Embed Size (px)
DESCRIPTION
dental
Citation preview

The Journal of Prosthetic Dentistry
35January 2012
Goodacre et alGoodacre et al
The clinical impression procedures described in this article provide a method of recording the morphology of the intaglio and cameo surfaces of complete denture bases and also identify muscular and phonetic locations for the prosthetic teeth. When the CAD/CAM technology for fabricating complete dentures becomes commercially available, it will be possible to scan the denture base morphology and tooth positions recorded with this technique and import those data into a virtual tooth arrangement program where teeth can be articulated and then export the data to a milling device for the fabrication of the complete dentures. A prototype 3-D tooth arrangement program is described in this article that serves as an example of the type of program than can be used to arrange prosthetic teeth virtually as part of the overall CAD/CAM fabrication of complete dentures. (J Prosthet Dent 2012;107:34-46)
CAD/CAM fabricated complete dentures: concepts and clinical methods of obtaining required morphological data
Charles J. Goodacre, DDS, MSD,a Antoanela Garbacea, DDS,b W. Patrick Naylor, DDS, MPH, MS,c Tony Daher, DDS, MSEd,d Christopher B. Marchack, DDS,e and Jean Lowry, PhDf
Loma Linda University School of Dentistry, Loma Linda, Calif; Loma Linda University School of Allied Health Professions, Loma Linda, Calif; University of Southern California School of Dentistry, Los Angeles, Calif
Presented at the Academy of Prosthodontics meeting, Hilton Head, NC, May 6, 2011.
aProfessor, Department of Restorative Dentistry, Loma Linda University School of Dentistry.bAdvanced Education Student, Implant Dentistry and Prosthodontics, Loma Linda University School of Dentistry. cAssociate Dean for Advanced Dental Education; Professor, Department of Restorative Dentistry, Loma Linda University School of Dentistry.dAssociate Professor, Department of Restorative Dentistry, Loma Linda University School of Dentistry.eAssociate Clinical Professor, Advanced Prosthodontics, University of Southern California School of Dentistry.fEmeritus Professor, Speech-Language Pathology, Loma Linda University School of Allied Health Professions.
The acronym CAD/CAM repre-sents Computer-Aided Design (CAD) and Computer-Aided Manufactur-ing (CAM). In some industries, an equivalent term, CAD/NC (Numerical Control) is used. With this design and manufacturing technology, CAD soft-ware defines the geometry of an ob-ject while CAM programming directs the fabrication process.
The CAM manufacturing compo-nent was actually developed in ad-vance of the CAD technology.In the 1950’s, manufacturers first adopted tools controlled by a system of num-bers and letters to produce objects with complex shapes in both an accu-rate and repeatable manner (Numeri-cally Controlled or NC). Paper tapes
fed numerical data into machines that then positioned and directed tools to create the shape of the item in production.1 The world’s first CAM software program using a numeri-cal control programming tool named PRONTO, was developed in 1957 by Dr Patrick J. Hanratty, who is often re-ferred to as the father of CAD/CAM technology.2
It was not until the late 1960s that numerically controlled machines became commercially available. How-ever, the development began in 1962 as an outcome of a universal and en-hanced NC programming language known as Automatically Programmed Tools (APT) created at the Massachu-setts Institute of Technology. Surpris-
ingly, the introduction of Computer-Aided Design (CAD) had little impact on Computer Numerical Control (CNC) processes until the actual de-velopment of enhanced CAD applica-tions occurred. This resulted in a last-ing linkage between CAD and CAM1
software and machinery, and the technology expanded from that point forward.
Initial dental applications
In the early 1980s, CAD/CAM tech-
nology was used to produce clinical dental restorations when Andersson3 envisioned the use of titanium for the fabrication of crowns. Anders-son selected titanium because of the
established biocompatibility he had learned about from the pioneering work of Brånemark, who is recognized for the development and introduction of contemporary dental implants. Since casting titanium was not pos-sible at that time, dental restorations were fabricated by using another pro-cess. In 1982, Andersson developed the CAM portion of the fabrication process by using a combination of spark erosion and copy milling.3 In that same year, he cemented the first CAM fabricated titanium complete crown.3
Andersson quickly recognized that the potential commercialization of the process would be costly and the resulting fabrication processes would involve digitization, a realization which then led to the development of the CAD fabrication process. His pioneer-ing activities became commercially available as the Procera method of fabricating crowns in 1983. The Proc-era system was subsequently acquired by Nobelpharma (now Nobel Bio-care) in 1988. The patent that served as the basis for the 1982 production process did not limit fabrication to the use of a physical definitive die of the prepared tooth but included the potential use of a virtual tooth prepa-ration and definitive die derived from a computer. Andersson indicated that the first CAD/CAM Procera crown, derived from a computer file rather than a conventional gypsum die, was fabricated around 1990 (Personal communication, Matts Andersson PhD, e-mail November 2010).
Another important dental appli-cation of CAD/CAM technology also occurred in the 1980s. Mörmann4 de-veloped an interest in tooth-colored restorations. He wanted dentists to be able to produce durable inlay res-torations chairside by scanning cav-ity preparations intraorally and using the resulting CAD data to form a ce-ramic restoration that would fit the prepared tooth by using CAM tech-nology. Mörmann developed a proto-type CAD/CAM device in 1983, and a system became fully functional in
1985. In September of that same year, Mörmann placed the first chairside fabricated ceramic restoration with equipment introduced and marketed as the CEREC 1 system (Sirona Dental Systems LLC, Charlotte, NC).5 That first clinical restoration was an MOD feldspathic porcelain inlay fabricated for a maxillary left second molar.4
The design and milling of single crowns, partial fixed dental prostheses, and a variety of implant components and prostheses have since become relatively common clinical and labora-tory procedures. Despite these many advances, CAD/CAM technology has yet to be used for the fabrication of conventional complete dentures.
Transition to complete denture fabrication
Since 1995, the principal author has used a series of clinical procedures intended to facilitate the fabrication of conventional complete dentures and implant prostheses. These same procedures can also be adapted for the fabrication of complete dentures with CAD/CAM technology when it becomes commercially available.
The clinical technique is different from conventional complete denture methods in that it requires impres-sions that record the shape of both the intaglio and cameo surfaces of complete denture bases while also identifying muscular and phonetic lo-cations suitable for the placement of prosthetic teeth. In the future, it will be possible to scan the morphology recorded by using this technique and to transfer that digital data to a CAD software program where denture teeth can be virtually placed into appropri-ate positions. Then a dental labora-tory technician can export the denture base form and tooth arrangement morphology to a milling machine for the fabrication of the maxillary and mandibular complete dentures.
As an additional step beyond this clinical technique, a prototype CAD program, known as the 3D Tooth Arrangement Program, was devel-
oped by the principal author aided by computer programmers in 2009. This prototype software was created for the following 4 purposes: 1) to pilot test the software programming and obtain student and faculty input on its design and use; 2) to help stu-dents visualize the different types of occlusal schemes that can be created for complete dentures by being able to produce mandibular movements between different types of opposing 3-dimensional (3-D) denture teeth; 3) to teach students how to arrange teeth virtually before performing the actual laboratory procedure; and 4) to permit faculty to develop a library of acceptable and inappropriate tooth arrangements to assess student competency. This program was used for the first time by second year dental students at the Loma Linda University School of Dentistry in the fall of 2010 during the complete denture preclinical course. The educational applications and benefits of this program will be de-scribed in a subsequent publication.
The purpose of this article is to de-scribe the clinical procedures required to record the morphology of the inta-glio and cameo surfaces of complete denture bases as well as the muscular and phonetic locations suitable for the placement of prosthetic denture teeth.
CLINICAL TECHNIQUE
The following technique includes all the requisite steps required to pro-duce maxillary and mandibular de-finitive impressions of the edentulous arches in a manner that will permit the application of CAD/CAM technology.
The overall goal is to make de-finitive edentulous impressions that capture the edentulous ridges and borders (vestibules) while record-ing as much as possible of the func-tional soft tissue that will be in con-tact with the facial surfaces of the denture bases located occlusal to the denture borders. Additionally, the impressions should record muscu-lar and phonetic positions suitable for placing prosthetic denture teeth.

