Embed Size (px)
Citation preview

C
Ma
b
c
d
a
ARRAA
KEPAM
1
huimda[hiioh
p
A
0h
Vaccine 31 (2013) 5903– 5908
Contents lists available at ScienceDirect
Vaccine
jou rn al hom ep age: www.elsev ier .com/ locat e/vacc ine
an vaccine legacy explain the British pertussis resurgence?
aria A. Rioloa,b,∗, Aaron A. Kinga,b,c,d, Pejman Rohania,c,d
Center for the Study of Complex Systems, Ann Arbor, MI 48109, USADepartment of Mathematics, University of Michigan, Ann Arbor, MI 48109, USADepartment of Ecology and Evolutionary Biology, University of Michigan, Ann Arbor, MI 48109, USAFogarty International Center, National Institutes of Health, Bethesda, MD 20892, USA
r t i c l e i n f o
rticle history:eceived 3 July 2013eceived in revised form 3 September 2013ccepted 10 September 2013vailable online 16 October 2013
eywords:pidemiologyertussisge-structureathematical model
a b s t r a c t
Pertussis incidence has been rising in some countries, including the UK, despite sustained high vaccinecoverage. We questioned whether it is possible to explain the resurgence without recourse to complexhypotheses about pathogen evolution, subclinical infections, or trends in surveillance efficiency. In par-ticular, we investigated the possibility that the resurgence is a consequence of the legacy of incompletepediatric immunization, in the context of cohort structure and age-dependent transmission. We con-structed a model of pertussis transmission in England and Wales based on data on age-specific contactrates and historical vaccine coverage estimates. We evaluated the agreement between model-predictedand observed patterns of age-specific pertussis incidence under a variety of assumptions regarding theduration of immunity. Under the assumption that infection-derived immunity is complete and lifelong,and regardless of the duration of vaccine-induced immunity, the model consistently predicts a resur-gence of pertussis incidence comparable to that which has been observed. Interestingly, no resurgenceis predicted when infection- and vaccine-derived immunities wane at the same rate. These results were
qualitatively insensitive to rates of primary vaccine failure. We conclude that the alarming resurgence ofpertussis among adults and adolescents in Britain and elsewhere may simply be a legacy of historicallyinadequate coverage employing imperfect vaccines. Indeed, we argue that the absence of resurgenceat this late date would be more surprising. Our analysis shows that careful accounting for age depend-ence in contact rates and susceptibility is prerequisite to the identification of which features of pertussisional
epidemiology want addit. Introduction
The resurgence of pertussis in some highly developed countriesas caused a good deal of alarm [1]. In the United Kingdom, thenexpectedly large outbreak of 2012 – responsible for fourteen
nfant deaths – has prompted consideration of new preventioneasures, including vaccination of pregnant women and a booster
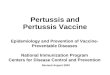
ose for adolescents [2–5]. Fig. 1 depicts annual pertussis incidencegainst the background of vaccine uptake in England and Wales4,6]. Since 2000, a gradual increase in incidence among adultsas been apparent. More recently, a sharp rise in incidence among
nfants and toddlers has become evident. This pattern of increasingncidence, especially among adults and adolescents, has emergedver the past two decades in a number of countries where pertussis
ad been considered under control [1,7–17].A variety of mechanisms have been proposed to explain thishenomenon. Chief among these are the vaccine-driven evolution
∗ Corresponding author at: Department of Mathematics, University of Michigan,nn Arbor, MI 48109, USA. Tel.: +1 734 276 7379.
E-mail address: [email protected] (M.A. Riolo).
264-410X/$ – see front matter © 2013 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.vaccine.2013.09.020
explanation.© 2013 Elsevier Ltd. All rights reserved.
of Bordetella pertussis (the main aetiological agent) [15], improvedsurveillance [16], changes in diagnostic tests [17], cessation of nat-ural immune boosting [18,19], and the switch from whole-cell toacellular vaccines [20], with concomitant changes in the nature andduration of protection [17,20]. Less attention has focused on thelong-term consequences of inadequate coverage with an imper-fect vaccine. Though effective vaccines have been widely used inEngland & Wales since 1957, their efficacy has never been perfectand vaccine coverage has only exceeded 90% since the 1990s. Aswe show here, the gradual accumulation within the population ofindividuals who have avoided both infection and vaccination andthus have escaped receiving protection sets the stage for a resur-gence, even in the absence of the aforementioned complexities.Focusing squarely on the recent pertussis epidemiology in Englandand Wales, we developed a transmission model to determine theextent to which observed patterns of incidence are a predictableconsequence of this legacy of imperfect vaccination.
