Embed Size (px)
Citation preview
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
1
2
E. Government-issued photo identification / Texas Driver's License
CONTINUE ON NEXT PAGE
Child Support or Unemployment Benefits: Provide a Payment Detail Summary Sheet (date printed must reflect on or after date of signed application)
Food Stamp / SNAP or TANF: Benefit Letter must be within 30 days of application date. If any other income is listed on the award letter, you MUST submit all documented income separately as indicated above.
Assistance is available for Webb County residents only. For your 2019 Application, steps 1 - 5 listed below must be turned in completed and legible with all required documentations. Contact the Main Office for any questions at (956) 523-4182.
PLEASE INCLUDE COPIES OF THE FOLLOWING:
B. If you receive the following monthly payments, a 2019 award letter is required such as: (Bank Statements and Tax Returns will NOT be accepted.)Most current Social Security (SS) or Supplemental Security Income (SSI)
2019 Application: Pages 1 - 10
3 consecutive pay stubs5 consecutive pay stubs
If you are paid Bi-Weekly or Semi-MonthlyIf you are paid Weekly
If you are paid Monthly If you are paid Twice a Month 2 consecutive pay stubs
1 pay stub
Missing documentation or incomplete applications will result in delayed process or denial of application. ALL DOCUMENTS MUST BE SIGNED.
Income: Must be submitted for ALL household members .
A. If you receive pay stubs, submit the consecutive stubs for the past thirty (30) days from date of signatures on application. See below for income breakdown.
Housing/Section 8 Assistance - Proof of utility reimbursement (if applicable)
A. Applications may be submitted by:
i. Email: [email protected]
ii. Mail/Drop-off: 520 Reynolds, 2nd Floor, Laredo, TX 78040
C. If you are unemployed and not receiving any income, are self-employed, paid in cash, or receiving family support:Complete "Declaration of Income Statement" found on page 6
D. If you are employed, but missing a check stub or employees and employers information is not on check stubs:Complete "Employment Verification" found on page 7
Retirement or Pension VA or VA Disability Benefits Insurance / Workman's Comp / Annuity Payments Child Support or Unemployment Benefits / Food Stamp / SNAP or TANF
Fill out "Voluntary Child Support" form if receiving voluntary child support from child's non-custodial parent.
i of ii Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
1
2
Si se le paga Semanalmente
E. Identificación con foto emitida por el gobierno/licencia de conducir de Texas
CONTINUAR EN LA SIGUIENTE PÁGINA
Beneficios por incapacidad de VAPagos de Seguro/Compensación de Trabajo/Pagos de AnualidadSubsidio de Manutención o Desempleo/Cupones de Alimentos/SNAP o TANFBeneficios de Manutención o Desempleo: Proporcione una hoja de Resumen de detalle de pago (la fecha impresa debe reflejarse en o después de la fecha de la solicitud firmada)Estampilla de comida/SNAP o TANF: la carta de beneficios debe ser dentro de los 30 días de la fecha de la solicitud. Si se enumeran otros ingresos en la carta de adjudicación, deberá presentar todos los ingresos documentados por separado como se indicó anteriormente.
C. Si está desempleado y no recibe ningún ingreso, es autónomo, pagado en efectivo o recibiendo apoyo familiar: Llene "Declaración de Resultados " que se encuentra en la página 6
D. Si usted está empleado, pero falta un talón de cheque o empleados y la información de los empleadores no está en talones de cheque:Complete "Verificación de Empleo " que se encuentra en la página 7
5 talones de cheques de pago consecutivosSi se le paga Quincenal o Semestral 3 talones de cheques de pago consecutivosSi le pagan Dos Veces al Mes
La asistencia solo está disponible para los residentes del Condado de Webb. Para su aplicación 2019, los pasos 1-5 enumerados a continuación deben ser completados y legibles con todas las documentaciones requeridas. Contacte la oficina principal para cualquier pregunta en (956) 523-4182.
POR FAVOR INCLUYA COPIAS DE LO SIGUIENTE:
2019 aplicación: Páginas 1 - 10
Ingresos: Deben presentarse para TODOS los miembros del hogar.
A. Si recibe talones de pago, envíe los talones consecutivos durante los últimos treinta (30) días a partir de la fecha de la firma en la solicitud. Ver abajo para desglose de ingresos.
A. Las solicitudes pueden presentarse por:
i. Email: [email protected]
ii. Correo/Entregar Personalmente: 520 Reynolds, 2º Piso, Laredo, TX 78040
La falta de documentación o aplicaciones incompletas resultará en proceso retrasado o denegación de aplicación. TODOS LOS DOCUMENTOS DEBEN SER FIRMADOS.
Vivienda/Sección 8 Asistencia-Prueba de reembolso de servicios públicos (si corresponde)Jubilación o Pensión
2 talones de cheques de pago consecutivosSi se le paga Mensualmente 1 talone de cheque
B. Si recibe los siguientes pagos mensuales, se requiere una carta de adjudicación de 2019 por ejemplo: (Estados de cuenta bancarios y declaraciones de impuestos no serán aceptados.)Beneficios de Seguro Social más actual (SS) o Ingreso Suplementario de Seguro Social (SSI)
i of ii English on Back Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
3)
4)
Birth Certificate (not a birth certificate card)
U.S. Passport/Passcard
Proof of citizenship or legal residency (ONLY COPIES - NOT RESPONSIBLE FOR ANY ORIGINALS)
If applying for CEAP (light assistance), complete pages 8-10 of application and provide the following information as well as the information found on page "i":
Government-issued photo identification for EVERYONE in the household.
