Embed Size (px)
Citation preview
Callosotomy for drop events and Peri-Insular Hemispherotomy following neonatal strokes are
highly effective single stage operations in Pediatric Epilepsy Surgery
Jeffrey P. Blount MDCurtis J. Rozzelle MDHyunmi Kim MD PhD MPHRani Singh MDMonisha Goyal MDPongkiat Kankirawatana MD
ISPN Kobe, Japan
October 22, 2016
The Burden and Challenge of MRE in Children• Epilepsy is a major Public Health Problem
• Common and can have substantial physical and psychological consequences• Premature death• Traumatic injury• Mental Health Disorders• Impaired learning and behavior-----, thought contagious or associated with witchcraft
and the occult in some societies---further escalating the burden---stigma, social isolation
• Global Burden of Diseases Index (2010) • Uncontrolled epilepsy second only to HIV in overall disability weight score
• Prevalence and incidence higher in the developing world• 9.7 persons per 1000; nearly twice that of the West• Most common in youngest patients (<20) in developing world and older
patients (30-50) in more developed countries• In Sub-Saharan Africa more than 90% with epilepsy are <20 years old
Fisher RS. Epilepsia 2005Da-Biop A. Lancet Neurology 2014
Lancet Commission on Global Surgery:
• 47 million deaths and 16 USD trillion per year restored.
• NSG probably 20%.
• WHO declares essential surgery a global priority
• Must think of training locals...(many of whom are very capable)
• Finding solutions : look at resources, find strengths and weaknesses- define achievable goals.
Barriers to effective treatment in children• Medical treatment- “the treatment gap”
• (number of people with active epilepsy)- (number properly treated for
epilepsy),expressed as a percentage
• it reflects the proportion seeking treatment for epilepsy and who adhere to the