2. Materials and methods
We constructed an age-stratified compartmental model of per-tussis transmission dynamics. Individuals are categorized by yearly

5904 M.A. Riolo et al. / Vaccine 3
1990 199 5 200 0 200 5 201 0Year
0
10
40
100
200
# C
ases
/ 10
0,00
0
0-12 months1-4 yea rs15+ yea rs
B Confirmed cases by age
1950 196 5 198 0 199 5 201 00
25
50
75
100
% u
ptak
e
1950 196 5 198 0 199 5 201 0Year
0
10
40
100
200
400
# C
ases
/ 10
0,00
0
National immun isation programm e
A Pertuss is notifications
Fig. 1. Incidence of pertussis in England and Wales over time based on total notifica-tions (panel A, solid line) and lab confirmed cases by age (panel B) [2,12]. Incidencesayp
autuwoti
wbcaate
earvdd(g
˜
re plotted on a square root scale for clarity. Estimated vaccine uptake for each birthear is plotted in panel A (dashed line)[4]. Although the national immunizationrogram began in 1957, uptake data is unavailable between 1957 and 1966.
ge groups up to age 75, with an additional category for infantsnder five months of age (i.e. too young to have received at leastwo doses of pertussis vaccine under the pre-1990 vaccine sched-le in the UK). For convenience, these age categories are labeledith indices starting from zero, so that N0 designates the number
f 0–6 month olds, N1 is the number of 6 month to 1 year olds, N2 ishe number of 1 year olds, and so on up to N75. The total populations designated by N.
All ages except for 0–5 month olds are tracked as yearly cohorts,ith annual aging occurring at the start of each school year. New-
orns are assumed to age continuously at rate a = 12/5 year−1,orresponding to the assumption that a newborn spends on aver-ge 5 months in the 0–5 month age category. Susceptible newbornsging at time t have probability u(t)e of being protected by vaccina-ion, where u(t) is the vaccine uptake at time t and e is the vaccinefficacy.
The model is initialized with conditions from the pre-vaccinera and proceeds by updating the numbers of individuals in eachge category who are susceptible, latently infected, infectious,ecovered, or vaccinated, respectively. Those in the recovered andaccinated classes are protected from infection for a period, theuration of which is a random variable, as we detail below. Theynamics of susceptible (Si), exposed (Ei), infectious (Ii), recoveredRi and R′
i), and vaccinated (Vi and V ′
i) individuals in age group i are
iven by:
dSi
dt= wV V ′
i + wRR′i − �i(t)Si + (bN − aS0)ıi,0 + a(1 − eu(t))S0ıi,1 (1)
dEi
dt= �i(t)Si − �Ei + aE0(ıi,1 − ıi,0) (2)
dIi
dt= �Ei − rIi + aI0(ıi,1 − ıi,0) (3)
dRi
dt= rIi − ωRRi + aR0(ıi,1 − ıi,0) (4)
1 (2013) 5903– 5908
dR′i
dt= ωRRi − ωRR′
i + aR′0(ıi,1 − ıi,0) (5)
dVi
dt= eu(t)aS0ıi,1 − ωV Vi + aV0(ıi,1 − ıi,0) (6)
dV ′i
dt= ωV Vi − ωV V ′
i + aV ′0(ıi,1 − ıi,0) (7)
where ıi,j is the Kronecker delta, which is one if i and j are equaland zero otherwise.
The model described by these equations was implemented as adiscrete, stochastic system. Specifically, we implemented a multi-nomial modification of Gillespie’s �-leap method [21–23]. Thisformulation allows us to quantify dynamic variability arising fromsmall, random perturbations in our system and additionally helpsto avoid conclusions resulting from unrealistic quantities (e.g. oneten-billionth of an infected person). The overall population usedin our simulations (around 63 million people) is large enoughthat one might expect these effects to be relatively minor. How-ever, we chose to use discrete, stochastic dynamics because ourmodel includes a large number of age categories differing in inci-dence, immune history, and contact rates, and some events thatare relatively rare (e.g. contact between infected 65 year olds andsusceptible 15 year olds) could still be dynamically important.
