Embed Size (px)
Citation preview
Integration of Information - Sharing a Train of Thought
Canadian Hospital Pharmacy Leadership ConferenceJune 6, 2015
HIMSS Analytics Adoption Model Integrated Pharmacy, eMAR and CPOE
Systems Regional Data Repositories for Drug
Information Medication Reconciliation Notes Patient Access to Information
Session Objectives
HIMSS Electronic Medical Record Adoption Model (EMRAM)
Healthcare Information and Management Systems Society – 52,000 members
Global, cause-based, not-for-profit organization focused on better health through IT
Leads efforts to optimize health engagements and care outcomes using IT
Vision: ◦ Better health through information technology
Mission:◦ Globally, lead endeavors optimizing health engagements
and care outcomes through information technology
ABOUT HIMSS
Wholly-owned, not-for-profit subsidiary of HIMSS
Collects and analyzes healthcare information: ◦ IT adoption and environments◦ IT department composition and costs◦ healthcare trends◦ purchase-related decisions past and near term future
Gather data for:◦ Every hospital in the US and Canada◦ Europe, Middle East, Asia on a country sample basis
ABOUT HIMSS ANALYTICS
HIMSS Analytics’ EMR Adoption Model (EMRAM) tracks the adoption of ℠EMR applications within hospitals and health systems
First created in 2005 Institutions work to complete the 8 stages Each level of maturity is a score derived from
a comprehensive survey of the hospital’s IT environment
WHAT IS AN EMR ADOPTION MODEL ?
Progressively sophisticated steps track the accessibility of information within an EMR ◦ Ensures critical clinical information and Clinical Decision
Support guidance are available to the clinician at the point of care
Gated model - all technologies in a stage must be accomplished before hospital can move up
Goal of reaching Stage 7 - an environment where paper charts are no longer used
EMR ADOPTION MODEL EXPLAINED
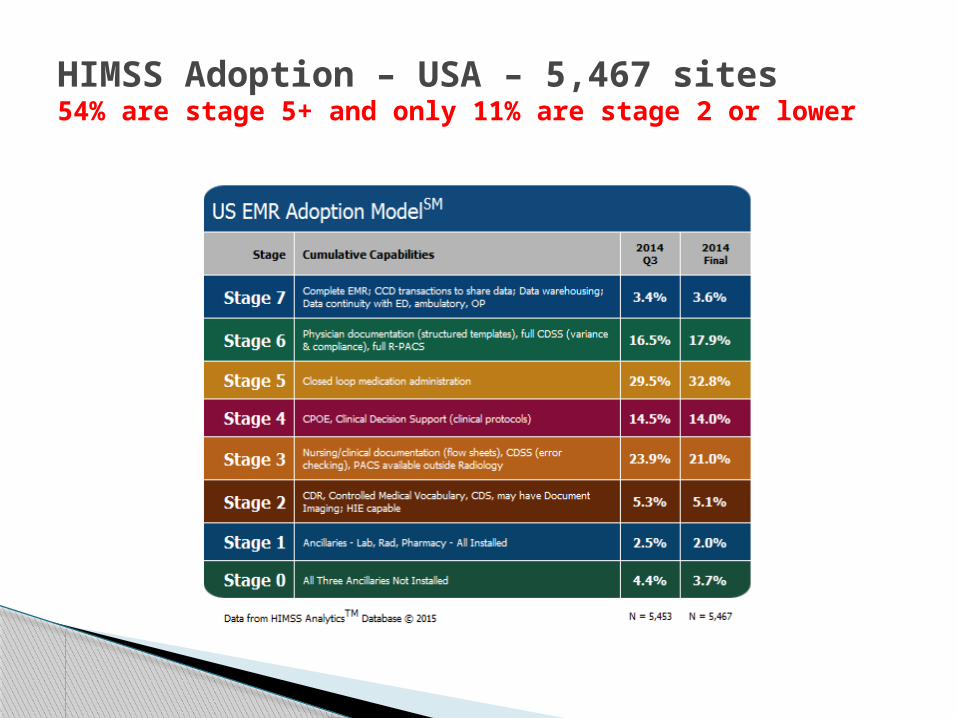
HIMSS Adoption – USA – 5,467 sites54% are stage 5+ and only 11% are stage 2 or lower
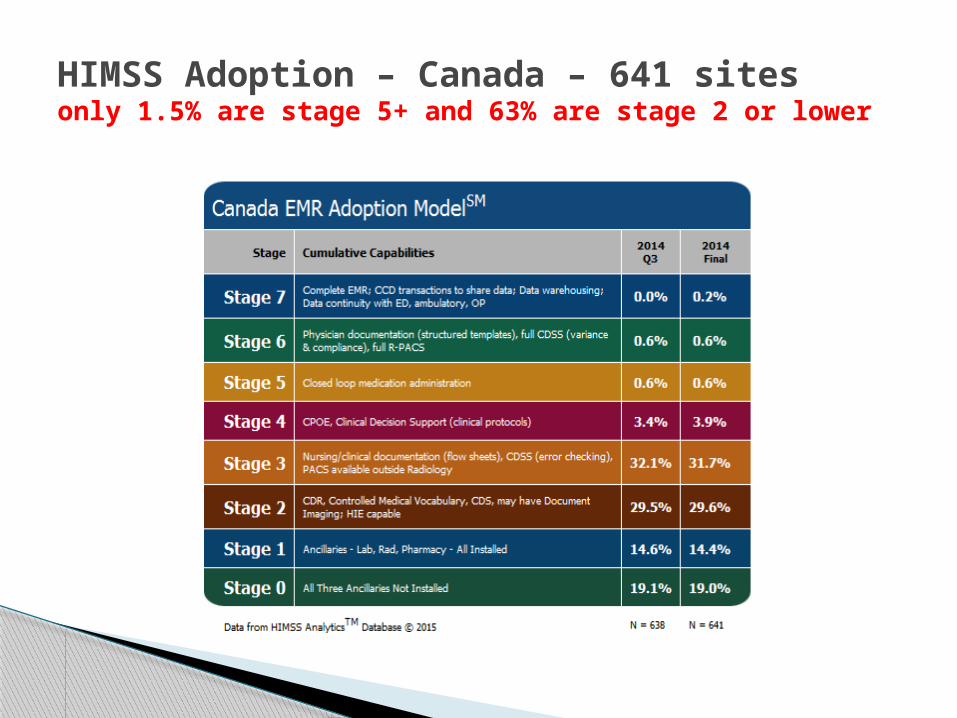