The Journal of Prosthetic Dentistry
35January 2012
Goodacre et alGoodacre et al
The clinical impression procedures described in this article provide a method of recording the morphology of the intaglio and cameo surfaces of complete denture bases and also identify muscular and phonetic locations for the prosthetic teeth. When the CAD/CAM technology for fabricating complete dentures becomes commercially available, it will be possible to scan the denture base morphology and tooth positions recorded with this technique and import those data into a virtual tooth arrangement program where teeth can be articulated and then export the data to a milling device for the fabrication of the complete dentures. A prototype 3-D tooth arrangement program is described in this article that serves as an example of the type of program than can be used to arrange prosthetic teeth virtually as part of the overall CAD/CAM fabrication of complete dentures. (J Prosthet Dent 2012;107:34-46)
CAD/CAM fabricated complete dentures: concepts and clinical methods of obtaining required morphological data
Charles J. Goodacre, DDS, MSD,a Antoanela Garbacea, DDS,b W. Patrick Naylor, DDS, MPH, MS,c Tony Daher, DDS, MSEd,d Christopher B. Marchack, DDS,e and Jean Lowry, PhDf
Loma Linda University School of Dentistry, Loma Linda, Calif; Loma Linda University School of Allied Health Professions, Loma Linda, Calif; University of Southern California School of Dentistry, Los Angeles, Calif
Presented at the Academy of Prosthodontics meeting, Hilton Head, NC, May 6, 2011.
aProfessor, Department of Restorative Dentistry, Loma Linda University School of Dentistry.bAdvanced Education Student, Implant Dentistry and Prosthodontics, Loma Linda University School of Dentistry. cAssociate Dean for Advanced Dental Education; Professor, Department of Restorative Dentistry, Loma Linda University School of Dentistry.dAssociate Professor, Department of Restorative Dentistry, Loma Linda University School of Dentistry.eAssociate Clinical Professor, Advanced Prosthodontics, University of Southern California School of Dentistry.fEmeritus Professor, Speech-Language Pathology, Loma Linda University School of Allied Health Professions.
The acronym CAD/CAM repre-sents Computer-Aided Design (CAD) and Computer-Aided Manufactur-ing (CAM). In some industries, an equivalent term, CAD/NC (Numerical Control) is used. With this design and manufacturing technology, CAD soft-ware defines the geometry of an ob-ject while CAM programming directs the fabrication process.
The CAM manufacturing compo-nent was actually developed in ad-vance of the CAD technology.In the 1950’s, manufacturers first adopted tools controlled by a system of num-bers and letters to produce objects with complex shapes in both an accu-rate and repeatable manner (Numeri-cally Controlled or NC). Paper tapes
fed numerical data into machines that then positioned and directed tools to create the shape of the item in production.1 The world’s first CAM software program using a numeri-cal control programming tool named PRONTO, was developed in 1957 by Dr Patrick J. Hanratty, who is often re-ferred to as the father of CAD/CAM technology.2
It was not until the late 1960s that numerically controlled machines became commercially available. How-ever, the development began in 1962 as an outcome of a universal and en-hanced NC programming language known as Automatically Programmed Tools (APT) created at the Massachu-setts Institute of Technology. Surpris-
ingly, the introduction of Computer-Aided Design (CAD) had little impact on Computer Numerical Control (CNC) processes until the actual de-velopment of enhanced CAD applica-tions occurred. This resulted in a last-ing linkage between CAD and CAM1
software and machinery, and the technology expanded from that point forward.
Initial dental applications
In the early 1980s, CAD/CAM tech-
nology was used to produce clinical dental restorations when Andersson3 envisioned the use of titanium for the fabrication of crowns. Anders-son selected titanium because of the
established biocompatibility he had learned about from the pioneering work of Brånemark, who is recognized for the development and introduction of contemporary dental implants. Since casting titanium was not pos-sible at that time, dental restorations were fabricated by using another pro-cess. In 1982, Andersson developed the CAM portion of the fabrication process by using a combination of spark erosion and copy milling.3 In that same year, he cemented the first CAM fabricated titanium complete crown.3
Andersson quickly recognized that the potential commercialization of the process would be costly and the resulting fabrication processes would involve digitization, a realization which then led to the development of the CAD fabrication process. His pioneer-ing activities became commercially available as the Procera method of fabricating crowns in 1983. The Proc-era system was subsequently acquired by Nobelpharma (now Nobel Bio-care) in 1988. The patent that served as the basis for the 1982 production process did not limit fabrication to the use of a physical definitive die of the prepared tooth but included the potential use of a virtual tooth prepa-ration and definitive die derived from a computer. Andersson indicated that the first CAD/CAM Procera crown, derived from a computer file rather than a conventional gypsum die, was fabricated around 1990 (Personal communication, Matts Andersson PhD, e-mail November 2010).
Another important dental appli-cation of CAD/CAM technology also occurred in the 1980s. Mörmann4 de-veloped an interest in tooth-colored restorations. He wanted dentists to be able to produce durable inlay res-torations chairside by scanning cav-ity preparations intraorally and using the resulting CAD data to form a ce-ramic restoration that would fit the prepared tooth by using CAM tech-nology. Mörmann developed a proto-type CAD/CAM device in 1983, and a system became fully functional in
1985. In September of that same year, Mörmann placed the first chairside fabricated ceramic restoration with equipment introduced and marketed as the CEREC 1 system (Sirona Dental Systems LLC, Charlotte, NC).5 That first clinical restoration was an MOD feldspathic porcelain inlay fabricated for a maxillary left second molar.4
The design and milling of single crowns, partial fixed dental prostheses, and a variety of implant components and prostheses have since become relatively common clinical and labora-tory procedures. Despite these many advances, CAD/CAM technology has yet to be used for the fabrication of conventional complete dentures.
Transition to complete denture fabrication
Since 1995, the principal author has used a series of clinical procedures intended to facilitate the fabrication of conventional complete dentures and implant prostheses. These same procedures can also be adapted for the fabrication of complete dentures with CAD/CAM technology when it becomes commercially available.
The clinical technique is different from conventional complete denture methods in that it requires impres-sions that record the shape of both the intaglio and cameo surfaces of complete denture bases while also identifying muscular and phonetic lo-cations suitable for the placement of prosthetic teeth. In the future, it will be possible to scan the morphology recorded by using this technique and to transfer that digital data to a CAD software program where denture teeth can be virtually placed into appropri-ate positions. Then a dental labora-tory technician can export the denture base form and tooth arrangement morphology to a milling machine for the fabrication of the maxillary and mandibular complete dentures.
As an additional step beyond this clinical technique, a prototype CAD program, known as the 3D Tooth Arrangement Program, was devel-
oped by the principal author aided by computer programmers in 2009. This prototype software was created for the following 4 purposes: 1) to pilot test the software programming and obtain student and faculty input on its design and use; 2) to help stu-dents visualize the different types of occlusal schemes that can be created for complete dentures by being able to produce mandibular movements between different types of opposing 3-dimensional (3-D) denture teeth; 3) to teach students how to arrange teeth virtually before performing the actual laboratory procedure; and 4) to permit faculty to develop a library of acceptable and inappropriate tooth arrangements to assess student competency. This program was used for the first time by second year dental students at the Loma Linda University School of Dentistry in the fall of 2010 during the complete denture preclinical course. The educational applications and benefits of this program will be de-scribed in a subsequent publication.
The purpose of this article is to de-scribe the clinical procedures required to record the morphology of the inta-glio and cameo surfaces of complete denture bases as well as the muscular and phonetic locations suitable for the placement of prosthetic denture teeth.
CLINICAL TECHNIQUE
The following technique includes all the requisite steps required to pro-duce maxillary and mandibular de-finitive impressions of the edentulous arches in a manner that will permit the application of CAD/CAM technology.
The overall goal is to make de-finitive edentulous impressions that capture the edentulous ridges and borders (vestibules) while record-ing as much as possible of the func-tional soft tissue that will be in con-tact with the facial surfaces of the denture bases located occlusal to the denture borders. Additionally, the impressions should record muscu-lar and phonetic positions suitable for placing prosthetic denture teeth.

36 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
37January 2012
Goodacre et alGoodacre et al
Impression trays
The edentulous impressions can be made by using either a custom tray (Fig. 1A) or a stock tray that can be molded to conform to the shape of each patient’s arch and provide the required border extensions.
Newly designed thermoplastic stock trays (Vident, Brea, Calif ) (Fig. 1B), specifically designed for edentu-lous patients, have been developed by Dr Stephen Wagner. They are ad-vantageous for this technique as the
trays can be adapted to the shape of the edentulous arch by softening each tray in an 80°C (180°F) water bath for 1 minute (no tempering needed) and then adapting it intraorally to fit the specific contours of each patient’s edentulous arch. In the softened state, the tray borders can be trimmed with scissors if the extensions need to be shortened. Likewise, the softened material can be stretched or added to when the tray needs to be extended to reach desired landmarks. After the tray has been customized to fit the
arch, only the borders are softened, and the patient’s musculature is ac-tivated to mold the softened borders (Fig. 1C).
Mandibular impression making
After the impression tray has been
selected (custom or stock tray), and conformed to the patient’s mouth, border molding is then performed. A medium-body vinyl polysiloxane impression material (Aquasil Mono-phase Smart Wetting Impression
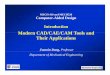
1 A, Custom acrylic resin mandibular impression tray. Tray handle is fabricated so it extends vertically from anterior ridge crest and then turns anteriorly to pass through lips with minimal interference with oral musculature. B, Maxil-lary and mandibular moldable stock trays. C, Maxillary tray was softened in hot water and intraorally molded to fit edentulous maxilla form. It was then border molded and coated with vinyl polysiloxane adhesive in preparation for definitive maxillary impression.
2 A, Mandibular vinyl polysiloxane impression made with moldable tray shown in Figure 1B. B, Scalpel used to remove impression material that flowed over ridge crest of tray. Exposed occlusal surface of tray coated with adhesive. C, Medium-body vinyl polysiloxane expressed onto occlusal surface of tray and extended occlusally to level of center of retromolar pads. D, Patient instructed to swallow 3 times while pressing lips together, thereby extruding impression material occlusally as result of muscular contraction. E, Dashed line shows depth of tongue depression used to trim impression material. F, Impression material trimmed at depth of lingual tongue depression, thereby locating neutral zone identified by flat area.
A
A
D
B
B
E
C
C
F
Material; Dentsply Intl Inc, Milford, Del) is recommended for this proce-dure because the completed impres-sion can be removed from the mouth and repositioned intraorally multiple times without adversely altering the polymerized material and the border extensions. A light-body impression material (Aquasil LV Smart Wetting Impression Material; Dentsply Intl Inc) is then used to complete the mandibular impression (Fig. 2A).
The mandibular posterior neutral zone impression technique
Once the border molding and de-finitive impression is completed, an accompanying neutral zone impres-sion6,7 is made on the occlusal surface of the tray by removing impression material that may have extended onto the tray’s occlusal surface and by coat-ing the tray with adhesive (Fig. 2B). It is critical to preserve the impression material closest to the impression tray borders because it has recorded the form of the corresponding contacting buccal mucosa.
Medium-body vinyl polysiloxane impression material (Aquasil Mono-phase Smart Wetting Impression Material, Dentsply Intl Inc) is then dispensed along the entire occlusal surface of the tray, from each ret-romolar pad area of the tray to the handle, at a vertical height sufficient to reach the level of the center of the retromolar pads bilaterally (Fig. 2C). The impression is promptly placed intraorally, and the patient asked to swallow 3 times in succession while pressing their lips together and press-
ing their tongue laterally against their lips and cheeks. These mouth and tongue movements activate the oral musculature, so the impression mate-rial is compressed between the lower lip, cheeks, and tongue muscles, thereby recording the location of the posterior neutral zone.
After completing these move-ments, the patient is instructed to re-lax the mandible and tongue. The im-pression can be removed in as short a time as 2 minutes, if needed, for pa-tient comfort. If the material has not completely polymerized, sufficient viscosity will have developed to es-tablish the desired form of the neutral zone. The repeated swallowing and resulting compression of the impres-sion material between the tongue and cheeks extrudes the impression mate-rial occlusally (Fig. 2D).
The lateral borders of the tongue usually create a depression in the lin-gual surface of the impression mate-rial. Differences in the form of the de-pressions are to be expected given the variations in pressure recorded by the tongue against the mandibular mo-lars. According to Fröhlich et al,8 the force ranges from 11.3 kPa to 49.6 kPa with a median pressure of 27.7 kPa. In another study by these same authors, a maximum pressure range of 2.8 kPa to 39.1 kPa was recorded by the tongue against the lingual aspect of the mandibular second premolar and first molar during swallowing.9
A scalpel is used to cut through the material in a faciolingual direction at the depth of the depression (Fig. 2E). Experience has shown that the deep-est aspect of the lingual depression
is typically located vertically around the center of the retromolar pads, a level that is useful in approximating the height of the mandibular occlusal plane.
After sectioning through the neu-tral zone impression, a flat occlusal platform is formed that represents the faciolingual location of the posterior neutral zone and provides a physi-ological guide for posterior tooth po-sitioning (Fig. 2F).
Mandibular anterior tooth positioning impressions
Sometimes the mandibular tray
handle interferes with the lingual mor-phology of the anterior aspect of the neutral zone impression. When this occurs, the tray handle should be re-moved along with any impression ma-terial that may be covering the occlu-sal aspect of the tray in the area where the mandibular anterior teeth will be located (Fig. 3A). Impression material adhesive is applied and medium-body impression material is dispensed over this exposed anterior region (Fig. 3B), the tray is placed intraorally, and the patient is instructed to swallow once and then pronounce the letters “Q” and “U” 3 times consecutively to mold the lingual area (Fig. 3C). After the patient completes these sounds, the lower lip is grasped and pulled facially so the impression can be re-moved without having the lip displace the impression material. Although the pressure of the resting lip against this area is light (mean of 0.9 kPa),10 it is still capable of displacing unpolymer-ized impression material.
3 A, Tray handle and lingual impression material removed. Adhesive applied. B, Impression material applied. C, Im-pression material molded by pronouncing letters “Q” and “U”.
A B C

