Embed Size (px)
Citation preview

CalHEN 2.0 A Look at What Has Been Accomplished:
A Perspective on Improvement
September 21, 2016
CalHEN 2.0 Wrap-Up Event
Beth Rowett, MA, MHA, CPHQ Executive Director Performance Improvement

Beth Rowett, Executive Director, Performance Improvement
Fatemeh Kiani, Director, Hospital Quality Intelligence Initiative
Kim Werkmeister, Clinical Improvement Educator
Lindsay Stowe, Clinical Improvement Advisor
Lynn Forsey, Clinical Improvement Advisor
Martha Ackman, Clinical Improvement Advisor
Noga Yaniv, Performance Data Analyst
Sara Bader, Clinical Improvement Advisor
Scott Masten, Senior Biostatistician
Shweta Krishnan, Program Coordinator
CalHEN 2.0 Team Members

HEN 1.0 36-month to reduce all-cause preventable inpatient harm by 40% and 30-day readmissions by 20% • 2011-2014 three-year initiative funded by CMS
• AHA/HRET HEN contributed to improve care in ten clinical areas resulting in 69,000 patients who had harm prevented and an estimated cost savings of over $200 million across 30 states
• CalHEN reduced harm in 8,994 lives and saved 60 million in dollars
• Highlights from 148 hospitals in CalHEN 1.0 include: o 65% reduction of Birth Trauma
o 58% reduction in Pressure Ulcers
o 44% reduction of Early Elective Deliveries
o 44% reduction of Preventable VTE
o 28% reduction in Falls with Injury
o 16% reduction in CLABSI

CalHEN 2.0 - Topics
Core Topics with Performance Metrics 1. Adverse Drug Events 2. CAUTI 3. CLABSI 4. EED/OB Harm 5. Falls 6. Pressure Ulcers 7. SSI 8. VAE 9. VTE 10. Readmissions
Additional Topics with Performance Metrics 1. Sepsis 2. C. difficile Crosscutting Areas of Focus 1. Patient and Family
Engagement 2. Health Care Disparities 3. Leadership and Governance
CalHEN hospitals work on all 10 Core Topics, C.diff and Sepsis

• Needs Assessment for every hospital • Two Site Visits for every hospital • Required Data Submission Completed: 149 CalHEN 2.0
hospitals (84%)
CalHEN 2.0 - Highlights
Webinars: • 19 ENGAGE! Webinars • National Patient Safety Awareness Week (2
webinars) • PfP 2.0 Measurement Affinity Group Case
Study: CalHEN Actionable Report • C. difficile and Antimicrobial Stewardship
with Dr. Kalvin Yu • Patient Falls Coaching Series (5 webinars) • VTE Webinar with Dr. Jenkins • ADE Webinar with HSAG • Readmissions Webinar
In-Person Events: • ENGAGE! Kickoffs, Southern and
Northern California • HCRO Kickoffs, Southern and Northern
California • Patient Falls Workshop with Pat
Quigley, Northern and Southern California
• IHI Model for Improvement Workshop, Southern and Northern California
• CalHEN CPHQ Training in Sacramento • CalHEN CPPS Training in Newport
Beach

6

7

LMS Foundations Course
Organizational Reliability
System Reliability
How the World works
Human reliability
8

Learning Management System (LMS) • Available to all staff of CalHEN Member Hospitals at no
cost until March 2017
• Efficient – under 2 hours
• Reverse Classroom – Learning Individualized – Application in a Group
• English and Spanish – with more languages to be
added as needed
• Accessible – Mobile Phone, Laptop, Desktop
9

Questions?
10

HEN 2.0 Overview
• 12 month initiative funded by CMS, with the goal of a 40% reduction in harm and a 20% reduction in avoidable readmissions
• AHA/HRET HEN contributed to improving care in eleven clinical areas, resulting in 26,883 patients who had harm prevented and an estimated cost savings of almost $200 million across 34 states
• CalHEN 2.0 prevented 800 harm events representing an estimated savings of over $2 million.
• Highlights from 179 hospitals in CalHEN 2.0 include: o 65% reduction of Early Elective Deliveries
o 19.7% reduction in Obstetric Trauma
o 15% reduction in VTE
o 12.6% reduction in Ventilator-Associated Events
o 10.6% reduction in Falls with Injury
Source: HRET October 2015 – May 2016

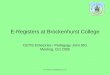
CalHEN 2.0 Average Rate Reduction for March-May 2016 (from Baseline)
Bett
er
Color CodeMet 40% Reduction GoalReduction <40%Got worse
Source: HRET October 2015 – May 2016
ADE
Comp
CDI SSI
CompositeReadmissio..
CLABSI CAUTIFalls with
Injury VAE VTEPrU (2)
OB Harm 2
Overall SepsisEED
-100.0%
-80.0%
-60.0%
-40.0%
-20.0%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%Re
-29.1%
-10.0%
51.1%
65.1%
10.6% 12.6%15.1%
18.0% 19.7%
-8.2%-2.5%
1.4% 3.9%

Early Elective Deliveries (EED)
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero
Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
EED 47 28 1 19 97
1.64
1.77 2.59
1.16
1.38 1.44 0.99 1.23
1.55
Baseline
Target
0.00
1.00
2.00
3.00
4.00
5.00
6.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
Early elective deliveries
Source: HRET October 2015 – June 2016
Rate

3rd and 4th Degree Lacerations in Vaginal Deliveries
14.36 13.81 14.16 13.33 12.91 15.22 14.11
15.67 15.19 Baseline
Target
0.00
5.00
10.00
15.00
20.00
25.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
OB Trauma - Vaginal Delivery without Instrument (per 1,000 patients)
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
OB Harm 48 11 9 37 105
Source: HRET October 2015 – June 2016
Rate

Post-Op Venous Thromboembolism (VTE)
3.06 3.45 3.42 3.24 3.22
2.70 2.87 3.29
2.76 Baseline
Target
0.00
1.00
2.00
3.00
4.00
5.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
Post-Operative Pulmonary Embolism (PE) or Deep Vein Thrombosis(DVT) Rate (per 1,000 patients)
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
VTE 34 27 6 42 109
Source: HRET October 2015 – June 2016
Rate

Falls with Injury
0.62 0.55 0.59 0.59 0.63
0.51 0.53 0.52 0.55
Baseline
Target
0.00
0.20
0.40
0.60
0.80
1.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
All Documented Patient Falls with an Injury Level of Minor or Greater(per 1,000 patient days)
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
Falls 68 7 8 74 158
Source: HRET October 2015 – June 2016
Rate

30 day Readmissions (All Cause)
9.09 9.40 9.64 9.22 9.25 9.04 9.05 9.12
7.32
Baseline
Target
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
Readmissions within 30 Days (All Cause)
Topic
Hospitals Meeting 20%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-20%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
Readmissions 28 5 22 84 139
Source: HRET October 2015 – June 2016
Rate

Catheter-Associated Urinary Tract Infections (CAUTI)
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
CAUTI 64 33 6 62 166
1.07 1.24 1.14
1.00 1.15
0.95 0.95
1.26 1.19
Baseline
Target
0.00
0.50
1.00
1.50
2.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
CAUTI Rate (per 1,000 catheter days) – All Inpatient locations …
Source: HRET October 2015 – June 2016
Rate

Central Line-Associated Blood Stream Infections (CLABSI)
1.04 0.89 0.78
0.96 0.97 0.97 0.82
1.01
0.70 Baseline
Target
0.000.200.400.600.801.001.201.401.601.802.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
CLABSI Rate (per 1,000 central line days) – All inpatient locations
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on this
Topic
CLABSI 67 31 4 58 163
Source: HRET October 2015 – June 2016
Rate

Ventilator-Associated Events (VAE)
2.38
1.44
1.99
2.91 2.63
1.63
2.12 2.16 1.81
Baseline
Target
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
Ventilator Associated Condition (VAC) (per 1,000 ventilator…
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
VAE 32 38 0 19 116
Source: HRET October 2015 – June 2016
Rate

Surgical Site Infections (SSIs) Composite Measure
1.58
1.96 1.66
1.81 1.52 1.63
2.01
1.59
1.30 Baseline
Target
0.00
0.50
1.00
1.50
2.00
2.50
3.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
SSI Composite rate - All procedures reported
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
SSI 51 14 3 71 145
Source: HRET October 2015 – June 2016
Rate

Pressure Ulcers
0.96 0.82
0.41
0.80 0.63
1.18 1.18 0.91
0.62
Baseline
Target 0.00
0.50
1.00
1.50
2.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
Pressure Ulcer Rate, Stages 3+ (per 1,000 patients)
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on this
Topic
PrU 1 15 53 0 11 80
0.3
0.3
0.5
0.2
0.3 0.5
0.3
0.3
0.4
0
0.2
0.4
0.6
Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16
% P
atie
nts
w/
Stag
e II+
PU
Patients with at least one Stage II or Greater Nosocomial Pressure Ulcer
Baseline Goal All Hospitals
Prevalence (CALNOC)
Incidence
Source: HRET October 2015 – June 2016
Rate
Number of hospital that submitted PrU 2 data = 111

Adverse Drug Events (ADE) Composite Measure
1.06 1.07 1.15 0.97
1.23 1.24 1.14 1.16 1.32
Baseline
Target
0.00
0.50
1.00
1.50
2.00
2.50
3.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
ADE Composite rate - All areas reported
Topic
Hospitals Meeting 40%
Reduction Target
Hospitals Maintaining Zero Harms
Hospitals Showing
Reduction between 0-40%
Hospitals Showing No Reduction
Hospitals Reporting on
this Topic
ADE 33 13 5 44 95
Source: HRET October 2015 – June 2016
Rate

C. difficile Infections (CDI)
0.83 0.83 0.88 0.91 0.86 0.83 0.78 0.76 0.79
Baseline
Target
-0.10
0.10
0.30
0.50
0.70
0.90
1.10
1.30
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
c. diff Rate (per 1,000 patient days) – All Inpatient locations excluding NICUs
Source: HRET October 2015 – June 2016
Number of hospital that submitted data = 155
Rate

Overall Sepsis (Incidence)
77.01 85.38 85.98 91.87 97.40 79.64 74.16
45.41
71.04
Baseline
Target
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
160.00
180.00
2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05 2016-06
Overall sepsis rate (per 1,000 discharges)
Source: HRET October 2015 – June 2016
Number of hospital that submitted data = 26
Rate

Hospital Improvement Innovation Network (HIIN)
2-year with option for third year to reduce all-cause patient harm by 20% and 30-day readmissions by 12% • September 30, 2016 – September 29, 2018 funded
by CMS • Recruitment target of well over 200 hospitals
participating with HQI • Integration of Hospital Engagement Network (HEN)
with the Quality Improvement Network-Quality Improvement Organization (QIN-QIO)
Chasing zero!