HIMSS Adoption – Canada – 641 sitesonly 1.5% are stage 5+ and 63% are stage 2 or lower
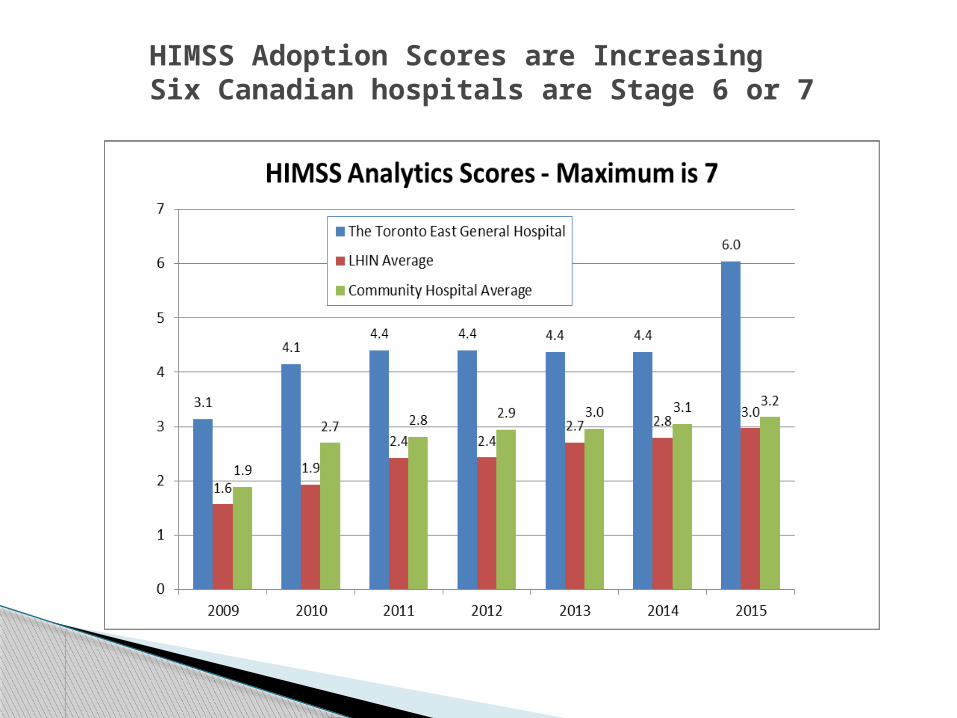
HIMSS Adoption Scores are Increasing Six Canadian hospitals are Stage 6 or 7
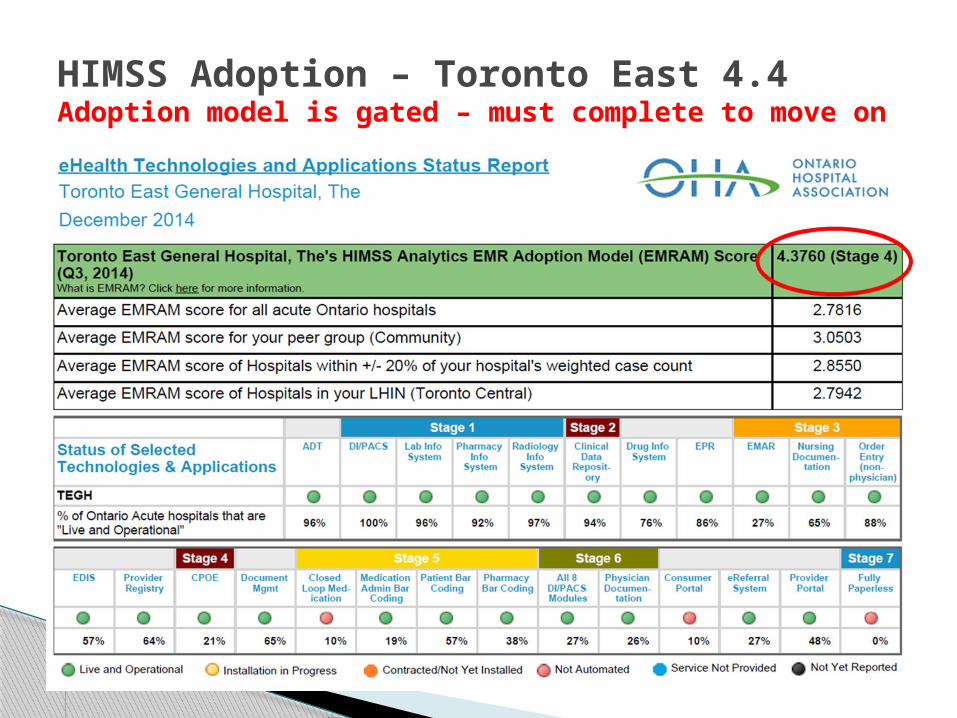
HIMSS Adoption – Toronto East 4.4Adoption model is gated – must complete to move on
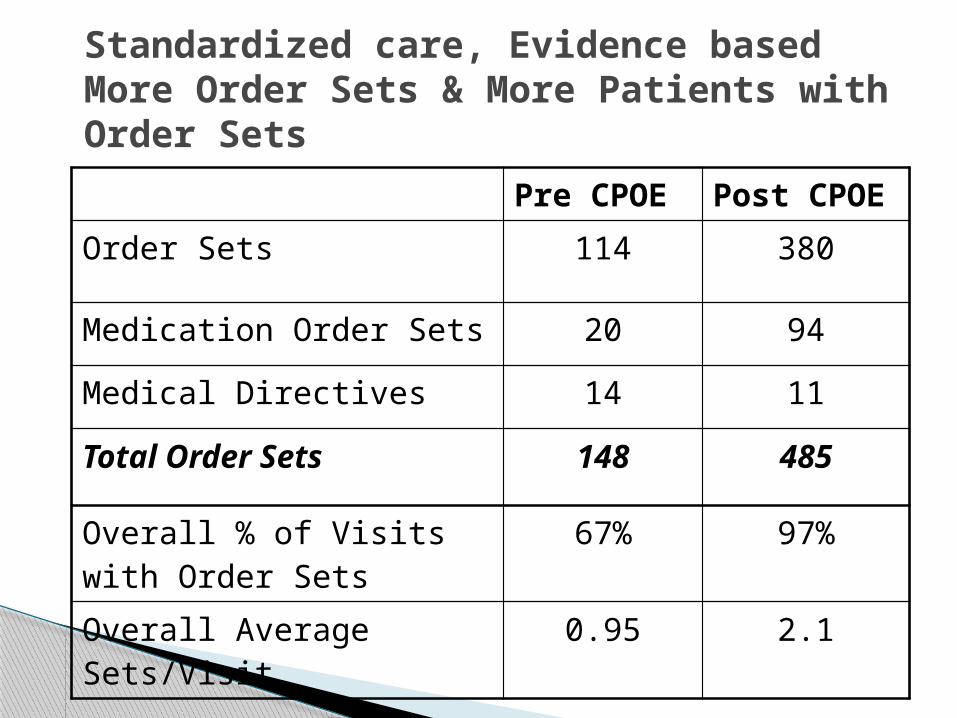
Standardized care, Evidence basedMore Order Sets & More Patients with Order Sets
Pre CPOE Post CPOE
Order Sets 114 380
Medication Order Sets 20 94
Medical Directives 14 11
Total Order Sets 148 485
Overall % of Visits with Order Sets
67% 97%
Overall Average Sets/Visit 0.95 2.1
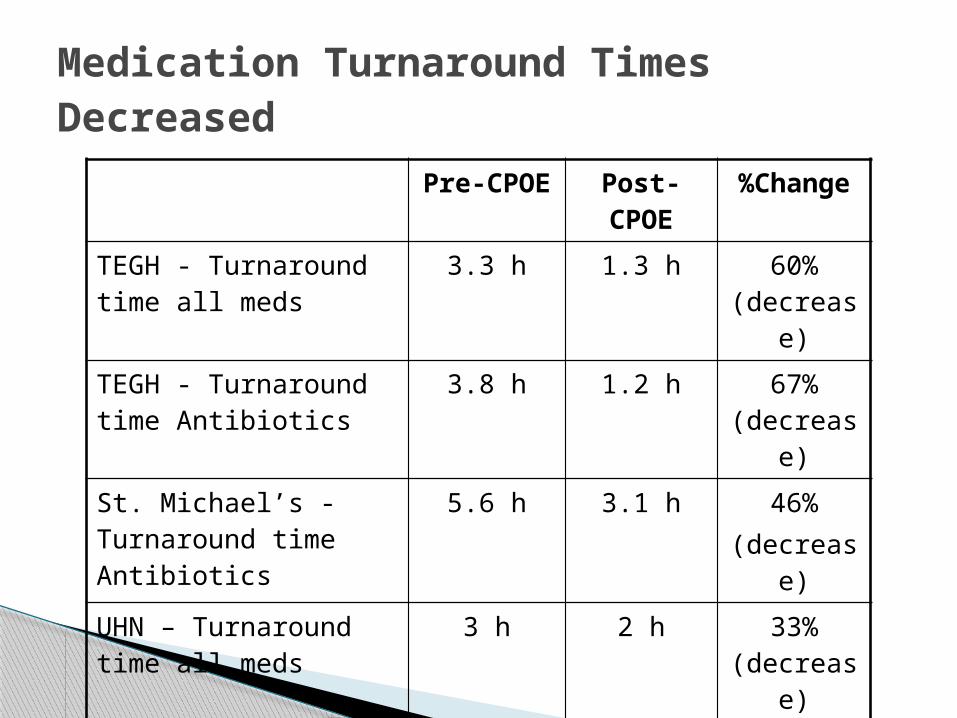
Medication Turnaround Times Decreased
Pre-CPOE Post-CPOE
%Change
TEGH - Turnaround time all meds
3.3 h 1.3 h 60% (decrease)
TEGH - Turnaround time Antibiotics
3.8 h 1.2 h 67% (decrease)
St. Michael’s - Turnaround time Antibiotics
5.6 h 3.1 h 46%(decrease)
UHN – Turnaround time all meds
3 h 2 h 33% (decrease)
UHN – Now dose turnaround time
1.8 h 1.4 h 23% (decrease)
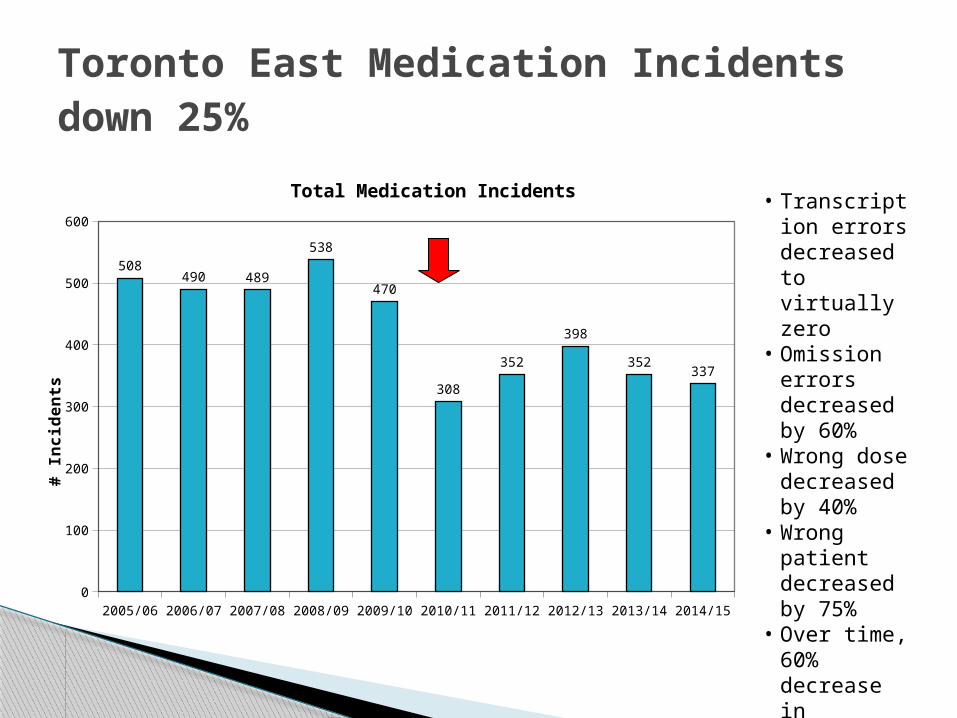
Toronto East Medication Incidents down 25%
• Transcription errors decreased to virtually zero
• Omission errors decreased by 60%
• Wrong dose decreased by 40%
• Wrong patient decreased by 75%
• Over time, 60% decrease in Moderate Severity incidents
2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14 2014/150
100
200
300
400
500
600
508490 489
538
470
308
352
398
352337
Total Medication Incidents
# In
cid
en
ts
Integrated Pharmacy, eMAR and CPOE Systems
200 Hospitals have ascended to the top of HIMSS EMRAM (Stage 7)
Secret to success – Single Clinical Data Repository◦ Enterprise-wide with core clinical system
152 Epic 41 Cerner 5 Meditech 1 Allscripts
◦ Best of breed hospitals are not achieving Stage 7 Clinical Decision support hard to achieve
Healthcare IT News April 2015
Software to support hospital’s core business is from a core vendor
Single source of truth without interfaces Single vendor solution for Pharmacy,
CPOE and eMAR◦Medication reconciliation software is integrated
