Embed Size (px)
Citation preview
Department Name/Subheading | Vol. XX, No. XX, 2011
Vol. 7 Mar. 2013
Contents:• Economic Aspects of
CABANA Research
• International Spotlight
• North American Spotlight
• North American Spotlight
• A Message from the NHLBI
• Critical Importance of Data Quality and Subject Follow-up
• Enrollment Updates
• Kristi’s Korner
Economic Aspects of CABANA ResearchDaniel B. Mark, MD, MPHPrincipal Investigator of Economic and Quality of Life Coordinating CenterDuke Clinical Research Institute The economy of the US is still in serious trouble. We know this because the newspapers, the talking heads on the news programs on TV and the Internet tell us so almost every day. They say the number one reason is the cost of US health care. We spend and will spend in the future much more than we can afford. This undermines the economy similar to the way slow rot
undermines an old tree. To make matters worse, the macro parameters of health in the US, such as life expectancy, are not any better than for countries with far less health care spending. Even countries that spend less than the US on health care are struggling with the relentless tendency of yearly rising medical costs.
We in medicine are the victims of our own success. Medical care costs more, in part at least, because it continues to improve. Comparing today’s costs with those 10 years ago fails to account for the ways in which we can do more for patients now. The conclusion: medicine is still rife with wasteful care and something major needs to be done. That something is playing out now as there are dramatic shifts in how care is organized, delivered and paid for.
One aspect of these shifts is an unprecedented focus on what is now called comparative effectiveness research, or simply � guring out what works and what doesn’t, and discarding the latter. In an unconscious irony, although the federally supported comparative effectiveness research is legislatively prohibited in the Accountable Care Act from considering cost effectiveness, it is actually the cost effectiveness of care that this legislation seeks to de� ne. Sound confusing? Consider three things: 1) most care that is in current use provides some bene� t that can actually be measured given a large enough sample of patients, 2) it is not the presence of bene� t that is of most interest but the magnitude of bene� t, and 3) the relation
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
For more information check out our web site at www.cabanatrial.org
– Continued on next page.

2 CABANA News | Vol. 7 | Spring 2013
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
between the extra bene� t provided and the extra cost required to provide that bene� t is what cost effectiveness analysis assesses. To say that some therapy is more cost effective is to say that it’s a more ef� cient way of providing health bene� ts to society for a given monetary investment.
Economics starts with the fundamental assumptions that our resources are � nite and if we choose to produce more health care, we lose the ability to produce something else we value, like education or better transportation systems. How much money the country should spend on health care overall is a policy question, to be settled by the elected representatives at state and national government levels. How to spend the available money most ef� ciently to provide the most health bene� ts for society is what cost effectiveness is designed to assist with.
As you are aware, the CABANA trial is measuring costs in the US patients, and cost effectiveness as key secondary
endpoints of the trial (the US perspective is the primary analysis planned, but analyses from other country perspectives will be possible using much of the same analysis work). As noted, we no longer exist in a world where the medical community can insist that everything they want to do be paid for. Assuming the trial shows bene� ts for ablation therapy as postulated in our NHLBI grant application, payers, patients and policy makers, among others, will want to know the rest of the story: is AF ablation good value for money, or not? Or, to put it another way, does AF ablation produce enough bene� ts such that it provides an ef� cient way to increase health care bene� ts relative to conventional benchmarks for cost effectiveness (such as the <$50,000 US per quality adjusted life year benchmark). Our plan at the DCRI Economic and Quality of Life Coordinating Center is to start working on these analyses as soon as possible following the main clinical analysis, after data base lock. So fasten your seat belts! The best part of the CABANA ride is yet to come. CABANA will clearly be a practice changing clinical trial.