36 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
37January 2012
Goodacre et alGoodacre et al
Impression trays
The edentulous impressions can be made by using either a custom tray (Fig. 1A) or a stock tray that can be molded to conform to the shape of each patient’s arch and provide the required border extensions.
Newly designed thermoplastic stock trays (Vident, Brea, Calif ) (Fig. 1B), specifically designed for edentu-lous patients, have been developed by Dr Stephen Wagner. They are ad-vantageous for this technique as the
trays can be adapted to the shape of the edentulous arch by softening each tray in an 80°C (180°F) water bath for 1 minute (no tempering needed) and then adapting it intraorally to fit the specific contours of each patient’s edentulous arch. In the softened state, the tray borders can be trimmed with scissors if the extensions need to be shortened. Likewise, the softened material can be stretched or added to when the tray needs to be extended to reach desired landmarks. After the tray has been customized to fit the
arch, only the borders are softened, and the patient’s musculature is ac-tivated to mold the softened borders (Fig. 1C).
Mandibular impression making
After the impression tray has been
selected (custom or stock tray), and conformed to the patient’s mouth, border molding is then performed. A medium-body vinyl polysiloxane impression material (Aquasil Mono-phase Smart Wetting Impression
1 A, Custom acrylic resin mandibular impression tray. Tray handle is fabricated so it extends vertically from anterior ridge crest and then turns anteriorly to pass through lips with minimal interference with oral musculature. B, Maxil-lary and mandibular moldable stock trays. C, Maxillary tray was softened in hot water and intraorally molded to fit edentulous maxilla form. It was then border molded and coated with vinyl polysiloxane adhesive in preparation for definitive maxillary impression.
2 A, Mandibular vinyl polysiloxane impression made with moldable tray shown in Figure 1B. B, Scalpel used to remove impression material that flowed over ridge crest of tray. Exposed occlusal surface of tray coated with adhesive. C, Medium-body vinyl polysiloxane expressed onto occlusal surface of tray and extended occlusally to level of center of retromolar pads. D, Patient instructed to swallow 3 times while pressing lips together, thereby extruding impression material occlusally as result of muscular contraction. E, Dashed line shows depth of tongue depression used to trim impression material. F, Impression material trimmed at depth of lingual tongue depression, thereby locating neutral zone identified by flat area.
A
A
D
B
B
E
C
C
F
Material; Dentsply Intl Inc, Milford, Del) is recommended for this proce-dure because the completed impres-sion can be removed from the mouth and repositioned intraorally multiple times without adversely altering the polymerized material and the border extensions. A light-body impression material (Aquasil LV Smart Wetting Impression Material; Dentsply Intl Inc) is then used to complete the mandibular impression (Fig. 2A).
The mandibular posterior neutral zone impression technique
Once the border molding and de-finitive impression is completed, an accompanying neutral zone impres-sion6,7 is made on the occlusal surface of the tray by removing impression material that may have extended onto the tray’s occlusal surface and by coat-ing the tray with adhesive (Fig. 2B). It is critical to preserve the impression material closest to the impression tray borders because it has recorded the form of the corresponding contacting buccal mucosa.
Medium-body vinyl polysiloxane impression material (Aquasil Mono-phase Smart Wetting Impression Material, Dentsply Intl Inc) is then dispensed along the entire occlusal surface of the tray, from each ret-romolar pad area of the tray to the handle, at a vertical height sufficient to reach the level of the center of the retromolar pads bilaterally (Fig. 2C). The impression is promptly placed intraorally, and the patient asked to swallow 3 times in succession while pressing their lips together and press-
ing their tongue laterally against their lips and cheeks. These mouth and tongue movements activate the oral musculature, so the impression mate-rial is compressed between the lower lip, cheeks, and tongue muscles, thereby recording the location of the posterior neutral zone.
After completing these move-ments, the patient is instructed to re-lax the mandible and tongue. The im-pression can be removed in as short a time as 2 minutes, if needed, for pa-tient comfort. If the material has not completely polymerized, sufficient viscosity will have developed to es-tablish the desired form of the neutral zone. The repeated swallowing and resulting compression of the impres-sion material between the tongue and cheeks extrudes the impression mate-rial occlusally (Fig. 2D).
The lateral borders of the tongue usually create a depression in the lin-gual surface of the impression mate-rial. Differences in the form of the de-pressions are to be expected given the variations in pressure recorded by the tongue against the mandibular mo-lars. According to Fröhlich et al,8 the force ranges from 11.3 kPa to 49.6 kPa with a median pressure of 27.7 kPa. In another study by these same authors, a maximum pressure range of 2.8 kPa to 39.1 kPa was recorded by the tongue against the lingual aspect of the mandibular second premolar and first molar during swallowing.9
A scalpel is used to cut through the material in a faciolingual direction at the depth of the depression (Fig. 2E). Experience has shown that the deep-est aspect of the lingual depression
is typically located vertically around the center of the retromolar pads, a level that is useful in approximating the height of the mandibular occlusal plane.
After sectioning through the neu-tral zone impression, a flat occlusal platform is formed that represents the faciolingual location of the posterior neutral zone and provides a physi-ological guide for posterior tooth po-sitioning (Fig. 2F).
Mandibular anterior tooth positioning impressions
Sometimes the mandibular tray
handle interferes with the lingual mor-phology of the anterior aspect of the neutral zone impression. When this occurs, the tray handle should be re-moved along with any impression ma-terial that may be covering the occlu-sal aspect of the tray in the area where the mandibular anterior teeth will be located (Fig. 3A). Impression material adhesive is applied and medium-body impression material is dispensed over this exposed anterior region (Fig. 3B), the tray is placed intraorally, and the patient is instructed to swallow once and then pronounce the letters “Q” and “U” 3 times consecutively to mold the lingual area (Fig. 3C). After the patient completes these sounds, the lower lip is grasped and pulled facially so the impression can be re-moved without having the lip displace the impression material. Although the pressure of the resting lip against this area is light (mean of 0.9 kPa),10 it is still capable of displacing unpolymer-ized impression material.
3 A, Tray handle and lingual impression material removed. Adhesive applied. B, Impression material applied. C, Im-pression material molded by pronouncing letters “Q” and “U”.
A B C

38 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
39January 2012
Goodacre et alGoodacre et al
It is also possible to form the an-terior-facial aspect of the impression tray by trimming away the facial im-pression material without disturbing the lingual form and applying adhe-sive (Fig. 4A). After dispensing medi-um-body impression material and re-seating the tray, the patient is asked to pronounce the letters, “Q” and “U”, 3 times in succession and then say the word, “Christmas,” 3 times. As soon as the patient finishes pronouncing the word “Christmas,” the lower lip is pulled anteriorly away from the impression material and the tray re-moved so the anterior material can polymerize without being displaced by the lower lip. Once polymerization is complete, the material is trimmed so that it is level with the posterior neutral zone areas (Fig. 4B).
Production of the sounds required to form the letters, “Q” and “U”, and saying the word, “Christmas,” acti-vates the muscles of the chin as well as those muscles associated with the mentolabial angle. These facial move-ments, in turn, create the form of the mandibular anterior denture base.
Maxillary impression making
As with the mandible, maxillary
edentulous impressions can be made with either a custom or stock impres-sion tray. The posterior extension of the tray is determined by the location of the vibrating line that delineates the transition between the immov-able hard palate tissue and the mov-able tissue of the soft palate. This line is located by having the patient
say “Ahh”11 and marking the junc-tion between movable and station-ary soft tissue with an indelible pencil or marker (Dr. Thompson’s Sanitary Color Transfer Applicators; Great Plains Dental Products Co Inc, King-man, Kans). Trim or stretch the tray so its posterior border coincides with the location and form of this vibrating line. The depth to which the soft tis-sue anterior to the vibrating line can be displaced determines the depth of the posterior palatal seal.
The palatal thickness of the max-illary impression tray should be suffi-cient to provide tray rigidity but not be excessive. A thickness of 2 mm is preferable. This dimension is critical so the tray’s thickness does not inter-fere with the development of palatal contours since the patient’s speech will be used to produce tongue move-ments which then shape medium-body vinyl polysiloxane impression material that will be applied on the cameo surface of the palatal portion of the tray.
Next, the maxillary impression is made so as to accurately record the edentulous ridge morphology and the border extensions. On the facial surface of the tray, the light-body im-pression material should be extended as far as possible occlusally beyond the borders (flanges) by muscular and manipulative movements made dur-ing the border molding. It is through this process that the tissue contact-ing facial surfaces of the denture are formed (Fig. 5). If there are areas on the facial surface of the tray where the cameo surface morphology has not
been completely recorded, more tray adhesive should be applied to the af-fected area(s), followed by a thin lay-er of additional light-body impression material.
Speech analysis in prosthodontics
The clinical assessment of speech
has been used effectively in prosth-odontics for many decades. In fact, a number of articulation tests have been recommended for evaluating the quality of a patient’s speech and pho-netics. In 1959, Morrison12 published a 1 stanza test he recommended as a means to establish the occlusal verti-cal dimension as well as the retruded contact position. Guichet13 proposed reading prose familiar to the dentist as a means of evaluating anterior tooth positions. In 1973, Chierici and Lawson,14 published several test sen-tences designed for evaluating articu-latory factors involved in consonant sound production. A speech articu-lation test consisting of 12 sentences was proposed by Kestenberg15 in 1983 and Howell16 published the results of a 1986 study in which subjects read aloud a passage of text known as “The Rainbow Passage.”
Silverman17-19 is credited with de-vising a method to evaluate phonet-ics that he referred to as the “closest speaking space,” and his technique continues to be used today. The let-ter “S” produces the most frequently used sibilant (hissing) sound that oc-curs during speaking and reading.19 In fact, asking patients to make the “S” sound has been used clinically to
4 A, Facial impression material removed. B, Facial impression material ap-pearance after molding by pronouncing letters “Q” and “U” and saying word “Christmas”.
5 Maxillary impression made with border molded tray shown in Figure 1C.
A B
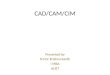
6 A, Clinical image showing contact area between tongue, teeth, and palate when /s/ and /z/ sounds are pro-nounced in stimulus sentences found at top of picture. B, Image showing contact area when /sh/ and zh/ sounds are pronounced. C, Image showing contact area when /l/ sound is pronounced. D, Image showing contact area when /t and d sounds are pronounced. E, Image showing contact area when /ch/ and /j/ sounds are pronounced. F, Image showing contact area when /n sound is pronounced. G, Image showing contact area when r sound is pronounced.H, Image showing contact area when the y as in “yellow” sound is pronounced. I, Image showing posterior area of contact between tongue, teeth, and hard/soft palate when /k/, /g/, and /ng/ sounds are pronounced.
A
“s” & “z”
Tongue contacts the palatal mucosa and
teeth except for a nar-row central area of the
anterior palate
Sue is missing one piece. (s sound)Zelma is busy. (z sound)
Chuck is watching Butch. (ch sound)Jane enjoyed the fudge. (j sound) Ned won many prizes. (n sound)
Tom wanted a bite. (t sound)Did Eddy lead. (d sound)
Ralph arrived after everyone else. (r sound)
King Gregory was gagging.(k, g , and ng sounds)
Young men like yellow kayaks.(y as in yellow)
She is washing the dish. (sh sound)Measure the garage. (zh sound) Lee will allow it. (l sound)
“t” & “d”
Tongue contacts the palate and
teeth all around the arch followed
by anterior release with sus-tained posterior
contact
Contact folled by release
Contact folled by release
Contact folled by release
Stabilization Stabilization
“r”
Tongue contacts the posterior palatal
mucosa and teeth but does not contact the
anterior palate
“y”
Tongue contacts the palate and posterior teeth but does not contact the central area of the anterior
palate
“y”, “g”, “ng”
Tongue contacts the poste-rior hard palate, soft palate, and most posterior teeth fol-lowed by release in the center
of the soft palate
“ch” & “j”
Tongue contacts the palate and
teeth all around the arch followed by anterior release
with sustained posterior contact
“n”
Tongue main-tains continuous contact with the
palate and teeth all around the arch
D
G
B
E
H
C
F
I
“sh” & “zh”
Tongue contacts the palate and posterior
teeth but does not con-tact the central area of
the anterior palate
“l”
Tongue tip contacts anterior palate
Stab
iliza
tion
Stab
iliza
tionStabilization
Stabilization