with CPOE and Pharmacy systems◦Tracking Allergies in a single database◦Integration with Smart IV pumps
Core Clinical Systems
“Dissent and foot-dragging can’t be an option. It’s critical to embrace these enterprise-wide projects with the attitude that “there is no alternative”…And we’re going to use this as a clinical transformation and not an IT project.”
John Hoyt HIMSS Analytics Need advanced analytics for Stage 7 – hard to
achieve with Best of Breed Difficult technically Data quality issues with disparate systems
Healthcare IT News April 2015
Reasons for not using alert functionality in Pharmacy Information Systems (PIS):◦ Use of a CPOE system for this functionality◦ Lack of a database in PIS to drive functionality◦ Lack of integration with other modules, such as Labs for
renal function◦ Lack of patient demographic information such as patient
weight, age, etc. Consistent, comprehensive decision support for all
clinicians is only possible with core clinical systems
2007/08 Hospital Pharmacy in Canada Report Technology section
Regional Data Repositories for Drug Information
Defined in many segments of the IT world Allow data from disparate systems to populate a
single repository Interface standards for Healthcare, real time
HL7 – various versions IHE for Document sharing
Terminology standards for inter-operability Snomed CT – clinical terminology UCUM – unified codes for unit of measure HCDPD – Health Canada Drug Product Database GTIN – Global Trade Item Number
Technology Standards
Purpose is to build a patient medication profile across the continuum of care
Support the following business functions ePrescribing Dispensing & Managing Rx status Adding OTC or samples information Drug queries Patient Medication queries Contra-indications e.g. drug-drug, drug-allergy, dose checks
No standards for Medication Reconciliation process at this time
Canada Health Infoway (CHI) Drug Information System (DIS) Standard
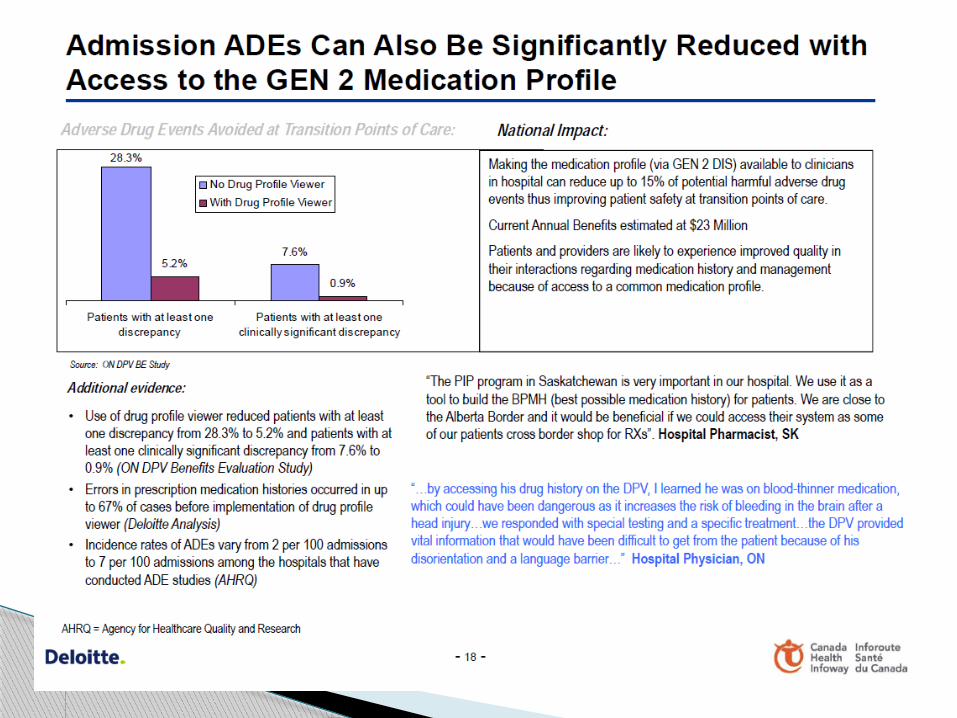
Quality Reduced ADEs Decreased medication abuse Increased medication compliance Increased patient and provider satisfaction Increased timely access to information