We have been given the opportunity to collaborate with another NIH supported trial, the RECRUIT Trial. This trial is designed to speci� cally enhance the enrollment of minorities through specialized training and recruitment tools. If minority populations are accessible to your site, we encourage you to join in this trial as well. A special THANK YOU to our sites, Baylor All Saints Medical Center, University of North Carolina at Chapel Hill, Cooper University Hospital, Robert Wood Johnson University Hospital, Scott and White Memorial Hospital, Mount Sinai Medical Center, that have already expressed their interest in this important collaborative effort. Here’s my next challenge to each site, Please enroll at least 1 subject this next month. That would de� nitely boost our total and exceed the goal of 55-60. With 128 active sites, we can do this... As we move further in 2013, I look forward to watching the steadily climbing enrollment. – Kristi
Kristi Monahan, RN, Project DirectorCABANA Administration, Mayo Clinic
Re� ecting back on February, AHA’s-Go Red for Women month, I would like to personally recognize and THANK those sites that met or exceeded the challenge of enrolling 1 female into CABANA. Leading that challenge was Columbia University-Dr. Garan and University of Calgary-Dr. Veenhuyzen, enrolling not only 1 but 2 women during February. Followed by Providence Saint Vincent Medical Center-Dr. Halperin, Virginia Hospital Center-Dr. Rashid, Cardiac Study Center-Dr. Salam, Cardioaniologisches Centrum Bethanien-Dr. Chun, Asklepios Klinik Barmbek-Dr. Groenefeld, and Research Institute of Circulation Pathology-Dr. Pokushalov each enrolling 1 woman.
As you are all aware, as an NIH supported trial, we strive to comply with the guidelines for speci� c enrollment rates of women and minorities. We, as an overall team (again, a special thanks to those listed above) are meeting the rate for women enrollment, however, our minority recruitment continues to be lower than anticipated.
risti’sKorner

3 CABANA News | Vol. 7 | Spring 2013
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
Critical Importance of Data Quality and Subject Follow-upDr. Kerry Lee, PhD, Duke Clinical Research Institute Many of the communications you have received to date in CABANA have been focused on recruiting and enrolling
patients, as that has been the key emphasis in order to kick-start the study and move CABANA forward toward the study’s enrollment goals. Now with over 1,000 subjects enrolled, it is important that attention be focused on the quality and completeness of the subject data, particularly the critical follow-up data required to accurately characterize the clinical course and outcomes of CABANA subjects after their enrollment.
There are several aspects of data quality that re� ect on the integrity of the study and that will impact the scienti� c rigor and credibility of the results. First and foremost, it is important to maintain regular contact with the subjects in order that the important follow-up and outcome information is collected and that subjects don’t “fall through the cracks” and become lost to follow-up or decide they no longer want to be a part of the study. It is essential that the number of subjects who are lost to follow-up or withdraw consent be kept to an absolute minimum. If there is a high rate of subject withdrawal or lack of complete follow-up, the study will be criticized and disregarded by the clinical and scienti� c community, and the impact that it could otherwise have on the future care of patients with atrial � brillation will be greatly reduced.
It is also important that data entry be kept up to date. Entering the data as soon as possible after contact with the subject has the advantage that the data are reported while still fresh in mind and before important details and documentation are forgotten or perhaps misplaced. As a result, any queries that might be generated from the data can be addressed more ef� ciently than would be possible after memory of the visit has faded and the trail leading to a correct response has become cold. Timely entry of data is also very important so that subject status reports generated regularly by the Coordinating Center for the study leadership, the NHLBI, and the Data and Safety Monitoring Board (DSMB) are up to date, complete, and accurate. We urge you to give high priority and major emphasis to subject follow-up and data quality. The randomization of a subject is an important beginning, but it is only the � rst step. The key to successfully completing CABANA and fully achieving the study’s goals depends not only on enrolling patients, but of crucial importance is how well we achieve complete follow-up and provide accurate and complete data. Missing follow-up in a relatively small number of subjects
could alter the outcome and interpretation of the study. Furthermore, differential follow-up in the two arms of the trial could seriously compromise the scienti� c interpretation of the trial.
Following are a few suggestions to keep in mind as you work to minimize subject withdrawals from the trial and ensure that subject follow-up is as complete as humanly possible.
• Prior to randomizing the subject, make certain he/she is fully informed about what is expected of them in terms of regular follow-up contacts. It may be helpful to emphasize the bene� ts to the subject of the regular follow-up contacts.