Permanent resident card
Certificate of Naturalization
Certificate of Citizenship
For Children under 16: Clinic, doctor, hospital or school record
For EVERYONE 16 AND OLDER: TX ID or TX Driver's license
DD-214 (if a veteran)
***** NOTE: If you qualify for CEAP, the payment plan will be for the energy provider submitted. Should the client change provider the payment plan will be voided.*****
*****Disconnection Notices are not considered bills*****
Disconnection Notice (if applicable) DOES NOT GUARANTEE ASSISTANCE FOR DISCONNECTION
Billing History
Past 2 bills
Current Electric Bill: Provide complete bill - You must submit a front and back copy of your electric bill showing meter number and service address. If disconnect notice, provide disconnect electric bill and previous bill statement. If any payments made, submit receipts or confirmation number with date of payment, and amount.
5)
ii of ii Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
3)
4)
5)
Certificado de Ciudadanía
***** Nota: Si usted califica para el CEAP, el plan de pago será para el proveedor de energía enviado. Si el cliente cambia de proveedor, el plan de pago será anulado *****
Aviso de desconexión (si corresponde) NO GARANTIZA LA ASISTENCIA PARA LA DESCONECION
Historial de Facturación
Últimas 2 facturas
*****Los avisos de desconexión no se consideran facturas *****
Factura eléctrica actual: Proporcione una factura completa-debe presentar una copia de su factura de electricidad que muestre el número de medidor y la dirección de servicio. Si el aviso de desconexión, proporcione la factura eléctrica de desconexión y la declaración de factura anterior. Si se hiso un pago, enviar recibos o número de confirmación con la fecha de pago, y el monto.
Si solicita el CEAP (asistencia de electricidad), complete las paginas de 8 - 10 de la aplicación y proporcione la siguiente información, así como la información en pagina "i":
Identificación con foto emitida por el gobierno para todos en el hogar.
Para niños menores de 16 años: expediente clínico, médico, hospitalario o escolar
Para todos los mayores de 16 años: TX ID o TX licencia de conducir
DD-214 (si un veterano)
Comprobante de ciudadanía o residencia legal (SOLO COPIAS - NO SOMOS RESPONSIBLES POR NINGUN DOCUMENTO ORIGINAL)
Acta de Nacimiento (no una tarjeta de certificado de nacimiento)
Pasaporte/passcard de los E.E.U.U.
Certificado de Naturalización
Tarjeta de residente permanente
ii of ii English on Back Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
2)
3)
5)
6)
i)
1)
3)
Provide truthful statements regarding financial, social or personal data. Fraud is a reason for denial or termination of services. Clients may be required to repay any benefits received as a result of providing untrue information. All information is subject to verification with employers and/or landlords among others;
Report any change in utility provider, change of address or account number when receiving utility assistance;
Applicants have a responsibility to:
2)
7)
Cooperate in deciding and implementing the plan of action. It represents what the applicant is expected to do to help themself;
Provide required information to verify eligibility for assistance whenever the case is opened or reopened;
8)Treat agency staff with respect: abusive language, threats, violent acts, use of alcohol, drugs or other intoxicants will not be tolerated. Violators will be asked to leave; police/security will be called if applicant refuses to leave. Repeat offenses may lead to denial of assistance for a period of time.
Payment Plan can not exceed the maximum qualified amount. However, WCCAA will only commit to the amount stipulated on active payment plan to the client. Funds will be distributed upon availability. Any charges not covered by the program MUST be paid for by me (the participant) in order to prevent disconnections of electrical services. Should additional charges arise after the review of my documentation, I will be informed.
Date Case Number (OFFICE USE)
Client's Signature Printed Name
APPLICANT RIGHTS AND RESPONSIBILITIES
1)
4)
As a participant, I do hereby give permission to obtain and release personal information regarding my case to Webb County Community Action Agency (WCCAA) as deemed necessary to further assist my household in accessing services and funding sources for reporting purposes. Information requested or released may include, but is not limited to, the following: 1) Services provided to or requested from the household by agency and other agencies of Webb County Community Action Agency; 2) Status on utility accounts, payment and consumption histories, 3) Proof of income, residency and household members; 4) Employment and 5)Education.
Applicants have a right to:
Confidentiality of information obtained during the application process. To facilitate coordination of services, communication with other agencies, utility providers, apartment complexes, etc. will not be considered a breach of confidentiality. Information provided on the application forms or during the application process are subject to verification after the applicant voluntarily signs a Release of Information form;
A clear explanation of services offered by CAA and eligibility criteria for those services;
Courteous Service and have the request completed in a timely manner;
Apply for assistance from Community Action Agency (CAA) if they live in Webb County and funding is available for the assistance they request;
See "Appeals Process".
Review/Appeal decisions made regarding their application.