HIIN Topics
Core Topics with Performance Metrics
1. Adverse Drug Events
2. CLABSI
3. CAUTI
4. C. difficile
5. Falls
6. Pressure Ulcers
7. Sepsis
8. SSI
9. VTE
10. VAE
11. Readmissions
Additional Topics with Performance Metrics
1. Multi-Drug Resistant Organisms (MRSA)
2. Culture of Safety
3. All-Cause Harm Metric

“CMS believes that systematic identification, use and spread of known evidence-based practices at national scale throughout large peer learning networks of hospitals and health care delivery providers is the best methodology for bringing about rapid change.” -CMS HIIN Request for Proposal
Centers for Medicare and Medicaid


Discussion and Questions

How Can We Possibly Continue to Work on these Topics?

Marathon vs. Sprint

How it is Designed to Work

What it Actually Looks Like

Success Through Collaboration

Managing a Portfolio of Improvement
The pool of different improvement efforts by which a health care organization attempts to make care safe, timely, effective, efficient, equitable, and/or patient centered.

Step 1
Take an inventory

Step 2
Use a matrix to prioritize

Step 3
Divide and conquer

Divide and Conquer
Maximize measures – use the inventory to leverage your bench talent

Divide and Conquer
Calendar data sampling and focused reviews

Divide and Conquer
Assign ownership appropriately – so everyone knows who’s “Got It”

Your Turn
• Working in groups, decide the top 5 priority projects/topics in your organization’s improvement portfolio
• For Your Top 5 Priorities, how are those connected to other work being done in your hospital? Is there other work being done that is similar or somewhat replicated in another area of the hospital? How do you know?

Your Turn Continued
• How can we best engage other “owners” in the process of improving care?
• What kind of practical help can HQI provide in the work of improvement?

Poster Session I
• Bulletin Boards 1 and 3, plus slide show posters
• Remember to fill out feedback cards

Break Time

Poster Session II
• Bulletin Boards 2 and 4, plus slide show posters
• Remember to fill out feedback cards

Hardwiring Improvement: The Sustainability Challenge

49

50

51

Your Turn
• What has your organization put in place to sustain the improvements that have been made?
• How will you ensure this work continues, or monitor if further work needs to be done?
• How can data be used to inform this work and the next steps that are needed?

Break Time


The Rules
• 2 minutes per turn
• When you hear “Switch”, move two places to the left
• Bring your writing pad, pen and business cards
• Discussion topic: One innovation, test of change, new process, etc. that you are proud of in the past year in your hospital related to reducing harm

Poster Awards



Situation: Review the implementation of the Nose- To-Toes™ Surgical System (manufacturer code #9012) and the effectiveness it has had on our Surgical Site Infections (SSI) and SSI Standard Infection Ratios. Background: The cost to treat one SSI can range from $25,546 to upwards of $90,000⁵. In part, we implemented Nose-To- Toes™ Surgical System in February of 2016. In 2015, there were 49 SSIs in 4,805 procedures with an SSI Standard Infection Ratio (SIR) of 0.69. In 2016 YTD (Jan to June) we have had 17 SSIs in 2,631 procedures with a SSI SIR of 0.44; Overall, there was a 35% reduction in the SSI SIR from 0.68 in 2015 to 0.44 in the first half of 2016. Assessment: From February 2016 to June 2016 we invested $12,711⁶ in the product. On average, from February to July 2016, we used about seven (7) #9012 kits per work/procedure day Overall, for 2016 YTD (Jan – June) it can be assumed we have seen a cost savings of $178,884 when compared to our 2015 SSI numbers YTD (see Figure 2)
Recommendation: Implement the Nose-To-Toes™ Surgical System to all procedures and determine the overall clinical and financial impact the expansion would have.
Figure 1. Surgical Site Infections, 2013 – 2016 Qtr 2
Figure 2. Cost Savings: 2015 vs 2016 YTD
Has been shown to address multi-drug resistant organisms on the skin prior to surgery when used as a part of the facility's preop protocol.¹²³ 1. Edmiston CE, et al., Skin antisepsis: efficacy of innovative chlorhexidine-impregnated surgical skin wipe (CIW) compared to traditional chlorhexidine surgical prep (TCP). Abstract presented at Surgical Infection Society (SIS) Annual Meeting,April 2006. 2. Time Kill and MIC Testing conducted by an independent laboratory; data on file. 3. Testing conducted by an independent laboratory; data on file. 4. Data provided by facility. 5. Stone PW, et al.,AM J Infect Control. Nov 2005;33(9):501-9. 6. Data based on ordering history provided by manufacturer.
# of SSIs Cost per SSI Treatment Cost Product Cost Total Cost ROI
Pre 2015 49 $25,546 $1,251,754 $0 $1,251,754 --
Pre 2015 YTD (6 mo) 25 $25,546 $625,877 $0 $625,877 -- Post 2016 YTD (6 mo) 17 $25,546 $434,282 $12,711 $446,993 $178,884
Cumulative Return On Investment: $178,884
MISSION HOSPITAL REG MED CTR - MISSION VIEJO, CA Initiative to Reduce Surgical Site Infections (SSI)
$800,000
$600,000 Treatment Cost $1,251,754
$400,000
ROI $178,884 Product Cost $12,711
Treatment Cost $625,877
$200,000 Treatment Cost $434,282
$0

By the end of June 2016, decrease the
reportable CAUTI infection rate by 25% in
Providence Holy Cross Medical center
(PHCMC).
Aim Statement
Interventions
Next Steps
Lessons LearnedDMAIC
• Implementing a hospital wide initiative is
more challenging, requiring more
resources and unit differences to be
considered.
• In the area of control, the taskforce had
decided to postpone setting a control
plan, leaving the audits per units’
discretion. Without the data on indication
use (see DMAIC), we are unable to
determine actual compliance to the nurse
driven protocol.
Establishing a comprehensive control plan
hospital wide will be our first priority.
Monitoring individual unit data and having
unit leadership accountable for the results.
Indwelling urinary catheter care explored
per unit. Revalidate skills on insertion, peri-
care, and maintenance.
Team Members
Sponsor: Steve Tanner, Director of QI and
Accreditation
Team Members:
Carol Paderna, Quality Management Specialist
Robert Gentry, Assistant Nursing Manager,
Pulmonary Telemetry
Jennifer Caing, Nursing Educator
CAUTI Prevention
Mission Hills, CA
Hospital Logo
Background & Problem Overview
References
Reportable CAUTI incidences at Providence
Holy Cross Medical Center (PHCMC) was the
highest in the PHS Southern California region
in 2015.
CAUTI is preventable harm to patients and we
identified that strictly following a nurse driven
indwelling urinary catheter (UC) removal
protocol is one of the best tools to decrease
CAUTI infections.
American Nurses Association (n.d.), Streamlined evidence-based RN tool: Catheter associated urinary tract infection (CAUTI) prevention. Retrieved form ANA website
Focused in one unit: Pulmonary Tele
• (T)(I) : Based on audit results, implemented
education surrounding use of the Indwelling Urinary
Catheter Removal Protocol and Foley Care Bundle
evidence based practice.
Hospital wide: Spreading the message
• (I) Mandatory provider orders for all UC insertions;
strict indications followed; fallouts sent
• (I) CAUTI multidisciplinary taskforce established
Feb 2016:
• (S) All nursing staff CAUTI education program
Charts
DEFINE: Limit length of time catheter is in place
(Follow indwelling urinary catheter removal protocol)
MEASURE: Collect data regarding device days and
utilization rate
ANALYZE: Used Pareto charts to study trends in the units
IMPROVE: Brainstorm on alternatives to catheters
CONTROL: Three data points to monitor: indication use,
device utilization (device days/patient days), & infection
rate
The nurse driven protocol
had a positive effect UC
device days and
utilization rate but did not
translate to a decrease in
reportable CAUTI rate.
Reportable CAUTI infections
Pulmo Tele
Unit PHCMC
Jan – June
2015 vs 201667%↓ 5%↑