Productivity Enhanced provider communications Increased provider efficiency Enhanced drug cost management
Anticipated DIS Benefits - CHI
Very slow progress compared to Labs, XRay Majority of in-use repositories obtain data from Rx
dispensing in retail pharmacy only◦ PEI exception and includes MD samples, hospital Rx,
OTC/herbal◦ Western Provinces 100% for retail Rx◦ Rest of Canada is 0%-80% of Rx
Access/adoption is partial◦ Western jurisdictions is mainly pharmacists and ER◦ Very little access/adoption by Community MDs◦ Hospital adoption rates vary from 50% for ER and low of
30% for Inpatients (CHI)
Canadian DIS Experience
©Canada Health Infoway 2015 26
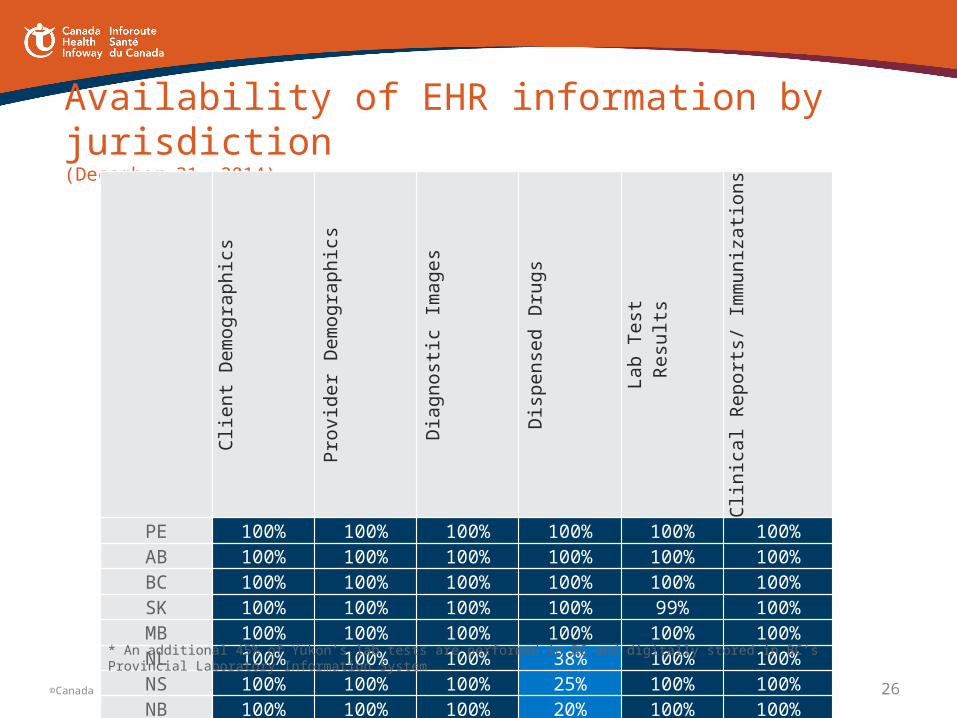
Availability of EHR information by jurisdiction(December 31, 2014)
Client Demograp
hics
Provider Demograp
hicsDiagnostic
ImagesDispensed
DrugsLab Test Results
Clinical Reports/ Immunizations
PE 100% 100% 100% 100% 100% 100%AB 100% 100% 100% 100% 100% 100%BC 100% 100% 100% 100% 100% 100%SK 100% 100% 100% 100% 99% 100%MB 100% 100% 100% 100% 100% 100%NL 100% 100% 100% 38% 100% 100%NS 100% 100% 100% 25% 100% 100%NB 100% 100% 100% 20% 100% 100%NT 100% 100% 100% 0% 100% 100%QC 100% 100% 100% 80% 77% 95%ON 100% 100% 100% 27% 75% 100%NU 100% 100% 80% 80% 90% 80%YT 0% 0% 100% 0% 50%* 100%
* An additional 45% of Yukon’s lab tests are performed in BC and digitally stored in BC’s Provincial Laboratory Information System
Typically would be only on discharge Hospital EMRs with CPOE already have ePrescribing
function with printed / signed Rx Legibility benefit already realized
Technically more difficult since you need trigger events
Theoretically could be medication reconciliation at discharge if performed 100% of the time [7x24]
All clinicians have to use the same tool/process Need to consider Data Quality and Single Source of
Truth (Core systems) Likely one of the last items in jurisdictional EPRs
Drug Information from Hospitals
Medication Reconciliation Notes
Accreditation Canada◦ Medication reconciliation is a required organizational
