Embed Size (px)
Citation preview
216 CALIFORNIA AND WESTERN MEDICINE Vol. XXII, No.5
narrow sharp chisel a triangular section of the nasalbones, with the base down, is removed from themedian line, and as much of the upper border ofthe septum as is necessary to obtain a correctedline of the bridge. The nasal bones are then frac-tured medialward, using a broadnosed hemostat. Theabove procedure accomplishes two things-the humpof the nose is removed, and the bridge is narrowed,avoiding the undesirable flattening and broadeningof the bridge obtained by the rasping operation andwhich is especially noticeable with an already broadnose. Moreover, the operation is accomplished ina thoroughly surgical manner, as all work is underthe operator's eye and, most important of all, thedanger of infection is minimized, as the nasal cavityis not entered at all. This avoids the necessity ofpacking, which is most uncomfortable to the patientand is attended with some danger, as it may favora sinusitis. The resulting scar at the base of thecolumella is practically negligible.A suggestion regarding cartilage for transplant
which some of you may have folowed, but whichwill bear repetition, is to bury the spare cartilagein the subcutaneous tissue of the abdominal wall.It remains there unchanged and obviates the painfulreoperation for obtaining a new piece, if by anychance the first graft should fail.For maintaining the alignment of a laterally dis-
located bridge after correction, I prefer to use acap splint on the upper incisors with a strong,springy wire extending outward and then upwardand terminating in a flattened vulcanite pad. Theamount and direction of the pressure applied canbe accurately controlled and can be easilv andquickly changed. The apparatus is light and com-fortable and, in my experience, is superior to aplaster mold or an ordinary metal splint, from thestandpoint of both the patient and surgeon.
Doctor de River (closing)-The technique used byPierce I think is very good. A similar technique, Ibelieve, has been described by Major Gillies of Eng-land, and more recently by J. D. Lewis of Minne-apolis in a recent number of the "Annals of Otol-ogy, Rhinology and Laryngology." The burying ofcartilage in the abdominal wall in cases where theremay be future use for the cartilage is advisable andis a custom that I have followed many times. Mel-linger mentions the fact that he always makes a castof the face before operating; this, too, has been ,aroutine procedure that I follow in all cases. I en-deavor to make a replica of the entire face beforeattempting any operative procedure; this enables meto study the case from all angles. On completion ofthe operation a recast is made.As to the choice of anesthesia I have not con-
sidered this question of great importance, perhapsbecause I have done such a large number of casesunder local anesthesia and feel that I can secureperfect anesthesia by the local method with aminimum of shock and risk to the patient. I quiteagree with Mellinger regarding the withdrawal ofthe graft after it has been introduced; the avoidanceof the practice lessens the chance of carrying infec-tion back into a sterile field. Forceps should un-questionably always be used when handling a graft.Too much cannot be said regarding the avoidanceof digital manipulation of the graft.Conclusion-In all cases surgical judgment, cou-
pled with an artistic temperament. and an anatomicalfamiliarity with the parts to be corrected, is the sinequa non of success. Whether using grafting bone,cartilage, or using celluloid as a supporting bridge,as suggested by some operators, matters not, pro-vided the operator possesses the skill and patiencerequired of all undertaking this type of surgery, forwhen the curtain falls at the grand finale the suc-cess of the performance is judged by one word, andthat is-results.
INFLUENCE OF PILLOW HABITS ONTHE DEVELOPMENT OF THE
UPPER JAW*By HARVEY STALLARD, D. D. S., San Diego.
INTRODUCTION
A common facial deformation, due principally topillow habits, is marked by a narrow upper jaw,a large mandible, a contracted palate, a narrownose, and a deflected nasal septum. Since the dentalarches and jaws form a great part of the face, thistype of defiormity has been designated by dentists as"narrowed upper jaw," "Gothic arch," "V-shaped"or "church roof" palate, etc. Faces having such oralfeatures are referred to as "dished," "bell," or "urn"faces. When the deformity is confined to one side,the cheek is flattened or depressed, making the faceseem twisted or "lop-jawed." The compression ofone maxilla makes the jaws appear to close cross-wise, hence the malocclusion is called a cross-bite.