Prevention of Hospital-Acquired CDI
Mission Hills, CA
Aim Statement
Our goal is to implement effective strategies for reducing the incidence of CDI at PHCMC.
Background & Problem Overview
The epidemiology of CDI is changing rapidly, showing a significant increase in incidence and severity in recent years. CDI is the most common cause of HAIs in U.S. hospitals, and is the leading cause of gastroenteritis-associated death.[1]
Interventions
Diarrhea Decision Tree (S): Algorithm emphasizes early detection of CDI within first 3 days of admission and prompt isolation after first loose stool occurrence.
Hand Washing (S): “Speak Up for Safety” campaign empowers staff to “speak up” for hand hygiene through photos of coworkers with clean hands posted across the hospital.
Antibiotic Stewardship (S): Pharmacist reviews appropriateness of antibiotics on admission and daily. Pharmacist may place order for Culturelle® at start of antibiotics.
Appropriate Testing (S): Stool specimens are sent within 1 hour of collection. No solid stool specimens. Only 1 test in any 7-day period.
Stool Documentation (S): Computer-based alert system notifies RN if more than 3 stools have no assessment documented. RN is prompted to refer to the Bristol Stool Chart.
UV Light Cleaning (S): Daily and terminal room cleaning with bleach. UV-C disinfection post-terminal clean.
Transportation (S): Receiving department alerted of isolation status. Patient is draped in yellow isolation gown prior to transport.
Culturelle® is a registered trademark of I-Health, Inc.
Run Charts
The graph below captures PHCMC CDI rates from Q1 of 2014 through Q1 of 2016. Our innovative initiatives have reduced our CDI rates from nearly 11 at the end of 2014 to roughly 6 in Q1 of 2016. Infection Control Ticker tracks all HAIs by unit; it is circulated weekly to all PHCMC email users.
To address ongoing surveillance and sustainability of staff compliance, we are currently implementing a shift checklist for HAIs.
*To request a copy of the shift checklist, please contact Laura Collis at [email protected]
Reference(s) 1 Lessa, F.C., et al. (2015). Burden of Clostridium difficile Infection in the United States. New England Journal of Medicine, 372, 825-834.
Lessons Learned
1. Monitoring of “Hot Beds”: By visually mapping out the rooms occupied by a CDI patient from admission to discharge, we can ensure these rooms are properly disinfected.
2. Mini-RCA: Case debriefings can highlight areas for needed improvement. We have found that high-risk patients are not routinely identified within the first 3 days of admission (leading to mis sed opportunities to identify community-acquired CDI), isolation precautions are not initiated after the first loose stool occurrence (primarily due to lack of staff education), stool documentation is often inconsistent or incomplete (having no assessment), and probiotics are not routinely prescribed at the start of antibiotics.
3. Community Collaboration: Formation of a SNF Collaborative can heighten awareness of CDI and improve communication between facilities regarding the transfer of CDI patients.
Next Steps
Pending approval of Enzyme Immunoassay (EIA) Test: We currently use the PCR test that is highly sensitive on indications if C. diff is present, but not if the bacteria are toxin-producing.
Increase in Availability of UV-C Disinfection: Specialized technicians are available during limited hours with a focus on isolation rooms, critical care, and ER (largely due to cost).
Systematization of Cleaning Process: Standardization of room setup, and reinforcement of guidelines for cleaning and storing of moveable medical equipment.
Team Members
Our C. diff Task Force is an interprofessional initiative that meets on a monthly basis. It is comprised of: Nursing, Epidemiology, EVS, Pharmacy, Laboratory and Transportation. Our Antibiotic Stewardship Team is lead by our physician champion and ID pharmacist.
“Facilities Dashboard”. On this dashboard, our core quality measures – including CDIs – are summarized
with our baseline (defined as where we were last year), current target, and current year-to-date scores.
Each summary measure is highlighted in either red, yellow, or green for users to easily identify our
strong points as well as, most importantly, areas of opportunity. Further detail on any measure can be
easily retrieved by clicking on the measure of interest on the front page of the dashboard. The
dashboard is circulated among our Senior Leadership and Nurse Managers on a monthly basis, in
addition to being available on our PHCMC Quality Department SharePoint on our intranet for all users to
download. With these data at their fingertips, our leadership and staff stay well informed and can
effectively act and direct changes as necessary.
The implementation of these efforts has not been without challenges. Although we do believe that
room sanitation using UV-C rays is effective, the equipment is not allocated to all rooms every day,
largely due to cost. To this end, the equipment vendor is currently analyzing data pertaining the rooms
that have been routinely sanitized with the ultraviolet light to demonstrate that the benefits to this
technology outweigh the costs.
Another challenge we have faced is that clinical staff are not consistently using the Diarrhea Decision
Tree or they are unable to determine if the patient has diarrhea. In cases where the Decision Tree is not
used, there may a delay in identification of a CDI (as tests are not ordered) and potentially a delay in
isolation precautions, compromising the provision of optimal care for patients with this infection and
increasing the risk of transmission to other hospitalized patients. To meet this challenge, Nurse
Champions are commissioned to assure that clinical staff are taking (and potentially re-taking) an online
class on CDIs and are assessed for competency in this topic.
5. DESCRIBE THE RESULTS OF THE EFFORT
The graph below captures PHCMC CDI rates for the 9 quarters from the first quarter of 2014 thought the
first quarter of 2016. Since the high of nearly 11 at the end of 2014, we have experienced a significant
reduction in our CDI rates to roughly 6 in the first quarter of 2016.
0.00
2.00
4.00
6.00
8.00
10.00
12.00
Q1,2014
Q2,2014
Q3,2014
Q4,2014
Q1,2015
Q2,2015
Q3,2015
Q4,2015
Q1,2016
CD
I Rat
e
Providence Holy Cross Medical Center CDI Rate by Quarter Q1, 2014 - Q1, 2016
Note:HAIPreventionShiftChecklistwillbereviewedduringcasedebriefingifHAIoccurs.
*ForpatientswithloosestoolsonadmissionORscreenedashighrisk,obtainMDordertocollectspecimenafterthefirstloosestooloccurrence(ifwithin3daysofadmission).Sendspecimenwithin1hour.
HAIPrevention:ShiftChecklist PHCMCDate:____________________ AuditorName(s):____________________ Unit:____________________
ShiftChecklistGuidelines:Checklistmustbecompletedforeverypatientwithan
indwellingurinarycatheter,centralline,andloosestools.ChargeRNcompleteschecklisteveryshift
(informationisverifiedwithprimaryRN).OncomingChargeRNre-verifieschecklisteveryshift.
All“no”responsesmustbeexplainedinthecommentssection(indicatenumberifapplicable).Statewhether
ornotjust-in-timeeducationwasprovided.
Leavechecklistin“HAIPrevention”binderundertheappropriatemonth.
CAUTIPrevention CLABSIPrevention CDIFFPreventionPatientEducation
DailyNeedCriteriaMet
(docu-
mented)
Indicateneedin
Commentssection.
(1)Securementdeviceused;(2)Notubing
kinksordependentloops;
(3)Bagbelowlevelofbladder,offfloor,lessthan
2/3full
PeriCareperformedeveryshift
(docu-mented)
DailyNeedCriteriaMet
(docu-
mented)
Indicateneedin
Commentssection.
(1)Dressingdry&intact;(2)Occlusive
dressingchangedw/inlast7days;(3)Labelwithduedateofnextdressingchange
present(docu-
mented)
(1)Linespatent;(2)Unused
lumensclamped;(3)Novisiblebloodintubingorconnector;(4)Curos™
capsused;(5)Tubinglabeled(docu-
mented)
(1)Contactenteric
precautions;
(2)Patient-dedicatedequipment;(3)Bleachtodisinfectsharedequipment
(*seenoteatbottom)
(1)Appropriateuseof
antibioticsandProtonPumpInhibitors;(2)Culturelleprescribed(ifapplic-
able)
(1)Assessmentdocumented
foreverystool
occurrence;(2)
Isolationprecautionsdocumented
asstartedormaintained
HAIpreventioneducation
provided(docu-
mented)
ChecklistRe-Verified
(everyshiftbyoncomingChargeRN)
MRN:
RM#:
RN(s):
CNA(s):
¨ Y
¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N
Comments:¨ Y ¨ N
MRN:
RM#:
RN(s):
CNA(s):
¨ Y
¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N
Comments:¨ Y ¨ N
MRN:
RM#:
RN(s):
CNA(s):
¨ Y
¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N
Comments:¨ Y ¨ N
MRN:
RM#:
RN(s):
CNA(s):
¨ Y
¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N
Comments:¨ Y ¨ N
MRN:
RM#:
RN(s):
CNA(s):
¨ Y
¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N ¨ Y ¨ N
Comments:¨ Y ¨ N

Prevention of Hospital-Acquired Pressure Ulcer
Providence Holy Cross Medical Center | Mission Hills, CA
Aim Statement Our goal is to implement effective strategies for reducing the incidence of HAPU at PHCMC.
Background & Problem Overview Pressure ulcers are not only uncomfortable and painful for patients but they can also be costly for impatient care facilities, such as PHCMC. Because most pressure ulcers can be prevented through identification, risk assessment, and preventive measures, their frequency can be a useful indicator of quality of care. 1
Interventions SKIN Bundle:
o S – surface and skin inspection o K – keep them moving o I – incontinence and moisture
management o N – nutrition management
10 Commandments of Pressure Ulcer Prevention (PUP):
1. Sacral area photo at admission 2. Double signature and wound staging
as indicated 3. Repositioning every two hours with a
turn clock schedule
4. Repositioning using 30° side turning
using wedges or pillows 5. Side to side only positioning for
patients with coccyx pressure ulcers 6. Float heels off mattress at all times,
using pillows 7. For suspected pressure ulcer:
documentation in EMR, photo, notify physician, wound nurse, family and charge nurse, occurrence report is completed.
8. Access the Wound Resource manual for bed decision tree (support surface_ per unit’s guidelines
9. Tracheostomy care every shift per protocol with tracheostomy foam dressing when newly inserted for up to 10 days post – op
10. Collaboration with respiratory therapy when patient is on BIPap / CPAP and all patients using oxygen must have nasal canula with oxy ears.
Run Charts
House-wide pressure ulcers have been steadily decreasing from 2012 to 2015.
PHCMC uses Braden Scale on EMR to assess risk for pressure ulcer
*To request a copy of the Braden Scale, please contact Monica
Twedell at [email protected]
Reference(s) 1 Perneger TV, Héliot C, Raë A, Borst F, Gaspoz J. Hospital-
Acquired Pressure Ulcers: Risk Factors and Use of Preventive Devices. Arch Intern Med. 1998;158(17):1940-1945. doi:10.1001/archinte.158.17.1940.
Lessons Learned
1. Standardization – By standardizing the process for pressure ulcer prevention it has been
determined that we could decrease wounds and pressure ulcers. In addition through our thorough risk assessment and with the use of the Braden Scale we have seen our numbers drop.
2. Photo Documentation – During admission and upon assessment if skin lesion is noted photo is taken as a point of reference. In addition, a photo of the sacral area is also taken as a baseline. We have noted that this step helps identify ulcers as nurses can go back and reassess those photos. In addition it also makes our nursing staff more responsible to check both patients and photos for skin lesions and ulcers.
3. Compliance – CNA’s found it most challenging in adopting PUP bundle due to changes in practice. One of the major changes that CAN’s had to adapt to was getting ride of diapers.
Next Steps
Continuous Education – We continue to educate nursing staff on the importance of the PUP Bundle and ensure they are all committed to prevention.
Continuous Monitoring – We continue to monitor the prevalence of pressure ulcers to ensure PUP Bundle is effective.
Sacral Dressing – We implemented house wide sacral dressing to reduce pressure ulcers.
Team Members Our HAPU Taskforce is an interprofessional initiative that meets on a monthly basis. It is comprised of: Nursing, Epidemiology, EVS, Pharmacy, Laboratory and Transportation. Our Antibiotic Stewardship Team is lead by our physician champion and ID pharmacist.

To decrease avoidable admissions, targeting a ratio ofobserved to expected readmissions of less than 1.0.
Historically, approximately 1 in 5 Medicare patientswere readmitted to the hospital within 30 days ofdischarge. This accounted for an estimated $17 billionannually in Medicare expenditures that may havebeen largely avoided – an expense that is now beingshifted to hospitals under the ACA’s HospitalReadmission Reduction Program. Improvements inpatient care can reduce readmissions and ease thisfinancial burden.
Team Members
Our efforts to reduce readmissions is a collaborativeeffort among Senior Leadership, Physicians and Nurses;and across the Education, Pharmacy, Dietary, CaseManagement, and Quality Improvement Departments.
Aim Interventions
Effective Readmission Reduction Strategies: Closing the Revolving Door by Improving Patient Care
Background & Relevance
A Spider Chart is an excellent quality improvement tool thatprovides a two-dimensional snapshot of three or more variables.The Spider Chart above simultaneously displays the PHCMCReadmission OE Ratio from June 2015 – May 2016, computed usinga 12 month moving average, for 8 separate diagnosis. Data pointsin the highlighted area represent better than expected OE Ratios.Overall, our Readmission OE Ratio was 0.94 during the period, andtrending downward over the past several years.
The Emergency Department’s Care Transition Teamincludes a dedicated Case Manager 7 days perweeks/16 hours per day
Every admitted patient is assigned a “readmissionrisk” score
Daily work lists flag 30-day readmissions Medication reconciliation is conducted on admission
(by a Pharmacy Tech in the ED) and again atdischarge.
Daily Interprofessional Care Rounds Monday - Friday Any staff member can request a Palliative Care Team
consultation Patients and their primary caregivers are educated
using the “teach-back” method; “After VisitSummary” is reviewed with patient before discharge;and nurses may request Pharmacy reviewmedications with patients if necessary
Case Management schedules follow up appointmentsprior to discharge
Referral to a Post-acute Physician Panel member ifthe patient does not have a primary doctor
Post discharge phone calls are made within 48 hours Special focus on CHF patients: Nursing, Pharmacy,
Dietary and Case Management are provided a list ofthese patients daily; Quality Improvement tracks CHFeducation and conducts post-discharge phone calls
Regional Readmission FMEA to find the gaps andbridge them
Next Steps
Conduct physician review of readmission cases Investigate funding opportunities to establish an
FQHC staffed by a Nurse Practitioner
Lessons Learned
To Close the Revolving Door:
Repeatedly ask: “Is this a safe discharge?” Deliver clinical excellence to every patient at every encounter Practice a high level of communication across the Care Team Provide a smooth transition to the next level of care by
assuring patients understand their treatment plan, haveaccess to further care, have been given the right medications,and have a support system in place
Give PCPs access to the discharge summary and plan of care

