Embed Size (px)
Citation preview

CASE REPORT
24 PRACTICAL NEUROLOGY MAY 2019
CaseClinical PresentationMr L is age 41 with a history of multiple sclerosis (MS), bipo-
lar disorder, and parkinsonism that has persisted despite being off neuroleptics for 1.5 years (Figures 1 and 2). He presented with right hemiparkinsonism characterized by a moderate
amplitude rhythmic resting, postural and action hand tremor, moderate bradykinesia, and cogwheel rigidity at the wrist and elbow. His right leg and arm swing were depressed.
HistoryAt age 35, Mr. L was diagnosed with MS after he pre-
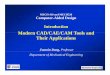
sented with diplopia and his brain MRI findings showed demyelinating lesions in the brain (Figure 1), cervical, and thoracic spinal cord as well as unmatched oligoclonal bands in his cerebrospinal fluid. At that time, his diplopia improved spontaneously and he was started on fingolimod to treat his MS.
Hemiparkinsonism in a Patient With Multiple Sclerosis In this case, there was a causal relationship between comorbid diseases.
By Andrea P. Lee, MD; Giulietta M. Riboldi, MD; Ilya Kister, MD; Jonathan E. Howard, MD; and Ritesh A. Ramdhani, MD
Figure 1. Imaging assessments before and after the onset of parkinsonian symptoms: Axial (A) and coronal (B) T2 FLAIR sections
before the onset of hemiparkinsonism.
A B

CASE REPORT
MAY 2019 PRACTICAL NEUROLOGY 25
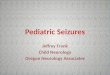
Figure 2. Axial T2 FLAIR (A) and coronal T1 (B) sections of brain MRI performed after patient developed right-sided hemiparkinsonism.
A new left hyperintense lesion is visible in the left globus pallidus with peripheral ring enhancement (B). Follow-up brain MRI (C,
D) at the time the patient was evaluated by a movement disorder specialist. Axial FLAIR MRI (C) shows a left pallidal lesion without
gadolinium enhancement (D).
A
B
C
D

CASE REPORT
26 PRACTICAL NEUROLOGY MAY 2019
A year later, Mr. L developed mania and was diagnosed with bipolar disorder. He was initially treated with olanzap-ine and aripiprazole and then transitioned to aripiprazole and lithium. At age 37, 2 years later, he developed a right-hand action tremor.
By age 40, Mr. L’s tremor was reportedly worse and he complained of a decline in dexterity of his right hand with reduction in size of his handwriting and worsening gait. His neuroleptics had been discontinued. Brain MRI findings then showed new demyelinating lesions with discontinu-ous rim enhancement in the left globus pallidus, left fron-tal centrum semiovale, and right periatrial white matter MRI (Figure 2A-D, p. 25).
TreatmentConsidering Mr. L’s history and continued parkinsonian
symptoms despite not taking neuroleptics, lithium treat-ment was tapered and discontinued.
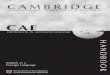
Follow Up, Diagnosis, and Further ManagementApproximately 10 months later, Mr. L had an ioflupane
dopamine transporter scan (DaTSCAN) with normal pre-synaptic dopamine transporter uptake findings (Figure 3). His rest tremor, bradykinesia, and rigidity were unchanged, although his action tremor had improved. Levodopa or other dopaminergic agents were not initiated out of con-cern for worsening mania.
OutcomeMr. L was subsequently treated with quetiapine 100 mg
daily. His parkinsonism has not worsened in over 2 years.
DiscussionMultiple sclerosis (MS) is an autoimmune demyelinating
disease that commonly causes white matter plaques, but deep grey matter nuclei can also be affected. MS manifests with a wide range of neurologic symptoms depending on the location of lesions. Parkinsonism is rarely comorbid with MS. Here we present a case of MS causing hemiparkinson-ism, which developed subacutely in the context of an acute demyelinating lesion in the contralateral basal ganglia.
Parkinsonism associated with multiple sclerosis has been previously reported in the literature—implicated as both coincidental and causal.1,2 Coincidentally occurring parkin-sonism with MS is supported by absence of demyelinating lesions in the basal ganglia on MRI, with abnormal uptake on DaTSCAN.2-4 Evidence for a causal relationship includes a strategically placed plaque in the basal ganglia-thalamo-cortical network that is time locked to the onset of parkin-sonism, which subsequently improves with high-dose cor-ticosteroids.1,5,6 Although hemiparkinsonism can be seen in idiopathic Parkinson’s disease, secondary etiologies such
as tumors and vascular insults have been reported.7-9 The temporal relationship of bradykinesia onset in our patient with an active demyelination in contralateral globus pal-lidus as well as lack of symptom progression over 2 years of follow up support the hypothesis that heimparkinson-ism was caused by a demyelinating plaque. A normal DaTSCAN suggests postsynaptic dopaminergic dysfunction related to the lesion and makes coincidental Parkinson’s disease unlikely. The diagnosis of drug-induced parkin-sonism (DIP) is unlikely, because his symptoms occurred 1.5 years after discontinuing olanzapine and aripiprazole and did not improve following lithium taper. Furthermore, to our knowledge, DIP rarely causes hemiparkinsonism. Of note, quetiapine, which has a low propensity to cause DIP, was added a year after the symptoms developed, without any adverse effect on parkinsonian symptoms. A system-atic analysis is warranted to determine whether a higher incidence of parkinsonian symptoms in MS patients with plaques within basal ganglia-thalamocortical network may exist and whether dopamine receptor-blocking agents can unmask parkinsonism in such MS patients. n
Figure 3. Ioflupane dopamine transporter scan (DaTSCAN).
Presynaptic dopamine uptake is preserved on both sides.
(Continued on page 67)

