Embed Size (px)
Citation preview
CADCA Mid-Year Training Institute
What’s Trending in Tobacco:
E-cigarettesWednesday, July 23, 2014 - Orlando, FL
Christine Cheng, Partner Relations Director

Overview• History: invented by a Chinese pharmacist in 2003
• Rapid evolution of devices: a moving target
• Poll questions
• YouTube videos: from Consumer Reports, http://
www.youtube.com/watch?v=100b-l_0z9s from CNN, http://
www.youtube.com/watch?v=EqvlxEQaQnE2
Poll Questions1. Show of hands, how many have tried an
e-cigarette?
2. How open are you to discussing the potential benefits and risks of e-cigarettes as a smoking cessation tool?
3. Are you willing to incorporate e-cigarettes into a smoking cessation treatment plan?
3

E-cigarette Devices Currently Available
4
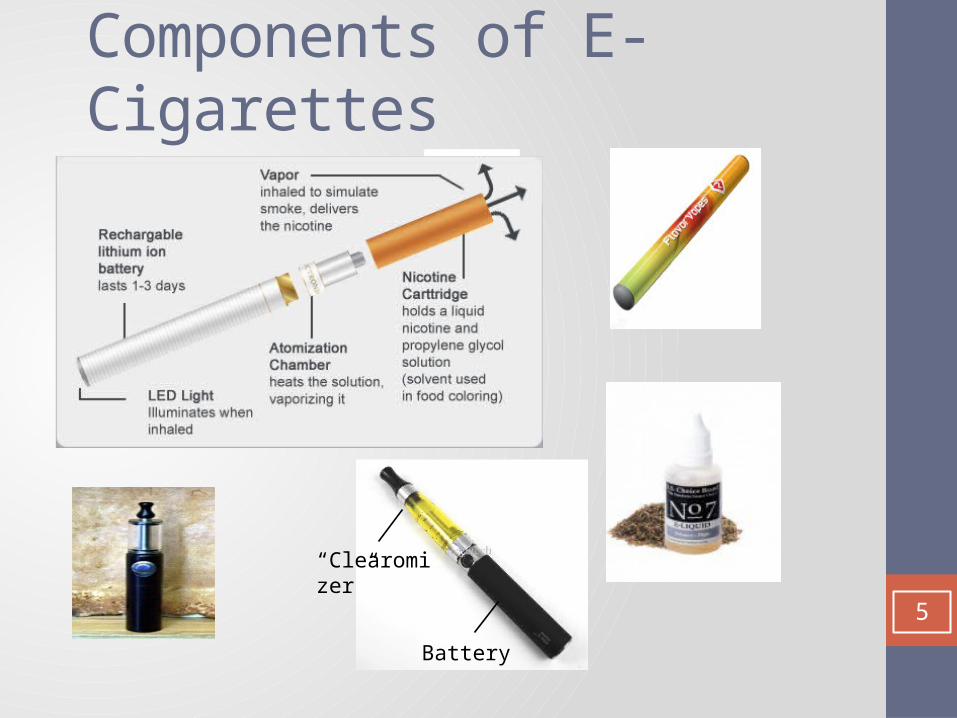
Components of E-Cigarettes
Battery
“Clearomizer”
Battery
5
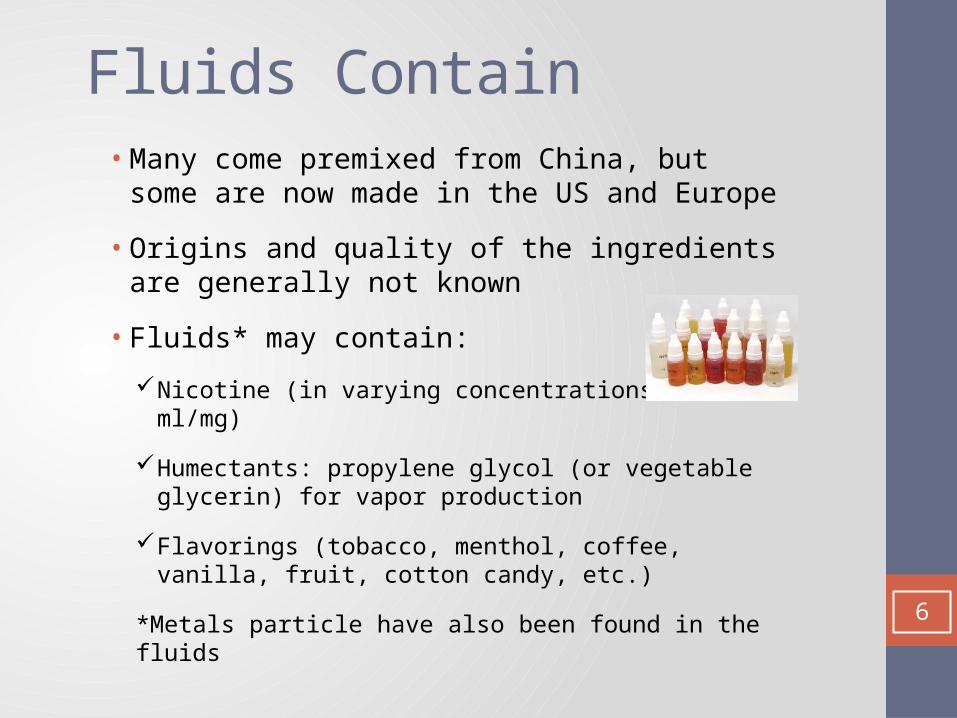
Fluids Contain• Many come premixed from China, but some are
now made in the US and Europe
• Origins and quality of the ingredients are generally not known
• Fluids* may contain:
Nicotine (in varying concentrations 0-100 ml/mg)
Humectants: propylene glycol (or vegetable glycerin) for vapor production
Flavorings (tobacco, menthol, coffee, vanilla, fruit, cotton candy, etc.)
*Metals particle have also been found in the fluids6