• Increase the utilization of sepsis treatment bundles to reach a compliance rate of > 40% by year-end 2016.
• Decrease the overall sepsis mortality to < 15% by year-end 2016.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Implementation of Sepsis Screening process for Nursing in the EHR with integrated SIRS and Sepsis Alerts for nursing and Providers (I)
Implementation of Sepsis 3-hour and 6-hour treatment bundles (I)
Implementation of Code Sepsis process of inpatient areas for positive sepsis screens utilizing the Rapid Response Team (T)
Implementation of nurse-driven protocols to begin elements of the sepsis 3-hour treatment bundle (I)
Project rollout did not provide an opportunity to test on a small scale.
EHR processes causing confusion with staff leading to actions that circumvent the intended outcome (early recognition and treatment).
The screening process casts a “wide net” leading to misidentification.
Efforts needed from leadership to assist in encouraging more physician engagement.
Review effectiveness of Code Sepsis process to reduce redundant or duplicate lab draws.
Review screening process for accuracy and focus education on the process to improve identification.
Improve sharing our successes and identified opportunities for improvement.
Team MembersAnne Engleman MSN, RN-Sepsis LeadM. Bragg, MD-ED physician championScott Jagger RN-ED DirectorMaryann Lansangan RN-IP DirectorS. Eskandari MD-Hospitalist championSandy Martin-DCQIPat Swaller-CNO
Sepsis MortalityJFK Memorial Hospital
Indio, CA
Background & Problem Overview
References
Sepsis is a costly medical condition with the potential for poor patient outcomes. Evidence from the Society of Critical Care Medicine’s Surviving Sepsis Campaign shows using evidenced-based practice for treating severe sepsis and septic shock improve s patient outcomes through early recognition and treatment.
18.22%
14.33%
10%
17.65%
11.11%
5.88%
30.77%
11.76%
19.05% 18.75%
0%
15.15%
9.76%
13.51%
15.69%
10.26%
29.79%
17.86%
15.15%
4%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
Mor
talit
y R
ate
Sepsis by DRG Mortality Rate
Prev. Yr. Median Mortality Rate
33%
25% 25%22.2%
25.0%
66.7%
70.0%
33.3%
83.3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16
% C
om
plia
nce
CMS SEP-1 CORE MEASURE BUNDLE COMPLIANCE
Levy, et.al. (2014). Surviving Sepsis Campaign: Association between performance metrics and outcomes in a 7.5-year study. Intensive Care Med.40, 1623-1633.Hall, M., Williams, S., DeFrances, C. & Golosinskiy, A.(2011). Inpatient Care for septicemia or sepsis: A challenge for patients and hospitals. NCHS Data Brief, 62.

Monterey Park Hospital has maintained a rate of zero (0) CAUTI since January 2013. Multiple actions, including daily assessment, protocol for removal and strict technique have contributed to the success of our program.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
• Physician compliance with daily assessment of need for Foley Catheterization.
• RN working with physicians to identify need for continued or discontinuation.
• Ancillary educated about maintaining collection bag below the level of the bladder and above floor & maintaining unobstructed urine flow when they deal with patients.
• Accountability at all levels • Empowering staff to act• Compliance from physicians
Team Members
Milad Shokair, ICP, Hy Ngo, MD, Evelyn Ku, CNO, Liliana Ocampo, RN, Cynthia Garcia, RN, Debbie Miller, RN, Josephine Reyes, RN’ Ruth Honig, DCPI
HAC DescriptorMonterey Park Hospital
Monterey Park, CA
Background & Problem Overview
References
In 2010 the CAUTI rate was 0.9, in 2011 the rate was 0.3. We have been 0 since 2012.
CDC Bundles for reducing HAI
• Review of every urine culture to determine if HA or MDRO for isolation purposes (S)
• Daily assessment of need for Foley & discontinue when appropriate (I)
• SNF patients with Foley, replace Foley on admission. (I)
• On-going observations of nursing practices for compliance (I)
• Sharing of results of infection reduction actions.(S)
0.9
0.3
0 0 0 000.10.20.30.40.50.60.70.80.9
1
YTD10
YTD11
YTD12
YTD13
YTD14
YTD15
Hospital Wide Catheter AssociateUrinary Tract Infections

To reduce the incidence of CLABSI on the Oncology Unit by 20% from a baseline rate of 2.8 in 2015 to 2.26 by 12/2016
Target Condition for bathing is 75% of patients to be bathed daily from the 1/2016 baseline of 28% and 75% of neutropenic patients to be bathed with CHG
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Blood Culture Draw Process:1) Create supply kit with instructions and a checklist
for blood culture specimen draw (S)
2) Pretest/educate/self test/audit staff knowledge (I,S)
Patient Bathing:1) Supplies:: CHG and warmer stocked on unit (i)
2) Policy change :Bathing must be done daily in shower or with CHG wipes. Patient encouraged 2X per day. (S)
Key:Tested (T), Implemented (I) or Spread (S)
Bundling supplies in a kit with a check off sheet ensures sustained compliance.
Giving patients two options for bathing and auditing documentation and process led to sustained change in the bathing process.
Next Steps:
1) Secure vender to outsource blood culture supply bundle kit and stock tin all acute care hospitals in system.
2) Educate clinical staff throughout system
3) Put together process to audit neutropenic bathing processes throughout system
Team MembersProject Champion : Jennifer Taylor RN, BSN,OCN,AMSRNManager Oncology: Amy VandenHeuvelMSN, RN, CRRNInfection Control: Leslie Stanfield RN,BSN,CICEducation: Jaqueline Baker BSN, RN-BC, ONC
CLABSI REDUCTION in ONCOLOGY
Background & Problem Overview
References
Variation in blood culture draw practice along with non-robust bathing process contributed to an increase in CLABSI on the Oncology Unit
• Blood culture draw practice:- Supplies in multiple locations. Staff knowledge deficit
• Bathing-:Practice not reinforced .CHG- not currently utilized for neutropenic patients
1)www.apic.org/Resource_/.../CHG_crosswalk_PS1504_winter.pdf
2) apic.org/Resource_/.../2015/APIC_CLABSI_WEB.pdf3)apic.org/Resource_/TinyMceFileManager/.../AC13_Prog_FINAL.pdf
4)http://www.cdc.gov/getsmart/healthcare/implementation/clinicianguide.html

Reduce ICU CAUTI by 40% from baseline FY2015 rate of 3.10% to 1.19% for FY2016
Achieved 62% reduction from FY2015.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
1. Identify focus group of frontline staff to review data and identify strategies based on current performance. (Implemented)
2. Daily CAUTI Rounds in ICU by CAUTI prevention team June – Aug 2015 to assess Foley care combined with CAUTI prevention education to nursing and education of patient/family. (Tested and implemented)
3. CAUTI Prevention Project implemented in ICU Sept 2015 – July 2016 Nurse competency for Foley insertion demonstrated in simulation lab, Foley placement, Daily needs assessment, Daily Meatal cleansing, documentation and stabilization. (Tested and implemented)
4. March- Apr 2016 New Foley Kit educated and implemented for all nursing units. (Implemented)
Only start with one or two units.
Engage Senior leadership - Gain CNO/DON Nursing Support.
Perform assessment of current practice. Eyes on daily practice. Aseptic Insertion means different things to different people thus identify one standard (definition).
Peri Care and perineal cleansing prior to and after insertion are critical.
Do not assume all staff understand the “why” behind the proposed practice.
Use stories to illustrate a point and change practice.
Assure staff have appropriate resources.
Continue the gain and success in the ICU units.
Expand process to Med-Surg Units starting with frontline staff focus groups.
Team MembersKari Love Team Leader, SJH Systemwide Infection Preventionist
Rita Crasta RN, MSN CAUTI Prevention EducatorPatty Futrell RN, CAUTI Prevention EducatorLynette Kingsberry MSMB, TechnologistKielle Smith RN, Nurse Educator UrologyDuane Elkins Urology Technologist
CAUTI PreventionCovenant Medical Center
Lubbock Texas
Background & Problem Overview
References
The infection is considered catheter-associated if an indwelling catheter has been in place for greater than two days on the infection date. CAUTI complications can cause discomfort in the patient and increase hospital length of stay, health care costs and mortality (Saint, 2000). Despite intensive CAUTI prevention education, the CAUTI SIR remained elevated.
Fuchs, M.A., Thornlow, D. K., Champagagne, M.T., (2011). Evaluation of An Evidence-based, Nurse-Driven Checklist to prevent Hospital –Acquired catheter-Associated Urinary Tract Infections in Intensive
Care Units. Journal Of Nursing care and Quality / April – June 2011.
Magers. T. L., (2014). An Evidence Base Practice (EPB) Mentor and Unit Based EBP Team: A strategy for successful Implementation of a practice Change to Reduce Catheter – Associated Urinary Tract Infections Worldviews on Evidence-Based Nursing , October 2014; 11 (5):
m2

