Embed Size (px)
Citation preview

Accepted Manuscript
Can Trauma Surgeons Manage Mild Traumatic Brain Injuries?
Tiffany L. Overton, MA, MPH Shahid Shafi, Md George F. Cravens, MD Rajesh R.Gandhi, MD, PhD
PII: S0002-9610(14)00179-2
DOI: 10.1016/j.amjsurg.2014.02.012
Reference: AJS 11155
To appear in: The American Journal of Surgery
Received Date: 13 September 2013
Revised Date: 29 January 2014
Accepted Date: 11 February 2014
Please cite this article as: Overton TL, Shafi S, Cravens GF, Gandhi RR, Can Trauma SurgeonsManage Mild Traumatic Brain Injuries?, The American Journal of Surgery (2014), doi: 10.1016/j.amjsurg.2014.02.012.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 1
Can Trauma Surgeons Manage Mild Traumatic Brain Injuries?
Running head: MANAGEMENT OF MILD TBI Authors: Corresponding Author: Tiffany L. Overton, MA, MPH [email protected] O: 817-702-5913 F: 817-702-5162 Trauma Services JPS Health Network 1500 S. Main St. Fort Worth, Tx 76104 Shahid Shafi, MD [email protected] JPS Health Network George F. Cravens, MD [email protected] Rajesh R. Gandhi, MD, PhD [email protected]
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 2
BACKGROUND
Traumatic brain injury (TBI) is an important public health concern and a leading cause of
morbidity and mortality.(1) The vast majority of TBI are considered mild (70-85% ),(1, 2) and
are defined as Glasgow Coma Scale (GCS) score of 13 to 15 and a temporary disruption of brain
function after a traumatic injury.(3-6) Controversy surrounds the most appropriate management
of mild TBI (MTBI).(7) The American College of Surgeons recommends neurosurgical
evaluation of any patient with a GCS score less than 15 at two hours after injury and patients
greater than 65 years of age(4) even though less than 1% of patients with MTBI require
neurosurgical intervention.(8, 9) This requirement creates a burden on scarce neurosurgical
resources, which is likely to become worse with shortage of neurosurgeons and aging of the
population.(10) In fact, there is emerging evidence that patients with intracranial bleeds can be
safely managed in trauma centers without neurosurgical services, except in the case of moderate
to severe TBI.(11, 12)
To study this issue, we implemented a protocol of selective neurosurgical consultation in
2008 that enabled trauma surgeons to manage patients with MTBI without neurosurgical
consultations. This study reports our initial experience with management of MTBI by trauma
surgeons alone. We hypothesize patients with MTBI managed by trauma surgeons will be the
same as outcomes for patients managed by neurosurgeons.
METHOD
This is a retrospective analysis of patients treated at a major urban level 1 trauma center
at a public institution over a period of 7 years (January 2006-June 2012). Patients were
monitored before (2006 – 2008) and after (2008-2012) the implementation of the protocol
mentioned above. The inclusion criteria consisted of patients with mild TBI defined as an

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 3
intracranial hemorrhage less than or equal to 1 centimeter and a Glasgow Coma Score of 13 or
greater at the time of arrival. Exclusion criteria consisted of patients with additional intracranial
injuries (i.e. intraparenchymal hemorrhages, diffuse axonal injuries with white matter shearing),
and patients transferred to another acute care facility or those who left against medical advice.
Based on these criteria, 171 patients were included in the study. Patients were divided into two
groups: those managed by trauma surgeons alone (n = 51, 30%) and those who were managed by
neurosurgeons (n = 120, 70%). Management by a neurosurgeon was defined by whether or not a
neurosurgeon was consulted. Neurosurgical consultations could occur at any point during the
patients’ admission, so patients with a shift and neurosurgical consultation after initial exam
were included in the neurosurgical management group. The need for neurosurgery consultation
was at the discretion of the trauma surgeons.
The primary outcome of interest was Glasgow Outcome Score (GOS). GOS ranges from
1 to 4, with higher scores reflecting better outcomes. Patients were classified into two categories
based upon their GOS. Scores equal to or less than 3 suggest moderate to severe outcomes and
scores greater than 3 suggest good outcomes. Severity of TBI was measured using the
Abbreviated Injury Scale (AIS) and the Glasgow Coma Scale (GCS).(13, 14) Overall, injury
severity was measured using the Injury Severity Score (ISS)(15) and systolic blood pressure
(SBP) upon presentation to the emergency department.