“Harmless” Vapor
7
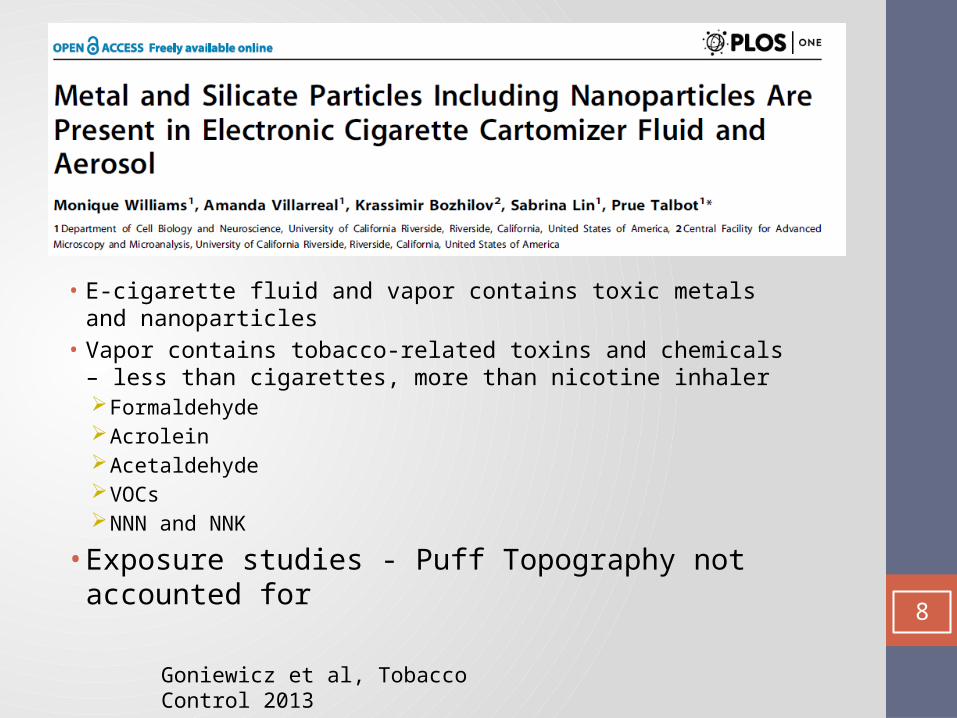
• E-cigarette fluid and vapor contains toxic metals and nanoparticles• Vapor contains tobacco-related toxins and chemicals – less than
cigarettes, more than nicotine inhaler Formaldehyde Acrolein Acetaldehyde VOCs NNN and NNK
• Exposure studies - Puff Topography not accounted for
Goniewicz et al, Tobacco Control 2013
8

9

E-cigarette User’s Exhale
10

Look Familiar?
Videos from www.smokestik.com Image from www.ecigaretteschoice.com; www.v2cigs.com
11

12

What Attracts and Sells
http://www.npr.org/2014/03/03/284006424/e-cigarette-critics-worry-new-ads-will-make-vaping-cool-for-kids
13