Refuse services;
If approved for CEAP, I am aware the payment will take up to 45 business days from the day of the pledge. I am also aware that I am responsible for any and all charges that might arise.
6)
5)
4)
WCCAA Page 1 of 10 Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
2)
3)
5)
6)
i)
8)
Nombre Impreso Firma del Cliente
Fecha Numero de Caso (USO DE OFICINA)
Proporcionar la información requerida para verificar la elegibilidad para asistencia siempre que el caso sea abierto o reabierto;
Proporcionar declaraciones veraces sobre los datos financieros, sociales o personales. El fraude es una razón para la negación o terminación de los servicios. Se puede requerir a los clientes que paguen cualquier beneficio recibido como resultado de proporcionar información falsa. Toda la información está sujeta a verificación con los empleadores y/o los propietarios, entre otros;
Tratar al personal de la agencia con respeto: el lenguaje abusivo, las amenazas, los actos violentos, el uso de alcohol, drogas u otros intoxicantes no serán tolerados. Se pedirá a los infractores que se marchen; la policía/seguridad será llamada si el solicitante se niega a irse. Las ofensas repetidas pueden llevar a la denegación de asistencia por un período de tiempo.
4)El Plan de Pago no puede exceder el monto máximo calificado. Sin embargo, WCCAA sólo se compromete a la cantidad estipulada en el plan de pago activo para el cliente. Los fondos se distribuirán según disponibilidad.
5)Cualquier cargo no cubierto por el programa DEBE ser pagado por yo (el participante) con el fin de evitar desconexiones de los servicios eléctricos. Si se presentan cargos adicionales después de la revisión de mi documentación, estaré informado.
6)Si se aprueba para el CEAP, soy consciente de que el pago tardará hasta 45 días hábiles desde el día de la promesa. También soy consciente de que soy responsable de todos los cargos que pudieran surgir.
1)
3)
7)
Una explicación clara de los servicios ofrecidos por la CAA y los criterios de elegibilidad para dichos servicios;
Los solicitantes tienen la responsabilidad de:
2)Cooperar en la decisión y aplicación del plan de acción. Representa lo que se espera que haga el solicitante para ayudarse a sí mismo;
Notificar cualquier cambio en el proveedor de servicios públicos, cambio de dirección o número de cuenta al recibir asistencia de servicios públicos;
4)
Véase "Proceso de Apelaciones ".
Decisiones de revisión/apelación tomadas con respecto a su aplicación
Servicios de Rechazo;
Confidencialidad de la información obtenida durante el proceso de solicitud. Para facilitar la coordinación de los servicios, la comunicación con otras agencias, proveedores, complejos de apartamentos, etc. no se considerará una violación de la confidencialidad. La información proporcionada en los formularios de solicitud o durante el proceso de solicitud está sujeta a verificación después de que el solicitante firme voluntariamente un formulario de Divulgación de Información;
DERECHOS Y RESPONSABILIDADES DEL SOLICITANTE
Como participante, por la presente doy permiso para obtener y divulgar información personal con respecto a mi caso al servicio a Agencia de Acción Comunitaria del Condado de Webb (WCCAA) según se considere necesario para ayudar más a mi hogar en el acceso a servicios y fuentes de financiamiento para informar propósitos. La información solicitada o liberada puede incluir, pero no se limita a, los siguientes: 1) Los servicios prestados o solicitados por la Agencia y otras agencias de la Agencia de acción comunitaria del Condado de Webb; 2) Estado en cuentas de utilidad, historial de pago y consumo; 3) Prueba de ingresos, residencia y miembros del hogar; 4) Empleo y 5) Educación.
Los solicitantes tienen derecho a:
1)
Servicio cortés y que sus solicitud sea completado en la brevedad posible;
Solicitar ayuda de los Agencia de Elección a la Comunidad (CAA) si viven en el Condado de Webb siempre y cuando los fondos estén disponibles para la asistencia que solicita;
WCCAA Página 1 de 10 English on Back Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
Retirement SystemsUtility Providers
Medical & Child Care
The groups or individuals that may be asked to release the above information include, but are not limited to:
GROUPS OR INDIVIDUALS THAT MAY BE ASKED
INFORMATION COVERED
RELEASE AND CONSENT FORM
companies in the categories listed below to release information regarding employment, income and/or assets for purposes of verifying information on my/our application for participation in a Webb County Community Action Agency program. I/we authorize release of information without liability to the administrator/ owner/management listed above, and/or Webb County Community Action Agency and/or the Department’s service provider.
the undersigned hereby authorize all persons or
I/We understand that previous or current information regarding me/us may be needed. Verifications and inquires that may be requested include, but are not limited to: personal identity, student status, employment, income, assets, and medical or child care allowances. I/We understand that this authorization cannot be used to obtain information about me/us that is not pertinent to my eligibility for and continued participation in a Webb County Community Action Agency.
Social Security Administration State Unemployment Agencies
SignatureAdult Member Printed Name
SignatureAdult Member Printed Name
Public Housing Agencies
II. APPLICANT CERTIFICATION
I/We agree that a photocopy of this authorization may be used for the purposes stated above. The original of this authorization is on file and will stay in effect for a year and one month from the date signed. I/We understand I/We have a right to review this file and correct any information that is incorrect.
