-
8/7/2019 calcium met 3
1/67
MODERATORS
PROF DEEPAK RAI
DR MAHESHA K
PRESENTER: DR NABEEL SHAMS
-
8/7/2019 calcium met 3
2/67
INTRODUCTION
-
8/7/2019 calcium met 3
3/67
` Calcium -most abundant mineral in the human
body.
` 1.5%- total body weight.
` Along with phosphorous it forms the principal
contituents of the bone.
` Normal serum level 9-11mg/dl
-
8/7/2019 calcium met 3
4/67
` Calcium is an divalent cation with multiple roles in
vertebrate physiology
` They can be grouped as either structural or
metabolic
-
8/7/2019 calcium met 3
5/67
-
8/7/2019 calcium met 3
6/67
1.Dietary source` Whole milk 10%
` Low fat milk 18%
` Cheese 27%
` Other dairy products 17%
` Vegetables 7%(Spinach, Turnip, Cabbage, Soya beans)
2. From bones- Resorption`
-
8/7/2019 calcium met 3
7/67
`DISTRIBUTION OF CALCIUM
-
8/7/2019 calcium met 3
8/67
` 1) calcium in plasma
` 2) calcium in bones
-
8/7/2019 calcium met 3
9/67
`
` About 41% combined - plasma proteins
nondiffusible form
` About 9% combined- anionic substances of theplasma and
interstitial fluids (citrate and phosphate,
for instance)
` Remaining 50%- both diffusible through the
capillary membrane and ionized
-
8/7/2019 calcium met 3
10/67
` The ionised calcium concentration in serum is
approximately 5mg/dl.
` It is the ionised fraction that is biologically activeand is
closely regulated
-
8/7/2019 calcium met 3
11/67
-
8/7/2019 calcium met 3
12/67
i) Rapidly exchangeable calcium
ii) slowly exchangeable calcium
-
8/7/2019 calcium met 3
13/67
` i) The rapidly exchangeable calcium- maintains
the plasma calcium level
ii) The slowly exchangeable calcium-
bone remodelling
-
8/7/2019 calcium met 3
14/67
MEN 400 mg
WOMEN 400mg
PREGNANT WOMEN 1000mg
-
8/7/2019 calcium met 3
15/67
` ABSORBTION AND EXCRETION
-
8/7/2019 calcium met 3
16/67
-
8/7/2019 calcium met 3
17/67
-
8/7/2019 calcium met 3
18/67
-
8/7/2019 calcium met 3
19/67
` Calcium ions-poorly absorbed from the intestines
` Vitamin D promotes calcium absorption from the
intestines
` Majority of absorbtion takes place from the 1st and
2nd psrt of deudenum
-
8/7/2019 calcium met 3
20/67
About 35% of injested calcium is usually
absorbed and the remaining is excreted in faeces
In contrast the absorbtion of phoshate from the
intestines occurs very easilyAbout 10% of the injested calcium
is excreted in
urine
98-99% -reabsorbed from renal tubules
-
8/7/2019 calcium met 3
21/67
` Majority of reabsorbtion-distal convolutedtubules and proximal
part of collecting duct
` The bone contains a type of exchangeablecalcium that is always
in equilibrium with calcumions in the extra cellular fluid
The exchangeable calcium provides an bufferingmechanism to
maintain the calcium ionconcentration
-
8/7/2019 calcium met 3
22/67
Parathormone and Vit D play a major role
-
8/7/2019 calcium met 3
23/67
` FACTORS AFFECTNG CALCIUM ABSORBTION
-
8/7/2019 calcium met 3
24/67
` Factors causing increased absorbtion
` a) Vit D
` b) PTH
` c) Acidity` d) Amino acids
-
8/7/2019 calcium met 3
25/67
Factors causing decreased absorbtion
a)Phytic acid ( present in cereals)
b)Oxalates( leafy vegetables- formation ofinsoluble calcium
oxalates)
c) Malabsorbtion syndromes
d) Phosphate: optimum ratio of calcium tophosphorus alowing
maximum absorbtion is 1:2 to2:1
-
8/7/2019 calcium met 3
26/67
` REGULATION OF THE BLOOD CALCIUM
LEVEL
-
8/7/2019 calcium met 3
27/67
` Calcium metabolism is mainly regulated by
` Parathormone
` 1,25 dihydroxycholecalciferol(calcitriol)
` Calcitonin
-
8/7/2019 calcium met 3
28/67
-
8/7/2019 calcium met 3
29/67
` PARATHORMONE
-
8/7/2019 calcium met 3
30/67
` Parathhormone secreted by chief cells of the
parathyroid gland
` The pricipal regulator of PTH secretion is the ECFionised
calcium concentration
` The regulation of PTH is mediated by calcium
sensing receptor( CASR)
-
8/7/2019 calcium met 3
31/67
` Plasma PTH concentrations exhibit diurnal
variation
` They are stable during the afternoon and evening
` They rise around 50% around 2:00 am andsubsequently fall below
50% of the afternoon
values by 9:00am
-
8/7/2019 calcium met 3
32/67
` Parathyroid hormone binds to cell surface
receptors in its target tissues
` The two principal target tissues are bone and
kidney where it activates adenylate cyclase and
phospholipase C
-
8/7/2019 calcium met 3
33/67
` ACTIONS OF PARATHORMONE
-
8/7/2019 calcium met 3
34/67
` On bone
` - stimulates osteoclastic activity hence
enhances the resorption of calcium from the
bones
` Resorption of calcium- two phases
` a) Rapid phase
` b) Slow phase
-
8/7/2019 calcium met 3
35/67
` Rapid phase- occurs within minutes
` causes increased permeability of
osteoclasts and osteoblasts for calcium
` Slow phase- Occurs by activation of osteoclasts