Chi-square and Fisher exact test were used as appropriate for categorical variables,
whereas Student t test and ANOVA were used for continuous variables. Multivariate analysis
was undertaken using backward stepwise binary logistic regression analyses to measure the
association of trauma vs. neurosurgical management on outcome while controlling for
confounding effects of age, gender, race/ethnicity, injury severity, insurance status, and GCS

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 4
motor scores upon arrival to the emergency department. Results are presented as medians and
interquartile range (IQR), proportions, and odds ratios (ORs) with 95% confidence interval (CI).
Statistical Package for the Social Sciences for Windows, Version 20 (SPSS Inc., Chicago) was
used for all statistical analyses, with p < .05 considered significant.
RESULTS
Neurosurgical consultations among MTBI patients significantly decreased from 94% to
65% after implementation of the protocol in 2008 (Table I) even though the patients presenting
after protocol implementation had significantly higher injury severity scores.
Patients managed by trauma surgeons alone and those managed by neurosurgeons were
similar in age, race/ethnicity, gender distribution, injury severity, length of stay, or mechanism of
injury (Table II). Neurosurgeon consultations were called for in the majority of patients
presenting with a GCS of 15 (x2 = 6.914, p < 0.032).
Neurologic outcome of the patients in the two groups was also similar. GOS indicated
good recovery for the majority of patients (Trauma Surgeons 82% vs. Neurosurgeons 78%, p =
ns). Patients were primarily discharged home (Trauma Surgeons 82% vs. Neurosurgeons 79%, p
= ns) with moderate disability (Trauma Surgeons, 77%; Neurosurgeons, 81%). There were no
differences in patients’ hospital length of stay or ICU length of stay by management service
(Table III).
Multivariate regression analysis yielded younger age, lower ISS, and higher GCS motor
scores as significant predictors for better outcomes (Table IV). Neurosurgeon consultation was
not associated with patient outcomes.
The American College of Surgeons recommends obtaining neurosurgical consultation for
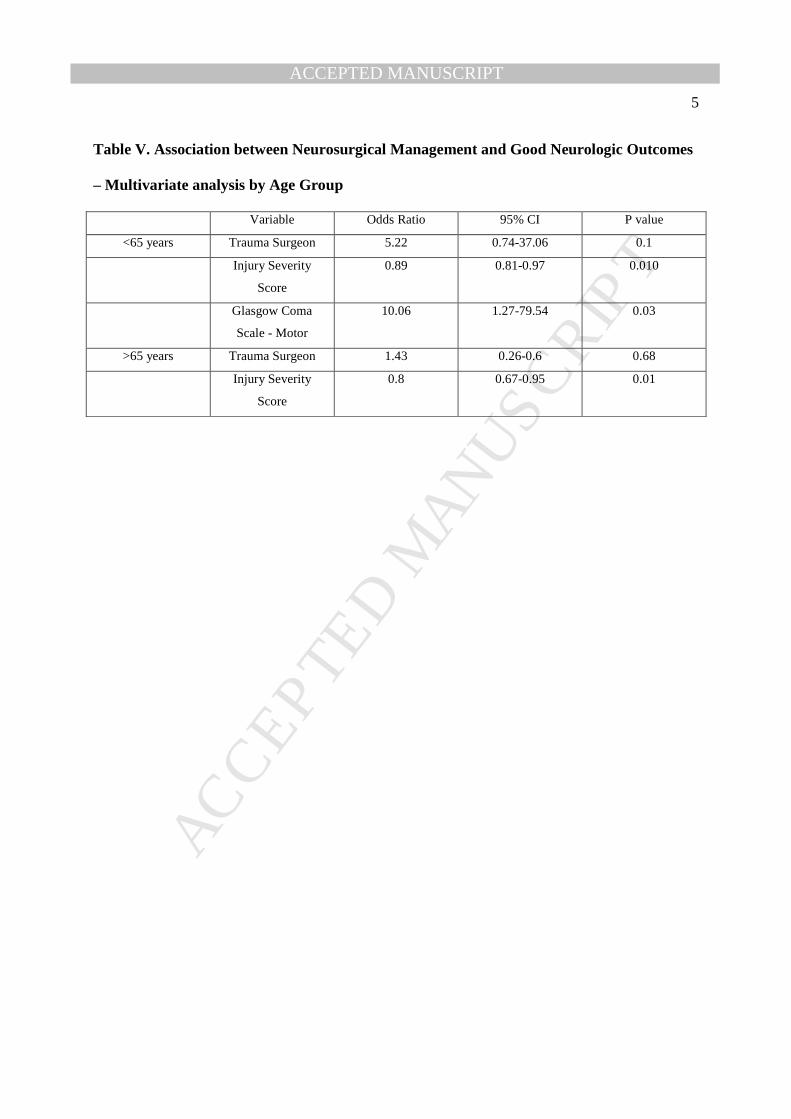
patients older than 65 years of age with blunt TBI. Table V shows the multivariate analysis for

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 5
patients younger and older than 65 years separately. Again, management by neurosurgeons was
not associated with neurologic outcomes of the patients over or under 65 years of age.