OCCURRENCE OF THESE DEFORMITIES
"Dished" and "twisted" faces are often associatedwith impeded speech and disturbed nasal respirationso that they were probably noticed by observers ofearly times. However, earlier descriptions of oraLor facial deformations have been so brief and indefi-nite that it is impossible to determine whetherancient writers refer to these two types of progna-thism. Their greatest frequency has been in thecolder parts of the north temperate zone, occurringmore often among those of English descent. Theyare found among Italians, Brazilians, Australians,Chinese, Filipinos, Russians, and to a more limitedextent, perhaps, in all other civilized peoples.
THEORIES OF THEIR CAUSES
Idiocy and Heredity-The first medical writersto discuss causes of these two malformations be-lieved they were symptoms of idiocy (Downs: 1871 ;Ireland: 1874). This assumption was combated byKingsley (1879), who after examining many idiotsof different nationalities, said that idiots had nomore irregularities of teeth than any other class,and concluded that their oral deformities were dueto family traits.
Such malformations have been attributed to hered-ity because they are often traceable back in fam-ilies and in members of the same household maybe strikingly similar. The most popular doctrinetaught is that, through mixing of many races, a childwould inherit large teeth from one parent and smalljaws from another, or a small palate from one anda large mandible from the other. Another belief,once regarded as the most scientific, was that con-tracted palates and jaws -result from disturbedinnervation, neurosis, and evolutionary reversions(Talbot: 1903; Ballenger: 1911).
Rickets, Trauma, Mouth-breathing, and Endo-crine Disturbances Suggested-Rickets has been sug-gested as a cause by many writers (Bosworth: 1889;Ballenger: 1911), but it was early denied by Shaus(1887). Bosworth believes many contracted palateswere due to mouth-breathing, which, he imagined,was caused by partly occluded nostrils resulting
* Read before the San D)iego County Medical Society,May 22, 1923.
CALIFORNIA AND WESTERN MEDICINE
from inflammation following accidental trauma.Wallace, enlarging upon the influence of mouth-breathing and poor mastication, stated that constantmouth-breathing allows the tongue to lie in the floorof the mouth, away from the palate, so that its lat-eral influence is less than that of the cheeks; this, heclaimed, atrophies the upper jaw and overdevelopsthe lower, so that with poor mastication and infre-quent closure, the upper teeth and their alveol'arprocesses developed downward unrestrictedly, re-sulting in long teeth and the high, narrow palate.Recently, disturbed endocrine organs have been heldresponsible for oral deformities.
Mechanical Explanations of Their Developpment-Farrar (1888) believed a cross-bite was due toone of the following causes: (1) incorrect antagon-ism of teeth, (2) a too short ramus of the mandibleon one side, and (3) a faulty location of the glenoidfossa. Angle (1911) attributed the beginning ofthese deformations to the child sucking the cheekshabitually, but the development (1907) to the per-verted forces transmitted through the teeth.
Pillowing on the Face in Infancy Suggested-Marshall (1913), reporting correction of a badlydeflected nose, so often characterizing "twistedfaces," suggests pillowing on one side of the facein infancy as a cause. Case (1921) attributes de-velopment of cross-bites to infants lying and nurs-ing too much on one side of the face.The writer's attention was called to cross-bites
in 1918 by John C. McGuire, D. D. S., who sug-gested that they were caused by pillowing always onthe same side in infancy. In 1920 Angle suggestedas the cause the child's habit of pillowing its cheekon a hand. The same year Spencer Atkinson,D. D. S., reported a case in which he had observedthis method of pillowing to be a causal factor.
INVESTIGATION OF PILLOW HABITS
Location of the Work- This account is basedupon studies of several hundred subjects of South-ern California which were found in schools, pre-school clinics, industries, hospitals, homes, asylums,streets, private practices of Los Angeles and SanDiego.Method of Investigating-At first the writer re-
lied on what the patients said about their methodof pillowing. Among the first patients examinedwas one having a much contracted palate. Hismother said he always slept on his abdomen, keep-ing his fists under the pillow with the knuckles up-ward and resting his cheeks alternately on themounds made in the pillow. On each side, thearrangement of his upper teeth showed the imprintof his knuckles. Other patients having cross-bitesadmitted pillowing their cheeks most of the nighton a hand or arm. When a parent did not discoverthe habit, a visit was paid the child's bedside. Themost convincing evidence was obtained by studyingsleeping children. Subjects having nearly normaljaws do not have these pillow habits.
General Evidence-The main fact to interest thewriter in these two types of malformations wastheir frequent return to former conditions evenwhen treated by the best of orthodontists. Correc-
tist working unaware of the habit; when it is dis-continued treatment is rapid. No matter how welltreated and mechanically retained, the teeth willreturn to their former alignment if the habit is notstopped, but where it is broken the treatment issuccessful.