Age group i gains susceptible members through immune wan-ing and, if i = 0 or i = 1, births and the aging of susceptible newborns,respectively. The birth rate b = 1/75 year−1 is chosen to keep thepopulation steady given the 75 year lifespan. Individuals leave thesusceptible category by becoming exposed or, in the infant cate-gory, aging. The force of infection acting on age group i at time t is
�i(t) = q∑
k
Fhk(t)chkIk
Nk
where chk is the average rate (in contacts per year) at which an indi-vidual who is between 5h and 5h + 5 years old makes contact withthose between 5k and 5k + 5 years of age and q is the probability ofinfection given exposure. The number of infected individuals andtotal individuals in the kth five-year age block are denoted by
Ik =∑
5k<i≤5k+5
Ii and Nk =∑
5k<i≤5k+5
Ni
with I0 and N0 included in the calculation of N0 and I0, respectively.Values of cij and q were adopted from an earlier study [24]. In
particular, rates of daily contacts cij were obtained from the POLY-MOD study [25] (see Figs. S1D and 2A), and q was fixed at 4% asestimated in Ref. [24], leading to a pre-vaccine era mean age of firstinfection consistent with historical estimates (Fig. 2B). The neces-sary steps for obtaining contact rates cij from the data are describedin detail in Section S1 of the supplementary material.
To capture the strong seasonality in children’s social con-tacts [26], we incorporated an age-dependent seasonal forcingterm Fhk(t) based on school holidays. For 0 < h < 3 or 0 < k < 3 (i.e.when either party is 5–15 years old), Fhk(t) = �(1 ± 0.2), with + whenschool is in session and − during school holidays. Because there aremore school days than holidays, we use the normalization constant� to ensure that Fhk (t) has a mean of 1.0 over the whole year. Theschool holidays used in our simulations were July 19 September 8,October 28 November 3, December 21 January 10, and April 10, 25.If neither party is 55 years old, Fhk (t) = 1, leaving the contact rate
unaltered year round.Beginning in 1957, we assume that infants are vaccinated atsix months of age. From 1966, we used available estimates of vac-cine uptake for the UK (Fig. 1A) [6,27]. Uptake data for the period

M.A. Riolo et al. / Vaccine 31 (2013) 5903– 5908 5905
Fig. 2. (A) Age-specific pattern of contacts per day, normalized to run between 0 (white) and 1 (red). Infants, toddlers, and adults are involved in fewer contacts per daythan school aged children. Furthermore, most contacts are between people of similar age (the strong, central diagonal). Of the remaining contacts, most appear to be inter-generational (the two weaker diagonals), largely composed of household contacts between parents and children. Panels B–D depict the results of a single realization of ourt acy. (Bp by agt ces to
peaoatimfeIoc
iia
dtdndInolo
ln
TB
ransmission model with lifelong vaccine-derived immunity and 85% vaccine efficopulation susceptible to pertussis (cyan) by year. (C) Incidence (in cases/100,000)hat is susceptible to pertussis, plotted over time. (For interpretation of the referen
rior to 1966 are unavailable; we assumed uptake ramped up lin-arly from 1957 to 1966. The results presented in the main textssume a value of 60% coverage in 1957. We explored other values;ur results are qualitatively unaffected (see appendix S2). In thebsence of a serological marker for protection, the efficacy of per-ussis vaccines and the durations of infection- and vaccine-derivedmmunity are highly uncertain [28,29]. The results presented in the
ain text assume a vaccine efficacy of 85%, biologically plausibleor both the acellular and whole cell vaccines [30] though otherfficacies produced qualitatively similar results (see appendix S3).n further tests of the robustness of our results, we similarly variedur assumptions regarding human lifespan and the shape of theontact matrix (see appendix S1 and S6).
In our simulations, individuals exposed to pertussis becomenfectious after an average of 8 days (� = 365/8 year−1) and thenfectious period lasts 15 days on average (r = 365/15 year−1), agains in the model of Ref. [24].
We model two stages of resistance, Ri and R′i, so that the
uration of immunity is gamma distributed with shape parame-er two. The waning rate is given by wR = 2.0/dR year−1 where dR
enotes the mean duration (in years) of infection derived immu-ity. Like infection-derived immunity, the duration of vaccineerived immunity is gamma distributed with shape parameter two.
n simulations with lifelong natural (or vaccine derived) immu-ity, wR (or wV) is set to zero. We varied the assumed durationsf vaccine- and infection derived immunity, respectively, betweenifelong immunity and durations gamma-distributed with means
f 70, 40, and 10 years (see Table 1).For the initial conditions of our simulations, we used the popu-ation at the end of the 150th year of a run with lifelong immunity,o vaccination, and a total population of approximately sixty-three
able 1iological interpretation of average immune durations.
