Embed Size (px)
Citation preview

Canadian Diabetes Association Clinical Practice Guidelines
Treatment of Hypertension
Chapter 25
Richard E. Gilbert, Doreen Rabi, Pierre LaRochelle, Lawrence A. Leiter, Charlotte Jones, Richard Ogilvie, Sheldon Tobe, Nadia Khan, Luc Poirier, Vincent Woo

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
ASSESS for hypertension (≥130/80 mmHg)
TREAT to target <130/80 mmHg
USE multiple antihypertensive medications if needed
to achieve target (often necessary)
USE initial combination therapy if systolic blood
pressure >20 mmHg above target or diastolic blood
pressure >10 mmHg above target
2013Hypertension Checklist

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
BP >130/80 mm Hg
Confirmed on a second occasion in either the office,
home or by appropriate ambulatory measurement.
Making the Diagnosis of Hypertension in Patients with Diabetes

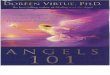
UKPDS Study Group. BMJ 1998; 317:703-13.
50
40
30
20
10
0
Years from randomization
Pat
ient
s w
ith e
vent
s (%
)
0 1 2 3 4 5 6 7 8 9
Less tight control (mean BP 154/87 mmHg)
Tight control (mean BP 144/82 mmHg)
Tight BP control:24% reduction of events(95% CI 8-38)
Tight BP control:24% reduction of events(95% CI 8-38)
Hypertension in Diabetes (UKPDS)
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Arch Intern Med 2005;165:1410-1419
Benefits of BP Lowering in DM
• Meta-analysis of 27 randomized trials showed
intense BP reduction (i.e., by 6/4.6 mmHg)
resulted in:– 36% reduction in stroke
– 27% reduction in total mortality
– 25% reduction in major cardiovascular events

Hansson et al. Lancet. 1998;351:1755.
P<0.005
MI,
str
oke,
CV
m
orta
lity/
1000
pt-
yDiabetes Subgroup
90 mm Hg (n=501) 85 mm Hg (n=501) 80 mm Hg (n=499)
Goal of therapy: target diastolic BP
24.4
18.8
11.9
30
25
20
15
10
5
0
Hansson et al. Lancet. 1998;351:1755.
HOT: BP Control Reduces CV Events
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
<130/80 mmHg
Multiple anti-hypertensive agents may be needed to achieve the desired target
Target Blood Pressure

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Threshold equal or over 130/80 mmHg and target below 130/80 mmHg
With Nephropathy* or CVD or CV
risk factors
*Urinary albumin to creatinine ratio >2.0 mg/mmol
Diabetes
WithoutThe above
Isolated Systolic Hypertension
Systolic-diastolicHypertension
A combination of 2 first line drugs may be considered as initial therapy if the blood pressure is >20 mmHg systolic or >10 mmHg diastolic
above target
Combinations of an ACEI with an ARB are specifically not
recommended in the absence of proteinuria
Pharmacotherapy for Hypertension in Patients with Diabetes
*Based on at least 2 of 3 measurementsCVD = Cardiovascular Disease; CV = Cardiovascular

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
THRESHOLD equal or over 130/80 mmHg and TARGET below 130/80 mmHg
If Creatinine over 150 µmol/L or creatinine clearance below 30 ml/min (0.5 ml/sec), a loop diuretic should be substituted for a thiazide diuretic if control of volume is desired
DIABETESwith
Nephropathy or CVD or
CV risk factors
ACE Inhibitoror ARB
IF ACEI and ARB are contraindicated or not tolerated, SUBSTITUTE• Long-acting CCB or• Thiazide diuretic
Addition of a Dihydropyridine CCB is preferable to HCTZ
3 - 4 drugs in combination may be needed
Monitor serum potassium and creatinine carefully in patients with CKD prescribed an ACEI or ARB
CCB = Calcium Channel Blocker; HCTZ = Hydrochlorothiazide; CKD = Chronic Kidney Disease
Pharmacotherapy of Hypertension with Nephropathy, CVD or CV Risk Factors

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
THRESHOLD equal or over 130/80 mmHg and TARGET below 130/80 mmHg
DIABETESwithout
Nephropathy, CVD or CV risk factors
1. ACE Inhibitor or ARB or
2. Dihydropyridine CCB or Thiazide diuretic
IF ACE Inhibitor, ARB, DHP-CCB and Thiazide are contraindicated or not tolerated,
SUBSTITUTE– Cardioselective BB* or– Long-acting NON DHP-CCB
Combination of first line agents
Addition of one or more of:Cardioselective BB or Long-acting CCB
Combinations of an ACE Inhibitor with an ARB are specifically not recommended in the absence of proteinuria
Pharmacotherapy of Hypertension in Diabetes without Nephropathy, CVD or CV Risk Factors
*Cardioselective BB: Acebutolol, Atenolol, Bisoprolol , Metoprolol

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Threshold equal or over 130/80 mmHg and Target below 130/80 mmHg
With Nephropathy, CVD or CV risk factors
ACE Inhibitor or ARB
Diabetes
Withoutthe above
1. ACE Inhibitor or ARB or
2. Thiazide diureticor DHP-CCB
Monitor serum potassium and creatinine carefully in patients with CKD prescribed an ACEI or ARB
Combinations of an ACEI with an ARB are specifically not recommended in the absence of proteinuriaMore than 3 drugs may be needed to reach target values
If Creatinine over 150 µmol/L or creatinine clearance below 30 ml/min ( 0.5 ml/sec), a loop diuretic should be substituted for a thiazide diuretic if control of volume is desired
Combination of 2 first line drugs may be considered
as initial therapy if the blood pressure is
>20 mmHg systolic or >10 mmHg diastolic
above target
> 2-drug combinations
Summary of Pharmacotherapy for Hypertension in Patients with Diabetes

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
1. Persons with diabetes mellitus should be treated to
attain a *SBP of <130 mmHg [Grade C, Level 3] and a **DBP
of <80 mmHg [Grade A, Level 1]. (These target BP levels
are the same as the BP treatment thresholds).
Combination therapy using two first-line agents may
also be considered as initial treatment of hypertension
[Grade C, Level 3] if SBP is 20 mmHg above target or if
DBP is 10 mmHg above target. However, caution
should be exercised in patients in whom a substantial
fall in BP is more likely or poorly tolerated (e.g., elderly
patients and patients with autonomic neuropathy)
*SBP= Systolic Blood Pressure **DBP= Diastolic blood pressure
2013Recommendation 1

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
2. For persons with cardiovascular or kidney
disease, including microalbuminuria, or with
cardiovascular risk factors in addition to diabetes
and hypertension, an ACE inhibitor or an ARB is
recommended as initial therapy [Grade A, Level 1A]
3. For persons with DM and HTN not included in the
above recommendation, appropriate choices
include (in alphabetical order): ACE inhibitors [Grade A,
Level 1A], ARBs [Grade A, Level 1A], dihydropyridine CCBs
[Grade A, Level 1A], and thiazide/thiazide-like diuretics [Grade A, Level 1A].
Recommendations 2 and 3

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
4. If target BP levels are not achieved with standard-
dose monotherapy, additional antihypertensive
therapy should be used [Grade D, Consensus]. For
persons in whom combination therapy with an
ACE inhibitor is being considered, a
dihydropyridine CCB is preferable to
hydrochlorothiazide [Grade A, Level 1A]
2013Recommendation 4

CDA Clinical Practice Guidelines
www.guidelines.diabetes.ca – for professionals
1-800-BANTING (226-8464)
www.diabetes.ca – for patients