Reduce hospital acquired VTE’s by 40% from baseline CY2014 rate of 7.11% to 4.27% for FY2016
Achieved 65.96% reduction to 2.42% (FY2016).
Aim Statement Interventions
Next Steps
Lessons Learned
Run Charts Team Members
Chief Medical OfficerProcess Improvement SpecialistQuality Management SpecialistDirector of Data Analyst Nursing LeadershipClinical Nursing StaffPurchasingPhysical Therapy PharmacyEVS
VTE Reduction ProgramCovenant Hospital
Lubbock, Texas
Background & Problem Overview
References
Hospital-associated VTE’s, are the most common cause of preventable hospital death. Alongside severe mortality rates, VTE can cause long-term, chronic morbidities and up to 40 percent of patients may suffer a recurrent event within 10 years after the initial diagnosis. Hospital acquired VTE metrics were incorporated into the PSI program and became an NQF endorsed measure set. The PSI metric was also incorporated into the Value Based Purchasing Program (pay for performance). Despite significant risk factors present in almost all hospitalized medical and surgical patients, studies continue to demonstrate the significant underutilization of VTE preventive measures. CMC identified an excessive amount of VTE’s in spite of implementation of a standardized risk assessment and strongly encouraged utilization of prophylaxis within 24 hours of admission.
• Remain open to expect the unexpected.• Follow evidenced based guidelines i.e. guidelines
for selective Doppler evaluation to avoid false positives.
• Complexity of preventing patient harm extends beyond implementation of standardized order sets.
• Low-hanging fruit was found in communication so never assume on communication. Key opportunities were identified in:
• Patient education on equipment.• Enhanced clarity between staff
(anesthesiologist/circulator regarding times & pressures).
1. Jai Prakash Sharma, Rashmi Salhortra. Indian Journal of Orthopedics/July 2012/Vol. 46/ Issue 4 2. Drolet A., DeJuilio P.,Harkless S., Kaimin E., Leddy E. A., Lloyd J., Waters C., Williams S.. Critical Illness Special Series/ Physical Therapy/February 2013/Vol. 93/Number 2
Continue to monitor data and report out at safety huddles.Ensure timely response to gaps.Core measure data shared routinely with Medical staff and nursing staff.
• Analyzed data and noted an opportunity with mechanical device utilization and tourniquet times & pressure.
• Shared data and research with the following entities: orthosurgeons, anesthesiologists and OR clinical staff.
• All OR staff educated on the following: Tourniquet placement, time & pressure measurement.Standardized communication & documentation of time & pressure between OR clinical staff and anesthesiologists during procedure.
• Increased Mechanical Device Availability and UtilizationGemba walk for use of mechanical devices.Educated staff on utilization of mechanical devices for pts sitting in chairs.Patient education on re-usablity of hospital equipment (vs patient home equipment). Standardize purchase of additional equipment. Standardize placement of mechanical device in each patient room.
• Regular report out of VTE incidence and work group initiatives at safety huddles.
• Instituted an Ambulation Protocol:Each patient is walked 4 times per day.Criteria developed for PT consult .Spread availability and practice of gait belt utilization to nursing .

Decrease the incidence of inpatient healthcare acquired Clostridium difficile
infections (CDI).
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
(I) Nursing education provided to promote early detection , isolation and C-diff testing for patients with 3 or more liquid stools in 24 hours without any other identified causes.
(I) Patients were placed in presumptive Contact Precautions until C-diff was ruled out.
(I) All C-diff contact isolation rooms are now disinfected with Bleach twice a day by EVS .
(I) Nursing staff switched to bleach wipes to disinfect any equipment leaving the patient’s room.
(I) Visual reminders were placed near the contact isolation room to promote washing hands with soap and water after exiting the room.
(T) An Ultraviolet light disinfection system was trialed in Quarter 3 -2015. All discharge rooms were manually disinfected then secondarily disinfected with the Ultraviolet light machine.
F h li t d h i di t h th it i b i
The UV light trial seemed to have the biggest impact on our CDI rates. The team reviewed a number of manufactures before
choosing a machine. The use of the UV system added approximately 20 minutes to
room turnover times. and required additional EVS staff to operate.
Recommendations:
Purchase a Ultraviolet UV) light system and utilize this advanced disinfection method as an adjunct to existing manual cleaning protocols.
Create a dedicated Environmental Services position to ensure UV light disinfection is performed on every discharged patient room.
Team Members
Kathryn McLaughlin DNP, NP –Chief Nursing Officer
Jennifer Cole MSN, RN, CIC-Director of Infection Prevention
Nancy Banda -GM EVSJulie Collier -Director of Quality Tiffany Trejos -Quality Manager
Healthcare Acquired Clostridium Difficile Infections
Hemet Valley Medical Center Hemet, CA
Hospital Logo
Background & Problem Overview
References
Inpatient health care acquired CDI rates have increased annually and reducing this rate has become an organizational priority.
Center for Disease Control and Prevention. (2016). Clostridium Difficile Infection (CDI) Toolkit.

Reduce hospital readmissions by 20% from FY2014 rate of 11.2% to 9.0% for FY2015
Achieved 52% reduction to 5.4% (FY2015).
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Determine appropriate staff/team to engage in program.Engage leadership and establish buy in for program through alignment with population health, prevention of avoidable readmissions, and creation of healthier communities.Engage staff/team and establish buy in and commitment.Develop criteria for high risk populations.Determine methodology for patient invitation to join program.Develop tools to assess barriers to care including: health literacy, knowledge base regarding medications, availability of resources, access to a provider.Develop tool to assist in identifying and quantifying patient risk in order to determine the necessary amount of visitsImplement program.Evaluate the program – outcomes/impact, sustainment, patient and staff satisfaction/perception.
Patient/Staff satisfaction: noticeable shift in culture –frontline nurse teams have developed a more informed, compassionate perception of patients who are struggling to obtain and maintain good health. Rather than labeling these individuals, they are brainstorming and collaborating on how we can help them.Encouraging frontline staff to empower and engage patients in the care of their disease processes. Need to have a dedicated day-to-day project lead. Critical to have a staff selection process and orientation for the transition coaches.Effective education in the patient’s own environment is needed post discharge.Implementation of a Care Transitions Team that works at the hospital and provides assistance to patients post discharge has been shown to improve readmission rates and patient satisfaction scores.
Continue collaborative efforts among hospital departments in addition to outside agencies that patients transition to for further care.
Team MembersChief Medical OfficerDirector of Quality ManagementDirector of NursingNurse Mangers of Clinical AreasClinical Nursing StaffSenior Leadership
Readmission ReductionCovenant Plainview Hospital
Plainview, Texas
Background & Problem Overview
References
Excessive avoidable readmission rates have forced Medicare to implement the readmissions reduction program due to a reported spending rate of $17.8 billion a year on readmissions that could have been avoided. A fragmented health care system and lack of communication has left discharged patients confused about follow-up care, medications, and financial resources leading to unnecessary hospital readmissions secondary to deterioration of their health i.e. disease process.
Uecker, S. (2014) Your role in clear health communication: A health literacy skills workshop: training materials. Literacy Coalition of Central Texas
Dreyer, T. (2014, January 15). Care Transitions: Best Practices and Evidence-based Programs. Retrieved from http://www.chrt.org/publication/care-transitions-best-practices-evidence-based-programs/
1.38
1.92
0.83
1.35
1.3
1.01
0.77
1.27
1.2
1.07
0.88
1.12
0.470.45
0.79
0.32
0.59
0.32
0.9
0.79
0.86
0.86
0.63
0.7
0
0.5
1
1.5
2
2.5
Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15
30-Day Unplanned Readmissions O/E Ratio
Program implementation

Aim – Reduce hospital wide CAUTI by 40% (from 1.11 to 0.87) by September 23, 2016.
Aim Statement
Interventions
Next Steps
Lessons Learned
Run Charts
CAUTI prevention bundle education to nursing staff. (Implemented)
Transparency of data to clinical staff by posting outcomes on each unit. (Implemented)
Improved EHR documentation for urinary catheter care. (Implemented)
Bedside RNs, physicians, nursing educators and leadership further defined CDC recommended indications for catheterization for critical care patient and non critical care patients. (Implemented)
Insertion re-training and competency for all bedside nurses. (Implemented)
Development of Nursing Standardized Procedure for Discontinuation of Urinary Catheters. (Implemented)
Front-line staff (RNs. PCAs and physicians) engagement is very important. Everyone needed to be involved.
Active communication, education and reinforcement of process change with all bedside staff is necessary to evoke change.
Leadership buy-in to ensure accountability of bedside staff is a necessity.
Continue to focus on reducing patients harmed and money saved.
Monitor urinary catheter necessity and utilization of nursing standardized procedure to reduce unnecessary urinary catheter use.
Evaluate effective alternative products to decrease urinary catheter use.
Team Members
Project Champion,: Melissa Garcia, Infection Preventionist
CAUTI TaskforceNursing Clinical Quality CommitteeLani Malcolm-Koch, Nursing EducationSheryl Frost, Nursing DirectorBarbara Goss-Bottorff, Director Infection Prevention
Hospital-Wide CAUTI Prevention Process Implementation
Hoag Memorial Hospital PresbyterianNewport Beach and Irvine, CA
Background & Problem Overview
References
Hospital Acquired Infections harm patients and cost hospitals money. CAUTI’s are associated with increased morbidity, mortality, hospital cost and length of stay.
IHI How-to Guide: Prevent Catheter-Associated Urinary Tract InfectionHICPAC Guideline for Prevention of Catheter-Associated Urinary Tract Infections
SHEA/IDSA Strategies to Prevent Catheter-Associated Urinary Tract Infections in Acute Care Hospitals:
73% Improvement