Mean durationof immunity
Probability ofremainingimmune after10 years
Probability ofremainingimmune after25 years
Probability ofremainingimmune after50 years
70 years 0.97 0.84 0.5840 years 0.91 0.64 0.2910 years 0.41 0.04 0.0005
) Overall incidence (red), vaccine uptake (purple), and the overall fraction of thee during each year of a realization of the model. (D) The fraction of each age groupcolor in this figure legend, the reader is referred to the web version of the article.)
million individuals. All simulations were run for 250 years, withvaccination beginning in the 157th year. At the end of each year,for each age category we recorded the population, number of sus-ceptibles, number of successful vaccinations, and number of cases.The pre-vaccine behavior among runs with the same duration ofnatural immunity was very consistent (see Figs. 3 and S7).
Because of the computational cost of using Gillespie’s directalgorithm with so many age-categories, we use a multinomial �-leaping method [21–23], in which we move forward by a fixedtime step � and determine the set of events that occurred dur-ing that time step. All simulations presented in this paper use � =1/365 year.
At each step, we consider all the ways an individual can leaveeach category as a set of competing events. For a sufficiently smalltime step �, we can approximate an individual’s probability of leav-ing a category as the total rate at which individuals leave multipliedby the length of the time step. For example, susceptible newbornsleave the category by aging at rate a or by becoming exposed atrate �i (t), so each of the S0 susceptible newborns has probability(a + �0 (t))� of leaving the category. We determine the total num-ber who leave the category drawing from a binomial distribution,X ∼ B(S0, p0) in our example. The expected fraction of these indi-viduals leaving via each event is proportional to that event’s rate.Continuing our example, the X individuals leaving the suscepti-ble newborn category are aging with probability a/(a + �0(t)) andhave been exposed with probability �0(t)/(a + �0(t)), so we drawthe numbers of aging and exposure events (Xa, XE) from a multi-nomial distribution with X trials and probabilities (a/(a + �0(t)),�0(t)/(a + �0(t))). For aging infants, we perform one more binomialdraw with probability u(t)e to determine how many aging infantsare successfully vaccinated.
The number of births, which do not deplete any population cat-egories, is determined by drawing from binomial distribution B(N,b�), where b is the per capita annual birth rate. Because this isa discrete stochastic model, we also include an immigration rateof one infected individual per year, uniformly distributed amongage categories to help distinguish between stable eradication and a
chance extinction in an easily re-invaded population. Once the setof events taking place has been determined, the whole populationis updated according to those events and the time t is incrementedby �.
5906 M.A. Riolo et al. / Vaccine 31 (2013) 5903– 5908
Cas
es p
er 1
00,0
00
0
100
400
900
1600
Ove
rall
Lifelong70 yrs40 yrs10 yrs
A
0
625
2500
5625
10000
0-12
mon
thsLifelong
70 yrs40 yrs10 yrs
B
0
900
3600
8100
14400
1-4
year
s
Lifelong70 yrs40 yrs10 yrs
C
1940 196 5 199 0 201 5Year
0
64
256
576
1024
15+
year
s
Lifelong70 yrs40 yrs10 yrs
D
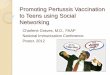
Fig. 3. Pertussis incidence through time for (A) the whole population, (B) infants under 1 year old, (C) toddlers 1–4 years old, and (D) adults and adolescents over 15 years old,plotted for model realizations assuming lifelong natural immunity. In each panel, different colored lines indicate predicted incidence when the duration of vaccine-derivedimmunity is varied from lifelong (black) to a mean of 10 years (lightest). For clarity, only one realization is plotted for each set of parameters, but other realizations matchedc figuri ader is
3
cltabio
daurpp1gtioatodf
l
losely (see Fig. S8). In the online supplementary materials, we present analogousmmunity. (For interpretation of the references to color in this figure legend, the re
. Results
In Fig. 2, we show a typical realization of the model, under theonservative assumption that infection-derived immunity is life-ong and that vaccination protects, on average, for 70 years (notehat we did not take into account under-reporting, thus all casesre included in model incidences). Vaccine efficacy is assumed toe 85%, consistent with estimates from Ref. [31]. Aggregate annual
ncidence, the estimated annual vaccine uptake and the percentagef the population susceptible to pertussis are shown in Fig. 2B.