It is possible to identify these malocclusions bythe contour of the faces, to diagnose pillowing habitsby the arrangement of the teeth, and to predict thekind of deformity by knowing the habitual malposi-tion of the face during sleep.
Origin of Wrong Pillow Habits-Many historiesshow that a child, when compelled to lie for a longtime on one side, on account of an abscess, injuryor burn on the other side of the body, will vary hisposition to obtain rest and will occasionally put thehand between the cheek and pillow. Some beganthe habit during long attacks of pneumonia andpleurisy. The habit is sometimes associated withsucking of thumbs or fingers. A patient having abilaterally constricted palate started the habit afterbecoming bedfast through infantile paralysis. Awoman suffering in early childhood from conjunc-tivitis, procured most comfort during the day byburying the forehead and eyes in a large pillow; byresting the cheeks on her hands, she preventedsmoothering, but started the habit.
Its beginning cannot always be traced to an ill-ness, abscess, burn, or injury, or even to a changein bedding or position of the bed. Some attributeits commencement to face-pillowing initiated by par-ent or nurse. The following shows how open tosuggestion a child is: One day a child was shownsome photographs of children pillowing their faceson their hands; she was impressed and began thehabit, which her mother stopped only by determinedefforts.
It is impossible to find a constant relation betweenthe effects of these habits and rachitis and, con-versely, evidence that rachitic children are predis-posed to such habits. When they appear in mem-bers of a family, those affected have similar pil-low habits. It seems reasonable that the habit ishanded down by instruction or imitation, ratherthan through heredity.
Observations on the Development of the Habit-Some infants who habitually sleep on their bellieshave shown marked effects of pillowing on thehands. Older children and many adults, amongthem several dentists, with more pronounced mal-formations, observed while asleep, were found pil-lowing on their hands or arms. The most typicalV-shaped palate found was in a physician who sleepson the abdomen, resting his cheeks alternately uponmounds in the pillow made by his arms, one ofwhich he keeps under the pillow at a time. Whenhe was a child a dentist tried to expand his upperjaw by transverse jackscrews, but so much pain was
caused at night that treatment was abandoned.Men of 65 or more having cross-bites were foundpillowing on one side as in infancy. These habitsoriginate early in life amid many different condi-tions, continue often through adolescence and intoadvanced age; in only a few did the habit startafter the twelfth year.
tive treatment is often prolonged by the orthodon-
May, 1924 217
The Inertia and Nature of the Habit -Many
CALIFORNIA AND WESTERN MEDICINE
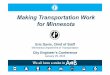
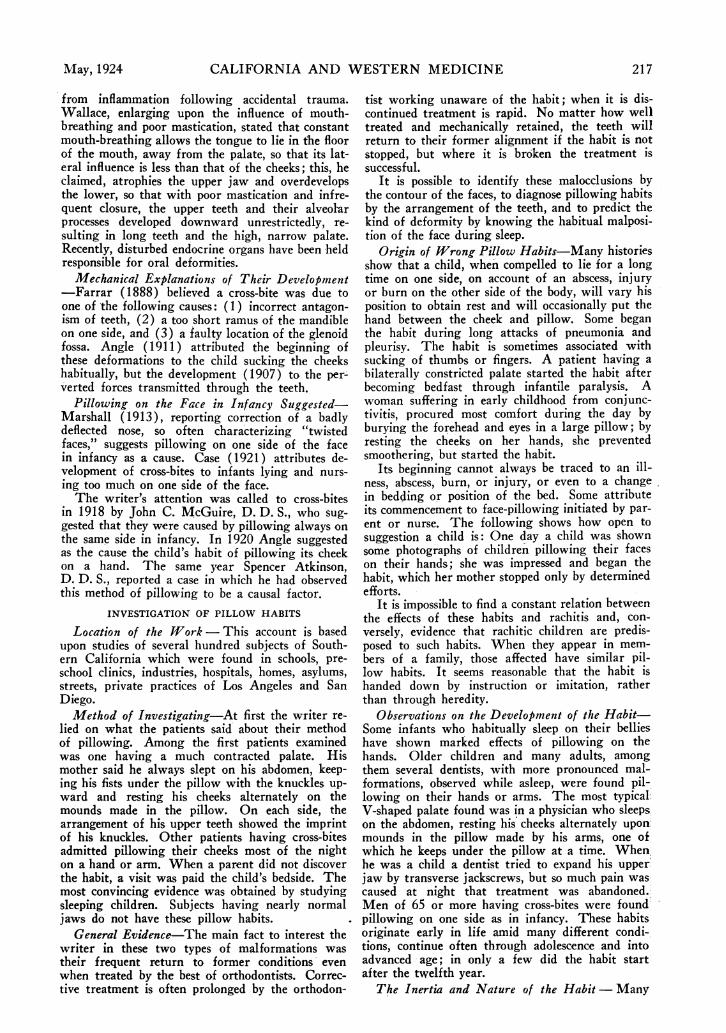
Figure 1--A typical cross-bite, unilateral constriction of the upper jaw.
