognitive decline: Vitamin B12, TSH, RPR, HIV Formal neuropsychological testing to evaluate for particular pattern of cognitive deficits Other types of evaluation to consider: sleep study for sleep apnea, evaluation for depression (“pseudodementia”)
32 Can’t Miss Cases in Neurology | October 2019

Statistics on Alzheimer’s, the most common form of dementia • Approximately 5 million individuals over age 65 in the US have Alzheimer’s (1
in 9 individuals > age 65). • Average lifespan after diagnosis of Alzheimer’s is 4-8 years (but can be up to
20 depending on how early diagnosis is made and social support structures) • Mini-mental state exam (MMSE) in Alzheimer’s score drops by 2-4 points per
year • At time of advanced dementia (inability to recognize family, limited speech,
total dependence), median survival ~1.3 years (death often due to infections and eating problems)
33 Can’t Miss Cases in Neurology | October 2019
Treatment for Alzheimer’s Dementia
Cholinesterase inhibitors are modestly effective: • donepezil • galantamine • rivastigmine
Memantine (NMDA receptor antagonist) can be used for moderate AD
34 Can’t Miss Cases in Neurology | October 2019

66-year-old woman brought in by her family for progressive changes in her personality over 5 years. Had become increasingly short-tempered, irritable, and disheveled. She would also complain of headaches upon awakening sometimes.
35
The Need for Full Evaluation of Cognitive Changes
Can’t Miss Cases in Neurology | October 2019

Case 4: Memory Loss
An 81-year-old man presents with cognitive decline over several years, according to his family. (He himself believes they are overreacting.) He has been repeating himself frequently and loses things around the house. He was formerly an active volunteer and golfer but can no longer participate in those activities. Once he got lost while driving a familiar route home.
Which of the following might be an appropriate treatment?
A. Carbidopa-levodopa
B. Gabapentin C. Riluzole D. Tetrabenazine E. Memantine 36 Can’t Miss Cases in Neurology | October 2019
KEY POINTS
37 Can’t Miss Cases in Neurology | October 2019
There are two pieces of information that contribute to making a neurological diagnosis: 1) Identifying the location of the problem in the nervous system
From the pattern of signs and symptoms From knowledge of very basic anatomy 2) Understanding the time course and progression of the illness

NEXT BEST STEPS
38 Can’t Miss Cases in Neurology | October 2019
Always keep in mind for any neurological complaint: 1) What part of the nervous system might be involved?
Brain, spinal cord, peripheral nerves, muscles, etc.
2) What kind of disease process might be at work? Is it a process that can be imaged, or subject to neurophysiological testing, or further evaluated clinically?




















![Managing Container-Based Apps: What You Can’t Miss [Webinar]](https://img.pdfslide.us/doc/110x75/58ecd7861a28abcc7d8b4755/managing-container-based-apps-what-you-cant-miss-webinar.jpg)