practice Need to support the reconciliation task with
Clinical Documentation Describes medication-related decisions to start, stop, hold
therapy Complementary to a drug profile Needs to be electronic to share with regional
electronic patient record repositories
Purpose of Med Rec Notes
“One Good Note”, CJHP 67(3) May/June 2014, p 250◦ Advocates for documenting more in the patient record
and less on monitoring forms◦ “If you’re going to spend the time performing a detailed
workup, why not share that information with your colleagues in the form of a concise and clearly written chart note?”
For continuity of care in the ideal world, on discharge, goes to:
Family Physician Pharmacy of Record
Performing a Task without Communication is not an Option
For Health Professionals, generally a single point of access in a Jurisdiction
Includes information such as: Visits/encounters, demographics Lab tests (hospital and community) Diagnostic test results and Images (hospital and community) Immunizations Allergies and Intolerances Medications Transcribed Reports / Discharge Summaries
Electronic Health Records
Relatively easy technical effort if there is a core clinical system since triggers are available
If have a shared Clinical Documentation system, the notes are available internally as well to the full care team (in a Core Clinical System)
Measurement of extent of medication reconciliation should also evaluate % of medication reconciliation notes
Medication Reconciliation Notes
Patient Access to Information
Medications I need to take What to keep taking New medications What to stop taking
How I might feel and what to do Changes to my routine Appointments I have to go to Where to go for more information Technically difficult to prepare if have a
Pharmacy system separate from core system
Standardized Discharge Summary - Content for Patients
Personal Health Records eg. Alberta Netcare, Sunnybrook MyChart, myUHN
Continuity of care record, particularly with chronic disease; can share with family, MDs