Consistent with observed patterns in England & Wales, inci-ence in our model declines with the onset of pediatric vaccinationnd rebounds during the early 1980s, after several years of lowptake due to the mid-1970s vaccine scare, before eventuallyeturning to lower overall incidence and a long inter-epidemiceriod. Although high vaccine coverage is maintained, our modelredicts a gradual increase in overall incidence beginning in the990s (Fig. 2B). In Fig. 2C, we dissect these incidence data by ageroup, demonstrating that, as expected, in the pre-vaccine era, per-ussis was most common in young children (with a mean age atnfection in our model of 5 years). This figure also shows that thenset of immunization was accompanied by a rise in the age of casesnd that, crucially, the increase in overall incidence over the pastwo decades appears to be primarily among adults. From the rolloutf the national infant vaccination program in 1957 to the present
ay, the mean age of infection in our model climbed steadily, butor a dip following the vaccine scare of the mid-1970s.This shift in age distribution was also apparent in the immuno-ogical profile of our simulated population (Fig. 2D). In the
es under alternative assumptions of the durations of vaccine-derived and natural referred to the web version of the article.)
pre-vaccine era, the proportion of susceptibles among the popu-lation fell sharply with age, as expected for a childhood infection.With the onset of pediatric vaccination, the fraction of susceptiblechildren decreased substantially, but those who escaped protec-tion (either due to incomplete coverage or primary vaccine failure)remained susceptible into adulthood. This effect is clearly visiblein Fig. 2D as a spillover of susceptibles into older age groups overtime, with cohorts born at the start of the vaccine era on the leadingedge of the wave.
Crucially, this rising incidence of pertussis in adults andadolescents occurred regardless of the assumed duration ofvaccine-derived immunity. We provide support for this statementin Fig. 3, which depicts the annual pertussis incidence in differentage groups for varying durations of vaccine- and infection-derivedimmunity. When infection-derived immunity was lifelong, anincrease in incidence among adolescents and adults was inevitableif vaccine-induced protection was not permanent (Fig. 3D). Withlong-lasting vaccine-derived immunity, there was also a notableincrease in infant (<1 year old) cases (Fig. 3B).
4. Discussion
Our results suggest that rising pertussis incidence among adultsand adolescents should not be surprising. Indeed, our simulations,even with the conservative assumptions of lifelong natural immu-
nity, a 70-year mean duration of vaccine immunity and 85% efficacypredicted a long- lasting honeymoon period [32] followed by aresurgence among older age groups. This pattern is a legacy ofincomplete vaccination with an imperfect vaccine: individuals born
cine 3
impvtbbi
atmirsw
lusmMqsih
cebttslSwHotc
atltbipciwd
A
drt
htolo
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
M.A. Riolo et al. / Vac
n the vaccine era are less likely to be infected as children andore likely to remain susceptible as teens and adults than their
re-vaccine predecessors. Thus, during the first few decades ofaccination, the population benefits both directly from vaccine pro-ection of children and indirectly from herd immunity establishedy natural infection in the pre-vaccine era. As cohorts of childrenorn in the vaccine era grow up, the latter effect diminishes and
ncidence among adults inevitably rises.In view of the considerable uncertainty surrounding the nature
nd duration of acquired immunity to pertussis [33], it is importanto assess the robustness of this conclusion. Accordingly, we varied
odel assumptions regarding the durations of natural and vaccine-nduced immunity. When these were assumed equal, there was noesurgence. Rather, the model predicted substantially higher andteady incidence among all age groups (Fig. S8), in contradictionith observation.
Our use of a model in which infection-derived immunity can beifelong may at first glance appear to be at odds with studies doc-menting reinfection [29]. However, a number of population-leveltudies have found that incidence data are best explained by trans-ission models with long-lasting natural immunity [24,34,35].oreover, evidence suggesting that pertussis re-infections are fre-
uently less transmissible than are primary infections [35,36], goesome way toward resolving the apparent discrepancy betweenmmune durations estimated from population-level data on the oneand and clinical studies on the other.