38 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
39January 2012
Goodacre et alGoodacre et al
It is also possible to form the an-terior-facial aspect of the impression tray by trimming away the facial im-pression material without disturbing the lingual form and applying adhe-sive (Fig. 4A). After dispensing medi-um-body impression material and re-seating the tray, the patient is asked to pronounce the letters, “Q” and “U”, 3 times in succession and then say the word, “Christmas,” 3 times. As soon as the patient finishes pronouncing the word “Christmas,” the lower lip is pulled anteriorly away from the impression material and the tray re-moved so the anterior material can polymerize without being displaced by the lower lip. Once polymerization is complete, the material is trimmed so that it is level with the posterior neutral zone areas (Fig. 4B).
Production of the sounds required to form the letters, “Q” and “U”, and saying the word, “Christmas,” acti-vates the muscles of the chin as well as those muscles associated with the mentolabial angle. These facial move-ments, in turn, create the form of the mandibular anterior denture base.
Maxillary impression making
As with the mandible, maxillary
edentulous impressions can be made with either a custom or stock impres-sion tray. The posterior extension of the tray is determined by the location of the vibrating line that delineates the transition between the immov-able hard palate tissue and the mov-able tissue of the soft palate. This line is located by having the patient
say “Ahh”11 and marking the junc-tion between movable and station-ary soft tissue with an indelible pencil or marker (Dr. Thompson’s Sanitary Color Transfer Applicators; Great Plains Dental Products Co Inc, King-man, Kans). Trim or stretch the tray so its posterior border coincides with the location and form of this vibrating line. The depth to which the soft tis-sue anterior to the vibrating line can be displaced determines the depth of the posterior palatal seal.
The palatal thickness of the max-illary impression tray should be suffi-cient to provide tray rigidity but not be excessive. A thickness of 2 mm is preferable. This dimension is critical so the tray’s thickness does not inter-fere with the development of palatal contours since the patient’s speech will be used to produce tongue move-ments which then shape medium-body vinyl polysiloxane impression material that will be applied on the cameo surface of the palatal portion of the tray.
Next, the maxillary impression is made so as to accurately record the edentulous ridge morphology and the border extensions. On the facial surface of the tray, the light-body im-pression material should be extended as far as possible occlusally beyond the borders (flanges) by muscular and manipulative movements made dur-ing the border molding. It is through this process that the tissue contact-ing facial surfaces of the denture are formed (Fig. 5). If there are areas on the facial surface of the tray where the cameo surface morphology has not
been completely recorded, more tray adhesive should be applied to the af-fected area(s), followed by a thin lay-er of additional light-body impression material.
Speech analysis in prosthodontics
The clinical assessment of speech
has been used effectively in prosth-odontics for many decades. In fact, a number of articulation tests have been recommended for evaluating the quality of a patient’s speech and pho-netics. In 1959, Morrison12 published a 1 stanza test he recommended as a means to establish the occlusal verti-cal dimension as well as the retruded contact position. Guichet13 proposed reading prose familiar to the dentist as a means of evaluating anterior tooth positions. In 1973, Chierici and Lawson,14 published several test sen-tences designed for evaluating articu-latory factors involved in consonant sound production. A speech articu-lation test consisting of 12 sentences was proposed by Kestenberg15 in 1983 and Howell16 published the results of a 1986 study in which subjects read aloud a passage of text known as “The Rainbow Passage.”
Silverman17-19 is credited with de-vising a method to evaluate phonet-ics that he referred to as the “closest speaking space,” and his technique continues to be used today. The let-ter “S” produces the most frequently used sibilant (hissing) sound that oc-curs during speaking and reading.19 In fact, asking patients to make the “S” sound has been used clinically to
4 A, Facial impression material removed. B, Facial impression material ap-pearance after molding by pronouncing letters “Q” and “U” and saying word “Christmas”.
5 Maxillary impression made with border molded tray shown in Figure 1C.
A B
6 A, Clinical image showing contact area between tongue, teeth, and palate when /s/ and /z/ sounds are pro-nounced in stimulus sentences found at top of picture. B, Image showing contact area when /sh/ and zh/ sounds are pronounced. C, Image showing contact area when /l/ sound is pronounced. D, Image showing contact area when /t and d sounds are pronounced. E, Image showing contact area when /ch/ and /j/ sounds are pronounced. F, Image showing contact area when /n sound is pronounced. G, Image showing contact area when r sound is pronounced.H, Image showing contact area when the y as in “yellow” sound is pronounced. I, Image showing posterior area of contact between tongue, teeth, and hard/soft palate when /k/, /g/, and /ng/ sounds are pronounced.
A
“s” & “z”
Tongue contacts the palatal mucosa and
teeth except for a nar-row central area of the
anterior palate
Sue is missing one piece. (s sound)Zelma is busy. (z sound)
Chuck is watching Butch. (ch sound)Jane enjoyed the fudge. (j sound) Ned won many prizes. (n sound)
Tom wanted a bite. (t sound)Did Eddy lead. (d sound)
Ralph arrived after everyone else. (r sound)
King Gregory was gagging.(k, g , and ng sounds)
Young men like yellow kayaks.(y as in yellow)
She is washing the dish. (sh sound)Measure the garage. (zh sound) Lee will allow it. (l sound)
“t” & “d”
Tongue contacts the palate and
teeth all around the arch followed
by anterior release with sus-tained posterior
contact
Contact folled by release
Contact folled by release
Contact folled by release
Stabilization Stabilization
“r”
Tongue contacts the posterior palatal
mucosa and teeth but does not contact the
anterior palate
“y”
Tongue contacts the palate and posterior teeth but does not contact the central area of the anterior
palate
“y”, “g”, “ng”
Tongue contacts the poste-rior hard palate, soft palate, and most posterior teeth fol-lowed by release in the center
of the soft palate
“ch” & “j”
Tongue contacts the palate and
teeth all around the arch followed by anterior release
with sustained posterior contact
“n”
Tongue main-tains continuous contact with the
palate and teeth all around the arch
D
G
B
E
H
C
F
I
“sh” & “zh”
Tongue contacts the palate and posterior
teeth but does not con-tact the central area of
the anterior palate
“l”
Tongue tip contacts anterior palate
Stab
iliza
tion
Stab
iliza
tionStabilization
Stabilization