` When the osteoclasts get activated they
release proteolytic enzymes and acids leading to
digestion of the organic matrix
-
8/7/2019 calcium met 3
36/67
` On kidneys-
` a) Reduces proximal tubular resorbtion of
phosphate
` b) Increases the distal tubular reabsorption of
calcium
` c) Formation of 1,25-dihydroxycholecalciferol from
25-hydroxycholecalciferol
-
8/7/2019 calcium met 3
37/67
` On GI tract
`
` PTH increases the absorption indirectly by forming
1,25-dihydrocholecalciferol in the kidneys
` PTH causes activation of Vit D
-
8/7/2019 calcium met 3
38/67
` Parathormone-controls extracellular calcium and
phosphate concentrations
` Excess activity- hypercalcemia
` Reduced activity- hypocalcemia
`
-
8/7/2019 calcium met 3
39/67
HYPERCALCEMIA
-
8/7/2019 calcium met 3
40/67
` 1. Parathyroid related
` a) Primary hyper parathyroidism
` b) Lithium therapy
` c) Familial hpercalciuric calciuria` 2. Malingnancy
related
` 3. Vit D realted
` 4. Associated with high bone turnover
` 5. Associated with renal failure
`
-
8/7/2019 calcium met 3
41/67
` Mild hypercalcemia often asymptomatic
` Symptoms occur if calcium >12mg/dl
` They include- constipation, polyuria, nausea
vomiting, peptic ulcer desease, weakness,
lethargy
-
8/7/2019 calcium met 3
42/67
` Forced calciuresis
` In case of dehydration 0.9% salinerapidly(250ml/hr)
` Bisphosphonates for hypercalcemia of malignancy
-
8/7/2019 calcium met 3
43/67
` HYPOCALCIMEA
-
8/7/2019 calcium met 3
44/67
` A)Decreased intake or absorption
` B)Increased loss
` C)Endocrine desease
` D)Others
-
8/7/2019 calcium met 3
45/67
` Primarily affects the neuromuscular and
cardiovascular systems
` A) Cardiovascular changes:
` Dilatation of the heart
` Prolonged duration of the ST segment and QT
interval` Arrythmias
-
8/7/2019 calcium met 3
46/67
` B) Neuromuscular changes:
` Hyper reflexia and convulsions
` Carpopedal spasm` Laryngeal stridor
` Physical findings- Chovstek sign and
Trousseaus sign
-
8/7/2019 calcium met 3
47/67
In severe symptomatic hypocalcimea-
10mg/kg of 10% calcium gluconate in one litre
of Dextrose infusion over 4-5 hours
In asymtomatic Hypcalcimea- Oral calcium 1-2gm
and vit d preparations
-
8/7/2019 calcium met 3
48/67
` Resorption of calcium from the bones
` Resorption of calcium from the renal tubules
` Absorbtion of calcium from the GI tract
-
8/7/2019 calcium met 3
49/67
` CONTROL OF PARATHYROIDSECRETION BY CALCIUM IONS
-
8/7/2019 calcium met 3
50/67
-
8/7/2019 calcium met 3
51/67
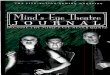
` The solid curve shows the acute effect when the
calcium concentration is changed over a period of
a few hours
`
` the calcium ion concentration changes over a
period of many weeks is shown by the dashedline.
-
8/7/2019 calcium met 3
52/67
` 1,251,25--DIHYDROXYCHOLECALCIFEROLDIHYDROXYCHOLECALCIFEROL
-
8/7/2019 calcium met 3
53/67
` Vitamin D- calcium absorption from the intestinal
tract
` vitamin D must first be converted the final active
product, 1,25-dihydroxycholecalciferol
-
8/7/2019 calcium met 3
54/67
-
8/7/2019 calcium met 3
55/67
-
8/7/2019 calcium met 3
56/67
` Promotes intestinal calcium absorption
` Promotes phosphate absorption by the intestines
` Decreases renal calcium and phosphate excretion
-
8/7/2019 calcium met 3
57/67
` CALCITONIN
-
8/7/2019 calcium met 3
58/67
` Secreted by parafollicular in the thyroid gland
` Plasma level of calcitonin is 1-2 mg/dl
` Degraded and excerted by liver and kidney
-
8/7/2019 calcium met 3
59/67
` On bones- stimulates osteoblastic activity
` On kidney inhibits the resorption of calcium fromrenal
tubules
` On intestine: prevents the absorption of calcium
-
8/7/2019 calcium met 3
60/67
` Bone is composed a) organic matrix
b)calcium salts
-
8/7/2019 calcium met 3
61/67
` Organic matrix- composed 95% of collagen fibers
and the rest ground substance
` Bone salts are deposited in the organic matrix
which are primarily calcium and phosphate
-
8/7/2019 calcium met 3
62/67
` -95% are collagen fibres, They give tensile
strength to the bone
` -The rest is homogenous gelatinous medium
called ground substance
-
8/7/2019 calcium met 3
63/67
` COMPOSED PRINCIPALLY OF CALCIUM AND
PHOSPHATE
-
8/7/2019 calcium met 3
64/67
` OSTEOBLASTS
` OSTEOCYTES
` OSTEOCLASTS
-
8/7/2019 calcium met 3
65/67
` Conversion of cartilage into bone ossification
` Ossification carried out by osteoblasts which laydown the
matrix
` Calcium is deposited in the matrix- calcification
-
8/7/2019 calcium met 3
66/67
` a) Bone and teeth formation
` b) Neuronal activity
` c) Skeletal muscle activity
`
d) Cardiac activity
` e) Smooth muscle activity
` f) Secretory activity of the glands
` g) Cell division and growth
` h) Coagulation of blood
-
8/7/2019 calcium met 3
67/67