• If a subject no longer wants to be a part of the study because they do not wish to return for follow-up as frequently as outlined in the protocol, � exibility in the frequency of follow-up is much better than losing the subject. Telephone follow-up rather than actual clinic visits may be more acceptable to the subject, especially where distance from the clinic is a factor. Most patients appreciate having medical caregivers follow-up with them, and if they are treated with care and compassion, it should be very rare that a subject requests no further follow-up contact.
• For working with diffi cult subjects, it is important that the physician investigator be involved and help intervene with the subject.
• If there are changes in personnel at your site, make certain that an appropriate transition occurs with respect to the ongoing follow-up of the subjects.
Remember that once subjects are randomized, they are in the trial, and should be carefully followed from that moment forward until either death or the end of the study. Again, we urge you to enter data promptly following each contact with the subject.
Thank you for all of your efforts in support of CABANA. We are all part of this highly important undertaking, and achieving success will require our united and best efforts.
Mark Your Calendar!For those attending:
Heart Rhythm 2013(Denver, CO)
Join us for a CABANA Reception on Wednesday, May 8, 2013
from 8-9:30 P.M. (venue to be determined).
4 CABANA News | Vol. 7 | Spring 2013
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
equipoise between these modalities. We are motivated by the clinical relevance of this trial and the high pro� le attention it has received. We feel privileged to be part of this effort. Above all, we are motivated by our patients. Veterans are always eager to be � rst in line to participate in a noble cause. In this case that of medical discovery. We dedicate our efforts in honor of their sacri� ce.
North American Spotlight: V.A. Pittsburgh Healthcare System – Pittsburgh, PA
For the past 15 years the arrhythmia service at the V.A. Pittsburgh Healthcare System has supported a robust clinical research program that has depended on the full array of clinical services provided. We have been privileged to be active participants in such important trials that have helped delineate the best practices in the management of cardiac arrhythmic disease. SAFE-T a V.A. Cooperative Study which studied the relative safety of amiodarone and sotalol in the management of atrial � brillation in the elderly and DEFINITE which helped establish the role of implantable de� brillators in patients with nonischemic cardiomyopathy were important practice de� ning trials started just over a decade ago. The V.A. environment lends itself well to intra-disciplinary and multidisciplinary collaboration and as a result investigator initiated trials studying the potential impact of CRT therapy on sleep disordered breathing as an example and the potential biomarker footprint for CRT responders as another were natural products in this environment.
Today, we are pleased to be active participants in CABANA. This is a timely study of a signi� cant clinical problem that begs clear direction. The technology available for ablation of atrial � brillation has matured and greatly facilitated the procedure with ever improving outcomes. However, the question as to its appropriate order as a tool in the effort to manage atrial � brillation has become more pressing than ever. This is where CABANA comes in as a timely, well thought out, trial. By randomizing to medical therapy versus ablation and closely monitoring near and intermediate term outcome the trial will help resolve the existing clinical
Left to right: Dr. Alaa Shalaby, PI Director of electrophysiology service; Mike Seese, Research Coordinator, Joe Falcona, Radiology Technician; Karen Nave, Clinical Nurse Specialist; John Linden, RN; Martin Mains, RN; John Nosbisch, RN; Dr. Eathar Razak, Electrophysiologist; Dr. Padmaraj Samerandra, Cardiologist; Not Pictured: Jennifer Cisar, Research Coordinator
woman in honor of National Wear Red Day® and to “keep with the beat” during Heart Health month. As 2013 moves along, we also note that CABANA has entered into its � fth year of funding support from the NHLBI and industry partners. While we celebrate CABANA’s fourth anniversary, we are reminded that there is still important work left to do to complete CABANA’s intended goals. Let’s take the early momentum of 2013 and build on it for the rest of this year. With 128 sites currently active, we can make the difference for atrial � brillation patients everywhere.