The demographics of our model are a rough caricature, with aonstant birth rate and type I demographics (life expectancy of sev-nty five years). The observed slow rise in adult incidence driveny the aging of vaccine-era cohorts, however, is reasonably robust:he same trends emerge under a variety of demographic assump-ions (Fig. S10), though the cohort effects exhibited in Fig. 3 are lessharply defined. In addition, incorporating immigration and popu-ation expansion would enhance the legacy effect described here.imilarly, the legacy of incomplete vaccination is still observedhen alternative contact matrix structures are assumed (Fig. S2).owever the detailed epidemiological picture, including the shapef the population’s immunity profile and the timing and speed ofhe predicted resurgence, is affected by the precise structure of theontact network.
These caveats notwithstanding, the principal conclusion of ourccounting should be clear. The legacies of infection and vaccina-ion are visible in a population’s immunity profile for decades andeave long-lived signatures on incidence dynamics. We submit thathe recent resurgence in adult and adolescent pertussis cases maye best understood as the end of a long honey-moon period, dur-
ng which infection-derived herd immunity and imperfect vaccinerotection combined to greatly reduce incidence. In the years toome, as those who as children benefited from infection-inducedmmunity die, more effective vaccines and vaccination campaigns
ill likely be required if we are to regain the upper hand on thisisease.
cknowledgements
PR and AAK developed the model framework. PR and MAResigned the study. MAR implemented the model, analyzed theesults, and wrote the first draft of the report. AAK and PR con-ributed to the writing of the report.
We thank Doug Jackson and an anonymous reviewer for theirelpful comments on the paper. PR and AAK are supported by
he Research and Policy in Infectious Disease Dynamics programf the Science and Technology Directorate, Department of Home-and Security, the Fogarty International Center, National Institutesf Health and by a research grant from the National Institutes of[
[
1 (2013) 5903– 5908 5907
Health (1R01AI101155). PR also received support from the VaccineModeling Initiative of the Bill & Melinda Gates Foundation.
Appendix A. Supplementary data
Supplementary data associated with this article can befound, in the online version, at http://dx.doi.org/10.1016/j.vaccine.2013.09.020.
References
[1] Jackson D, Rohani P. Perplexities of pertussis: recent global epidemiologicaltrends and their potential causes. Epidemiol Infect 2013 (in press).
[2] United Kingdom. Health Protection Agency. 2012 Press Releases: WhoopingCoughcases Continue to Increase; 2012 [accessed 03.07.13] http://www.hpa.org.uk/NewsCentre/NationalPressReleases/2012PressReleases/121130Whoopingcoughcasescontinuetoincrease/
[3] United Kingdom. Health Protection Agency. Cases of Whooping CoughDecline After Record Numbers in 2012; 2013. http://www.hpa.org.uk/NewsCentre/NationalPressReleases/2013PressReleases/130201Casesofwhoopingcoughdeclineafterrecordnumbers/
[4] United Kingdom. Health Protection Agency. Infection report: confirmed Per-tussis in England and Wales: data to end-September 2012. Health ProtectionReport, Vol. 6; 2012.
[5] Gulland A. Teenagers and newborn babies in England and Wales mayget pertussis jab as cases continue to rise. Br Med J 2012;345:e5919,http://dx.doi.org/10.1136/bmje5919.
[6] United Kingdom. Health Protection Agency. Completed Primary Coursesat Two Years of Age: England and Wales, 1966–1977, England only1978 onwards; 2008 [accessed 03.07.13] http://www.hpa.org.uk/web/HPAweb&HPAwebStandard/HPAweb C/1195733819251
[7] Celentano LP, Massari M, Paramatti D, Salamaso S, Tozzi AE. Resurgence ofPertussis in Europe. Pediatr Infect Dis J 2005;24:761–5.
[8] Güris D, Strebel PM, Bardenheier B, et al. Changing epidemiology of pertussis inthe United States: increasing reported incidence among adolescents and adults,1990–1996. Clin Infect Dis 1999;28:1230–7.
[9] Skowronski DM, De Serres G, MacDonald D, et al. The changing age and seasonalprofile of pertussis in Canada. J Infect Dis 2002;185:1448–53.
10] Quinn HE, McIntyre PB. Pertussis epidemiology in Australia over thedecade 1995–2005: trends by region and age group. Commun Dis Intell2007;31:205–15.
11] Crowcroft NS, Pebody RG. Recent developments in pertussis. Lancet2006;367:1926–36.
12] Tan T, Trindade E, Skowronski D. Epidemiology of pertussis. Pediatr Infect DisJ 2005;24(Suppl. 5):S10–8.