DISCUSSION
There are two primary findings of this study. First, by implementing a policy of selective
consultation, we were able to reduce neurosurgery consultations. Second, there was no difference
in neurologic outcomes between the patients with MTBI managed by trauma surgeons versus
neurosurgeons, suggesting that trauma surgeons can effectively manage such patients.
These findings are consistent with prior studies demonstrating the ability of trauma
surgeons to effectively manage patients with small ICH. This is likely related to the fact that only
0.1% to 0.3% of MTBI patients with abnormal head CT require neurosurgical intervention or
treatment.(8, 9, 16, 17) Non-operative management of TBI such as serial exams and imaging
studies, neuropsychology evaluation for concussion, and rehabilitation can be managed
effectively by trauma surgeons.
The main implication of our findings is that not all patients with MTBI require
neurosurgical consultation. This selective use of neurosurgical resources may be beneficial for
trauma centers, particularly in locations with scarcity of neurosurgeons. Currently, the ratio of
neurosurgeons to the population in the United States is approximately 1:61,000. With only
approximately 3,689 practicing board certified neurosurgeons and increasing demands for
neurosurgical services,(18) the availability of on-call neurosurgeons is a growing national issue
in trauma and emergency care.(19)
Neurosurgical workforce demands are usually estimated at one neurosurgeon per 100,000
population ratio,(20) but many states have zero to two neurosurgeons per 100,000 people.(21)
Trauma center designation depends upon 24 hour on-call neurosurgical coverage, and due in part

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 6
to this shortage, trauma centers in Pennsylvania, Tennessee, Missouri, Illinois, Texas, and
Florida were closed.(22) Not surprisingly, in a national survey of emergency department
directors, 75% reported inadequate neurosurgical coverage.(10) In addition, selective use of
neurosurgical resources may allow for more appropriate allocation of scarce neurosurgical
resources to more severely injured patients or non-trauma patients. The American College of
Surgeons needs to look more carefully at resource use on a larger scale, as frequent neurosurgical
consultation may not be necessary, and a reduction of consultations can reduce costs.
This study has a few limitations that should be recognized. This is a retrospective
analysis with all its inherent limitations. An important limitation is the possibility of type II error
due to a small sample size. Another limitation is the lack of follow-up data and patients’ long-
term outcomes. More discriminatory outcomes, such as the Disability Rating Scale, was
unavailable for these patients, so we were unable to evaluate more sensitive outcomes for
patients at discharge. Additionally, the protocol was voluntary and requesting neurosurgical
consultations may be related to on-call trauma surgeon’s preference.
In conclusion, implementation of a policy for selective neurosurgical consultation for
patients with mild TBI significantly reduced the number of neurosurgical consultations without
any impact on patient outcomes. Trauma surgeons can effectively manage patients with mild
TBI.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 7
REFERENCES
1. Centers for Disease Control and Prevention. Report to Congress on Mild Traumatic Brain
Injury in the United States: Steps to Prevent a Serious Public Health Problem. Atlanta, GA:
Department of Health and Human Services, 2003.
2. Thurman D, Guerrero J. Trends in hospitalization associated with traumatic brain injury.
JAMA. 1999;282:954-7.
3. Alexander MP. Mild traumatic brain injury: Pathophysiology, natural history, and clinical
management. Neurology. 1995;45:1253-60.
4. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support
Student Course Manual. Ninth ed. Chicago, IL,: American College of Surgeons; 2012.
5. Jennett B, MacMillan R. Epidemiology of head injury. Br Med J. 1981;282:101-4.
6. Wasserberg J. Treating head injuries. BMJ. 2002;325:454-5.
7. Blostein PA, Jones SJ. Identification and evaluation of patients with mild traumatic brain
injury: Results of a national survey of Level I Trauma Centers. J Trauma. 2003;55:450-3.