prescribed treatment
• Surgical treatment- largely unavailable due to:
• Scarcity of trained providers
• Cost of assessment, monitoring and imaging.
• Tragic because structural etiologies even more common than in developed
countries
• Infection (esp parasitic), Trauma, Strokes
Promoting Epilepsy Surgery Opportunities
• Ideal Surgical Intervention• Highly effective with minimal
complications for properly trained surgeons
• Inexpensive work-up for surgical candidacy• Semiology and Clinical Exam
• EEG
• Brain image- CT or MRI
• PIH for ischemic strokes of infancy
• Corpus callosotomy for severe generalized events with drop events
Pure pediatric series of 49 hemispherectomies35 PIH, 14 FH78% seizure freedom; 90 % Engel Class I or IIOnly those with CDs /hemimegencephaly had
recurrenceAll stroke patients SF
Effect durable over time
PIH for infantile hemispheric events-literature
• 19 patients with “vasculogenicepilepsy”• 7 children with large porencephalic
regions from MCA infarcts
• 7/7 seizure free
• Highly effective
• Extended resections occasionally needed beyond region of infarct for smaller regions of infarction
0
5
10
15
20
25
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
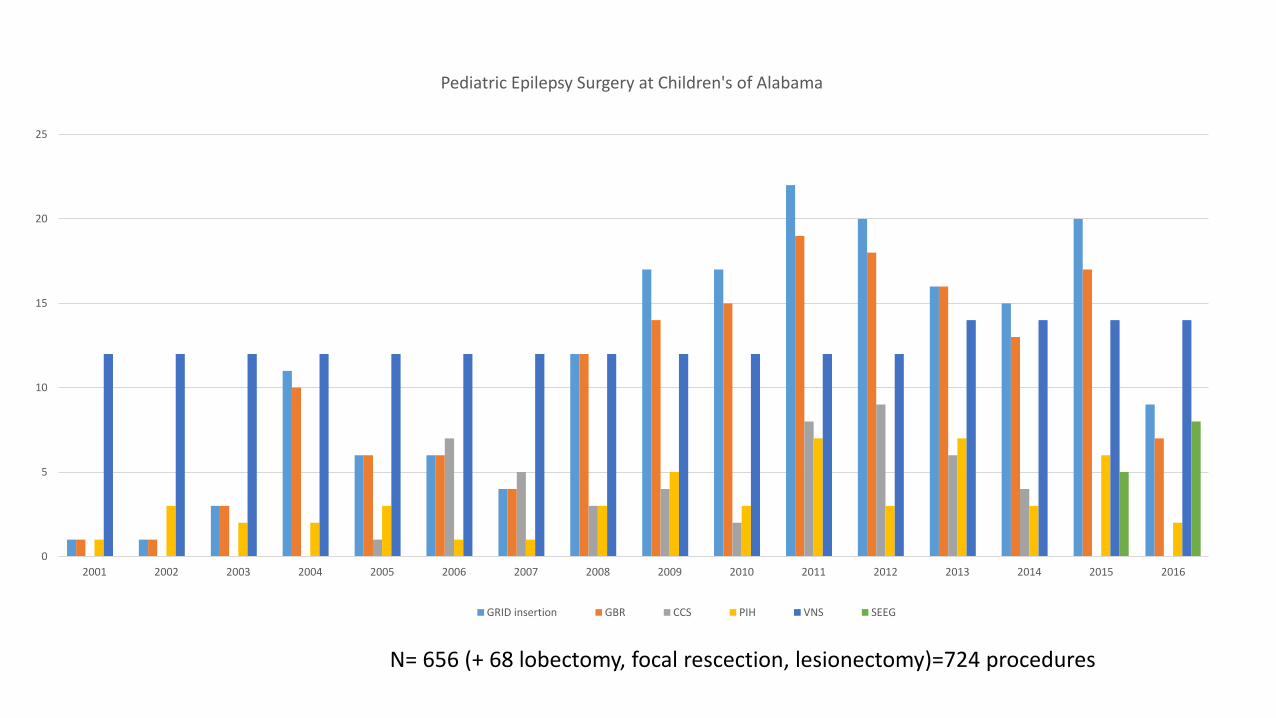
Pediatric Epilepsy Surgery at Children's of Alabama
GRID insertion GBR CCS PIH VNS SEEG
N= 656 (+ 68 lobectomy, focal rescection, lesionectomy)=724 procedures
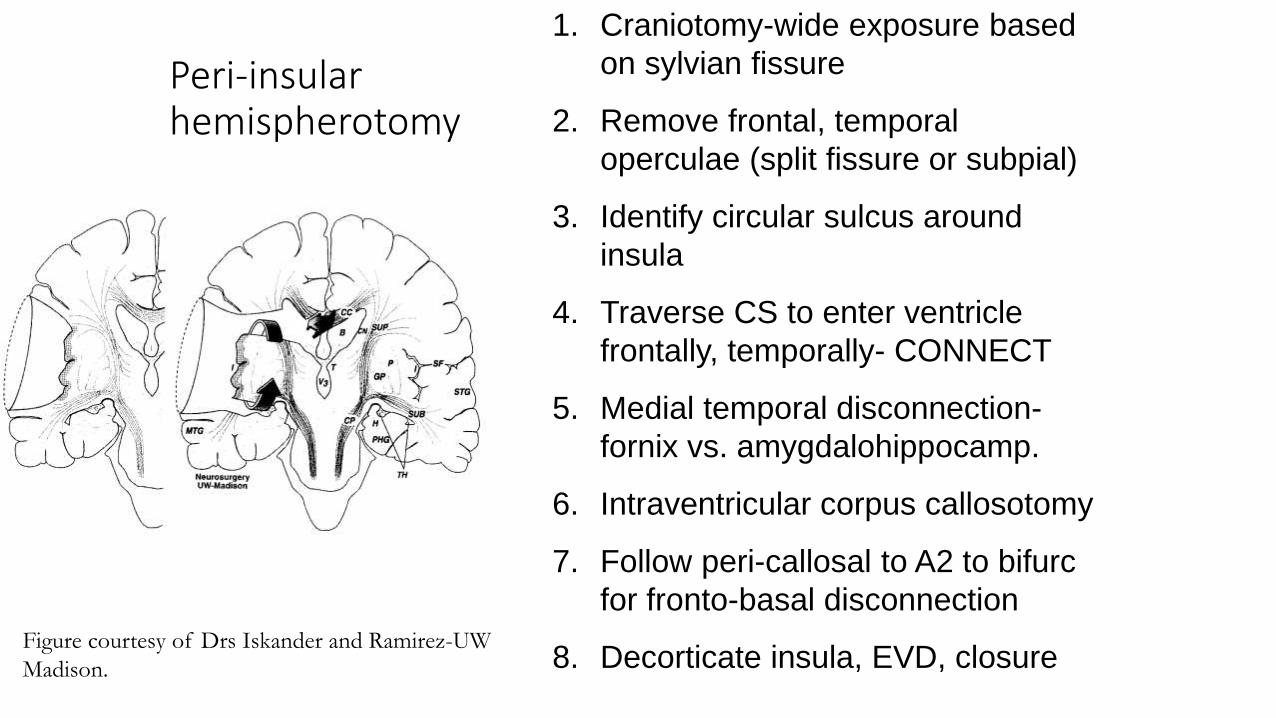
Peri-insular hemispherotomy
Figure courtesy of Drs Iskander and Ramirez-UW
Madison.
1. Craniotomy-wide exposure based
on sylvian fissure
2. Remove frontal, temporal
operculae (split fissure or subpial)
3. Identify circular sulcus around
insula
4. Traverse CS to enter ventricle
frontally, temporally- CONNECT
5. Medial temporal disconnection-
fornix vs. amygdalohippocamp.