times while studying sleeping children the writertried to make them rest directly on the pillow, butno matter how sound asleep, they resist change andreplace the hand to its habitual position. Whentold, while awake but unaware that they are beingexperimented upon, to lie first on one side and thenon the other, their habitual pillowing habits domi-nate. Patients lying on the normal side, when toldto turn over quickly, usually select the habitual pil-lowing method, automatically placing beneath thedeformed cheek the preferred arm or hand. Com-fort for these patients is obtained by indulging thehabit; on requiring discontinuance of the habit, dis-comfort and a few sleepless nights. will be expe-rienced before they become adapted to new positions.Since pillowing is comfortable and habitual, it hasgreat inertia.Amount of Force and Length of Time It Acts-
Children are in bed fully half of their lives; if theylie on their faces much, development of the jawswill be repressed. Any small constant external forcewill in time produce damaging imbalance in such acomplicated organ as the mouth. But we have herea force, derived from the weight of the head, act-ing on the plastic bones of childhood throughout thegreater part of each twenty-four hours, and, as casehistories show, many children suffering from thesedeformations have been confined to bed for longerperiods during which the force has continued for a
greater time. It is well known that a letter-carrier'sspine becomes deformed by carrying bundles con-stantly on the same shoulder. Similarly, facial de-pressions may be developed by pillowing the facehabitually upon hard objects.Normal Breathing and Vigorous Mastication In-
sufficient-If a normal breather pillows alternatelyon his right and left arms, he may have both dentalarches narrowed, or if infants rest habitually onjust pillows, their deciduous dental arches will benarrowed and their permanent anterior teeth will berotated and "bunched." Parents have been knownto give their children hard foods, remove their ton-sils and adenoids, taking every precaution to avoidmalocclusion except preventing face-pillowing, yettheir children have narrowed dental arches andcroWded anterior teeth, due principally to pillowhabits.When teeth are fully erupted and interdigitate
normally, the tongue, filling the mouth cavity,presses outward on them, the alveolar processes andthe palate, while the lips and cheeks bind the struc-tures on the outside, preventing too great expansion.If the mouth be closed most of the time, or duringswallowing, so that the opposing cusps interlock, themuscles of mastication and the hyoid muscles keepthe lower jaw in position, indirectly protecting theupper dental arch against pillowing. While pillowhabits damage the normal arrangement of teeth,
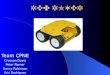
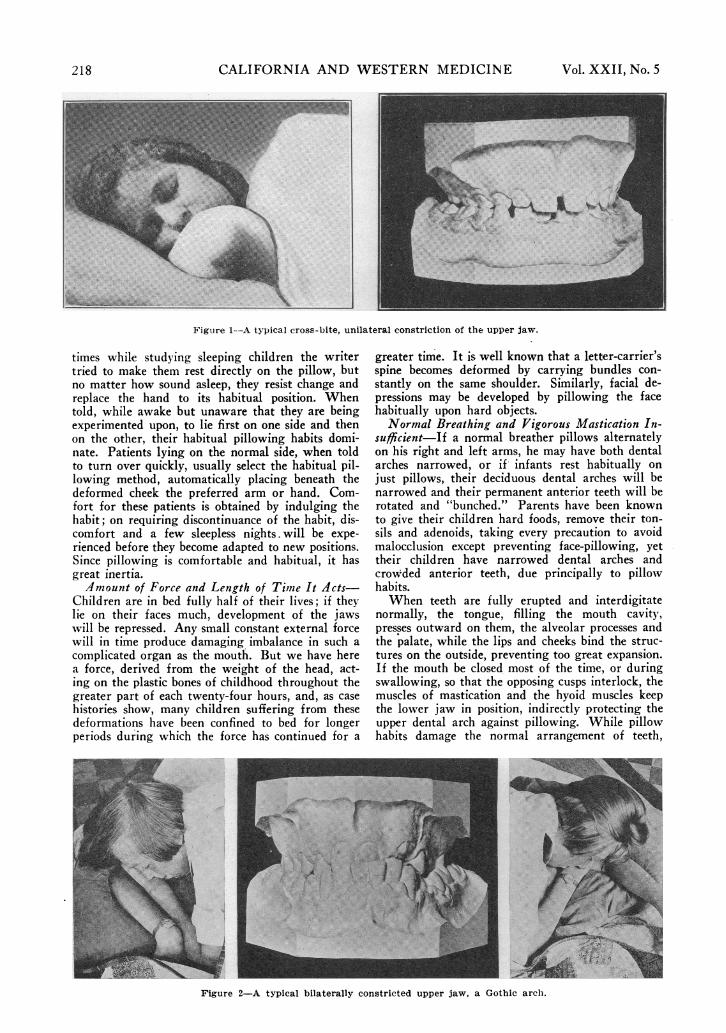
Figure 2-A typical bilaterally constricted upper jaw, a Gothic arch.