Veterans AdministrationsEducational Institutions
Date
SignatureAdult Member Printed Name Date
NOTE: ALL HOUSEHOLD MEMBERS 18 AND OLDER MUST SIGN.THIS GENERAL CONSENT MAY NOT BE USED TO REQUEST A COPY OF A TAX RETURN.
I. THIS SECTION TO BE COMPLETED BY APPLICANT
Welfare Agencies Support and Alimony ProvidersPast and Present Employers
Applicant/Resident Name:
I/We
Date
SignatureApplicant Printed Name Date
WCCAA Página 2 de 10 Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
Agencias de Bienestar
Nombre Impreso del Miembro Adulto Firma Fecha
Solicitante/nombre del residente:
Yo/Nosotros
Los grupos o individuos que pueden ser pedido para divulgar la información antedicha incluyen, pero no se limitan a:
Nombre Impreso del Miembro Adulto Firma Fecha
Nombre Impreso del Miembro Adulto Firma Fecha
Nombre Impreso del Solicitante Firma Fecha
Administraciones de Veteranos Proveedores de Servicios Públicos Agencias de Vivienda Pública Sistemas de Jubilación
II. CERTIFICACIÓN DEL SOLICITANTE
Yo/nosotros acordamos que una fotocopia de esta autorización puede ser utilizada para los propósitos indicados anteriormente. El original de esta autorización está en archivo y seguirá vigente durante un año y un mes a partir de la fecha de la firma. Yo/nosotros entendemos que tenemos derecho a revisar este archivo y corregir cualquier información que sea incorrecta.
NOTA: TODOS LOS MIEMBROS DEL HOGAR 18 Y MAYORES DEBEN FIRMAR. ESTE CONSENTIMIENTO GENERAL NO SE PUEDE UTILIZAR PARA
SOLICITAR UNA COPIA DE UNA DECLARACIÓN DE IMPUESTOS.
Reconocimiento del Cliente y Divulgación de Información
I. ESTA SECCIÓN SERÁ COMPLETADA POR EL SOLICITANTE
el abajo firmante autoriza a todas las personas o empresas en las categorías enumeradas a continuación para divulgar información sobre el empleo, los ingresos y/o los activos con el fin de verificar la información en mi/nuestra solicitud de participación en un programa de la Agencia de acción comunitaria del Condado de Webb. Yo/nosotros autorizamos la divulgación de información sin responsabilidad al Administrador/Propietario/Gerente mencionado anteriormente, y/o la Agencia de acción comunitaria del Condado de Webb y/o el proveedor de servicios del Departamento.
INFORMACIÓN CUBIERTA
Yo/nosotros entendemos que la información anterior o actual con respecto a mí/nosotros puede ser necesaria. Las verificaciones y consultas que se pueden solicitar incluyen, pero no se limitan a: identidad personal, estatus estudiantil, empleo, ingresos, activos, y subsidios médicos o de cuidado infantil. Entiendo que esta autorización no puede ser utilizada para obtener información sobre mí/nosotros que no es pertinente a mi elegibilidad y participación continuada en una agencia de acción comunitaria del Condado de Webb.