6. Intraventricular corpus callosotomy
7. Follow peri-callosal to A2 to bifurc
for fronto-basal disconnection
8. Decorticate insula, EVD, closure
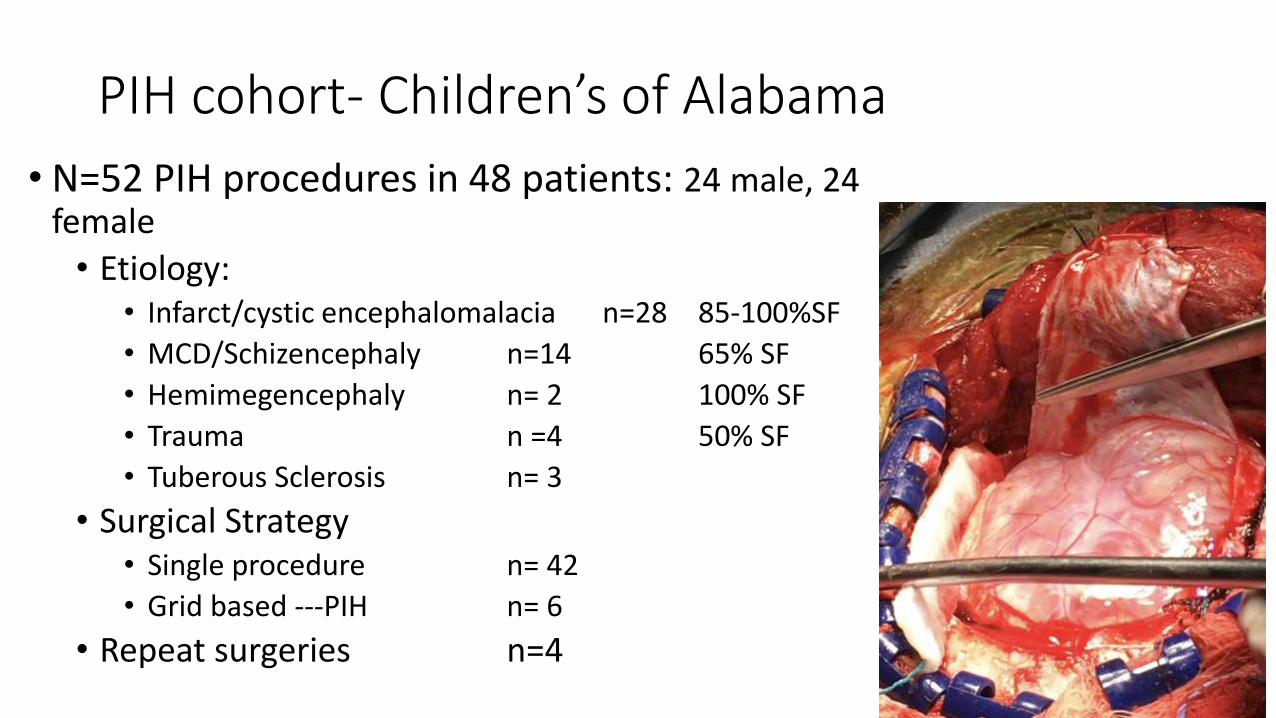
PIH cohort- Children’s of Alabama
• N=52 PIH procedures in 48 patients: 24 male, 24 female
• Etiology:• Infarct/cystic encephalomalacia n=28 85-100%SF
• MCD/Schizencephaly n=14 65% SF
• Hemimegencephaly n= 2 100% SF
• Trauma n =4 50% SF
• Tuberous Sclerosis n= 3
• Surgical Strategy• Single procedure n= 42
• Grid based ---PIH n= 6
• Repeat surgeries n=4
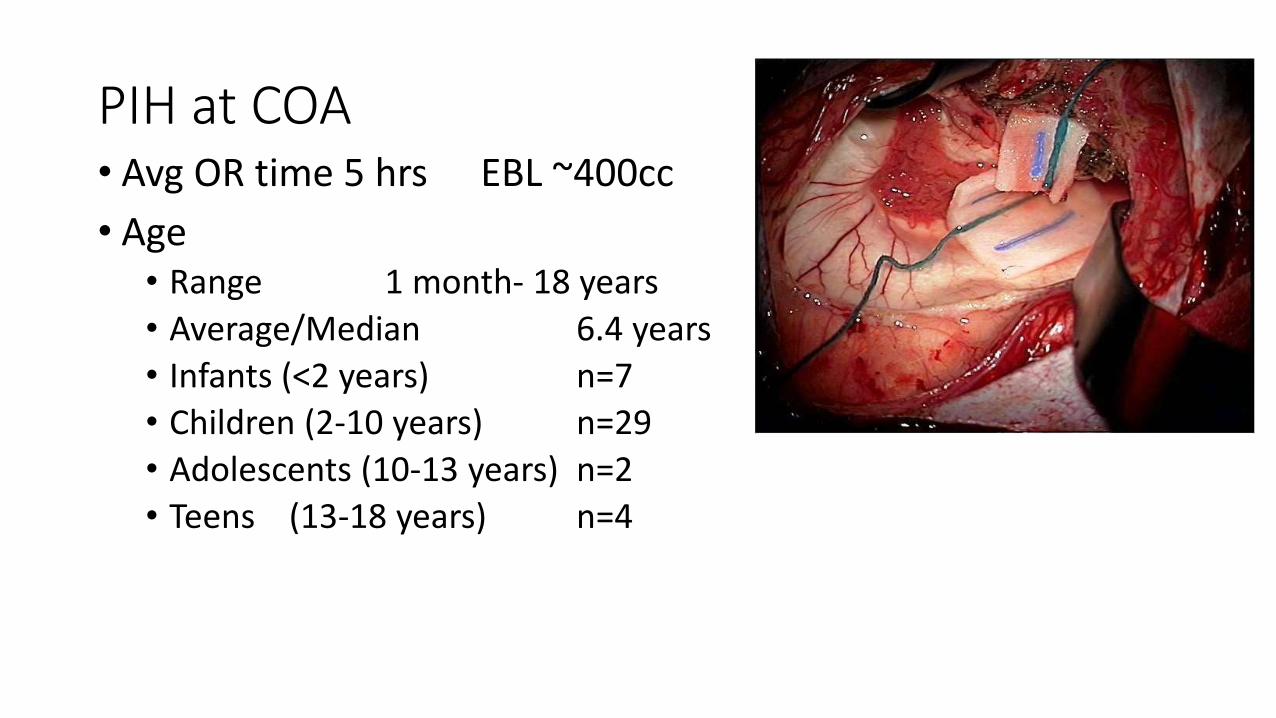
PIH at COA• Avg OR time 5 hrs EBL ~400cc
• Age• Range 1 month- 18 years
• Average/Median 6.4 years
• Infants (<2 years) n=7
• Children (2-10 years) n=29
• Adolescents (10-13 years) n=2
• Teens (13-18 years) n=4

PIH cohort- Children’s of Alabama
• Overall seizure freedom with PIH in purely Pediatric Series= 78%