8. Jeret JS, Mandell M, Anziska B, et al. Clinical predictors of abnormality disclosed by
computed tomography after mild head trauma. Neurosurgery. 1993;32:9-16.
9. Miller EC, Derlet RW, Kinser D. Minor head trauma: Is computed tomography always
necessary? Neurosurgery. 1993;32:9-16.
10. Rao MB, Lerro C, Gross CP. Shortage of on-call surgical specialist coverage: A national
survey of emergency department directors. Acad Emerg Med. 2010;17(12):1374-82.
11. Esposito TJ, Reed RL II, Gamelli RL, Luchette FA. Neurosurgical coverage: Essential,
desired, or irrelevant for good patient care and trauma center status. . Ann Surg. 2005;242:364-
70.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 8
12. Klein Y, Donchik V, Jaffe D, Simon D, Kessel B, Levy L, et al. Management of patients
with traumatic intracranial injury in hospitals without neurosurgical service. J Trauma.
2010;69:544-8.
13. Copes WS, Sacco WJ, Champion HR, Bain LW, editors. Progress in characterizing
anatomic injury. Proceedings of the 33rd Annual Meeting of the Association for the
Advancement of Automotive Medicine; 1998; Baltimore, Mass.
14. Teasdale G, Jennet B. Assessment of coma and impaired consciousness. Lancet.
1974;2:81-4.
15. Baker SP, O'Neill B, Haddon W, Long WB. The Injury Severity Score: a method for
describing patients with multiple injuries and evaluating emergency care. J Trauma.
1974;14:187-96.
16. Dunham CM, Coates S, Cooper C. Compelling evidence for discretionary brain
computed tomographic imaging in those patients with mild cognitive impairment after blunt
trauma. J Trauma. 1996;41:679-86.
17. Huynh T, Jacobs DG, Dix S, Sing RF, Miles WS, Thomason MH. Utility of
Neurosurgical Consultation for Mild Traumatic Brain Injury. The American Surgeon.
2006;72:1162-7.
18. Harbrecht BG, Smith JW, Franklin GA, Miller FB, Richardson JD. Decreasing Regional
Neurosurgical Workforce - A Blueprint for Disaster. J Trauma. 2010;68(6):1367-74.
19. Center for Workforce Studies. 2012 Physician Specialty Data Book. Washington, DC:
Association of American Medical Colleges, 2012.
20. Zuidema GD. The SOSSUS report and its impact on neurosurgery. J Neurosurg.
1977;46:135-44.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 9
21. Institute HPR. The Surgical Workforce in the United States: Profile and Recent Trends.
American College of Surgeons and Association of American Medical Colleges, 2010.
22. The Projected Physician Shortage and How Health Care Reforms Can Address the
Problem: Hearing before the Small Business, United States House of Representatives, First
Session Sess. (July 8, 2009, 2009).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Background: Current practices suggest patients with mild traumatic brain injuries (MTBI)
receive neurosurgical consultations, while fewer than 1% require neurosurgical intervention. We
implemented a policy of selective neurosurgical consultation with the hypothesis that trauma
surgeons alone may manage such patients with no impact on patient outcomes. Methods: Data
from a Level I trauma registry was analyzed. Patients with MTBI resulting in an intracranial
hemorrhage less than or equal to 1 centimeter and a Glasgow Coma Score of 13 or greater were
included. Patients with additional intracranial injuries were excluded. Multivariate regression
was used to determine the relationship between neurosurgical management and good neurologic
outcomes, while controlling for injury severity, demographics, and comorbidities. Results:
Implementation of the neurosurgical policy significantly reduced the number of such consults
(94% before vs. 65% after, p < 0.002). Multivariate analysis revealed that neurosurgical
consultation was not associated with neurologic outcomes of patients. Conclusions:
Implementation of a selective neurosurgical consultation policy for patients with MTBI reduced
neurosurgical consultations without any impact on patient outcomes, suggesting trauma surgeons