iA
218 Vol. XXII, No. 5
CALIFORNIA AND WESTERN MEDICINE
.......b >
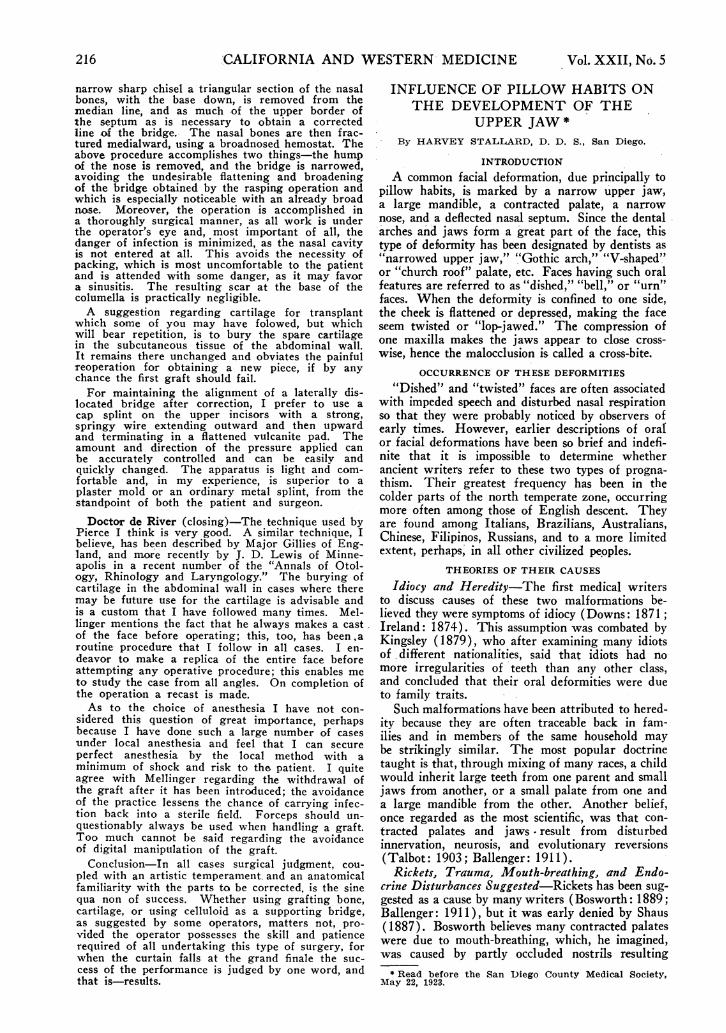
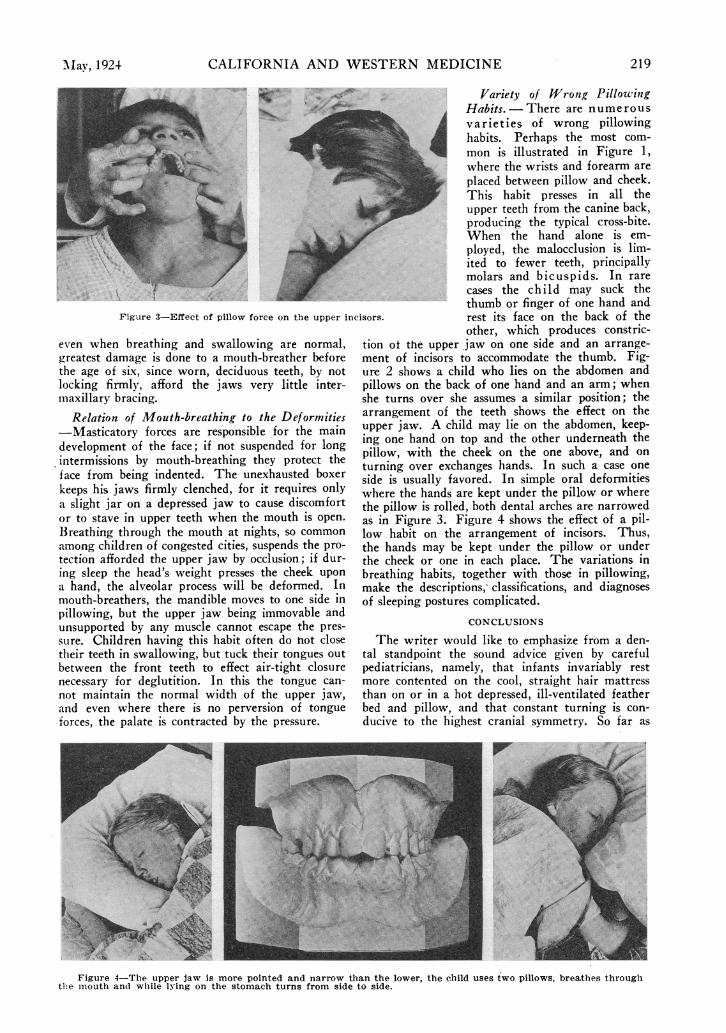
Figure 3-Effect of pillow force on the upper inc
even when breathing and swallowing are normal,
greatest damage is done to a mouth-breather before
the age of six, since worn, deciduous teeth, by not
locking firmly, afford the jaws very little inter-
miaxillary bracing.
Relation of Mouth-breathing to the Deformities
-Masticatory forces are responsible for the main
development of the face; if not suspended for long
intermissions by mouth-breathing they protect the
face from being indented. The unexhausted boxer
keeps his jaws firmly clenched, for it requires only
a slight jar on a depressed jaw to cause discomfort
or to stave in upper teeth when the mouth is open.
Breathing through the mouth at nights, so common
among children of congested cities, suspends the pro-
tection afforded the upper jaw by occlusion; if dur-
ing sleep the head's weight presses the cheek upon
a hand, the alveolar process will be deformed. In
mouth-breathers, the mandible moves to one side in
pillowing, but the upper jaw being immovable and
unsupported by any muscle cannot escape the pres-
sure. Children having this habit often do not close
their teeth in swallowing, but tuck their tongues out
between the front teeth to effect air-tight closure
necessary for deglutition. In this the tongue can-
not maintain the normal width of the upper jaw,and even where there is no perversion of tongue
forces, the palate is contracted by the pressure.
Variety of Wrong PillowingHabits.-There are numerousvarieties of wrong pillowinghabits. Perhaps the most com-mon is illustrated in Figure 1,where the wrists and forearm areplaced between pillow and cheek.This habit presses in all theupper teeth from the canine back,producing the typical cross-bite.When the hand alone is em-ployed, the malocclusion is lim-ited to fewer teeth, principallymolars and bicuspids. In rarecases the child may suck thethumb or finger of one hand andrest its face on the back of theother, which produces constric-