40 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
41January 2012
Goodacre et al Goodacre et al
identify the closest approximation of the maxillary and mandibular central incisors, thereby providing clinical in-formation regarding the intercuspal position.20,21 Additionally, there have been several studies that record the average distance between the closest speaking space and the intercuspal position.16,17, 22-26
Use of the tongue during speech to record palatal morphology
The tongue has the capacity to
change its position more than any other organ, varying its shape and size interminably.22 In speech, the tongue is the principal articulator of conso-nants by contacting specific regions of the hard palate, alveolar ridge, and teeth during speech. The tongue also changes position and shape to pro-nounce each vowel.27 As such, the tongue is an important component of the speech system because it must el-evate, narrow, thin, protrude, retract, produce a groove, and lie flat in the mouth to create different sounds.28
Thus when recording the contours of the palate, it is vital to capture the movements of the tongue during speech because the resulting tongue pressure exerted on the palate can be used advantageously to produce pala-tograms. A palatogram is defined as a graphic representation of the area of contact between the tongue and pal-ate during speech.29 It has also been described as a “map of the palate in-dicating all areas of tongue contact while producing different sounds used in normal speech.”30
As a result, palatograms are used to evaluate the nature of the tongue-palate contact that occurs during speech.31-43 Oakley-Coles is credited with developing the technique31 by painting his tongue with a mixture of gum and flour and then examining his tongue after speech to determine where it had contacted the palate.32
Maxillary complete denture pala-tograms have been made with several different materials: 1) applying talcum powder to the dry palatal surface of a
maxillary complete denture and observ-ing where it was removed by the tongue as a result of speech33-36; 2) applying cornstarch to the palate of a denture and then observing where it was re-moved by the tongue30, 37; 3) spraying green aerosol marking medium onto the denture palate and observing the areas that became moistened and thereby darkened by tongue con-tact39; 4) applying utility wax to the palate and having the patient speak and thereby mold the soft wax37; 5) applying impression wax to the palate of the denture and observing areas that became shiny and smooth when contacted by the tongue as opposed to other areas where the wax was dull from lack of tongue contact38; and 6) applying a thin mix of irreversible hy-drocolloid to the palate of a denture and using speech to create a custom-ized palatal form.39 While individual variations exist in the precise areas of tongue-palate contact, maps have been created that are representative of typical patterns of contact be-tween the tongue, palate, and maxil-lary teeth.33,35,36,39-41 Palatograms have also been recorded with electronic de-vices42 and electropalatography (EPG) has been used for 30 years in phonetic and clinical research associated with speech therapy.43 EPG devices typi-
cally are custom acrylic resin palates with sensors located in the thin pala-tal acrylic resin.43
When making palatograms, it is important to note that the degree of tongue pressure44 and the area of contact between the tongue and pal-ate vary considerably depending on the sounds being produced. There-fore, it is important to use a wide range of sounds known to produce tongue-palate contact. The lingual-alveolar consonants are examples of key sounds that can be used to record palatal morphology. Additionally, be-cause it has been proposed that single word tests are not reliable24 when as-sessing phonetics, sentences should be read aloud by the patient covering the range of sibilants (/s/, /z/, /sh/, /zh/, /ch/, and /j/) and other sounds that produce contact between the tongue and palate.
The use of stimulus sentences
In 1973, Tanaka45 published 10
stimulus sentences recommended for use in evaluating the morphology of the palate in complete denture wear-ers. The sentences placed the conso-nants /s/, /z/, /sh/, /zh, /l/, /t/, /d/, /ch/, /j/, and /n/ in 3 different loca-tions: at the beginning, in the middle,
Table I. Thirteen sentences that stimulate tongue-palatal contact
1. Sue is missing one piece (s sound)
2. Zelma is busy (z sound)
3. She is washing the dish (sh sound)
4. Measure the garage (zh sound)
5. Lee will allow it (l sound)
6. Tom wanted a bite (t sound)
7. Did Eddie lead (d sound)
8. Chuck is watching Butch (ch sound)
9. Jane enjoyed the fudge (j sound)
10. Ned won many prizes (n sound)
11. Ralph arrived after everyone else (r sound)
12. Young men like yellow kayaks (y sound)
13. King Gregory is gagging (k, g, and ng sounds)
Clodronate
Etidronate
Tiludronate
Risedronate
Pamidronate
Ibandronate
Alendronate
Zolendronic Acid
Zoledronic Acid
and at the end of sentences. These sounds are formed as the result of contact between the tongue and vari-ous parts of the teeth, alveolar ridge, posterior aspect of the hard palate, and anterior portion of the soft pal-ate (Figs. 6A-F). They also can be
used to establish the proper palatal morphology and tooth positioning for a complete denture.
There are 3 additional sounds pro-duced from tongue-palate contact that the authors recommend adding to the original 10 used by Tanaka, thereby resulting in a list of 13 sen-tences (Table I). The 3 new stimulus sentences added to Tanaka’s original list require production of the fol-lowing sounds: /r/; /y/, and the /k/, /g/, and /ng/sounds (Figs. 6 G to I). The /k/, /g/, and /ng/sounds are key sounds for the most posterior area of the palate46 since the posterior as-pect of the tongue elevates to create a seal across the soft palate, posterior alveolar ridges, and the second/third molars.
Clinical technique for establishing palatal morphology
The morphology of the palate is recorded by placing medium-body vi-nyl polysiloxane impression material onto the cameo surface of the pal-ate, replacing the impression intra-orally, and instructing the patient to read the 13 stimulus sentences aloud (Table I). It is advisable to rehearse this step with the impression in the patient’s mouth but before inject-ing the impression material onto the tray. Rather than attempt to capture the entire palate in 1 seating, a 2-step process is recommended.
First, the posterior aspect of the tray is thinned, and then a 3 mm thickness of medium-body vinyl poly-siloxane impression material is placed in the area of the second molars bilat-erally and across the posterior border of the tray (Fig. 7A). The posterior as-pect of the palate is developed first in the area of the second molars at the same time as the posterior extension to the soft palate is formed by plac-ing medium body impression material onto that area of the tray. The patient is instructed to read the following sentence 3 times: “King Gregory is gagging.” Pronunciation of the words in this sentence causes the tongue to
phonetically shape the impression material (Fig. 7B), thereby defining the second molar region along with the posterior palatal extension.
Secondly, to capture the remain-ing form of the palatal slope, a 3-mm thick layer of medium-body impres-sion material is dispensed onto the remainder of the palate (Fig. 7C). The patient is immediately instructed to read the first 12 stimulus sentences in order (Table I). The first 12 sentences are read aloud and then repeated in that same order to complete the form of the lingual palatal slope (Fig. 7D).
There are no speech sounds that establish the contours of the central portion of the palate. This portion of the denture base is formed by pro-ducing a smooth transition between the previously developed palatal mor-phology on 1 side of the arch with the corresponding palatal contour on the opposite side of the arch and devel-oping the appropriate thickness in the central area of the palate on the digi-tized impressions.
As an alternative to the reading of 13 stimulus sentences, 2 sentences have been developed by the authors that include all of the consonants capable of producing tongue-palate contact. Use of these alternative sen-tences involves expressing the appro-priate 3 mm thickness of heavy-body vinyl polysiloxane impression material over the entire palatal aspect of the impression tray and then reseating the impression and asking the patient to read the following 2 sentences: “What is your slow toe doing in the yellow liquid on the shelf? Is it trying to judge or measure the temperature, change its color, or just reach out and touch something grand and glorious.” The reading should be repeated twice.
Clinical technique for determining maxillary anterior tooth positions
The faciolingual and incisocervi-
cal locations of the maxillary anterior prosthetic teeth have traditionally been determined by using tooth vis-ibility and lip support. Phonetics and
7 A, Medium-body polyvinyl si-loxane impression material applied posteriorly so tongue can mold mate-rial during speech. B, Impression material molded by patient reading stimulus sentence “King Gregory is gagging.” C, Impression material applied to anterior aspect of tray. D, Impression material molded by patient reading first 12 stimulus sentences.
A
B
C
D

40 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
41January 2012
Goodacre et al Goodacre et al
identify the closest approximation of the maxillary and mandibular central incisors, thereby providing clinical in-formation regarding the intercuspal position.20,21 Additionally, there have been several studies that record the average distance between the closest speaking space and the intercuspal position.16,17, 22-26
Use of the tongue during speech to record palatal morphology
The tongue has the capacity to
change its position more than any other organ, varying its shape and size interminably.22 In speech, the tongue is the principal articulator of conso-nants by contacting specific regions of the hard palate, alveolar ridge, and teeth during speech. The tongue also changes position and shape to pro-nounce each vowel.27 As such, the tongue is an important component of the speech system because it must el-evate, narrow, thin, protrude, retract, produce a groove, and lie flat in the mouth to create different sounds.28
Thus when recording the contours of the palate, it is vital to capture the movements of the tongue during speech because the resulting tongue pressure exerted on the palate can be used advantageously to produce pala-tograms. A palatogram is defined as a graphic representation of the area of contact between the tongue and pal-ate during speech.29 It has also been described as a “map of the palate in-dicating all areas of tongue contact while producing different sounds used in normal speech.”30
As a result, palatograms are used to evaluate the nature of the tongue-palate contact that occurs during speech.31-43 Oakley-Coles is credited with developing the technique31 by painting his tongue with a mixture of gum and flour and then examining his tongue after speech to determine where it had contacted the palate.32
Maxillary complete denture pala-tograms have been made with several different materials: 1) applying talcum powder to the dry palatal surface of a
maxillary complete denture and observ-ing where it was removed by the tongue as a result of speech33-36; 2) applying cornstarch to the palate of a denture and then observing where it was re-moved by the tongue30, 37; 3) spraying green aerosol marking medium onto the denture palate and observing the areas that became moistened and thereby darkened by tongue con-tact39; 4) applying utility wax to the palate and having the patient speak and thereby mold the soft wax37; 5) applying impression wax to the palate of the denture and observing areas that became shiny and smooth when contacted by the tongue as opposed to other areas where the wax was dull from lack of tongue contact38; and 6) applying a thin mix of irreversible hy-drocolloid to the palate of a denture and using speech to create a custom-ized palatal form.39 While individual variations exist in the precise areas of tongue-palate contact, maps have been created that are representative of typical patterns of contact be-tween the tongue, palate, and maxil-lary teeth.33,35,36,39-41 Palatograms have also been recorded with electronic de-vices42 and electropalatography (EPG) has been used for 30 years in phonetic and clinical research associated with speech therapy.43 EPG devices typi-
cally are custom acrylic resin palates with sensors located in the thin pala-tal acrylic resin.43
When making palatograms, it is important to note that the degree of tongue pressure44 and the area of contact between the tongue and pal-ate vary considerably depending on the sounds being produced. There-fore, it is important to use a wide range of sounds known to produce tongue-palate contact. The lingual-alveolar consonants are examples of key sounds that can be used to record palatal morphology. Additionally, be-cause it has been proposed that single word tests are not reliable24 when as-sessing phonetics, sentences should be read aloud by the patient covering the range of sibilants (/s/, /z/, /sh/, /zh/, /ch/, and /j/) and other sounds that produce contact between the tongue and palate.
The use of stimulus sentences
In 1973, Tanaka45 published 10
stimulus sentences recommended for use in evaluating the morphology of the palate in complete denture wear-ers. The sentences placed the conso-nants /s/, /z/, /sh/, /zh, /l/, /t/, /d/, /ch/, /j/, and /n/ in 3 different loca-tions: at the beginning, in the middle,
Table I. Thirteen sentences that stimulate tongue-palatal contact
1. Sue is missing one piece (s sound)
2. Zelma is busy (z sound)
3. She is washing the dish (sh sound)
4. Measure the garage (zh sound)
5. Lee will allow it (l sound)
6. Tom wanted a bite (t sound)
7. Did Eddie lead (d sound)
8. Chuck is watching Butch (ch sound)
9. Jane enjoyed the fudge (j sound)
10. Ned won many prizes (n sound)
11. Ralph arrived after everyone else (r sound)
12. Young men like yellow kayaks (y sound)
13. King Gregory is gagging (k, g, and ng sounds)
Clodronate
Etidronate
Tiludronate
Risedronate
Pamidronate
Ibandronate
Alendronate
Zolendronic Acid
Zoledronic Acid
and at the end of sentences. These sounds are formed as the result of contact between the tongue and vari-ous parts of the teeth, alveolar ridge, posterior aspect of the hard palate, and anterior portion of the soft pal-ate (Figs. 6A-F). They also can be
used to establish the proper palatal morphology and tooth positioning for a complete denture.
There are 3 additional sounds pro-duced from tongue-palate contact that the authors recommend adding to the original 10 used by Tanaka, thereby resulting in a list of 13 sen-tences (Table I). The 3 new stimulus sentences added to Tanaka’s original list require production of the fol-lowing sounds: /r/; /y/, and the /k/, /g/, and /ng/sounds (Figs. 6 G to I). The /k/, /g/, and /ng/sounds are key sounds for the most posterior area of the palate46 since the posterior as-pect of the tongue elevates to create a seal across the soft palate, posterior alveolar ridges, and the second/third molars.
Clinical technique for establishing palatal morphology
The morphology of the palate is recorded by placing medium-body vi-nyl polysiloxane impression material onto the cameo surface of the pal-ate, replacing the impression intra-orally, and instructing the patient to read the 13 stimulus sentences aloud (Table I). It is advisable to rehearse this step with the impression in the patient’s mouth but before inject-ing the impression material onto the tray. Rather than attempt to capture the entire palate in 1 seating, a 2-step process is recommended.
First, the posterior aspect of the tray is thinned, and then a 3 mm thickness of medium-body vinyl poly-siloxane impression material is placed in the area of the second molars bilat-erally and across the posterior border of the tray (Fig. 7A). The posterior as-pect of the palate is developed first in the area of the second molars at the same time as the posterior extension to the soft palate is formed by plac-ing medium body impression material onto that area of the tray. The patient is instructed to read the following sentence 3 times: “King Gregory is gagging.” Pronunciation of the words in this sentence causes the tongue to
phonetically shape the impression material (Fig. 7B), thereby defining the second molar region along with the posterior palatal extension.
Secondly, to capture the remain-ing form of the palatal slope, a 3-mm thick layer of medium-body impres-sion material is dispensed onto the remainder of the palate (Fig. 7C). The patient is immediately instructed to read the first 12 stimulus sentences in order (Table I). The first 12 sentences are read aloud and then repeated in that same order to complete the form of the lingual palatal slope (Fig. 7D).
There are no speech sounds that establish the contours of the central portion of the palate. This portion of the denture base is formed by pro-ducing a smooth transition between the previously developed palatal mor-phology on 1 side of the arch with the corresponding palatal contour on the opposite side of the arch and devel-oping the appropriate thickness in the central area of the palate on the digi-tized impressions.
As an alternative to the reading of 13 stimulus sentences, 2 sentences have been developed by the authors that include all of the consonants capable of producing tongue-palate contact. Use of these alternative sen-tences involves expressing the appro-priate 3 mm thickness of heavy-body vinyl polysiloxane impression material over the entire palatal aspect of the impression tray and then reseating the impression and asking the patient to read the following 2 sentences: “What is your slow toe doing in the yellow liquid on the shelf? Is it trying to judge or measure the temperature, change its color, or just reach out and touch something grand and glorious.” The reading should be repeated twice.
Clinical technique for determining maxillary anterior tooth positions
The faciolingual and incisocervi-
cal locations of the maxillary anterior prosthetic teeth have traditionally been determined by using tooth vis-ibility and lip support. Phonetics and
7 A, Medium-body polyvinyl si-loxane impression material applied posteriorly so tongue can mold mate-rial during speech. B, Impression material molded by patient reading stimulus sentence “King Gregory is gagging.” C, Impression material applied to anterior aspect of tray. D, Impression material molded by patient reading first 12 stimulus sentences.
A
B
C
D