GRUPOS O INDIVIDUOS A LOS QUE SE PUEDE PEDIR
Empleadores Pasados y Presentes Médicos y ProveedoresProveedores de Apoyo y Pensión Agencias Estatales de Desempleo Instituciones Educativas Administración del Seguro Social
WCCAA Página 2 de 10 English on Back Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
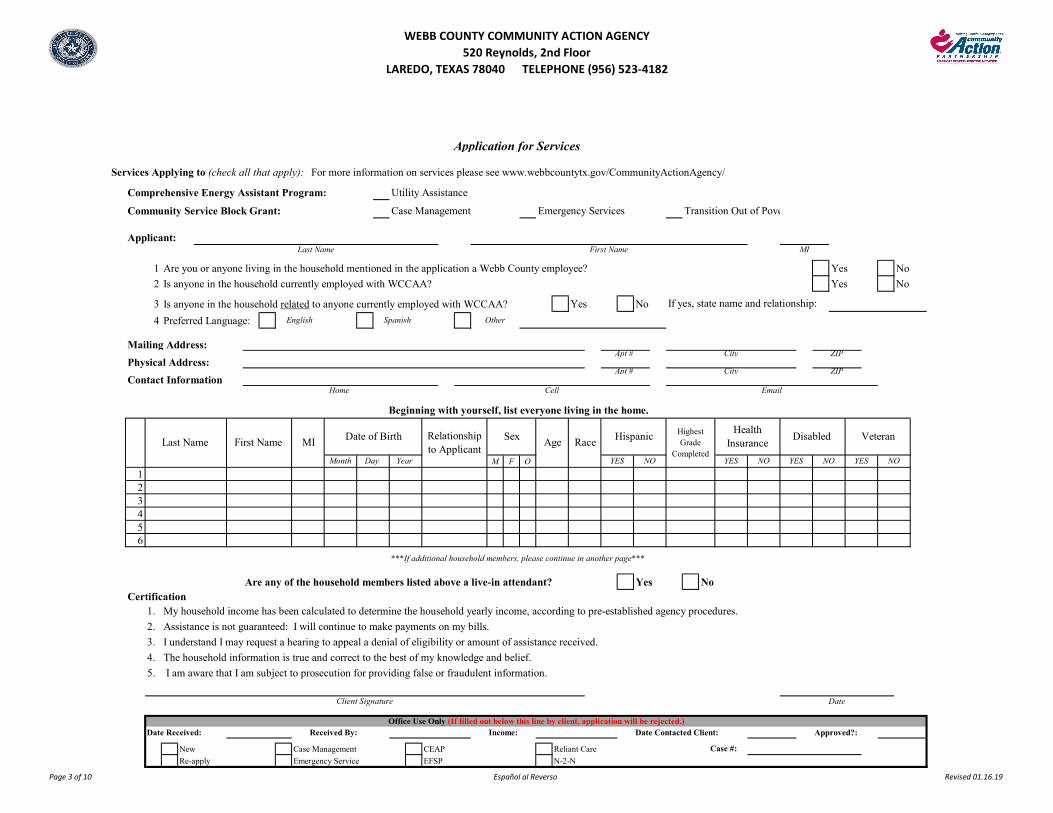
1 Are you or anyone living in the household mentioned in the application a Webb County employee? Yes No
2 Is anyone in the household currently employed with WCCAA? Yes No
3 Is anyone in the household related to anyone currently employed with WCCAA? Yes No
4 Preferred Language:
M F O
123456
Are any of the household members listed above a live-in attendant? Yes NoCertification
1. My household income has been calculated to determine the household yearly income, according to pre-established agency procedures.
2. Assistance is not guaranteed: I will continue to make payments on my bills.
3. I understand I may request a hearing to appeal a denial of eligibility or amount of assistance received.
4. The household information is true and correct to the best of my knowledge and belief.
5. I am aware that I am subject to prosecution for providing false or fraudulent information.
Date Received: Received By: Income: Date Contacted Client: Approved?:
New Case Management CEAP Reliant Care
Re-apply Emergency Service EFSP N-2-N
Contact Information
Physical Address:
Mailing Address:Apt # City ZIP
Apt # City ZIP
***If additional household members, please continue in another page***
Office Use Only (If filled out below this line by client, application will be rejected.)
Case #:
Client Signature Date
Highest Grade
Completed
Health Insurance
NO YES NO
Home Cell Email
Beginning with yourself, list everyone living in the home.
Last Name First Name MIDate of Birth Relationship
to Applicant Disabled Veteran
Month Day Year YES NO YES NO YES
SexAge Race
Hispanic
Case Management Emergency Services Transition Out of Poverty (T.O.P.) Program
Comprehensive Energy Assistant Program: Utility Assistance
Services Applying to (check all that apply): For more information on services please see www.webbcountytx.gov/CommunityActionAgency/
Community Service Block Grant:
Application for Services
Applicant:Last Name First Name MI
English Spanish Other
If yes, state name and relationship:
Page 3 of 10 Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
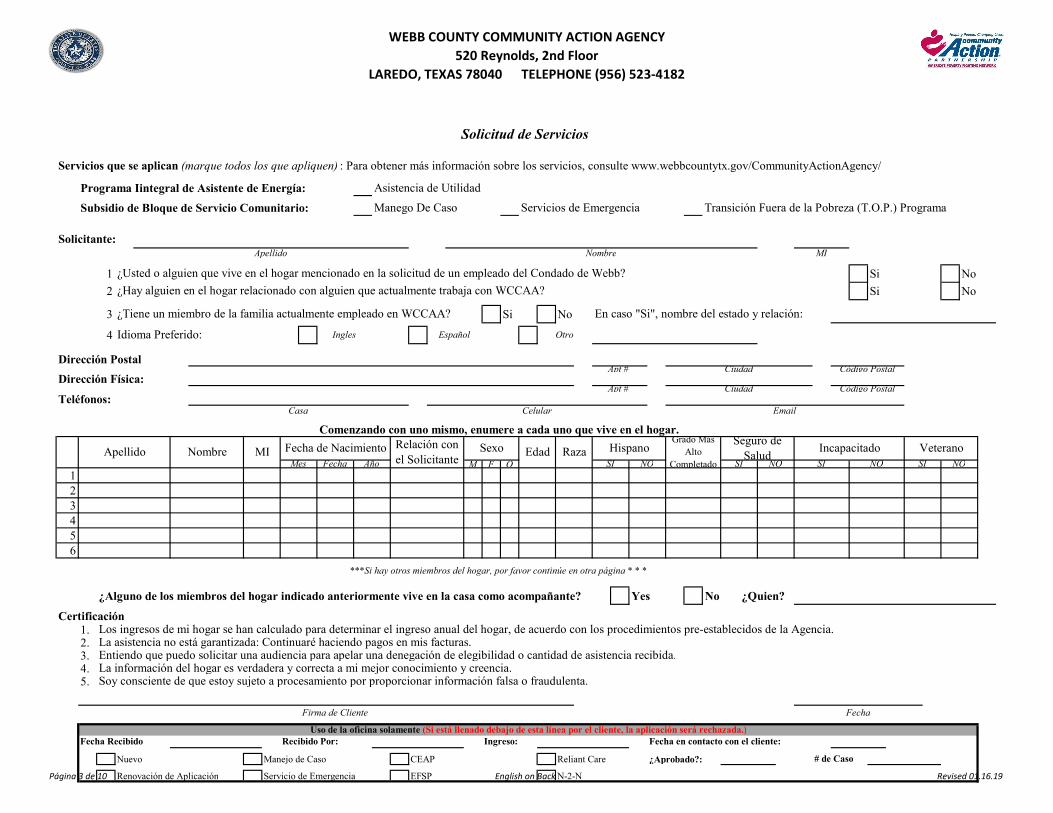
1 Si No
2 Si No
3 Si No
4
Teléfonos:
M F O123456
¿Alguno de los miembros del hogar indicado anteriormente vive en la casa como acompañante? Yes No ¿Quien?