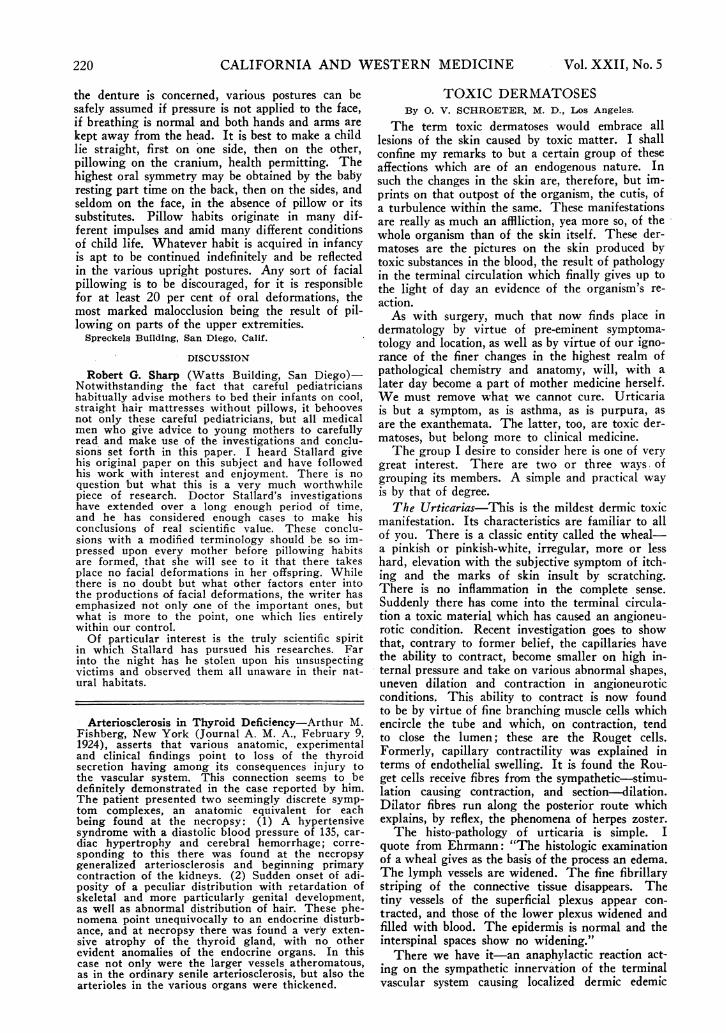
tion ot the upper jaw on one side and an arrange-ment of incisors to accommodate the thumb. Fig-ure 2 shows a child who lies on the abdomen andpillows on the back of one hand and an arm; whenshe turns over she assumes a similar position; thearrangement of the teeth shows the effect on theupper jaw. A child may lie on the abdomen, keep-ing one hand on top and the other underneath thepillow, with the cheek on the one above, and onturning over exchanges hands. In such a case oneside is usually favored. In simple oral deformitieswhere the hands are kept under the pillow or wherethe pillow is rolled, both dental arches are narrowedas in Figure 3. Figure 4 shows the effect of a pil-low habit on the arrangement of incisors. Thus,the hands may be kept under the pillow or underthe cheek or one in each place. The variations inbreathing habits, together with those in pillowing,make the descriptions, classifications, and diagnosesof sleeping postures complicated.
CONCLUSIONS
The writer would like to emphasize from a den-tal standpoint the sound advice given by carefulpediatricians, namely, that infants invariably restmore contented on the cool, straight hair mattressthan on or in a hot depressed, ill-ventilated featherbed and pillow, and that constant turning is con-ducive to the highest cranial symmetry. So far as
.,ri.
Figure 4-The upper jaw is more pointed and narrow than the lower, the child uses two pillows, breathes throughthe m-louth ancd while lying on the stomach turns from side to side.
.'NIav, 1924 219
220 CALIFORNIA AND WESTERN MEDICINE Vol. XXII, No.5
the denture is concerned, various postures can besafely assumed if pressure is not applied to the face,if breathing is normal and both hands and arms arekept away from the head. It is best to make a childlie straight, first on one side, then on the other,pillowing on the cranium, health permitting. Thehighest oral symmetry