Cost Savings Claims
http://tobacco.stanford.edu/tobacco_main/index.php
14

15
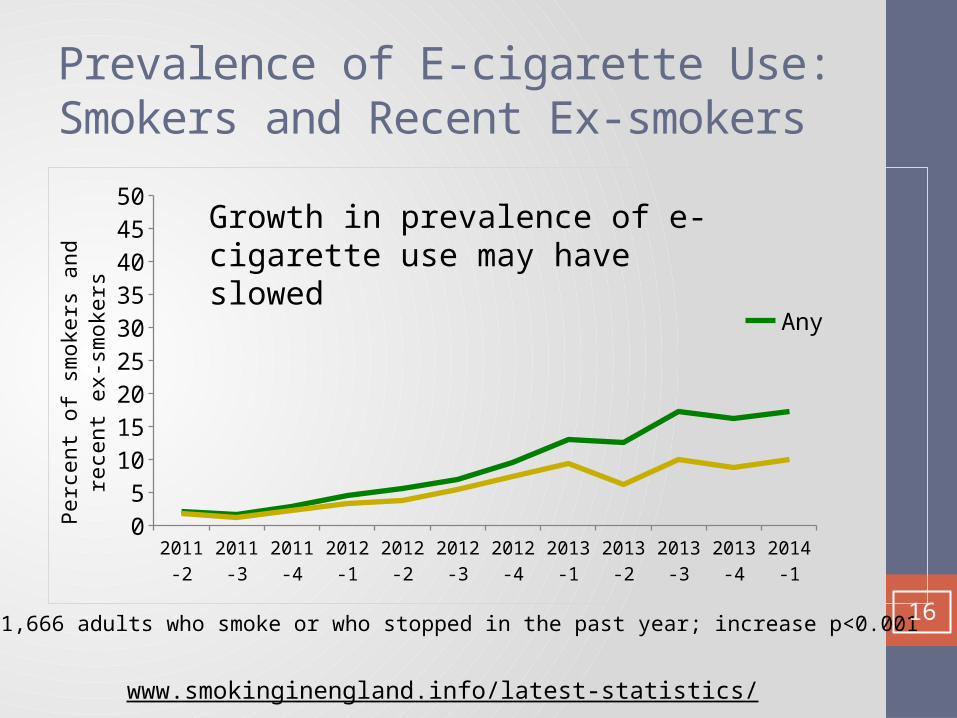
Prevalence of E-cigarette Use: Smokers and Recent Ex-smokers
2011-2
2011-3
2011-4
2012-1
2012-2
2012-3
2012-4
2013-1
2013-2
2013-3
2013-4
2014-1
05
101520253035404550
AnyDaily
Perc
ent o
f sm
oker
s and
rece
nt e
x-sm
oker
s
N=11,666 adults who smoke or who stopped in the past year; increase p<0.001
Growth in prevalence of e-cigarette use may have slowed
www.smokinginengland.info/latest-statistics/
16
Clinical Scenario #1
“I’m a heavy smoker and both my parents were smokers who died of lung cancer. I’ve tried all the meds but never quit for more than a week. I’ve heard that e-cigarettes can help smokers to quit and I really want to give it a shot. What can you tell me about them?”
17
Clinical Scenario #1 Response1. Support Quit Attempt 2. Assess motivation and dependence3. Assess prior quit attempts and inform
about all treatment/support options4. Inform on what we know and what we
don’t know about e-cigarettes5. Assist smoker to develop a plan to quit
smoking6. Arrange a follow-up 18
Clinical Scenario #2• 50 y.o. primary care patient with back pain,
hypertension, hyperlipidemia, depression and PTSD, here for routine follow up, incidentally noted she is still smoking 3 to 5 cpd, reduced from 10 cpd• She quit once “cold turkey” for 9 months 2 years ago• “not interested” in any medications, counseling, or
nicotine replacement• She is willing to set a quit date in the next 30 days
(her son’s birthday) and remarks, “Maybe I’ll get one of those electric cigarettes to quit, what do you think?” 19
“not interested”
• “I’ve tried everything” • Frequently NRT misused or incorrectly used• Unassisted quit attempts
• Correct misperceptions of approved therapies• Correct misperceptions of e-cigarettes• Treat Depression, PTSD
Shiffman S, Ferguson SG, Rohay J, Gitchell JG. Perceived safety and efficacy of nicotine replacement therapies among US smokers and ex-smokers: relationship with use and compliance. Addiction. 2008 Aug;103(8):1371-8
20
Clinical Scenario #2 Response1. Opportunity to engage patient in
counseling2. This is a “light” smoker 3. Significant psychiatric history4. ASK: why is she interested in e-cigarette?5. What does she think is different from
approved therapies?6. History of past quit attempts and
assistance? 21
Clinical Scenario #2 Follow Up
• This patient ended up with • Nicotine inhaler prescription (unfilled)
• Quit with nicotine gum and counseling on proper use• Saw a therapist to help manage stress• Remains tobacco free today
22
Clinical Scenario #3• 21 y.o. female presents for work physical for
restaurant job. Denies significant past medical history except asthma, treated with Albuterol (once or twice a day)• Denies smoking. Drinks 4-5 alcoholic drinks on
weekends. Has been using a vapor pen when out at parties sometimes. • She lives with her mom and 5 siblings. Mom (39)
recently quit smoking using an e-cigarette, which she continues to use. • Is her nicotine exposure significant? How do you
counsel her?23
Clinical Scenario #3 Background1. Screening challenges2. Binge drinkers frequently smoke 3. May present themselves as nonsmokers4. Need to screen specifically (only smokes
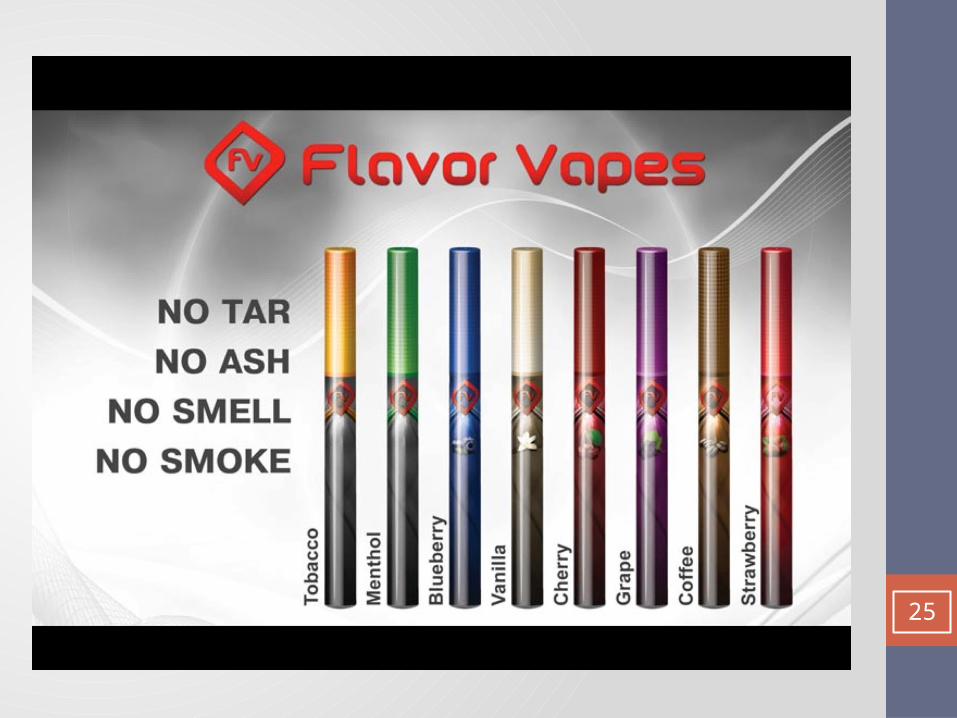
when drinks)5. Vapor pens = e-cigarettes6. Also e-hookah, vapes, sticks, hookah pens7. Recreational use common8. Young adults have highest rates of use9. May lead to or increase nicotine addiction
24
25