13] Wood N, MacIntyre P. Pertussis: review of epidemiology, diagnosis, manage-ment and prevention. Pediatr Respir Rev 2008;8:211–2.
14] United Kingdom. Health Protection Agency. Whooping Cough (Pertus-sis): Latest Epidemiological Data: Table 4: Pertussis Table by Age Group,Table 6: Pertussis Notifications and Deaths, and Table 7: Pertussis Noti-fications by Age; 2013 [accessed 03.07.13] http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/WhoopingCough/EpidemiologicalData
15] Mooi FR, van Loo IH, King AJ. Adaptation of Bordetella pertussis to vaccination:a cause for its reemergence? Emerg Infect Dis 2001;7:526–8.
16] Cherry JD. The science and fiction of the resurgence of pertussis. Pediatrics2003;112:405–6.
17] Cherry JD. Epidemic pertussis in 2012 the resurgence of a vaccine-preventabledisease. N Engl J Med 2012;367:785–7.
18] Águas R. Pertussis: increasing disease as a consequence of reducing transmis-sion. Lancet Infect Dis 2006;6:112–7.
19] Lavine JS, King AA, Björnstad ON. Natural immune boosting in pertussis dynam-ics and the potential for long-term vaccine failure. Proc Natl Acad Sci U S A2011;108:7259–64, http://dx.doi.org/10.1073/pnas1014394108.
20] Shapiro ED. Acellular vaccines and resurgence of pertussis. J Am Med Assoc2012;308(20):2149–50.
21] Gillespie DT. Approximate accelerated stochastic simulation ofchemically reacting systems. J Chem Phys 2001;115:1716–33,http://dx.doi.org/10.1063/11378322.
22] Keeling MJ, Rohani P. Modeling infectious diseases in humans and animals.Princeton, New Jersey, USA: Princeton University Press; 2008.
23] Pettrgrew MF, Resat H. Multinomial �-leaping method for stochastic kineticsimulations. J Chem Phys 2007;12:084101.
24] Rohani P, Zhong X, King AA. Contact network structure explains the changingepidemiology of pertussis. Science 2010;330:98285.
25] Mossong J, Hens N, Jit M. Social contacts and mixing patterns relevant to thespread of infectious diseases. PLoS Med 2008;5:e74.
26] Eames KTD, Tilston NL, Brooks-Pollock E, Edmunds WJ. Measured dynamicsocial contact patterns explain the spread of H1N1v influenza. PLoS ComputBiol 2012;8:e1002425, http://dx.doi.org/10.1371/journal.pcbi1002425.
27] Rohani P, Earn DJD, Grenfell BT. Impact of immunisation on pertussis transmis-sion in England and Wales. Lancet 2000;355:285–6.

5 cine 3
[
[
[
[
[
[[
[35] Broutin H, Viboud C, Grenfell BT, Miller MA, Rohani P. Impact of vaccination
908 M.A. Riolo et al. / Vac
28] Mills KHG, Ryan M, Ryan E, Mahon BP. A murine model in which protectioncorrelates with pertussis vaccine efficacy in children reveals complimentaryroles for humoral and cell-mediated immunity in protection against Bordatellapertussis. Infect Immun 1998;66:594–602.
29] Wendelboe AM, Van Rie A, Salmaso S, Englund JA. Duration of immunityagainst pertussis after natural infection or vaccination. Pediatr Infect Dis J2005;24:S58–61.
30] Greco D, Salmaso S, Mastrantonio P, et al. A controlled trial of two acel-lular vaccines and one whole-cell vaccine against pertussis. N Engl J Med1996;334:341–9.
31] Blennow M, Olin P, Granström M, Bernier RH. Protective efficacy of a whole cellpertussis vaccine. Br Med J 1988;296:1570–2.
[
1 (2013) 5903– 5908
32] McLean AR, Anderson RM. Measles in developing countries Part II.The predicted impact of mass vaccination. Epidemiol Infect 1988;100:41942.
33] Mills KHG. Immunity to Bordetella pertussis. Microb Infect 2001;3:65577.34] Wearing HJ, Rohani P. Estimating the duration of pertussis immunity using
epidemiological signatures. PLoS Pathog 2009;5:e1000647.
and birth rate on the epidemiology of pertussis: a comparative study in 64countries. Proc R Soc B 2010:1.
36] Mertsola J, Ruuskanen O, Eerola E, Viljanen MK. Intrafamilial spread of pertussis.J Pediatr 1983;103:359–63.