• but for those patients who harbor single distribution stroke as etiology the SF rate= 100%
• No major morbidity or mortality in this series provided that hydrocephalus risk is carefully controlled (EVD, shunt)
Surgical Failure/Complications
• Peri-operative mortality• DL-12 female; emergent C-S (dec FHR, polyhydramios). Rett. Szr since 6 mos.
• Poorly localized in infancy (Miami). VNS.
• Poly pharmacy
• 3 seizure types (1-20/day); recent decline in control despite meds. Onfi and Benzil.
• Interictal: MF. Independent.
• Ictal: Variable. O1 broadly projecting
• Drops “as if she had been shot”-father
Surgical complications/failure-case-1
• Corpus callosotomy 7/24/12• Surgically uneventful• Progressively severe SE post CCS• Phenobarb coma for days• EEG - controversial; L propensity for ictal events
• Already has R hemiparesis• Declining without control
• Left PIH• Unrecognized intrustion to ambient/QG cistern• Midbrain contusion
• Never re-gained consciousness
CC Candidacy
• Generalized szr disorder with prominent DROP events• Tonic drops-bisynchrony causes hypertonia with resulting “falls like a tree”
• Atonic drops-bisychrony induces global loss of tone with resultant “falls like fainted”
• Lennox-Gastaut Syndrome• Progressive/profound MR characteristic EEG
• Medically refractile bi-frontal epilepsy• With or without intracranial electrodes for staged rsxn.
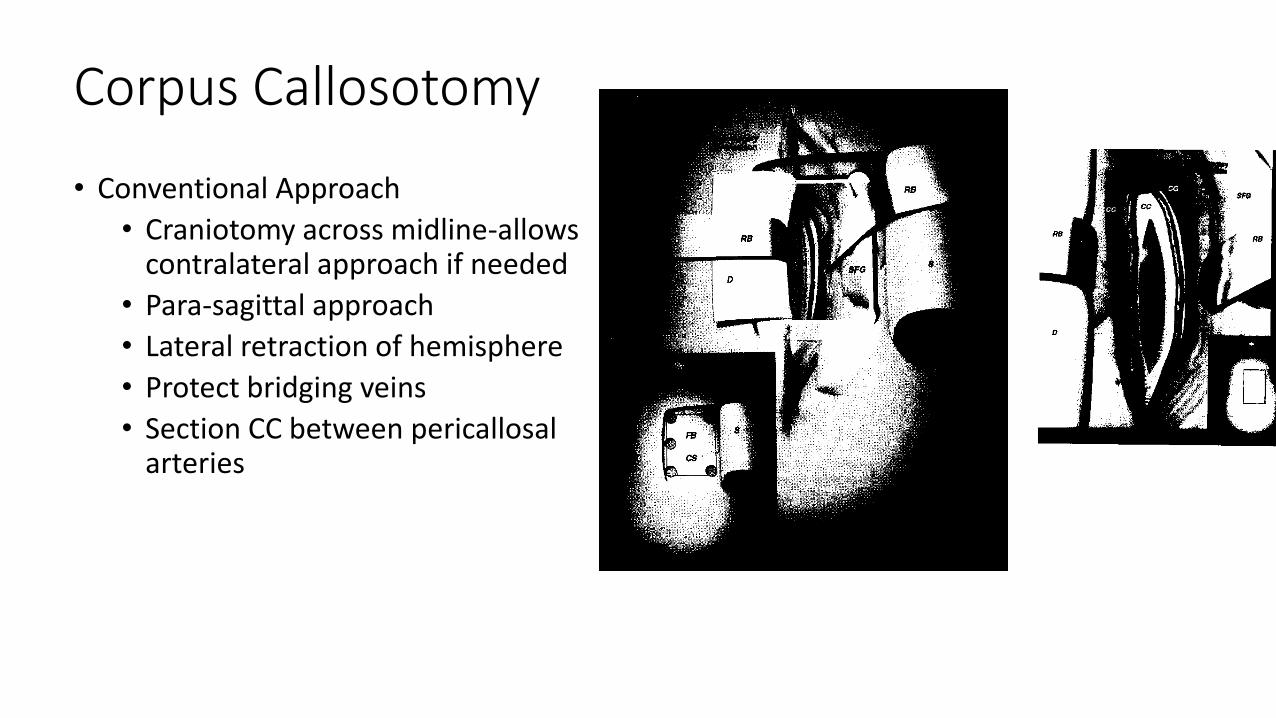
Corpus Callosotomy
• Conventional Approach
• Craniotomy across midline-allows contralateral approach if needed
• Para-sagittal approach
• Lateral retraction of hemisphere
• Protect bridging veins
• Section CC between pericallosal arteries
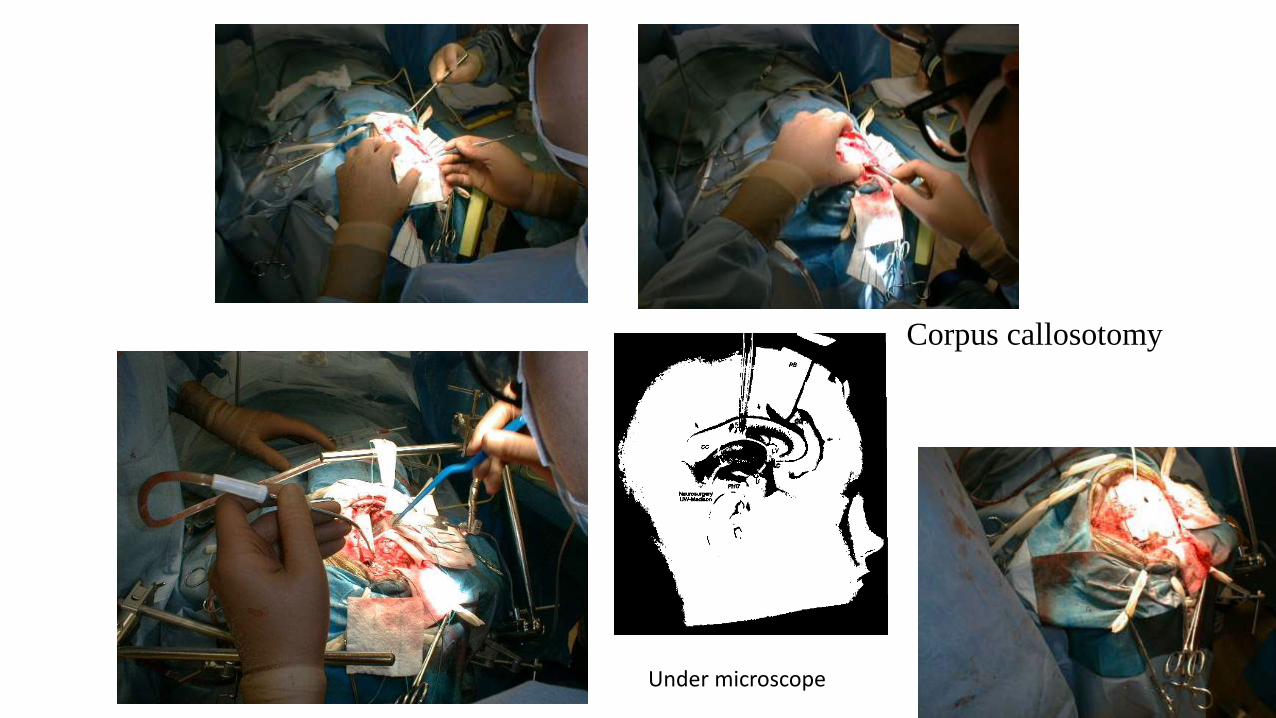
Corpus callosotomy
Under microscope
CCS- Shimuzu experience • Shimuzu et. al. Epilepsia 41 (Suppl 9)28-30, 2000.