may be obtained by the babyresting part time on the back, then on the sides, andseldom on the face, in the absence of pillow or itssubstitutes. Pillow habits originate in many dif-ferent impulses and amid many different conditionsof child life. Whatever habit is acquired in infancyis apt to be continued indefinitely and be reflectedin the various upright postures. Any sort of facialpillowing is to be discouraged, for it is responsiblefor at least 20 per cent of oral deformations, themost marked malocclusion being the result of pil-lowing on parts of the upper extremities.Spreckels Building, San Diego, Calif.
DISCUSSION
Robert G. Sharp (Watts Building, San Diego)-Notwithstanding the fact that careful pediatricianshabitually advise mothers to bed their infants on cool,straight hair mattresses without pillows, it behoovesnot only these careful pediatricians, but all medicalmen who give advice to young mothers to carefullyread and make use of the investigations and conclu-sions set forth in this paper. I heard Stallard givehis original paper on this subject and have followedhis work with interest and enjoyment. There is noquestion 'but what this is a very much worthwhilepiece of research. Doctor Stallard's investigationshave extended over a long enough period of time,and he has considered enough cases to make hisconclusions of real scientific value. These conclu-sions with a modified terminology should be so im-pressed upon every mother before pillowing habitsare formed, that she will see to it that there takesplace no facial deformations in her offspring. Whilethere is no doubt but what other factors enter intothe productions of facial deformations, the writer hasemphasized not only one of the important ones, butwhat is more to the point, one which lies entirelywithin our control.Of particular interest is the truly scientific spirit
in which Stallard has pursued his researches. Farinto the night has he stolen upon his unsuspectingvictims and observed them all unaware in their nat-ural habitats.