Information patients can enter How much you exercise, what you eat How you are feeling – symptom scales Medications including OTC and herbal medications Your health care team and emergency contact information
In Alberta some data downloaded to Portal Netcare electronic health record
Can include educational material
Patient Portals
Very appropriate to add to downloaded information in a Patient Portal
May want to consider standard email contact information for further questions
Language in notes needs to be appropriate for patient audience so it can serve a dual purpose◦ UHN has very well-written guidelines
Author will usually be clear in the report
Medication Reconciliation Notes

Setting a New Standard in Quality and Value40
Toronto East General Hospital, 825 Coxwell Avenue, Toronto, Ontario, M4C 3E7
Tel: (416) 461-8272 Fax: (416) 469-6106
www.tegh.on.ca
Pegi Rappaport
416-469-6580 Ext 6032
Level 1 – Labs, Rx and DI
Laboratory and Pharmacy, and Radiology Management Systems are all Live and Operational in the inpatient hospital and the laboratory system produces discrete data Cerner for Pharmacy, Radiology Soft (SCC) for Labs and Blood Bank CoPath for Pathology (shared service) Meditech for Microbiology (shared service) Agfa for PACS
Level 2 – Single Data Repository & ShareMajor ancillary clinical systems feed data to a clinical data repository (CDR) that provides physician access for retrieving and reviewing results. The CDR contains a controlled medical vocabulary between the interfaced systems, and the clinical decision support/rules engine (CDS) for rudimentary conflict checking. Information from document imaging systems may be linked to the CDR at this stage. The hospital is health information exchange (HIE) capable at this stage and can share whatever information it has in the CDR with other patient care stakeholders. Cerner Powerchart; exchange data with 8 external
systems, e.g. OLIS, PRO, eCHN, HRM, HDIRS, ENITS, EMPI, IAR
Can have disparate systems, but need a single CDR
Level 3 – Nursing Documentation