1.2.3.4.5.
Nuevo Manejo de Caso CEAP Reliant Care ¿Aprobado?:
Renovación de Aplicación Servicio de Emergencia EFSP N-2-N
¿Tiene un miembro de la familia actualmente empleado en WCCAA? En caso "Si", nombre del estado y relación:
Servicios que se aplican (marque todos los que apliquen) : Para obtener más información sobre los servicios, consulte www.webbcountytx.gov/CommunityActionAgency/
Programa Iintegral de Asistente de Energía:
Manego De Caso
Asistencia de Utilidad
Subsidio de Bloque de Servicio Comunitario: Transición Fuera de la Pobreza (T.O.P.) ProgramaServicios de Emergencia
¿Usted o alguien que vive en el hogar mencionado en la solicitud de un empleado del Condado de Webb?
¿Hay alguien en el hogar relacionado con alguien que actualmente trabaja con WCCAA?
Solicitud de Servicios
La información del hogar es verdadera y correcta a mi mejor conocimiento y creencia.Soy consciente de que estoy sujeto a procesamiento por proporcionar información falsa o fraudulenta.
Firma de Cliente Fecha
Fecha Recibido Recibido Por: Ingreso:
Idioma Preferido:
Solicitante:Apellido
NOSI
Nombre MI
Apt # Ciudad
CiudadApt #
# de Caso
Fecha en contacto con el cliente:
Dirección Física:Código Postal
Código Postal
CertificaciónLos ingresos de mi hogar se han calculado para determinar el ingreso anual del hogar, de acuerdo con los procedimientos pre-establecidos de la Agencia.
Entiendo que puedo solicitar una audiencia para apelar una denegación de elegibilidad o cantidad de asistencia recibida.La asistencia no está garantizada: Continuaré haciendo pagos en mis facturas.
Dirección Postal
Ingles Español Otro
VeteranoRelación con el Solicitante
Seguro de Salud
Grado Más Alto
Completado RazaEdadSexo Incapacitado
SI NOSI NO
HispanoFecha Año
Fecha de NacimientoMINombreApellidoMes