Arteriosclerosis in Thyroid Deficiency-Arthur M.Fishberg, New York (Journal A. M. A., February 9,1924), asserts that various anatomic, experimentaland clinical findings point to loss of the thyroidsecretion having among its consequences injury tothe vascular system. This connection seems to bedefinitely demonstrated in the case reported by him.The patient presented two seemingly discrete symp-tom complexes, an anatomic equivalent for eachbeing found at the necropsy: (1) A hypertensivesyndrome with a diastolic blood pressure of 135, car-diac hypertrophy and cerebral hemorrhage; corre-sponding to this there was found at the necropsygeneralized arteriosclerosis and beginning primarycontraction of the kidneys. (2) Sudden onset of adi-posity of a peculiar distribution with retardation ofskeletal and more particularly genital development,as well as abnormal distribution of hair. These phe-nomena point unequivocally to an endocrine disturb-ance, and at necropsy there was found a very exten-sive atrophy of the thyroid gland, with no otherevident anomalies of the endocrine organs. In thiscase not only were the larger vessels atheromatous,as in the ordinary senile arteriosclerosis, but also thearterioles in the various organs were thickened.
TOXIC DERMATOSESBy 0. V. SCHROETER, M. D., Los Angeles.
The term toxic dermatoses would embrace alllesions of the skin caused by toxic matter. I shallconfine my remarks to but a certain group of theseaffections which are of an endogenous nature. Insuch the changes in the skin are, therefore, but im-prints on that outpost of the organism, the cutis, ofa turbulence within the same. These manifestationsare really as much an afflliction, yea more so, of thewhole organism than of the skin itself. These der-matoses are the pictures on the skin produced bytoxic substances in the blood, the result of pathologyin the terminal circulation which finally gives up tothe light of day an evidence of the organism's re-action.As with surgery, much that now finds place in
dermatology by virtue of pre-eminent symptoma-tology and location, as well as by virtue of our igno-rance of the finer changes in the highest realm ofpathological chemistry and anatomy, will, with alater day become -a part of mother medicine herself.We must remove what we cannot cure. Urticariais but a symptom, as is asthma, as is purpura, asare the exanthemata. The latter, too, are toxic der-matoses, but belong more to clinical medicine.The group I desire to consider here is one of very
great interest. There are two or three ways ofgrouping its members. A simple and practical wayis by that of degree.The Urticarias-This is the mildest dermic toxic
manifestation. Its characteristics are familiar to allof you. There is a classic entity called the wheal-a pinkish or pinkish-white, irregular, more or lesshard, elevation with the subjective symptom of itch-ing and the marks of skin insult by scratching.There is no inflammation in the complete sense.Suddenly there has come into the terminal circula-tion a toxic material which has caused an angioneu-rotic condition. Recent investigation goes to showthat, contrary to former belief, the capillaries havethe ability to contract, become smaller on high in-ternal pressure and take on various abnormal shapes,uneven dilation and contraction in angioneuroticconditions. This ability to contract is now foundto be by virtue of fine branching muscle cells whichencircle the tube and which, on contraction, tendto close the lumen; these are the Rouget cells.Formerly, capillary contractility was explained interms of endothelial swelling. It is found the Rou-get cells receive fibres from the sympathetic-stimu-lation causing contraction, and section-dilation.Dilator fibres run along the posterior route whichexplains, by reflex, the phenomena of herpes zoster.The histo-pathology of urticaria is simple. I
quote from Ehrmann: "The histologic examinationof a wheal gives as the basis of the process an edema.The lymph vessels are widened. The fine fibrillarystriping of the connective tissue disappears. Thetiny vessels of the superficial plexus appear con-tracted, and those of the lower plexus widened andfilled with blood. The epidermis is normal and theinterspinal spaces show no widening."There we have it-an anaphylactic reaction act-
ing on the sympathetic innervation of the terminalvascular system causing localized dermic edemic