Nursing documentation (e.g. vital signs, flow sheets, nursing tasks/orders and electronic medication administration record (eMAR) are required; nursing notes, care plan charting, and are implemented and integrated with the CDR for at least one service in the hospital. The first level of clinical decision support is implemented to conduct error checking with order entry (i.e., drug/drug, drug/food, drug/lab conflict checking normally found in the pharmacy). Some level of medical image access from picture archive and communication systems (PACS) is available for access by physicians outside the Radiology department via the organization’s intranet. Cerner for CDR and Clinical Decision support with integrated
Multum; Agfa for PACS viewing internally and via VPN
Level 4 – CPOE (TEGH at this point for 5 years)
Computerized Practitioner Order Entry (CPOE) for use by any clinician authorized to create orders in your state(s) is added to the nursing and CDR environment along with the second level of clinical decision support capabilities related to evidence based medicine protocols. If one patient service area has implemented CPOE with physicians entering orders and completed the previous stages, then this stage has been achieved. Need % of total physician orders entered by physicians, such as 1-25% etc. Cerner Powerchart with 100% electronic orders for Day Surgery
and Inpatients◦ 57% orders entered by MDs directly◦ 4% by telephone/verbal◦ 17% from pre-authorized conditional and multi-phase orders◦ 10% from approved medical directives◦ 10% direct entry as per scope of practice (mainly pharmacists)
Level 5 – Closed Loop MedsThe closed loop medication administration environment is fully implemented. The eMAR and bar coding or other auto identification technology, such as radio frequency identification (RFID), are implemented and integrated with CPOE and pharmacy to maximize point of care patient safety processes for medication administration. You are satisfying the 5 rights of patient safety at the bedside and there is an override management process in place to review overrides that occur. Cerner Powerchart; One nursing unit – Mental Health (40 beds) 2015 A big change in processes for Pharmacy – Unit dose, bar code