42 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
43January 2012
Goodacre et al Goodacre et al
the lip position at rest also can be used to help identify the area where denture teeth can be appropriately located. To determine anterior tooth positions with these guides, the tray handle is removed along with the
impression material located over the occlusal aspect of the tray where the anterior teeth will be positioned. Af-ter applying tray adhesive, medium-body vinyl polysiloxane impression material is placed over the anterior
ridge crest area (Fig. 8A), and the pa-tient is instructed to pronounce the word “thank” followed by pronuncia-tion of the letter “V”. This combina-tion is pronounced 3 times and then the word “thank” is repeated an ad-
8 A, Maxillary tray handle removed along with polymerized impression material. Medium-body vinyl polysiloxane impression material placed into anterior-lingual area. B, Patient pronounced word “thank” and letter “V” to mold ma-terial. C, Polymerized impression material removed anteriorly, medium-body material deposited into area, and patient pronounced letters “Q” and “U” to mold anterior-facial aspect of impression.
9 A, Maxillary and mandibular impressions trimmed so posterior areas do not interfere with each other when patient closes at selected occlusal vertical dimension. B, Midline marked on maxillary impression and buccal corridor evalu-ated. C, Putty indices made over lubricated anterior aspect of maxillary impression. D, Anterior impression material trimmed away and hot wax spatula used to remove tray material, making room for anterior teeth. E, Maxillary anterior teeth arranged. F, Clinical evaluation of maxillary anterior teeth. G, Interocclusal record material placed over lubri-cated impressions with patient occluding at appropriate occlusal vertical dimension. H, Impressions and interocclusal record removed from mouth and record trimmed so intercuspation can be verified.
A B C
A
D
B
E
H
C
F
G
ditional 3 times. When pronouncing the word “thank”, the tongue molds the lingual aspect of the impression material and helps to locate the ap-proximate faciolingual position of the lingual surfaces of the anterior teeth (Fig. 8B). Pronouncing the letter, “V”, helps to identify the incisal length of the impression material and thereby establishes the approximate location of the incisal edge of the maxillary central incisors. After the pronuncia-tion exercise is completed, the patient is instructed to relax their tongue and lips for several seconds. Then the up-per lip is grasped gently and pulled facially so the entire maxillary impres-sion can be removed without disturb-ing any unpolymerized impression material.
Following polymerization of the impression material, the facial half of the anterior impression material is removed to expose the tray, the area coated with adhesive, and the impres-sion material deposited into the recess. The patient is instructed to pronounce the letters “Q” and “U” 3 times and then relax their tongue and lips for sev-eral seconds so the upper lip can rest against the impression material and establish an approximate anteroposte-rior position for the maxillary anterior teeth. The upper lip is then grasped and pulled facially so the impression can be removed without disturbing the incompletely polymerized impres-sion material (Fig 8C).
Resting the upper lip against the unpolymerized impression material is permissible since measurements of the resting pressure of the lip against the maxillary incisors are low. Conse-
quently, this level of pressure is unlikely to produce any substantive displace-ment of the impression material. In fact, in 1 study a slightly negative pres-sure was recorded at rest.47 A second study reported there was no labial pressure against the maxillary incisors in 11 out of 30 subjects and the mean pressure was low.48 When the same author compared adults with differ-ent occlusal relationships, the pres-sure was slightly more positive (mean of 0.08 kPa) for the normal horizon-tal overlap group; 0.14 kPa for the in-creased horizontal overlap group and 0.14 kPa for the reduced horizontal overlap group.49 Another study found the upper lip pressure at rest to be 0.2 kPa with a range from -0.7 to 1.4 kPa; the upper lip pressure was negative in 21 of the 84 children studied.50
A technique has been used where-by patients bring their lips together into light contact and air is blown between the teeth so the upper lip is pushed anteriorly by the air. The up-per lip is allowed to relax and assume its normal resting pressure.47 With this particular technique, a slightly negative pressure was found to be ex-erted on the maxillary incisors.47
Occlusal vertical dimension, tooth positioning, and interocclusal records
The occlusal vertical dimension is
established by using any one of sev-eral appropriate methods and marks placed on the skin for future refer-ence. The maxillary and mandibu-lar impressions are used as record bases to establish the occlusal verti-cal dimension and make interocclu-
sal records. The impressions are both seated simultaneously to evaluate the amount of impression material and tray material that typically has to be removed posteriorly because it inter-feres with proper mandibular closure at the established occlusal vertical di-mension. Following complete closure without interference between the 2 impressions, a scalpel is used to cre-ate notches in the impression materi-al and exposed tray material if present (Fig. 9A). The maxillary impression is placed intraorally so the midline can be marked on the impression with a permanent marker and the buccal corridor space can be assessed (Fig. 9B). The maxillary impression is then ready to have the 6 maxillary anterior prosthetic teeth selected at the initial diagnostic appointment arranged into the area now occupied by impression material. By using the impressions as record bases-wax rims, the previously selected maxillary anterior teeth are ar-ranged in the impression and the tooth size, form, and color verified. As with traditional complete denture tech-niques, different teeth can be selected, should a change need to be made.
Facial and lingual putty indices of the form of the maxillary anterior phonetic impression can be made for use as guides in arranging the anterior teeth (Fig. 9C). To arrange the maxil-lary anterior teeth, impression materi-al is removed along with the required amount of tray material (Fig. 9D) to create space for the addition of wax where the prosthetic anterior teeth are located (Fig. 9E). Once arranged, the positions of the anterior teeth are verified intraorally for proper phonet-
10 A, Scan of maxillary impression. B, Scan of mandibular impression. C, Teeth arranged in scanned impressions on virtual casts mounted at occlusal vertical dimension.
A B C

42 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
43January 2012
Goodacre et al Goodacre et al
the lip position at rest also can be used to help identify the area where denture teeth can be appropriately located. To determine anterior tooth positions with these guides, the tray handle is removed along with the
impression material located over the occlusal aspect of the tray where the anterior teeth will be positioned. Af-ter applying tray adhesive, medium-body vinyl polysiloxane impression material is placed over the anterior
ridge crest area (Fig. 8A), and the pa-tient is instructed to pronounce the word “thank” followed by pronuncia-tion of the letter “V”. This combina-tion is pronounced 3 times and then the word “thank” is repeated an ad-
8 A, Maxillary tray handle removed along with polymerized impression material. Medium-body vinyl polysiloxane impression material placed into anterior-lingual area. B, Patient pronounced word “thank” and letter “V” to mold ma-terial. C, Polymerized impression material removed anteriorly, medium-body material deposited into area, and patient pronounced letters “Q” and “U” to mold anterior-facial aspect of impression.
9 A, Maxillary and mandibular impressions trimmed so posterior areas do not interfere with each other when patient closes at selected occlusal vertical dimension. B, Midline marked on maxillary impression and buccal corridor evalu-ated. C, Putty indices made over lubricated anterior aspect of maxillary impression. D, Anterior impression material trimmed away and hot wax spatula used to remove tray material, making room for anterior teeth. E, Maxillary anterior teeth arranged. F, Clinical evaluation of maxillary anterior teeth. G, Interocclusal record material placed over lubri-cated impressions with patient occluding at appropriate occlusal vertical dimension. H, Impressions and interocclusal record removed from mouth and record trimmed so intercuspation can be verified.
A B C
A
D
B
E
H
C
F
G
ditional 3 times. When pronouncing the word “thank”, the tongue molds the lingual aspect of the impression material and helps to locate the ap-proximate faciolingual position of the lingual surfaces of the anterior teeth (Fig. 8B). Pronouncing the letter, “V”, helps to identify the incisal length of the impression material and thereby establishes the approximate location of the incisal edge of the maxillary central incisors. After the pronuncia-tion exercise is completed, the patient is instructed to relax their tongue and lips for several seconds. Then the up-per lip is grasped gently and pulled facially so the entire maxillary impres-sion can be removed without disturb-ing any unpolymerized impression material.
Following polymerization of the impression material, the facial half of the anterior impression material is removed to expose the tray, the area coated with adhesive, and the impres-sion material deposited into the recess. The patient is instructed to pronounce the letters “Q” and “U” 3 times and then relax their tongue and lips for sev-eral seconds so the upper lip can rest against the impression material and establish an approximate anteroposte-rior position for the maxillary anterior teeth. The upper lip is then grasped and pulled facially so the impression can be removed without disturbing the incompletely polymerized impres-sion material (Fig 8C).
Resting the upper lip against the unpolymerized impression material is permissible since measurements of the resting pressure of the lip against the maxillary incisors are low. Conse-
quently, this level of pressure is unlikely to produce any substantive displace-ment of the impression material. In fact, in 1 study a slightly negative pres-sure was recorded at rest.47 A second study reported there was no labial pressure against the maxillary incisors in 11 out of 30 subjects and the mean pressure was low.48 When the same author compared adults with differ-ent occlusal relationships, the pres-sure was slightly more positive (mean of 0.08 kPa) for the normal horizon-tal overlap group; 0.14 kPa for the in-creased horizontal overlap group and 0.14 kPa for the reduced horizontal overlap group.49 Another study found the upper lip pressure at rest to be 0.2 kPa with a range from -0.7 to 1.4 kPa; the upper lip pressure was negative in 21 of the 84 children studied.50
A technique has been used where-by patients bring their lips together into light contact and air is blown between the teeth so the upper lip is pushed anteriorly by the air. The up-per lip is allowed to relax and assume its normal resting pressure.47 With this particular technique, a slightly negative pressure was found to be ex-erted on the maxillary incisors.47
Occlusal vertical dimension, tooth positioning, and interocclusal records
The occlusal vertical dimension is
established by using any one of sev-eral appropriate methods and marks placed on the skin for future refer-ence. The maxillary and mandibu-lar impressions are used as record bases to establish the occlusal verti-cal dimension and make interocclu-
sal records. The impressions are both seated simultaneously to evaluate the amount of impression material and tray material that typically has to be removed posteriorly because it inter-feres with proper mandibular closure at the established occlusal vertical di-mension. Following complete closure without interference between the 2 impressions, a scalpel is used to cre-ate notches in the impression materi-al and exposed tray material if present (Fig. 9A). The maxillary impression is placed intraorally so the midline can be marked on the impression with a permanent marker and the buccal corridor space can be assessed (Fig. 9B). The maxillary impression is then ready to have the 6 maxillary anterior prosthetic teeth selected at the initial diagnostic appointment arranged into the area now occupied by impression material. By using the impressions as record bases-wax rims, the previously selected maxillary anterior teeth are ar-ranged in the impression and the tooth size, form, and color verified. As with traditional complete denture tech-niques, different teeth can be selected, should a change need to be made.
Facial and lingual putty indices of the form of the maxillary anterior phonetic impression can be made for use as guides in arranging the anterior teeth (Fig. 9C). To arrange the maxil-lary anterior teeth, impression materi-al is removed along with the required amount of tray material (Fig. 9D) to create space for the addition of wax where the prosthetic anterior teeth are located (Fig. 9E). Once arranged, the positions of the anterior teeth are verified intraorally for proper phonet-
10 A, Scan of maxillary impression. B, Scan of mandibular impression. C, Teeth arranged in scanned impressions on virtual casts mounted at occlusal vertical dimension.
A B C