23 million likes on FB10 million Twitter followers
26
Clinical Scenario #3 Asthma1. Inadequately controlled2. Personalized reason not to smoke or be
exposed to secondhand smoke or aerosol3. One study found acute pulmonary effects4. 5 minutes of e-cigarette use in healthy
smokers increased airway resistance5. Unknown clinical significance6. May affect susceptible people
27
Clinical Scenario #3 Response1. Discourage recreational “vapor pen” use2. Personalize to patient’s medical conditions3. Fetal exposure to nicotine not harmless4. Support mom’s quit attempt!5. Preserve smoke – and vapor free homes6. E-cigarettes are not harmless toys
28
• Average 1 per month increased to 215/month• Most common adverse events were vomiting, nausea,
and eye irritation29
Advice for Provider
• Screen for poly tobacco use including e-cigarettes• Field and devices are rapidly evolving• Engage with new opportunities to discuss
smoking cessation• Misinformation and false claims are rampant• Data are scarce • Continue to recommend approved NRTs and Rx• Monitor use in your clients, document and report
health concerns 30
Advocacy and Coalition Action
• Include e-cigarettes in tobacco free policies• Prohibit cessation and health claims• Apply cigarette advertising restrictions to
electronic cigarettes
31
Contact SCLC for Technical Assistance
Visit us online
• http://smokingcessationleadership.ucsf.edu
Call us toll-free
• 1-877-509-3786
Christine Cheng
• email: [email protected]