A Message from the NHLBILynn Rundhaugen, MPH
Happy New CABANA Year! We are only a few weeks into 2013, yet there has been a lot of activity in CABANA. The month of January marked the enrollment of participant number 1000 and the Data Safety and Monitoring Board (DSMB) met in person to review the study’s progress to date. January 2013 also goes down in the CABANA history books as the 5th time since the study began to reach enrollment of 40 subjects or more in a month. In February, sites were encouraged to enroll at least one
5 CABANA News | Vol. 7 | Spring 2013
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
North American Spotlight: Georgia Health Sciences University – Augusta, GA
The Georgia Regents University ( formerly the Medical College of Georgia) Cardiac Electrophysiology Program in Augusta, GA is a comprehensive arrhythmia treatment center providing care to adolescent and adult patients. We are proud to be participating in the CABANA trial.
In 2005, Dr. Robert Sorrentino left his practice at Duke to resurrect the then defunct EP program at MCG. In 2006, he recruited Dr. Adam Berman from Duke to Augusta to develop the complex ablation program. Over the past 8 years, our program has grown tremendously, now offering a full array of complex EP procedures in 2 state of the art EP labs including laser lead device extraction, Stereotaxis catheter ablations, and hybrid endocardial-epicardial AF ablation in select patient populations.
In 2012, Dr. Will Maddox was recruited from UAB to join our EP faculty to help serve our expanding patient base. A superb team of physician’s assistants and EP/Device nurses supports us. Our EP lab staff is very skilled in all aspects of complex device and catheter procedures.
As Georgia’s state medical university, our EP section is committed to teaching. In 2008, we launched an ACGME accredited EP fellowship program. Our section is very active in CME based learning activities, including hosting an annual CME event. We have been fortunate to serve as a clinical training site for Stereotaxis ablation procedures.
Additionally, we are very active in clinical investigations. Ongoing research includes drug, ablation and device-based protocols. We also conduct several translational research projects in conjunction with basic scientists on campus. We are indebted to our dedicated and hard-working research study coordinators who make our research possible.
The CABANA trial was initiated at our center in spring, 2012. All of our EP physicians are investigators here, and enrollment has been steadily increasing at our center. We collectively feel that the CABANA trial is of great importance to the � eld of cardiac electrophysiology. When we discuss the trial with patients and referring physicians, we often underscore the paucity of prospective randomized data regarding the invasive and medical treatment of AF. CABANA seeks to answer this fundamental question in AF care, and we feel its impact will be felt for years to come.
As a large medical center surrounded by a rural population, we often encounter patients with a recent diagnosis of AF and various other cardiovascular co-morbidities. Much of our enrollment has been from this population, the drug-naïve who are very interested in
progressive AF care. Consequently, we’ve enrolled a wide spectrum of patients with diverse pro� les. This highlights the “real-world” nature of AF care and confers further validity on the study’s design.
We hope CABANA enrollment will continue to grow. It’s interesting to us that many of our patients want to participate in clinical research because they feel that it will help others. We agree, but remind them that participation in CABANA may help them as well. We plan to continue our recruitment efforts and we’re grateful to the CABANA study team for their support of this important trial.
Left to Right: Adam E. Berman, MD FHRS; Carol Smith, RN; Rob Sorrentino, MD FHRS; Will Maddox, MD; Heather Burleson MMS, PA-C
The following new drugs have been approved for use within the CABANA trial by the Innovative Drug Therapy Committee:
Xarelato® (rivaroxiban)
Eliquis® (apixaban)
Pilsicainide
New Drug Approvals

6 CABANA News | Vol. 7 | Spring 2013
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
International Spotlight: Hanseatic Heart Center, Asklepios Klinik St. Georg – Hamburg, Germany
The electrophysiology (EP) unit at the Hanseatic-Heart-Center / St. Georg-hospital in Hamburg/Germany is committed to modern and state-of-the-art conservative and interventional treatment of patients suffering from various kinds of arrhythmias. Our EP unit has 3.5 EP labs for ablation therapies as well as for device implantation. The interventions are performed by 8 staff physicians and 4-5 international EP fellows per year. The development, investigation and application of novel diagnostic and therapeutic treatment options and treatment devices is one of our key scienti� c focuses. Particularly we concentrate on the treatment of atrial � brillation (AF) based on either antiarryhthmic drug therapy or on catheter ablation. In 2012 we performed 1800 catheter ablations at St. Georg hospital including 75% ablations of AF and atrial tachycardia after AF ablation. New ablation strategies as well as different energy sources were applied in the last 10 years. In addition to studies initiated in our center we actively participate in multiple-center international AF studies such as RAAFT, CABANA, EAST, Fire and Ice, Man and Machine, and ATTEST.