Keeping Hospitalized Patients Safe from Falls: Sustained Improvement Utilizing an Organizational Approach
Rose Newsom, MSN, NE-BC Kaweah Delta Health Care District, Visalia, California
It is impossible to prevent all falls in hospitalized patients. Through critical review of current practice, it is possible for healthcare organizations to improve and sustain a reduction in all falls. This is achieved through continuous quality improvement and commitment to provide needed resources to maintain focus on reducing patient falls with serious injury.
Interventions Results & Discussion
Conclusion
Purpose
This project describes how one rural, 581 bed, level III trauma center sustained reductions in total falls per 1000 patient days, total falls with injury per 1000 patient days and percentage of falls with moderate to severe injury through redesign of an existing falls prevention program.
With the support of organizational Senior Leadership, an aggressive redesign of an existing falls prevention program was launched in an effort to reduce total falls, falls with injury and severe falls with injury in the Fall of 2013. As a result, necessary financial resources became available to support this work.
Key interventions included:
1. Senior leadership support:• Reorganization of existing Falls Committee.2. Risk Assessment:• Falling Star Alert program: A post fall review at
the unit level.• Implementation of a Post Fall Nursing Order Set
to escalate nursing assessment of patients during the 24 hours post fall.
3. Communication:• Implementation of unit shift safety huddles.• Patient and family participation utilizing a
Partnership Agreement.4. Education:• Re-engineered education for direct care
providers with an emphasis on risk factor assessment, risk mitigation and accountability.
• Fall prevention education provided to all new employees during District Orientation.
• Creation of S-P-L-A-T: An easy mneumonic for room safety checks.
• Creation of a safety bring back session for all clinical staff to reinforce key interventions.
• Coming in 2016, development of community outreach to increase fall prevention awareness and reduction in fall related trauma.
5. Risk Mitigation:• Required interventions for moderate to high risk
patient populations: Attended toileting, use of alarming devices.
• Therapeutic pharmacy exchange for zolpidem in high risk populations.
• Purchase of fall mitigation tools: Various alarming devices, floor mats, shower mats.
6. Accountability:• Falls U: A weekly, non-punitive review of all falls.
Background
One third of adults, aged 65 and older, fall every year. Many sustain injuries that may be life-threatening or life-ending. Hospitalized adults are at greater risk of falling due to inherent risk factors associated with hospitalization. Falls that occur in the hospital setting remain a top adverse event which impacts morbidity and mortality of patients. In the acute inpatient setting, approximately 20% of patients will fall at least once.
Falls without serious injury cost hospitals $3,500-$16,500. A fall with serious injury is associated with adverse outcomes and increased mortality.
Keeping patients safe from falls with severe injury is a priority for healthcare organizations.
Goals & Objectives
Reduce falls and continue to maintain progress by benchmarking at or below the NDNQI average:
1.Total falls per 1000 patient days.2.Total falls with injury per 1000 patient days.3.Percent of falls with moderate to severe injury.
As a result of aggressive redesign of an existing falls prevention program in Q3 2013, this organization achieved and sustained reductions in total falls per 1000 patient days, total injury falls per 1000 patient days and percent of falls with moderate to severe injuries.
Percentage reductions in fall events from the 2012 baseline level:• Total Falls: 26.4%• Injury Falls: 39.4%• Percent Falls w/Mod/Sev Injury: 82.5%
The ongoing analysis of falls has allowed the organization to maintain the priority of fall prevention. All results are shared with team members on a quarterly basis, specifically with frontline staff through the Shared Governance Structure and Unit Based Councils.
Implications for Practice
Sustained emphasis on fall prevention utilizing a variety of methods helps to sustain reductions in falls with serious injury. An aggressive falls prevention program is one intervention hospitals can use to keep patients safe from harm. This translates into improved patient satisfaction, improved clinical outcomes and decreased falls associated costs.
References
VA . Implementation Guide for Fall Injury Reduction (2013). National Center for Patient Safety Virtual Breakthrough Series: Reducing Preventable Falls and Fall-Related Injuries.Retrieved from http://www.mghpcs.org/eed_portal/Documents/Falls/AttachmentK.pdf
Acknowledgments
It is important to acknowledge the work of Sandy Volchko, MSN, Dr. Christopher Patty, the Advanced Nursing Practice Team, and the members of the Falls/Mobility Quality Focus Team for their assistance in keeping patients safe from harm.
0
1
2
3
4
5
Q3 2012 Q4 2012 Q1 2013 Q2 2013 Q3 2013 Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q4 2014 Q1 2015 Q2 2015 Q3 2015 Q4 2015
Total Falls per 1000 Pt. DaysKD Rate KD 2012 Mean NDNQI Mean
0
0.2
0.4
0.6
0.8
1
1.2
Q3 2012 Q4 2012 Q1 2013 Q2 2013 Q3 2013 Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q4 2014 Q1 2015 Q2 2015 Q3 2015 Q4 2015
Total Injury Falls per 1000 Pt. DaysKD Rate KD 2012 Mean NDNQI Mean
0
2
4
6
8
10
12
14
16
Q3 2012 Q4 2012 Q1 2013 Q2 2013 Q3 2013 Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q4 2014 Q1 2015 Q2 2015 Q3 2015 Q4 2015
Percentage Falls with Moderate/Severe InjuryKD Rate KD 2012 Mean NDNQI Mean

Aim: Reduce hospital-onset Clostridiumdifficile infections (HO-CDI) rate by 20% fromthe baseline rate of 11.25/10,000 patient daysto 9.0/10,000 patient days by the end of 2016.Achieved rate of 6.0/10,000 patient days.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
• Cleaning (I) – EVS completed a hands-on cleaning competency and Infection Control monitors the cleaning of High-Touch Surface Area using UV gel.
• Early Detection (I) – EMR C.diff screening protocol, which automatically generates a C.diffPCR order if patient reports symptoms.
• Early Isolation (I) – All ‘rule –out’ C.diff patient are place into isolation. “Guilty Until Proven Innocent!”
• Daily C.diff Report (I) – Daily reports are sent to Nursing Directors, Infection Control and EVS to ensure timely collected, early isolation, and appropriate cleaning.
The daily C.diff report revealed that many C.diff orders were not appropriate based on the patient’s lack of symptoms or uses of enemas/laxative. PRMC focused more education on when C.diff test was indicated to include review of clinical presentation.
Maintain current interventions.
Improve overall hand hygiene compliance.
UV light disinfection system for terminal cleaning.
Improve lab turn-around time for C.diff PCR.
Team Members
Michelle Swetky, MPH – Manager of Infection ControlChris Belknap – Environmental Services Director Mary Siemantal, RN – Clinical Quality AnalystRoy Miser – Quality CoordinatorTeresa Mendoza, RN - Clinical Nurse Informatics CoordinatorSteve Owens, RN, MBA - Chief Nursing OfficerCynthia Damboise, MSN, MHA, RN, CCRN, PCCN – Director Medical Telemetry UnitsWill Morrell-Stinson RN, BSN, MSN, CCRN –Director Cardiac Telemetry Daisy M. Dorotheo, RN, BSN, MHA, ONC - Director Joint and Spine Surgical
Clostridium difficile Reduction Bundle Palmdale Regional Medical Center
Palmdale, CA
Background & Problem Overview
References
In 2015, PRMC observed an increase in HO-CDI. PRMC had a HO-CDI rate of 11.25/patient days, which was statistically greater than national data (SIR=1.54, p-value < 0.05).
1.Owens, Robert C, et al. “Antimicrobial-Associated Risk Factors for Clostridium difficile Infection.” Clinical Infectious Diseases (2008) 46 (Supplement 1): S19-S31.
2.Huslage, Kirk, et al. “A Quantitative Approach to Defining “High-Touch” Surfaces in Hospitals.” Infection Control & Hospital Epidemiology (2010) 31 (Issue 8): 850-853.
0
2
4
6
8
10
12
14
16
18
20
Jul-1
5
Aug
-15
Sep
-15
Oct
-15
Nov
-15
Dec
-15
Jan-
16
Feb-
16
Mar
-16
Apr
-16
May
-16
Jun-
16
Rat
e p
er 1
0,00
0 P
atie
nt -
day
s
HO-CDI Rate at PRMC
HO
Goal
· Implementation of Early Isolation· Completion of EVS competency· Daily Report
· Implementation of C.diff Screening

Reduce Catheter-Associated Urinary Tract Infection (Standard Infection Ratio) by 40% from 2012 to 2015. The Standard Infection Ratio (SIR) is the number of infections incurred over the risk-adjusted number of predicted infections.
Aim Statement
Interventions
Recommendations
Lessons LearnedRun Chart• CAUTI SIR reduced for PMC and POM 90
and 100 percent, respectively, from 2012H1 to 2015H2. Ongoing surveillance and having complete data transparency with clinicians establishes accountability and promotes general need for improvement.
• Insertion technique is variable across clinicians but there are consistent lapses in asepsis.
• Nurses see a patient more than the physician. Authority to remove catheter is extended to nursing to reduce utilization and thus risk for infection.
• Data Reliability: Ongoing surveillance and reporting of insertion, maintenance, and case data to clinicians consistently. This type of communication is valuable in maintaining vigilance towards CAUTI reduction methods.
• Resilience towards prompt removal: Encourage importance of daily assessment for catheter necessity by nursing and medical staff. Every day a patient has an indwelling catheter, the risk for infection increases. Provide tools for assessment (bladder scanners, EMR notifications, assessment reminders). Follow re-catheterization rates. Offer alternatives (external catheters) and instruction for use.
Team Members
Catheter-Associated Urinary Tract Infection Palomar Medical Center (PMC) & Pomerado Hospital (POM)
San Diego, CA
Background
Urinary tract infections are the most common type of healthcare-associated infections, accounting for more than 30 percent of healthcare-associated infections reported by acute care hospitals. CAUTI has been associated with increased morbidity, mortality, hospital cost, and length of stay. (https://www.cdc.gov/hicpac/CAUTI)
• Maintenance and insertion assessments followed with annual system-wide skills evaluation and education.
• Partnership with Medical Staff for daily assessment of necessity for catheter
• Nurse-driven catheter removal protocol• Device utilization and patient risk review,
and routine catheter maintenance auditing and reporting to clinicians
• Use of catheter alternative for male patients (Reliafit®).
Valerie Martinez RN, BSN, MHA, CPHQ, CIC, NEA-BCSusan Trout, RN, CICMelinda Kanter RN, BSN, CIC, CWCNAnnie Duran, RN, BS, CICJarrod Becasen, MPH, CICDr. Steve Kuriyama, MD, CICDr. Paul Neustein, MD
Dr. Paul V. Polishuk, MDRaeAnne Watson RN, MSN, PCCN, NE-BC Mel Russell, RN, MSNLourdes Januszewicz MSN APRN ACNS-BC CCRNKim Duong-Coburn, RNLynne Morris, BSN, RN

To decrease the number of falls with injury from baseline of .22 per 1000 patient days by 40% to rate of .13 per 1000 patient days by September 2016.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Attended Fall Workshop and participated in Fall webinar series.
Huddle revised describing the different areas of risk for falling, and appropriate education to the patient in understanding the risks. Discussed on a daily basis prior to every shift, with teach-back. (T&I)
During handoff the patient is educated (each shift) of the reasons for the high fall risk (I)
Slogan: Call, don’t fall! (I)
Post Fall Huddle: Asking the patient what was different this time, to understand the reason behind the fall and prevent it moving forward (T&I)Questions to ask:• Did the RN know the reason for the high risk?• Was it documented and discussed in handoff?• Was the Care Plan addressing the risk?
The staff needed to understand the reasons behind the patient’s high fall risk designation. Until the why is understood fall prevention is simply another task .
As the understanding of fall risk improves, so does the teaching and engagement of the patient.
Monthly data analysis to identify causative factors and locations of falls.
Ongoing real time education of the staff daily.
Continue to monitor the progress.
Team Members
Project Champion – Will Morrell-Stinson Senior Leader Sponsor - Steve OwensTeam Members - Mary Siemantel & Roy Miser (Quality); Debbie Cockerham-Slaughter (Risk); Daisy Dorotheo, Cindy Damboise, Rick Smith (Nursing Directors)
Ann Dexter (PT); Teresa Mendoza (IT); Jody Pienta; Diane Morrow; Jennifer Garcia
Falls with injuryPalmdale Regional Medical Center
Palmdale, CA
Background & Problem Overview Among older adults age 65 or greater, falls are the leading cause of injury-related death, the most common cause of non-fatal injuries and the leading cause of hospital admissions for trauma (CDC, 2015). Despite posted signage, education and punitive corrective actions taken fall s with injuries did not decrease.
0
0.1
0.2
0.3
0.4
Base
line
Oct
-15
Nov
-15
Dec
-15
Jan-
16
Feb-
16
Mar
-16
Apr
-16
May
-16
Jun-
16
Rate
per
1,0
00 P
atie
nt d
ays
Falls with Injury
Rate per 1,000 Patient days Improvement Target
Start of Interventions