Uso de la oficina solamente (Si está llenado debajo de esta línea por el cliente, la aplicación será rechazada.)
***Si hay otros miembros del hogar, por favor continúe en otra página * * *
CelularCasa
Comenzando con uno mismo, enumere a cada uno que vive en el hogar.
SI NO
Página 3 de 10 English on Back Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
1. H
ouse
hol
d T
ype
2. H
ousi
ng
Typ
e
3. R
esid
enti
al T
ype
Rec
eive
Foo
d S
tam
ps
Far
mer
Sea
sona
l /
Mig
rant
Far
mer
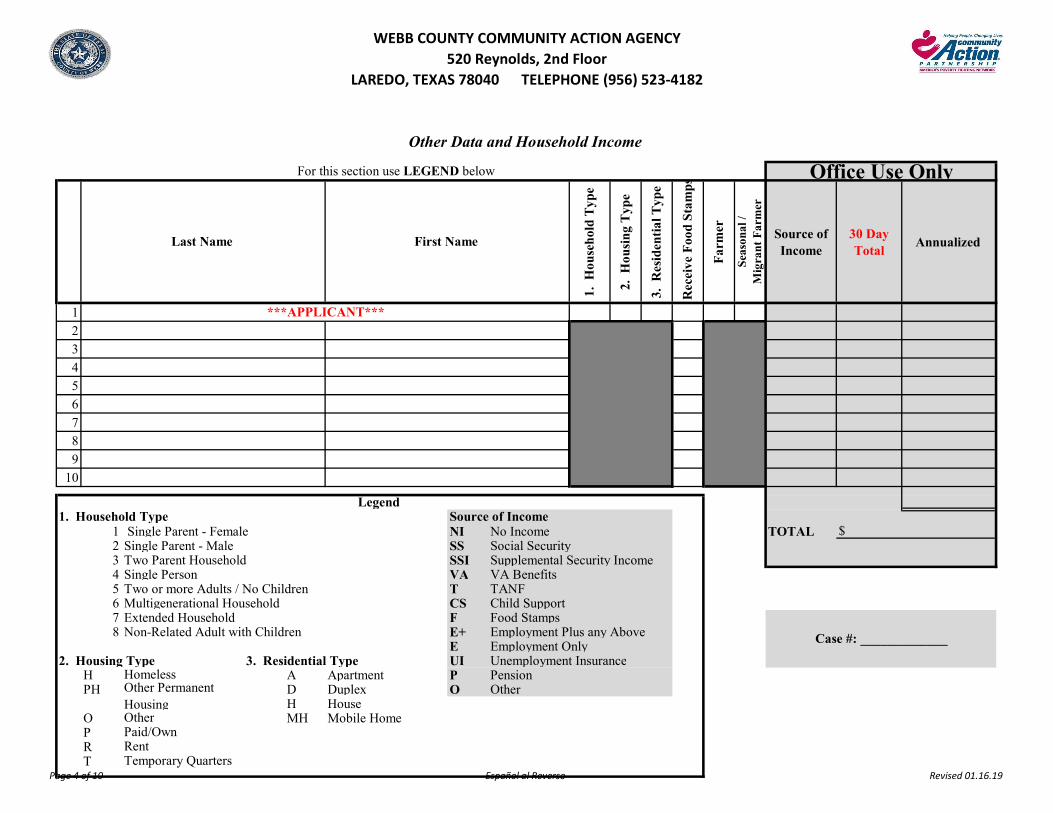
Source of Income
30 Day Total
Annualized
123456789
10
1 Single Parent - Female NI No Income TOTAL2 Single Parent - Male SS Social Security 3 Two Parent Household SSI Supplemental Security Income 4 Single Person VA VA Benefits 5 Two or more Adults / No Children T TANF6 Multigenerational Household CS Child Support 7 Extended Household F Food Stamps 8 Non-Related Adult with Children E+ Employment Plus any Above
E Employment Only 2. Housing Type 3. Residential Type UI Unemployment Insurance
H A Apartment P Pension PH D Duplex O Other
H HouseO MH Mobile Home PRT
Homeless
Temporary QuartersRentPaid/OwnOther
Other Permanent Housing
Other Data and Household Income
Case #: _____________
1. Household Type Source of Income $
Legend
Office Use Only
First Name Last Name
For this section use LEGEND below
***APPLICANT***
Page 4 of 10 Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
1. T
ipo
de H
ogar
2. T
ipo
de V
ivie
nda
3. T
ipo
Res
iden
cial
Rec
ibir
Cup
ones
d
e A
lim
ento
s
Gra
njer
o
Agr
icu
ltor
E
stac
ion
al/M
igra
nte
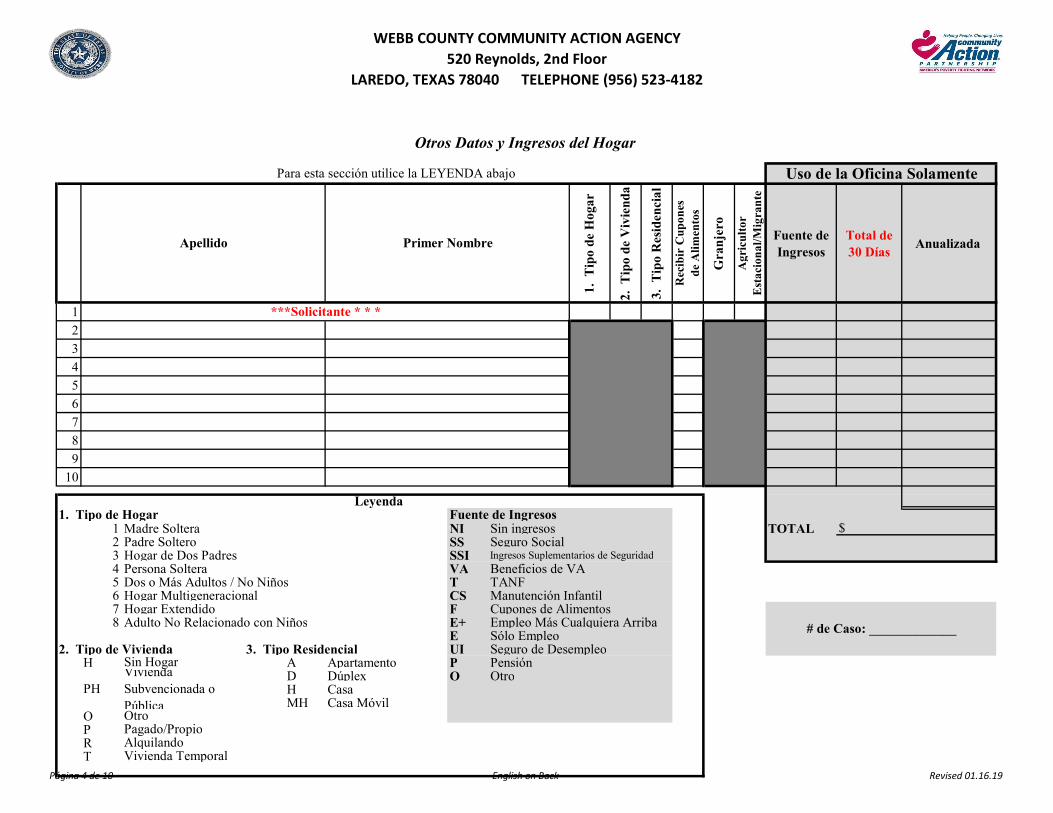
Fuente de Ingresos
Total de 30 Días
Anualizada
123456789
10