• Retrospective -158 operations
• 29/34 with drops pre op seizure free post op
• 4/34 with drops pre-op have only infrequent post op events
• Maehara, Shimuzu Epilepsia 42 67-71, 2001.• Satisfactory outcome (>90% reduction sz) in
• 85% with drops
• 32% Generalized tonic
• 31% GTC
• Predictors: total callosotomy-freedom from drops; age- improved QOL
• Shimuzu Epilepsia 46 (Suppl 1) 30-31, 2005• Large single institution experience
• CCS highly effective for drops and psychomotor events
• Failure of desired callosal section most common cause for failure
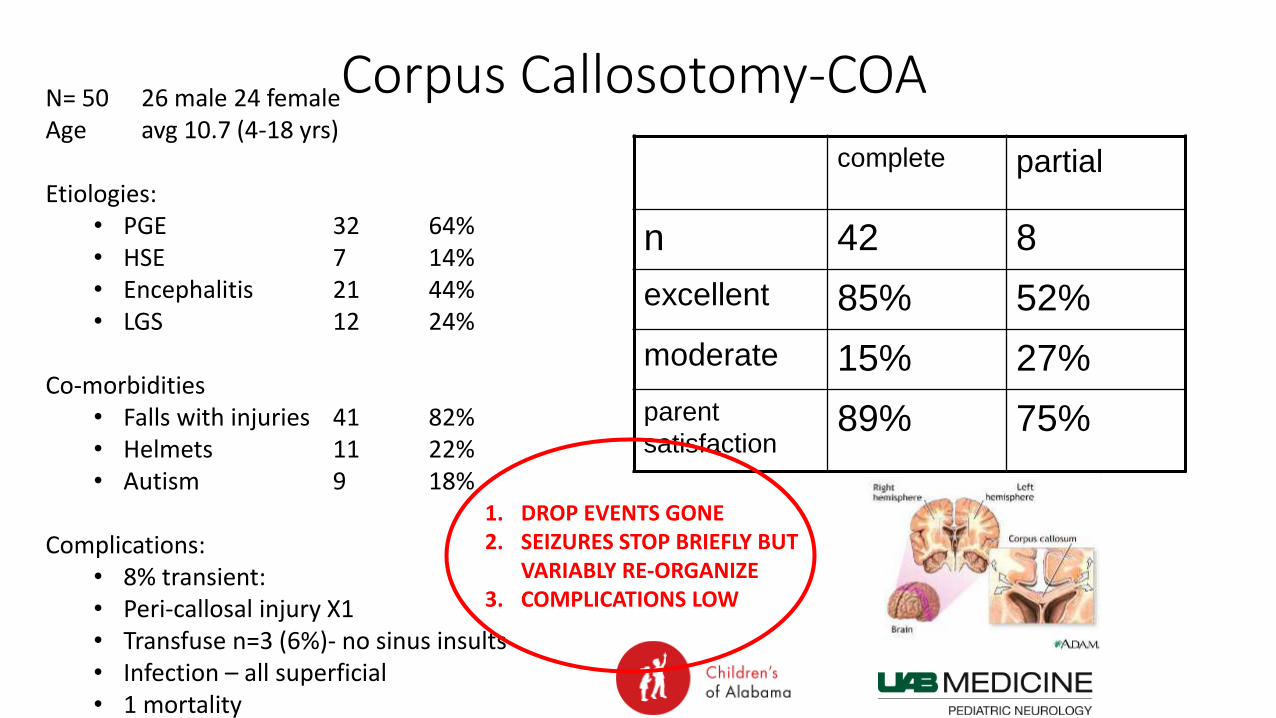
Corpus Callosotomy-COA
complete partial
n 42 8
excellent 85% 52%
moderate 15% 27%
parent
satisfaction89% 75%
N= 50 26 male 24 femaleAge avg 10.7 (4-18 yrs)
Etiologies:• PGE 32 64%• HSE 7 14%• Encephalitis 21 44%• LGS 12 24%
Co-morbidities• Falls with injuries 41 82%• Helmets 11 22%• Autism 9 18%
Complications:• 8% transient: • Peri-callosal injury X1• Transfuse n=3 (6%)- no sinus insults• Infection – all superficial• 1 mortality
1. DROP EVENTS GONE2. SEIZURES STOP BRIEFLY BUT
VARIABLY RE-ORGANIZE3. COMPLICATIONS LOW
BF• Age: 6 years old
• Handedness: Undetermined
• Seizure onset : 4 months of age
• Frequency: 10 clusters per day-multiple drops with injuries
• Duration: 5-10 seconds
• Birth History: full-term, normal delivery, no perinatal problem.
• Delayed development: she does not speak or follow commands, sits without assistance, can walk but not steadily.