MAY 2019 PRACTICAL NEUROLOGY 67
CASE REPORT
1. Etemadifar M, Afshar F, Nasr Z, Kheradmand M. Parkinsonism associated with multiple sclerosis: a report of eight new cases and a review on the literature. Iran J Neurol. 2014;13(2):88-93.
2. Pedemonte E, Trabucco E, Cella M. et al. Parkinsonism in multiple sclerosis patients: a casual or causal association? Parkinsonism Rel Dis. 2013(4);19:492-493.
3. Barun B, Brinar VV, Zadro I, et al. Parkinsonism and multiple sclerosis—is there association? Clin Neurol Neurosurg. 2008;110(9):958-961.
4. Damasio J, Ramos C, Valdemar L, da Silva AM, Magalhães M. A coincidental case of young-onset Parkinson disease and multiple sclerosis. Neurologist. 2011;17(5):286-288.
5. Folgar S, Gatto EM, Raina G, Micheli F. Parkinsonism as a manifestation of multiple sclerosis. Mov Disord. 2003;18(1):108-110.6. Saidha S, Mok TH, Butler M. et al. Multiple sclerosis exceptionally presenting as parkinsonism responds to intravenous
methylprednisolone. J Clin Neurosci. 2010;17(5):654-655.7. Ho BL, Lieu AS, Hsu CY. Hemiparkinsonism secondary to an infiltrative astrocytoma. Neurologist. 2008;14(4):258-261.8. Norris SA, Derdeyn CP, Perlmutter JS. Levodopa-responsive hemiparkinsonism secondary to cystic expansion from a coiled
cerebral aneurysm. J Neuroimaging. 2015;25(2):316-318.9. Robles LA. Pure hemiparkinsonism secondary to contralateral lacunar stroke in the substantia nigra. J Stroke Cerebrovasc Dis.
2016;25(2):e20-21.
Andrea P. Lee, MDDepartment of NeurologyWeill Cornell Medical CenterNew York, NY
Giulietta M. Riboldi, MD Fresco Institute for Parkinson’s and Movement DisordersDepartment of NeurologyNew York University Langone HealthNew York, NY
Ilya Kister, MDDepartment of NeurologyNew York University Langone HealthNew York, NY
Jonathan E. Howard, MDDepartment of NeurologyNew York University Langone HealthNew York, NY
Ritesh A. Ramdhani, MDDepartment of NeurologyDonald and Barbara Zucker School of Medicine at Hofstra/NorthwellNew York, NY
DisclosuresAPL and GMR contributed equally to the manuscript. The authors have no financial or other relationships rel-evant to this content to disclose.
(Continued from page 26)