To reduce HAPU from 1.42 in 2014 by 40% to .85 for 2016.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts Need to assure that during times of
staffing fluctuations it is important to re-focus on skin rounding and other patient safety priorities.
• Improved skin rounding process.• Unit specific skin champions, mandatory
competency for CVI and ICU staff.• Skin check during bedside report.• Include dietician in multi-disciplinary rounds so
nutritional needs can be addressed.• All HAPU’s will be referred for nursing peer
review.• Use the evidence-based HAPU assessment form
to objectively determine the predictability of the HAPU occurrence. Once the assessments are completed ,it will be reviewed monthly at the Skin Integrity team and a copy sent to the unit manager where the HAPU occurred, lastly, the assessment will be scanned into Quantros along with the HAPU occurrence to assure event archiving.
• All HAPU’s and assessments/analysis will be reported quarterly to the Patient Safety/PI Committee as part of the quarterly Skin Integrity team report.
• Incorporate educational opportunities specific to HAPU’s in the Core Measure and HAC Prevention Reminder booklet.
• Education re garding importance of consistent documentation.
Team Members
Terry Daggi, RN, Chair, Skin Integrity Team, Brenda,Scott-Manzur,RN, Acting CNO, Winter Lopez, RN,Sharon Gross, RHIA, Administrative Director,Roberta Wright, CPHQ, Outcomes Manager, AmyGraham, RN, Acting CNO, Tower, Howard Davis,MD, CMO
Sustaining HAPU ReductionProvidence Tarzana Medical Center
Tarzana, CA
Background & Problem Overview
References
Conducted HAPU FMEA in 2012. Work-outs with a black belt facilitator done with a focus on ICU and CVICU staff. Over the last three years we have maintained low HAPU rates. The HAPU rate for 2015, 2014 and 2013 was respectively: 1.13, 1.42 and 1.18.
1.71
1.281.181.42
0.9 0.8
1.31.55
1.8
0.6 0.6
1.5
1
1.9
10.6
0.290.3
0.8
0.31
3.13
1.8
0.7
0
1
2
3
4
5
6
2011 2012 2013 2014 J-15 F-15 M-15 A-15 M-15 J-15 J-15 A-15 S-15 O-15 N-15 D-15 J-16 F-16 M-16 A-16 M-15 J-13 J-16
HAPU RateLinear (HAPU rate)
10 HAPU’s reported for the month of May 2016 for a rate of 3.13 (year to date rate 0.95). This is a dramatic increase from previous months and years. It was determined that an intense analysis of the May HAPU’s be undertaken to analyze causation, trends and determine corrective action.
Conducted a mini root cause analysis on all of the seven ICU/CVICU cases. Analysis included: diagnosis, length of stay, nutrition, age, sex, whether the patient was on vasopressors and/or a ventilator/Bi-Pap. Convened a team to do the analysis of the RCA individual findings.
Conducted FMEA Workout with front line staff from ICU
and CVICU
Conducted mini-RCA

Increase compliance with SEP-1 Measure from 64.71% in November 2015 to >= 99% by
December 2016.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts Education in all forms is important as well
as constant repetition of the message.
• Incorporate educational opportunitiesspecific to SEPSIS in the Core Measure andHAC Prevention Reminder booklet.
• On-going education re importance ofconsistent documentation
• Continue review of SEP 1 cases.• Incorporate new July CMS changes in the
RRT policy regarding volume re-assessment.
• Continue education for both the ED and IPphysician.
• Preparing to submit application for JCSepsis certification.
Team MembersThomas Yadegar, M.D. Critical Care, Scott Brewster, MD, ED,Leonard Adelson, M.D., Pulmonary Med., Aaron Shelub, IC, B.Scott-Manzur RN, Acting CNO, Winter Lopez, RN, SharonGross, RHIA, Administrative Director, Roberta Wright, CPHQ,Outcomes Manager, Amy Graham, RN, Acting CNO, Tower,Howard Davis, MD, CMO, Janis Wernstrum, HIM, MarkWeber, ERN, Sepsis coordinator, Estelle Schwartz, RN, ED,Donna Matalon, RT, Brandy Frye, RN, Nurse Educator andWilly Ramos, Lab Director
Compliance with SEP-1 Providence Tarzana Medical Center
Tarzana, CA
Background & Problem Overview
References
Formed our Sepsis Study Group in Jan 2009. Measured severesepsis and septic shock patient population for compliancewith IHI severe sepsis bundle elements on a monthly basis.Particular focus placed on early antibiotics and IV fluidadministration per Providence System specification.Significant improvement in bundle compliance and mortalityreduction achieved since the inception of the sepsis team.Started SEP-1 core measure reporting in Oct. 2015. Monthlypercent compliance with the SEP-1 measure ranging from theupper 60’s into the 90’s. ER performance is strong. Challengesremain on the inpatient presentation side.
IHI, SCPSC, CMS
94.12%
64.71%
87.50%
61.11%
75.00%81.25%
60.00%66.67%
87.50%
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16
Ap
pro
pri
ate
Car
e S
core
PTMC: SEP-1 Measure
0.79
0.500.73
0.840.64
1.21 1.261.04 1.06
0.89 0.830.97
0.0
0.5
1.0
1.5
2.0
2.5
O/E
Rat
io
PTMC Mortality O/E - PHS Objective to Date
(90% Confidence Intervals)
Data reviewed monthly by Sepsis Team (I) Host physician sepsis experts to present to medical staff through CME program (I)
Sepsis order set created (T&I) Presented data and story of sepsis journey at HASC annual meeting in 2013. (I)
Cases not meeting measure referred for formal peer review. (I) Hosted the mobile sepsis simulation classroom at our facility. (I)ER MD champion works with ER staff to improve compliance. (I) Report sepsis outcomes data to HASC. (I)Engaged rapid response team to screen for sepsis on RRT calls Employed MEWS alert to identify patients at risk for sepsis. (I) Engaged nursing education department to teach assessment and treatment bundle implementation. (I)
Created an Epic Smart Phrase template to capture ER MD documentation required data points and compliance with post fluid bolus reassessment. (T&I)

To reduce the incidence of CLABSI on the Oncology Unit by 20% from a baseline rate of 2.8 in 2015 to 2.26 by 12/2016
Target Condition for bathing is 75% of patients to be bathed daily from the 1/2016 baseline of 28% and 75% of neutropenic patients to be bathed with CHG
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Blood Culture Draw Process:1) Create supply kit with instructions and a checklist
for blood culture specimen draw (S)
2) Pretest/educate/self test/audit staff knowledge (I,S)
Patient Bathing:1) Supplies:: CHG and warmer stocked on unit (i)
2) Policy change :Bathing must be done daily in shower or with CHG wipes. Patient encouraged 2X per day. (S)
Key:Tested (T), Implemented (I) or Spread (S)
Bundling supplies in a kit with a check off sheet ensures sustained compliance.
Giving patients two options for bathing and auditing documentation and process led to sustained change in the bathing process.
Next Steps:
1) Secure vender to outsource blood culture supply bundle kit and stock tin all acute care hospitals in system.
2) Educate clinical staff throughout system
3) Put together process to audit neutropenic bathing processes throughout system
Team MembersProject Champion : Jennifer Taylor RN, BSN,OCN,AMSRNManager Oncology: Amy VandenHeuvelMSN, RN, CRRNInfection Control: Leslie Stanfield RN,BSN,CICEducation: Jaqueline Baker BSN, RN-BC, ONC
CLABSI REDUCTION in ONCOLOGY
Background & Problem Overview
References
Variation in blood culture draw practice along with non-robust bathing process contributed to an increase in CLABSI on the Oncology Unit
• Blood culture draw practice:- Supplies in multiple locations. Staff knowledge deficit
• Bathing-:Practice not reinforced .CHG- not currently utilized for neutropenic patients
1)www.apic.org/Resource_/.../CHG_crosswalk_PS1504_winter.pdf
2) apic.org/Resource_/.../2015/APIC_CLABSI_WEB.pdf3)apic.org/Resource_/TinyMceFileManager/.../AC13_Prog_FINAL.pdf
4)http://www.cdc.gov/getsmart/healthcare/implementation/clinicianguide.html

Aim – For 2015 and 2016, sustain rates of CLABSI & CAUTI at 0 through increased
bundle compliance and handwashing
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
• Increase accuracy of line days reported, including daily tracking of line duration, start and stop dates
• Increase compliance with hand hygiene through training and leadership emphasis
• Report days since last infection in daily leadership huddles
Improvement in Hand Hygiene compliance does make a significant impact It is possible to decrease CLABSI & CAUTI rates by utilizing bundlesInvolving staff improves their commitment to follow evidence based guidelines
Continue to report wins at daily huddleReinforce continued adherence to bundle & Hand Hygiene ComplianceOngoing education & reinforcement of processes in place
Team MembersLorene Campbell, BSN, CIC, Infection PreventionistJessica Gruendler, DNP, RN-BC, CPHQConnie Malek, RN, MSNLisa Karamatic-Shaner, RN, BSNKim Brown Sims, RN, MBA, BSNClinical Nurse Supervisors
CLABSI & CAUTI ReductionSierra Vista Regional Medical Center
San Luis Obispo, CA
Background & Problem Overview
References
An estimated one million catheter-associated urinary tract infections (CAUTIs) occur yearly incurring a cost of $676-- $2836 per event. CAUTIs were among the first hospital-acquired conditions selected for non-payment by Medicare and have been targeted for complete elimination as “never events,”
Central line--associated blood stream infections (CLABSIs) are an important and deadly healthcare-associated infections (HAIs), with a reported mortality rate of 12%--25% and an average cost per case of $26,000
1) www.medscape.com/viewarticle/779178 2) Medicare Program; changes to the hospital inpatient prospective payment systems and fiscal year 2009 rates. Fed Regist 2008. Pp. 48473-91 3) MMWR_March 4,2011/60(08); 243-248
29
1514
23
27 27
31
29
25
20
2322
8 8
5
1
3
9
6
3
13
45
12
0
5
10
15
20
25
30
35
PICC Line and Midline Placement 2015PICC Midline
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec
71% 73%
65% 68%
78%82% 80% 81% 81% 79% 81% 81%
SVRMC Hand Hygiene 2015 YTD
Processes resulted in:
0 CLABSIs in the last 800 days (26 months)
For CAUTIS, only 2 infections in the same time frame

To increase sepsis bundle compliance from 23% to 50% by second quarter of 2016.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
• Form a sepsis team
• Develop an institution-specific Sepsis Protocol comprising all bundle elements
• Educate all stakeholders in the clinical areas.
• Test Protocol in the clinical environment using small PDCA cycles and modify as needed.
• Collect data on use of form and also outcomes and provide rapid feedback to the team
• All points are currently implemented
• Physician champions are essential• Front line staff buy-in is challenging• Good handoff is essential• Incomplete documentation by
physicians and nursing
1. Monthly reporting of fall outs to appropriate departments (revisit small sample size)
2. Education for all nursing staff in adult inpatient areas
3. Re education for Internal Medicine and Emergency Department Physicians as needed
4. Presentation of measure and data results to Integrated Quality Council for support and accountability by executive leadership
5. Team collaborationMultidisciplinaryTeam Members
Dr. Saadat – Physician ChampionDr. Sheth – Physician ChampionDr. Tinloy – Physician ChampionJennifer Halligan QI RN Project ChampionMary Barnes RN Nurse ChampionLeslie Gill RN QI CoordinatorCarla Bomben Deputy DirectorDavid Culberson CEO
Six-Hour Sepsis Bundle Compliance
French Camp, CA
.
Background & Problem Overview
References
We chose this project because it is a significant cause of inpatient mortality.
• CMS definition and guidelines• Surviving Sepsis Campaign• Encyclopedia of Measures (EOM)