AF is the most frequent arrhythmia in most EP units and its signi� cance will even increase in the future. Different therapeutic treatment options are established aiming for improvement of symptoms. Currently there are different antiarrhythmic drug therapies available which are associated with a moderate ef� cacy in terms of reduction of AF burden and variable side effect pro� les often resulting in discontinuation. Catheter-based ablation strategies aim for isolation of the pulmonary veins eventually extended to ablation of complex fractionated atrial electrograms (CFAE) or performance of linear lesions where necessary. However, so far there is only limited data available comparing both treatment strategies in a multicenter, prospective, randomized fashion. Recently the MANTRA-PAF study (antiarrhythmic treatment versus radiofrequency ablation in paroxysmal AF) was published and stated no signi� cant difference between the ablation group and the drug-therapy group concerning the cumulative burden of AF in patients with history of paroxysmal AF. However, at 24 months the burden of AF was signi� cantly lower in the ablation group and more patients in the ablation group were free from any AF as well as from symptomatic AF. Preliminary data from
the RAAFT-study (radiofrequency ablation versus antiarrhythmic drug therapy as � rst-line treatment of symptomatic atrial � brillation) show superiority of AF ablation over conservative treatment in terms of recurrence of symptomatic AF (41% vs. 58%, p=0.01). However, procedure-related complications or death still can occur in these studies.
So far more data based on large patient numbers is necessary before � nal conclusions can be drawn. The CABANA trial is an international, multicenter, prospective, randomized study. It is the � rst study comparing catheter ablation and antiarrhythmic drug therapy in AF patients focusing on total mortality and key secondary endpoints such as a composite endpoint of total mortality, disabling stroke, serious bleeding, or cardiac arrest and a composite endpoint of total mortality and cardiovascular hospitalization. The results of this study will further clarify the value of the currently established treatment options. Consequently every endeavor is made in our center to promote the study by enrolling as many subjects as possible. Just recently, we successfully enrolled the 1000th subject worldwide.