labeling of all medications including paediatrics Stage 7 requires:
◦ 95% of patients and 95% of medications have closed loop process for medications (includes ER admitted patients)
◦ Closed loop required for Blood Products and Breast milk
Level 6 – MD Documentation
Physician Documentation- What percent of physicians use the physician documentation system? AND What percent of physician documentation in the inpatient setting (excluding ED) is captured from structured template physician documentation that generates discrete data and triggers an immediate electronic alert from the Clinical Decision Support application that produces clinical guidance real-time for the provider? NEED TO STATE THE RULE-GUIDANCE that is built into the application and if possible send a screen shot. Cerner Powerchart Powernotes, Clinical Notes for direct entry
◦ 43% of physicians use the system◦ 28% of the notes are structured documentation
Real time guidance example is Allergy documentation – back checking against the medication profile and BPMH
Level 7 – Other requirements Document resuscitation medications after the fact on eMAR Anaesthesia medications documented on eMAR Full Dose Range Checking for medications - adults and paediatrics Diagnostic Imaging discrete results, e.g. abnormal, malignant as separate
data fields ER MDs use structured documentation to produce their notes Cataract Surgery Order entry and MAR documentation ECT documentation - replace current check sheet Business Intelligence to support Quality Improvement for patient care Patient Portal Clinically relevant paper documentation must be scanned within 24 hours of
creation





![HOSPITAL PHARMACY PROCUREMENT AND SUPPLY …jknj.moh.gov.my/farmasi/garispanduan/[2009] Requirement for the... · 4. HOSPITAL PHARMACY PROCUREMENT AND SUPPLY (HOSPITAL PHARMACY STORE)](https://img.pdfslide.us/doc/110x75/5cc11a7d88c9936f648bcddf/hospital-pharmacy-procurement-and-supply-jknjmohgovmyfarmasigarispanduan2009.jpg)