44 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
45January 2012
Goodacre et alGoodacre et al
ics and modified as necessary to meet the patient’s esthetic requirements (Fig. 9F). The anterior teeth identify the mediolateral orientation of the occlusal plane and along with the posterior impression material, they guide the anteroposterior angulation of the occlusal plane.
The occluding surfaces of the notched impressions are coated with a thin layer of petroleum jelly. Then the 2 impressions are reseated clini-cally and a small amount of soft wax (Periphery Wax, Heraeus Kulzer LLC, South Bend, Ind) is placed onto se-lected areas of the notched impression material as needed so that mandibu-lar closure at the established occlu-
sal vertical dimension will result in stabilized positioning of the impres-sions against the edentulous arches. A vinyl polysiloxane interocclusal re-cord material (EXABITE II NDS Bite Registration Crème; GC America Inc, Alsip, Ill) is injected intraorally so it can flow into the notched occlusal surfaces and around the teeth. The patient’s mandible is then immedi-ately guided to its retruded contact position, and the mandible is closed to the appropriate occlusal vertical dimen-sion where it is maintained motionless until the interocclusal record material is completely polymerized (Fig. 9G). A protrusive interocclusal record can also be made by using the notched impres-
sions. The impressions and interocclusal record are removed from the mouth so the record can be trimmed and accurate intercuspation of the 2 impressions can be further verified extraorally (Fig. 9H).
At this stage, the impressions and interocclusal record are scanned, the teeth arranged virtually in the scanned impressions (Fig. 10A-C), and the surfaces of the bases refined in the computer. The resulting data is then exported to a milling machine for fabrication of the dentures. The first set of complete dentures made with the described clinical proce-dures and milling process are shown in Figure 11A-D. The scanning, virtual arrangement of the teeth, base form
11 A, Maxillary proof of concept denture milled from clear acrylic resin that incorporated recesses into which denture teeth have been bonded. B, Mandibular milled denture base with teeth bonded in place. Note that clear resin block used with this first CAD/CAM fabricated denture was not sufficiently thick to reproduce retromolar pad area of clinical impression. C, Lateral view of mandibular denture showing teeth bonded in position. Note milling marks due to use of 3-axis milling machine and large tools during fabrication of this proof of concept denture. D, Maxillary denture placed intraorally.
A B 12 A, Virtual maxillary cast with posterior palatal seal “carved” into cast based on clinical measurements. B, Seal applied to scan of maxillary impression.
A B C
D
development, and the milling proce-dures were performed by using these procedures (Courtesy of Dr. Stephen Schmitt, Voxelogix Corporation, San Antonio, Texas). The 3-axis milling machine and large milling tool used in this first proof-of-concept denture resulted in a denture base with sub-stantial milling lines, but the clinical procedures were validated.
Subsequently, the process focused on the refinement of the base mill-ing by using a 5-axis milling machine and fine milling tools. Additionally, a posterior palatal seal technique was developed whereby a seal was cre-ated by “carving” it into the virtual cast based on clinical measurements that identified the appropriate loca-tion, form, and depth of the seal (Fig. 12A). The form created in the virtual cast was then applied to the scanned image of the impression so a seal would be present in the milled den-ture (Fig. 12B).
Recently, the previously described procedures have been used to scan clinical records (Fig. 13A), create and articulate virtual casts (Fig. 13B), ar-
range the teeth, and virtually form the bases (Fig. 13C). The resulting data were used to mill a denture base from a block of pink denture base resin with recesses into which conventional den-ture teeth were bonded (Fig. 13D-F).
Another future possibility would be to import the clinical base mor-phology and tooth position data into an enhanced version of the 3-D Tooth Arrangement Program, arrange the teeth and form the bases virtually, and then export the resulting data to a milling machine for fabrication of the prostheses.
SUMMARY It is anticipated that the fabrica-
tion of complete dentures will be commercially available with CAD/CAM technology. The clinical impres-sion procedures described in this ar-ticle record the morphology of the intaglio and cameo surfaces of com-plete denture bases and also identify muscular and phonetic locations for the placement of prosthetic denture teeth. This information can then be
scanned, the teeth and base forms virtually established, and the resulting data exported to a milling machine for fabrication of the denture bases.
In addition to the development of clinical procedures that record the required morphology, the prototype 3D Tooth Arrangement Program de-scribed in this article indicates that CAD programs can be developed whereby prosthetic teeth are arranged virtually as part of the CAD/CAM fab-rication of complete dentures.
REFERENCES
1. What is CAD/CAM? Internet. Harvard University Graduate School of Design. Available from http://internal.gsd.harvard.edu/inside/cadcam/whatis.html
2. CAD software history. Internet. CADAZZ.com. 2004. Available from http://www.cadazz.com/cad-software-history.htm
3. Marchack CB. The use of CAD CAM fabrication technology. chapter in Implant dentistry DVD-ROM v.1.0.07.378, Loma Linda University School of Dentistry, 2007.
4. Mörmann WH. The origin of the Cerec method: a personal review of the first 5 years. Int J Comput Dent 2004;7:11-24.
5. Mörmann WH. The evolution of the CEREC system. J Am Dent Assoc 2006;137suppl:7S-13S.
13 A, Scans of most recent patient treatment where maxillary and mandibular impressions were made and 4 maxil-lary incisors arranged. Scans have been articulated by using interocclusal record. B, Virtual mounted casts. C, Virtual arrangement of maxillary teeth and base formed from impression scan. D, Denture base being milled from block of pink denture base resin. E, Recesses in denture base being refined to accept cervical morphology of prosthetic teeth. F, Milled maxillary denture base with prosthetic teeth bonded in place. Milling was performed with 5-axis milling ma-chine and fine tools. Denture base is not polished. Small ridge on facial surface was produced as milling tool changed direction of approach to denture base.
A
D
B
E
C
F

44 Volume 107 Issue 1
The Journal of Prosthetic Dentistry
45January 2012
Goodacre et alGoodacre et al
ics and modified as necessary to meet the patient’s esthetic requirements (Fig. 9F). The anterior teeth identify the mediolateral orientation of the occlusal plane and along with the posterior impression material, they guide the anteroposterior angulation of the occlusal plane.
The occluding surfaces of the notched impressions are coated with a thin layer of petroleum jelly. Then the 2 impressions are reseated clini-cally and a small amount of soft wax (Periphery Wax, Heraeus Kulzer LLC, South Bend, Ind) is placed onto se-lected areas of the notched impression material as needed so that mandibu-lar closure at the established occlu-
sal vertical dimension will result in stabilized positioning of the impres-sions against the edentulous arches. A vinyl polysiloxane interocclusal re-cord material (EXABITE II NDS Bite Registration Crème; GC America Inc, Alsip, Ill) is injected intraorally so it can flow into the notched occlusal surfaces and around the teeth. The patient’s mandible is then immedi-ately guided to its retruded contact position, and the mandible is closed to the appropriate occlusal vertical dimen-sion where it is maintained motionless until the interocclusal record material is completely polymerized (Fig. 9G). A protrusive interocclusal record can also be made by using the notched impres-
sions. The impressions and interocclusal record are removed from the mouth so the record can be trimmed and accurate intercuspation of the 2 impressions can be further verified extraorally (Fig. 9H).
At this stage, the impressions and interocclusal record are scanned, the teeth arranged virtually in the scanned impressions (Fig. 10A-C), and the surfaces of the bases refined in the computer. The resulting data is then exported to a milling machine for fabrication of the dentures. The first set of complete dentures made with the described clinical proce-dures and milling process are shown in Figure 11A-D. The scanning, virtual arrangement of the teeth, base form
11 A, Maxillary proof of concept denture milled from clear acrylic resin that incorporated recesses into which denture teeth have been bonded. B, Mandibular milled denture base with teeth bonded in place. Note that clear resin block used with this first CAD/CAM fabricated denture was not sufficiently thick to reproduce retromolar pad area of clinical impression. C, Lateral view of mandibular denture showing teeth bonded in position. Note milling marks due to use of 3-axis milling machine and large tools during fabrication of this proof of concept denture. D, Maxillary denture placed intraorally.
A B 12 A, Virtual maxillary cast with posterior palatal seal “carved” into cast based on clinical measurements. B, Seal applied to scan of maxillary impression.
A B C
D
development, and the milling proce-dures were performed by using these procedures (Courtesy of Dr. Stephen Schmitt, Voxelogix Corporation, San Antonio, Texas). The 3-axis milling machine and large milling tool used in this first proof-of-concept denture resulted in a denture base with sub-stantial milling lines, but the clinical procedures were validated.
Subsequently, the process focused on the refinement of the base mill-ing by using a 5-axis milling machine and fine milling tools. Additionally, a posterior palatal seal technique was developed whereby a seal was cre-ated by “carving” it into the virtual cast based on clinical measurements that identified the appropriate loca-tion, form, and depth of the seal (Fig. 12A). The form created in the virtual cast was then applied to the scanned image of the impression so a seal would be present in the milled den-ture (Fig. 12B).
Recently, the previously described procedures have been used to scan clinical records (Fig. 13A), create and articulate virtual casts (Fig. 13B), ar-
range the teeth, and virtually form the bases (Fig. 13C). The resulting data were used to mill a denture base from a block of pink denture base resin with recesses into which conventional den-ture teeth were bonded (Fig. 13D-F).
Another future possibility would be to import the clinical base mor-phology and tooth position data into an enhanced version of the 3-D Tooth Arrangement Program, arrange the teeth and form the bases virtually, and then export the resulting data to a milling machine for fabrication of the prostheses.
SUMMARY It is anticipated that the fabrica-
tion of complete dentures will be commercially available with CAD/CAM technology. The clinical impres-sion procedures described in this ar-ticle record the morphology of the intaglio and cameo surfaces of com-plete denture bases and also identify muscular and phonetic locations for the placement of prosthetic denture teeth. This information can then be
scanned, the teeth and base forms virtually established, and the resulting data exported to a milling machine for fabrication of the denture bases.
In addition to the development of clinical procedures that record the required morphology, the prototype 3D Tooth Arrangement Program de-scribed in this article indicates that CAD programs can be developed whereby prosthetic teeth are arranged virtually as part of the CAD/CAM fab-rication of complete dentures.
REFERENCES
1. What is CAD/CAM? Internet. Harvard University Graduate School of Design. Available from http://internal.gsd.harvard.edu/inside/cadcam/whatis.html
2. CAD software history. Internet. CADAZZ.com. 2004. Available from http://www.cadazz.com/cad-software-history.htm
3. Marchack CB. The use of CAD CAM fabrication technology. chapter in Implant dentistry DVD-ROM v.1.0.07.378, Loma Linda University School of Dentistry, 2007.
4. Mörmann WH. The origin of the Cerec method: a personal review of the first 5 years. Int J Comput Dent 2004;7:11-24.
5. Mörmann WH. The evolution of the CEREC system. J Am Dent Assoc 2006;137suppl:7S-13S.
13 A, Scans of most recent patient treatment where maxillary and mandibular impressions were made and 4 maxil-lary incisors arranged. Scans have been articulated by using interocclusal record. B, Virtual mounted casts. C, Virtual arrangement of maxillary teeth and base formed from impression scan. D, Denture base being milled from block of pink denture base resin. E, Recesses in denture base being refined to accept cervical morphology of prosthetic teeth. F, Milled maxillary denture base with prosthetic teeth bonded in place. Milling was performed with 5-axis milling ma-chine and fine tools. Denture base is not polished. Small ridge on facial surface was produced as milling tool changed direction of approach to denture base.
A
D
B
E
C
F