To reduce inpatient all cause 30-day observed/expected readmission rate from
0.96 in July 2015 to 0.78 by FY 2018
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Established reducing all cause 30 day readmissions as a strategic goal for the hospital with Executive Leadership support (I)
Established a Perfect Care Readmission Reduction committee with Executive Leadership and physician membership. (I)
Partnered with SNF to focus on readmission reduction and collaboration. (I)
Reviewed weekly readmissions with subgroup of frontline process owners with affect on readmissions. (I)
Implemented palliative care evaluation in the ED with direct admission to appropriate GIP Hospice patients from the ED. (I)
Utilized the IHI readmission tool for assessment of hospital discharge failures. (I)
Implemented he LACE tool as a predictor to identify potential for readmitted patient . (T)
Considered caregiver training for care at home while the patient is in the hospital (T)
Focus on a thorough discharge, making the appropriate resources available for the patient and families, and scheduling discharge follow up physician appointment
Scheduling of post discharge appointments is an opportunity
Ensure there is executive leadership support
Implement a family caregiver training program prior to discharge.
Development of the resource guide for the staff involved in the discharge process
Next steps for testing: Caregiver training and physician appointments scheduling
Team Members
Project Sponsor: Teresa Frey RN VP Clinical Excellence
Physician Champion: Dr. Riad Abdelkarim CMO
Project Manager: Paulette Fletcher RNPerfect Care Readmission Committee: Ambulatory care services, Palliative Care, Nursing, RCP Navigator, Care Management, Hospitalist
Readmission ReductionSt. Jude Medical Center
Fullerton, CAHospital Logo
Background & Problem Overview
References
Noted that the St. Jude Medical Center all-cause readmissions rate was 10.6% above the national average.
Which led to identifying system processes within the discharge process that were not lean.
STARR initiative on Avoidable Rehoptialzations March 2014
AHRQ Prevention Avoidable Readmissions Dec 2011
Achieved the FY 2018 goal with a current rate .73 for FY 2016

Sepsis is the top driver of mortality in critical care units and the 10th leading cause of death in the United States. Approximately 90% of SJH-Orange patients admitted for severe sepsis and septic shock were admitted through the emergency department.
The critical status of these patients with sepsis necessitates early identification, implementing timely goal directed therapies, and admission to critical care or stepdown for further monitoring and treatment. For inpatients, deterioration in the patient’s condition and the ability to recognize signs of early sepsis is crucial to initiating early treatment.
To decrease the sepsis mortality risk adjusted, observed to expected (O/E), from 1/15 in November 2015 to <= 0.94 by April 31/, 2016.
Aim Statement
Interventions
Next Steps
Lessons Learned
Run Charts
I: One to one physician education
S: Mandatory nursing education
S: Electronic sepsis screens
S: Standardized order sets
S: Concurrent review of patient records
I: Standardized procedures for Sepsis RN
I: 24/7 Sepsis RN
Gather evidence-based research and baseline data prior to the first meeting. Select team members (stakeholders) and educate them on why it’s important they attend.
Engage frontline staff on your committee.
Incentivize physician committee members with small stipends to help offset their personal cost of attendance.
Test all electronic interventions from all points of view.
Share the story: When those perfect cases are reviewed, make a big deal about it. When incredibly sick patients survive, let the care team know the difference they made in that patient’s life.
Phase II of our sepsis mortality reduction efforts includes developing criteria for admission to varies nursing units, managing patient/family expectations, developing criteria for downgrading a patient’s status, and definitive discharge criteria.
Phase III will address Post Sepsis Syndrome.
Team MembersPeter Smethurst, MD, Intensivist (project champion)Cecille Lamorena, CCRN, (nursing champion) Katie Skelton, CNO (senior leader sponsor) ED physicians and RNs; ICU RNs; Intensivists; Quality RN; Data Analyst; and Hospitalists.
Reducing Sepsis MortalitySt. Joseph Hospital
Orange, CA
Background & Problem Overview
References
CDC, Surviving Sepsis Campaign
Mortality Jul-15
Aug-15
Sep-15
Oct-15
Nov-15
Dec-15
Jan-16
Feb-16
Mar-16
Apr-16
FYTD
Sepsis Mortality Rate O/E 0.88 0.39 0.56 0.74 1.15 0.71 0.95 1.00 1.01 0.51 0.80
30 Lives Saved!
Achieved: FY2016 risk adjusted sepsis mortality rate 0.80 which represents 20% fewer deaths than expected)
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
Ob
serv
ed t
o E
xpec
ted
Mo
rtal
ity
Rat
e Sepsis Mortality

“Hospitalized patients at high-risk for VTE may develop an asymptomatic deep vein thrombosis (DVT), and die from pulmonary embolism (PE) even before the diagnosis is suspected. The majority of fatal events occur as sudden or abrupt death, underscoring the importance of prevention as the most critical action step for reducing death from PE (Geerts, 2008).” (CMS, 2015) The Agency for Healthcare Research and Quality indicates that “the appropriate application of effective preventive measures in hospitals has major potential for improving patient safety by reducing the incidence of venous thromboembolism” (Shojania, 2001).” (CMS, 2015)
Reduce the VTE rate from 2015 baseline of <= .778 in the PSI-90 composite to <= to 6 for the PSI-12 (postop VTE) rate which represents a 23% improvement.
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
S: Force function VTE prophylaxis order sets.S: Concurrent record review for VTE prophylaxis.I: EMR revisions to nursing census boards (timed observations showed 79 seconds to determine VTE prophylaxis needs for an entire 36 unit).T: Standardized procedure (STP) for nursing to implement mechanical prophylaxis for all adult inpatients without contraindications.
Mechanical VTE prophylaxis devices were placed in the OR. The devices followed the patient, but the order did not.
Physicians would round on patients, see compression devices in use, and be confused when nursing asked for an order for compression devices.
This was a dissatisfier for nursing and physicians and led to the development of the STP.
Spread use of VTE Status Board in EMR to all nursing units.
Implement nursing VTE prophylaxis STP throughout the hospital.
Test use of portable mechanical VTE prophylaxis devices.
Team Members
Dr. Alex Ramirez and Peggy Walsh, RN (co-chairs)Tom Hill, VP Operations (senior leader sponsor)Dr. Hisham El Bayar (physician champion) Nursing managers, service line managers, clinical education, quality RNs, and data analysts.
VTE PreventionSt. Joseph Hospital
Orange, CA
Achieved: Postop VTE rate of .58 Note: There was one postop VTE . Drilldown of this event reflected patient developed a postop VTE despite being prophylaxed per protocol.
Background & Problem Overview
ReferencesAmin A, Spyropoulos AC, Dobesh P, et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE start). J Thromb Thrombolysis. 2010; 29:326-339.
Caprini JA, Arcelus JI. State of the art venous thromboembolism prophylaxis. SCOPE on Phlebology & Lymphology 1:2005, 228-240.
Cohen AT, Tapson VF, Bergmann JF, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371:387-394.
Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, Colwell CW. Prevention of venous thromboembolism. The Eighth ACCP Conference on antithrombotic and thrombolytic therapy. Chest. 2008; 133:381S-453S.
Guyatt, G.H., Akl, E.A., Crowther, M., Gutterman, D., Schunemann, H. Antithrombotic Therapy and Prevention of Thrombosis, 9th edition: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST 2012; 141(2)(Supp):7S-47S.
Heit JA, Silverstein MD, Mohr DN, Petterson TM, et al. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med 2000: 160:809-15.
Kucher N, Koo S, Quiroz R, Cooper JM, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. New England Journal of Medicine. 2005, 352(10), 969-1036.
National Quality Forum. National Voluntary Consensus Standards for Prevention and Care of Venous Thromboembolism: Policy, Preferred Practices, and Initial Performance Measures. A Consensus Report. Washington, DC. NQF; 2006.
Schleyer AM, Schreuder AB, Jarman KM, et al. Adherence to guideline-directed venous thromboembolism prophylaxis among medical and surgical inpatients at 33 academic medical centers in the United States. Am J Med Qual. 2011; 26:174-80.
Tooher R, Middleton P, Pham C, Fitridge R, et al. A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals. Ann Surg 2005; 241:397-415.
Measure Goal Jul-15
Aug-15
Sep-15
Oct-15
Nov-15
Dec-15
Jan-16
Feb-16
Mar-16
Apr-16
May-16
FYTD
PSI-90Composite
Score<= .778 .731 .547 .733 .464 .468 .655 .482 .629 .463 .641 .571 .590
PSI-12 Postop VTE <=6 0 0 0 0 0 0 0 1 0 0 0 1

Reduce CDI hospital acquired infections to below National Health and Safety Network (NHSN) 90th percentile by December 2016.
For whom?
Aim Statement
Interventions
Next Steps
Lessons LearnedRun Charts
Developed interdisciplinary CDI Reduction team with frontline staff -I
EVS partnership- for process improvement S
Summary of tests of change:
• Shoe covers in CDI rooms over alcohol gel- S
• Stop signs on isolation carts to notify visitors to speak to nurse prior to entering isolation room-S
• Protocol for nurses to screen for C. difficile when criteria met-S
• Created responsibility list of hospital items to be cleaned, i.e. by nursing or EVS. I
• Send letters to PCP when patient admitted with C. difficile to increase awareness- T
Physician partnership in projects is essential.
Frontline staff are powerful in communicating & creating change.
Use electronic automation to it’s fullest extent.
Continuous education on nursing protocol is essential for successful sustainment.
Prevention strategies for C. difficile include antimicrobial stewardship.
Increase partnership and awareness of out-patient physicians to reduce antimicrobial prescriptions where possible.
Recommendation: Increase awareness of risk of C. difficile.
Team Members
Project Sponsor: Teresa FreyPhysician Champion: Sajen Mathews, M.DPhysician Champion: Pauline Ho, M.d.Project Manager: Claudia Skinner, RN ,Selin Mirzaeian, RNCDI Reduction Team: Disciplines include nursing, EVS, Education Department, physicians
C. difficile Reduction (CDI)St. Jude Medical Center
Fullerton, CAHospital Logo
Background & Problem Overview
References
CDI is considered an urgent threat to public safety by the CDC. It is estimated that almost half a million infections occur in the U.S. in a single year, with 15,000 deaths attributable to CDI.
http://www.cdc.gov/drugresistance/biggest_threats.html