can effectively manage these patients.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Summary: Current practices suggest patients with mild traumatic brain injuries receive neurosurgical consultations, while less than 1% require neurosurgical intervention. We implemented a policy of selective neurosurgical consultation with the hypothesis that trauma surgeons alone may manage such patients with no impact on patient outcomes. Implementation of the neurosurgical policy significantly reduced the number of such consults, while neurosurgical consultation was not associated with neurologic outcomes of patients. This suggests that trauma surgeons can effectively manage patients with mild traumatic brain injuries.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Keywords: mild traumatic brain injury; neurosurgical management; neurosurgeon consultation; policy implementation; mild TBI management

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 1
Table I. Neurosurgical Consultations Before and After Protocol Implementation
Before Implementation
(n = 31)
After Implementation
(n = 140)
No Neurosurgical Consultation 2 (6%) 49 (35%)
Neurosurgical Consultation 29 (94%) 91 (65%)
Age (yr, median, IQR) 42 (24 72) 50.5 (31.5 69.8)
Gender (% male) 23 (74%) 95 (68%)
Race/Ethnicity (% White, Non
Hispanic)
21 (68%) 86 (61%)
ISS (median, IQR)* 16 (16 20) 17 (16 24)
First ED Systolic Blood Pressure 137 (122 159) 134 (120.5 154)
GCS
13 1 (3%) 9 (6%)
14 5 (16%) 28 (20%)
15 25 (81%) 103 (74%)
GCS Motor (median, IQR) 6 (6 6) 6 (6 6)
ISS, Injury Severity Scale; GCS, Glasgow Coma Scale. *significant difference between groups, p < 0.05

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 2
Table II. Patient Demographics and Injury Severity
Trauma Surgeon
(n = 51)
Neurosurgeon
(n = 120)
Age (yr, median, IQR) 48 (34 64) 49 (29 71)
Gender, % male 71% 68%
Race/Ethnicity (%White, Non
Hispanic)
58% 65%
ISS (median, IQR) 17 (16 25) 17 (16 21)
First ED Systolic Blood
Pressure (mm Hg, median,
IQR)
132 (122 154) 134 (120 156)
GCS (%)*
13 6% 6%
14 31% 14%
15 63% 80%
GCS Motor (median, IQR) 6 (6 6) 6 (6 6)
Mechanism of Injury
Fall 42% 48%
Motor vehicle 31% 23%
Assault 15% 13%
Motorcycle 10% 4%
Auto-Pedestrian 0% 3%
Other 2% 8%
ISS Injury Severity Scale; GCS, Glasgow Coma Scale.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 3
Table III. Crude Outcomes by Management Service
Trauma Surgeon
(n = 51, 30%)
Neurosurgeon
(n = 120, 70%)
Glasgow Outcome Score Good Recovery 42 (82%) 93 (78%)
Moderate Disability 7 (14%) 17 (14%)
Severe Disability 2 (4%) 2 (2%)
Death 0 (0%) 8 (7%)
Discharge Location Home 42 (82%) 95 (79%)
Facility 9 (18%) 16 (13%)
Other 0% 1 (1%)
Length of stay (days,
median, IQR)
2 (1 5) 3 (2 6)
ICU length of stay (days,
median, IQR)
1 (1 3) 2 (1 5)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 4
Table IV. Association between Neurosurgical Management and Good Neurologic Outcomes
– Multivariate analysis
Variable Odds Ratio 95% CI P value
Trauma Surgeon 1.74 0.61-4.92 0.300
Age 0.94 0.91-0.96 0.000
Injury Severity Score 0.87 0.81-0.94 0.000
Glasgow Coma Scale -
Motor
13.96 2.23-87.3 0.005
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 5
Table V. Association between Neurosurgical Management and Good Neurologic Outcomes
– Multivariate analysis by Age Group
Variable Odds Ratio 95% CI P value
<65 years Trauma Surgeon 5.22 0.74-37.06 0.1
Injury Severity
Score
0.89 0.81-0.97 0.010
Glasgow Coma
Scale - Motor
10.06 1.27-79.54 0.03
>65 years Trauma Surgeon 1.43 0.26-0.6 0.68
Injury Severity
Score
0.8 0.67-0.95 0.01















![TRAUMATIC BRIAN INJURY (TBI): COMPREHENSIVE REVIEWd-scholarship.pitt.edu/24486/1/Wolfe_mph_essay_4... · >12 mild [2-5]. Mild traumatic brain injury (mTBI) is the most common form](https://img.pdfslide.us/doc/110x75/5f600368ef575959696a6d58/traumatic-brian-injury-tbi-comprehensive-reviewd-12-mild-2-5-mild-traumatic.jpg)