• Current AEDs: Topiramate, Depakote
• Previous AEDs: ACTH, Oxcarbazepine, Lamotrigine, Valproate, Levetiracetam, Felbamate, Clonazepam
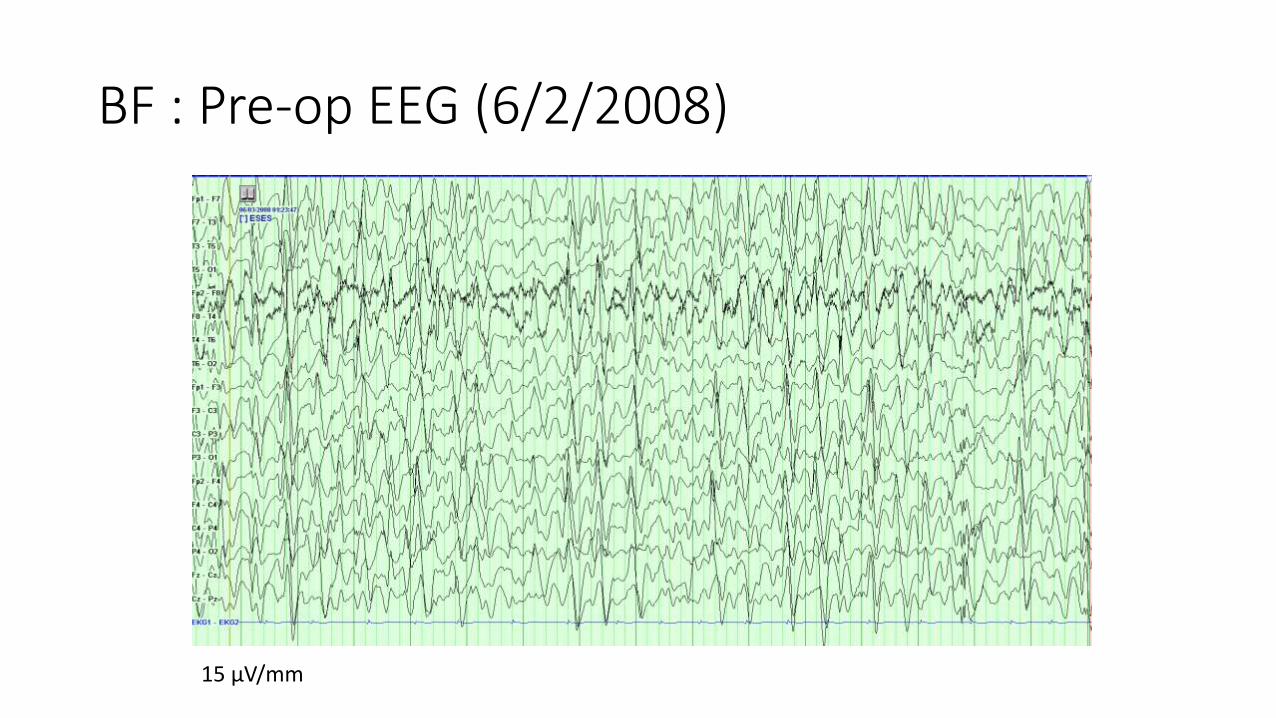
BF : Pre-op EEG (6/2/2008)
15 µV/mm
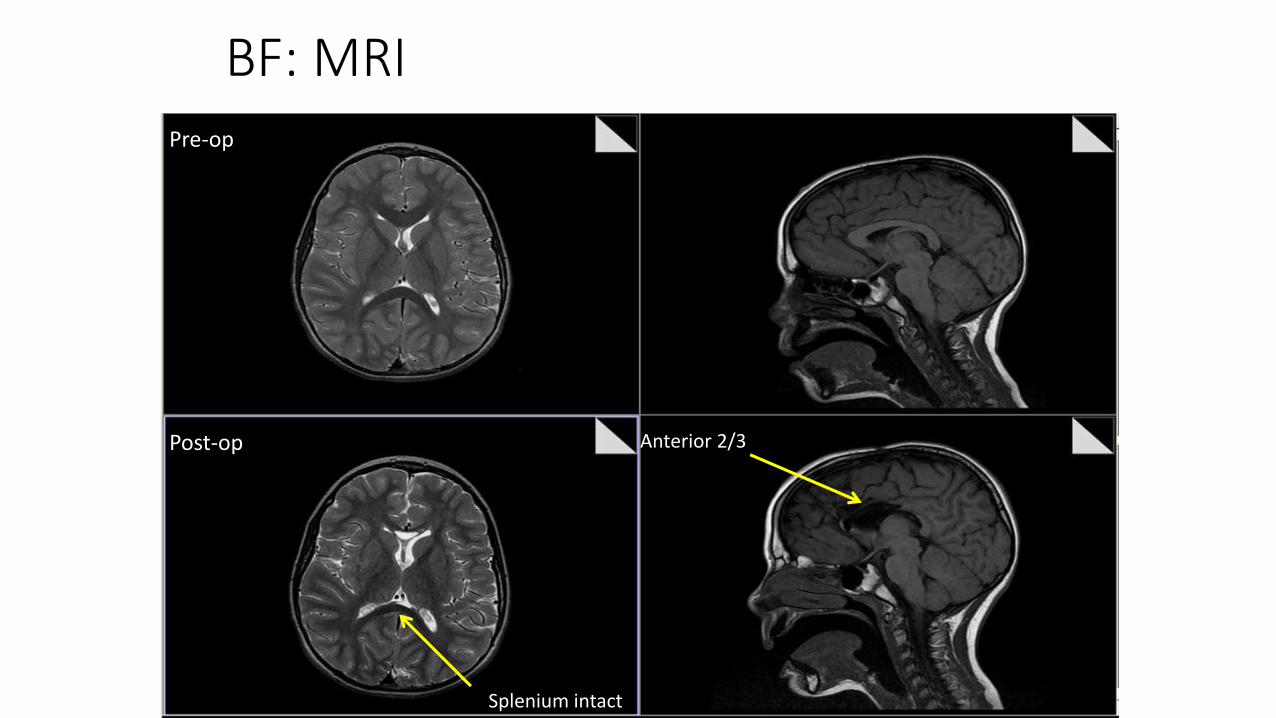
BF: MRIPre-op
Post-op
Splenium intact
Anterior 2/3
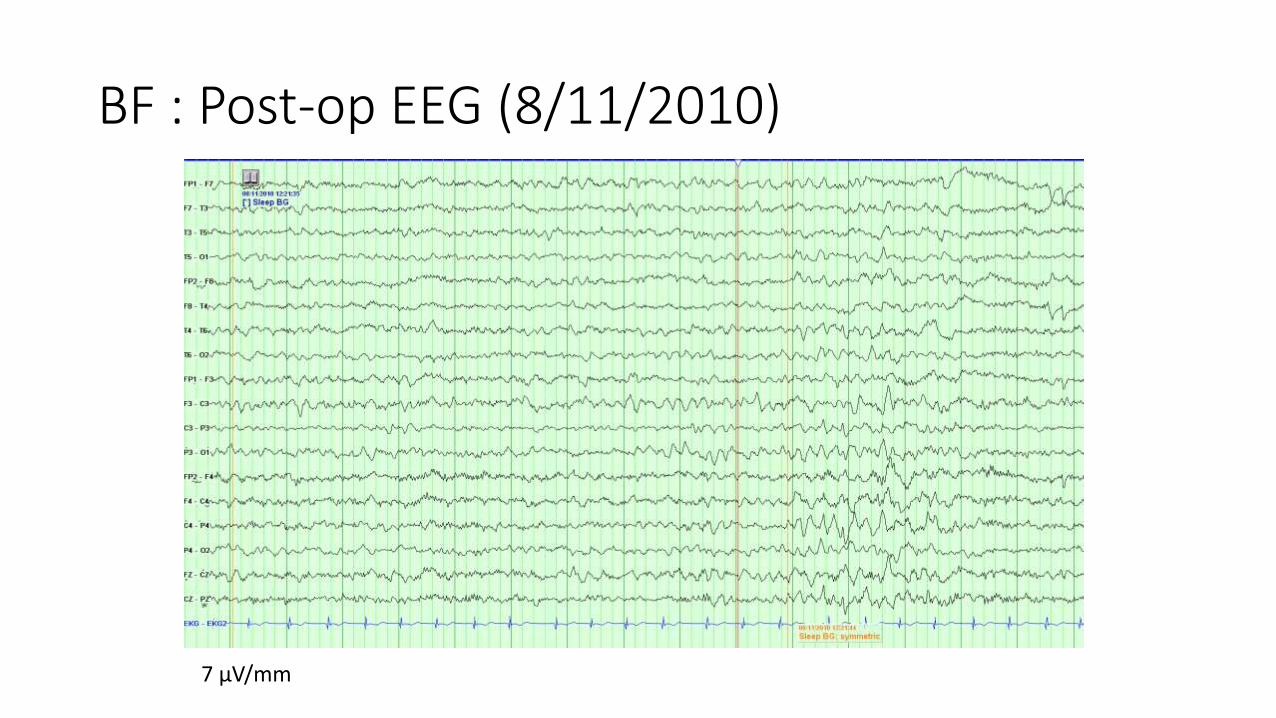
BF : Post-op EEG (8/11/2010)
7 µV/mm
BF
• Corpus callosotomy (6/12/2008)
• The last clinic follow-up (12/13/2010)
He had been free from epileptic spasm since surgery.
Conclusions• Epilepsy is a major World Public Health Issue
• Millions affected
• Extraordinary high burden of disease
• A major treatment gap exists on multiple fronts (PH, Med, Surg)• Access, awareness and overcoming social stigmas to gain access to care
• Medical• WHO campaign for diagnosis, support, AED access and affordability.
• Surgical- “Modest Proposal”• We must learn lessons from Lancet Commission on Surgery and not relegate surgery to
background role
• While some Epilepsy Surgery (IC-electrodes) prohibitively expensive an initial powerful armametarium might be:
• Lesional resection for parasitic infections
• PIH for hemispheric destructive lesions
• Corpus callosotomy for drop events
• ATL for partial-complex epilepsy in adults

MARCH 16-19, 2017 LOEWS CORONADO- SAN DIEGO, CALIFORNIA, USA
General Information: http://spinabifidaassociation.org/event/spina-bifida-world-congress/
Abstract deadline 10/31/16
Please follow this link to submit abstracts -
https://sbaworldcongress2017.abstractcentral.com/