46 Volume 107 Issue 1
The Journal of Prosthetic Dentistry Goodacre et al
6. Fish EW. Using the muscles to stabilize the full lower denture. J Am Dent Assoc 1933;20:2163-9.
7. Beresin VE, Schiesser FJ. The neutral zone in complete dentures. J Prosthet Dent 1976;36:356-67.
8. Fröhlich K, Thüer U, Ingervall B. Pressure from the tongue on the teeth in young adults. Angle Orthod 1991:61:17-24.
9. Fröhlich K, Ingervall B, Thüer U. Further studies of the pressure from the tongue on the teeth in young adults. Eur J Orthod 1992;14:229-39.
10.Thüer U, Janson T, Ingervall B. Applica-tion in children of a new method for the measurement of forces from the lips on the teeth. Eur J Orthod 1985;7:63-78.
11.Laney WR, Gonzalez JB. The maxillary den-ture: its palatal relief and posterior palatal seal. J Am Dent Assoc 1967;75:1182-7.
12.Morrison ML. Phonetics as a method of determining vertical dimension and centric relations. J Am Dent Assoc 1959;59:690-5.
13.Guichet NF. Occlusion. Edition 2, Anaheim, Niles F. Guichet, DDS, 1997. p 77.
14.Chierici G, Lawson L. Clinical speech con-siderations in prosthodontics: perspectives of the prosthodontist and speech patholo-gist. J Prosthet Dent 1973;29:29-39.
15.Kestenberg JM. Speech assessment in den-tistry. Aust Dent J 1983;28:98-101.
16.Howell PGT. Incisal relationships during speech. J Prosthet Dent 1986;56:93-99.
17.Silverman MM. Accurate measurement of vertical dimension by phonetics and the speaking centric space. Dent Dig 1951;57:308-11.
18.Silverman MM. The speaking method in measuring vertical dimension. 1952. J Pros-thet Dent 2001;85:427-31.
19.Silverman MM. Determination of vertical dimension by phonetics. J Prosthet Dent 1956;6:465-71.
20.Pound E. Let /S/ be your guide. J Prosthet Dent 1977;38:482-9.
21.Pound E. The vertical dimension of speech: the pilot of occlusion. J Calif Dent Assoc 1978;2:42-7.
22.Benediktsson E. Variations in tongue and jaw positions in “S” sound production in relation to front teeth occlusion. Acta Ondontol Scand 1957;15:275-303.
23.Gillings BR. Jaw movements in young adult men during speech. J Prosthet Dent 1973;29:567-76.
24.Burnett CA, Clifford TJ. Closest speaking space during the production of sibilant sounds and its value in establishing the vertical dimension of occlusion. J Dent Res 1993;72:964-967.
25.Burnett CA. Mandibular incisor posi-tion for English consonant sounds. Int J Prosthodont 1999;12:263-271.
26.Lu GH, Chow TW, So LK, Clark RK. A computer-aided study of speaking spaces. J Dent 1993;21:289-96.
27.Rothman R. Phonetic considerations in denture prosthesis. J Prosthet Dent 1961;11:214-23.
28.Palmer JM. Analysis of speech in prosth-odontic practice. J Prosthet Dent 1974;31:605-14.
29.Glossary of Prosthodontic Terms. 8th Ed. J Prosthet Dent 2005; 94:1-92.
30.Whitmyer CC, Esposito SJ. Principles of speech and their application to dental re-construction. Compend Contin Educ Dent 1998;19:378-82, 384-5.
31.Moses ER. A brief history of palatography. Q J Speech 1940;26:615-625.
32.Coles O. On the production of articulate sound. Trans Odontol Soc Great Britain 1872;4:110-23.
33.Moses ER. Palatography and speech move-ment. J Speech Disord 1939;4:103-14.
34.Sears VH. Principles and techniques for complete denture construction. St. Louis, CV Mosby Co, 1949, p. 312-321.
35.Allen LR. Improved phonetics in denture con-struction. J Prosthet Dent 1958;8:753-763.
36.Rothman R. Phonetic considerations in denture prosthesis. J Prosthet Dent 1961;11:214-223.
37.Hansen CA, Singer MT. Correction of defective sibilant phonation created by a complete maxillary artificial denture. Gen Dent 1987;35:357-60.
38.Goyal BK, Greenstein P. Functional con-touring of the palatal vault for improving speech with complete dentures. J Prosthet Dent 1982;48:640-46.
39.Farley DW, Jones JD, Cronin RJ. Palatogram assessment of maxillary complete dentures. J Prosthodont 1998;7:84-90.
40.Slaughter MD. Speech correction in full den-ture prosthesis. Dent Dig 1945;51:242-246.
41.Harley WT. Dynamic palatography--a study of linguopalatal contacts during the production of selected consonant sounds. J Prosthet Dent 1972;27:364-76.
42.Hamlet SL, Stone M. Speech adaptation to dental prostheses: the former lisper. J Prosthet Dent 1982;47:564-9.
43. Wrench AA, Advances in EPG palate de-sign. Adv Speech Lang Pathol 2007;9:3-12.
44.Proffit WR, McGlone RE. Tongue-lip pres-sures during speech of Australian Aborigi-nes. Phonetica 1975;32:200-20.
45.Tanaka H. Speech patterns of edentulous patients and morphology of the palate in relation to phonetics. J Prosthet Dent 1973;29:16-28.
46.Goodacre CJ, Lowry J. Speech. Chapter in Electronic atlas of human occlusion and the TMJ, DVD-ROM v.1.0, eHuman.com, 2008. p 141.
47.Gould MS, Picton DC. A study of pressures exerted on the lips and cheeks on the teeth of subjects with normal occlusion. Arch Oral Biol 1964;9:469-78.
48.Luffingham JK. Pressure exerted on teeth by the lips and cheeks. Dent Practit 1968;19:61-64.
49.Luffingham JK. Lip and cheek pressure exerted upon teeth in three adult groups with different occlusion. Arch Oral Biol 1969;14:337-50.
50.Thüer U, Ingervall B. Pressure from the lips on the teeth and malocclusion. Am J Or-thod Dentofac Orthop 1986;90:234-42.
Corresponding author:Dr Charles J. GoodacreLoma Linda University School of Dentistry11092 Anderson StreetLoma Linda, CA 92350 Fax: 909-558-0483 E-mail: [email protected]
Copyright © 2012 by the Editorial Council for The Journal of Prosthetic Dentistry.
Linsen et al
Clinical ImplicationsWithin the limitations of this study, the registration technique has an influence on condylar position and muscular symmetry. Greater symmetry in muscular activity and anterior condyle position dur-ing intermaxillary registration may result in higher occlusal stability and a reduction of nonphysiological condylar loads after prosthetic restorative and orthodontic treatments.
Statement of problem. It is unclear whether different intermaxillary registration techniques are related to a physiologi-cal condylar position that permits neuromuscular equilibrium.
Purpose. This study analyzes and quantifies the effects of different registration techniques on the condyle position and how the registration technique modulates bilateral masseter and anterior temporalis muscle electromyographic activity.
Material and methods. Three-dimensional electronic condylar position analysis (EPA) with an ultrasound-based jaw-tracking system and surface electromyographic activity (sEMG) was recorded during the registration of a manu-ally guided centric relation (CR), maximal intercuspation (MI), and Gothic arch tracing guided centric relation (DIR method). Participants were 26 stomatognathically healthy volunteers (mean age, 30.6 ±9.5 years). Data were analyzed by 1-way ANOVA and post hoc Bonferroni correction (α=.05).
Results. EPA showed significant differences (P<.001) for CR, MI, and DIR in the vertical, sagittal, and horizontal axes. The condyle position during DIR was found to be significantly more anteriorly and inferiorly located than with CR (P<.001) and MI (P<.04). There were no significant differences in the mean muscle activity among CR, MI, and DIR. Muscular symmetry ranged from 63.87 to 81.47%. Significantly higher symmetry for the anterior temporalis (P=.03) and the masseter (P=.03) was found during the DIR than with CR. Torque coefficients (potential laterodeviating ef-fect) were between 88.02% (CR) and 89.94% (MI).
Conclusions. Registration technique significantly influenced the condyle position, while mean muscular activity was minimally affected. With respect to muscular balance and activation, the DIR position proved to be capable of inducing the greatest motor unit activity when compared with manually guided CR and MI. (J Prosthet Dent 2012;107:47-52)
The influence of different registration techniques on condyle displacement and electromyographic activity in stomatognathically healthy subjects: A prospective study
Sabine S. Linsen, Dr Med Dent,a Helmut Stark, Prof Dr Med Dent,b and Azadeh Samaic
Preclinical Education and Dental Materials Science, Rheinische Friedrich-Wilhelms University of Bonn, Bonn, Germany
aAssociate Professor, Department of Prosthodontics.bClinical Professor and Head of Department, Department of Prosthodontics.cResearch Fellow, Department of Prosthodontics.
Recording maxillomandibular rela-tionships is a central aspect of prosth-odontics. For both dentate and eden-tulous patients, this measurement has an important role in prosthetic rehabil-
itation, temporomandibular dysfunc-tion (TMD) therapy, and orthodontic and maxillofacial planning, the treat-ment goal of which is to achieve har-monious relationships among teeth,
joints, and muscles. Different meth-ods are used for intermaxillary record-ings such as registration in maximum intercuspation (MI) or centric rela-tion (CR). MI refers to the complete
Erratum
Dr. Faysal Succaria is a new Diplomate of the American Board of Prosthodontics (ABP) effective February 2011, and should have been listed in the ABP Annual Report published in the December 2011 journal.





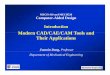

![CAD/CAM Denture Base Resins - AvaDent Digital Dentures · Besides poor denture design [2], denture failure is attributed to the denture base resins’ poor mechanical properties [3]](https://img.pdfslide.us/doc/110x75/5ed5623cf871d67955066b55/cadcam-denture-base-resins-avadent-digital-dentures-besides-poor-denture-design.jpg)