Left to Right: Karl-Heinz Kuck, M.D.; Feifan Ouyang, M.D.; Roland Tilz, M.D.; Sebastian Deiß, M.D.; Hisaki Makimoto, M.D.; Andreas Metzner, M.D.; Erika Jacobsen; Claudia Kalkowski; Shibu Mathew, M.D.; Not Pictured: Andreas Rillig, M.D.; Erik Wissner, M.D.; Peter Rausch, M.D.
7 CABANA News | Vol. 7 | Spring 2013
CABANA NewsCatheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation
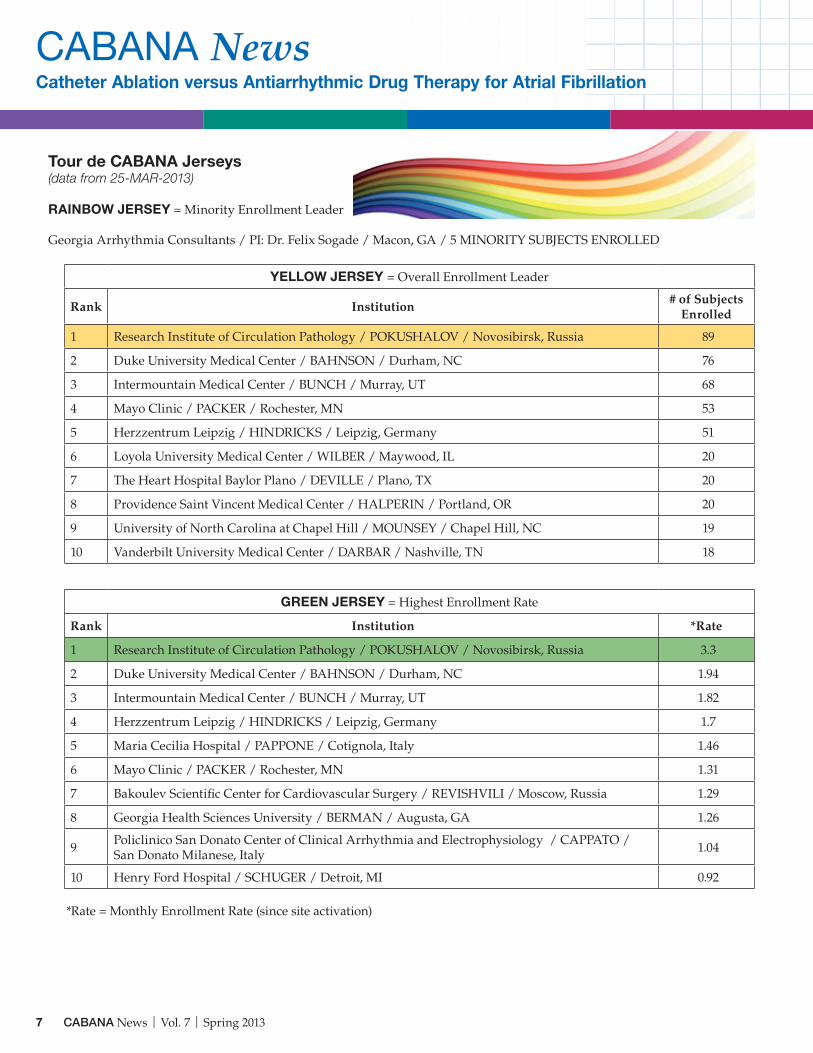
Tour de CABANA Jerseys(data from 25-MAR-2013)
RAINBOW JERSEY = Minority Enrollment Leader
Georgia Arrhythmia Consultants / PI: Dr. Felix Sogade / Macon, GA / 5 MINORITY SUBJECTS ENROLLED
YELLOW JERSEY = Overall Enrollment Leader
Rank Institution# of Subjects
Enrolled
1 Research Institute of Circulation Pathology / POKUSHALOV / Novosibirsk, Russia 89
2 Duke University Medical Center / BAHNSON / Durham, NC 76
3 Intermountain Medical Center / BUNCH / Murray, UT 68
4 Mayo Clinic / PACKER / Rochester, MN 53
5 Herzzentrum Leipzig / HINDRICKS / Leipzig, Germany 51
6 Loyola University Medical Center / WILBER / Maywood, IL 20
7 The Heart Hospital Baylor Plano / DEVILLE / Plano, TX 20
8 Providence Saint Vincent Medical Center / HALPERIN / Portland, OR 20
9 University of North Carolina at Chapel Hill / MOUNSEY / Chapel Hill, NC 19
10 Vanderbilt University Medical Center / DARBAR / Nashville, TN 18
GREEN JERSEY = Highest Enrollment Rate
Rank Institution *Rate
1 Research Institute of Circulation Pathology / POKUSHALOV / Novosibirsk, Russia 3.3
2 Duke University Medical Center / BAHNSON / Durham, NC 1.94
3 Intermountain Medical Center / BUNCH / Murray, UT 1.82
4 Herzzentrum Leipzig / HINDRICKS / Leipzig, Germany 1.7
5 Maria Cecilia Hospital / PAPPONE / Cotignola, Italy 1.46
6 Mayo Clinic / PACKER / Rochester, MN 1.31
7 Bakoulev Scientifi c Center for Cardiovascular Surgery / REVISHVILI / Moscow, Russia 1.29
8 Georgia Health Sciences University / BERMAN / Augusta, GA 1.26
9 Policlinico San Donato Center of Clinical Arrhythmia and Electrophysiology / CAPPATO / San Donato Milanese, Italy 1.04
10 Henry Ford Hospital / SCHUGER / Detroit, MI 0.92
*Rate = Monthly Enrollment Rate (since site activation)





