1 Madre Soltera NI Sin ingresos TOTAL2 Padre Soltero SS Seguro Social3 Hogar de Dos Padres SSI Ingresos Suplementarios de Seguridad4 Persona Soltera VA Beneficios de VA5 Dos o Más Adultos / No Niños T TANF6 Hogar Multigeneracional CS Manutención Infantil 7 Hogar Extendido F Cupones de Alimentos 8 Adulto No Relacionado con Niños E+ Empleo Más Cualquiera Arriba
E Sólo Empleo 2. Tipo de Vivienda 3. Tipo Residencial UI Seguro de Desempleo
H A Apartamento P Pensión D Dúplex O OtroH CasaMH Casa Móvil
OPRT Vivienda Temporal
PH
Sin Hogar
OtroPagado/PropioAlquilando
Vivienda Subvencionada o Pública
$
# de Caso: _____________
Leyenda 1. Tipo de Hogar Fuente de Ingresos
***Solicitante * * *
Otros Datos y Ingresos del Hogar
Para esta sección utilice la LEYENDA abajo Uso de la Oficina Solamente
Apellido Primer Nombre
Página 4 de 10 English on Back Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
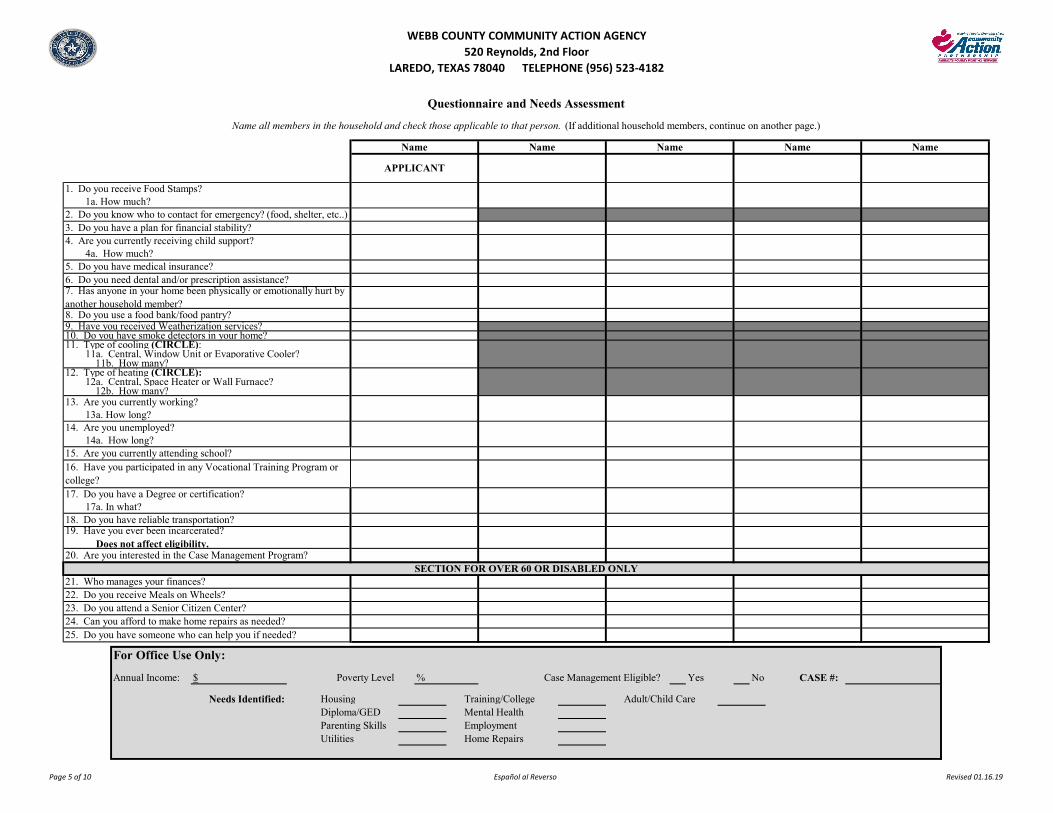
For Office Use Only:
Annual Income: $ Poverty Level % Case Management Eligible? Yes No CASE #:
Needs Identified: Housing Training/College Adult/Child Care Diploma/GED Mental Health Parenting Skills Employment Utilities Home Repairs
16. Have you participated in any Vocational Training Program or college?
APPLICANT
Questionnaire and Needs Assessment
Name all members in the household and check those applicable to that person. (If additional household members, continue on another page.)
SECTION FOR OVER 60 OR DISABLED ONLY
Name Name Name Name Name
12. Type of heating (CIRCLE): 12a. Central, Space Heater or Wall Furnace?
12b. How many?13. Are you currently working?
13a. How long?14. Are you unemployed?
8. Do you use a food bank/food pantry? 9. Have you received Weatherization services?10. Do you have smoke detectors in your home? 11. Type of cooling (CIRCLE):
11a. Central, Window Unit or Evaporative Cooler?11b. How many?
3. Do you have a plan for financial stability?4. Are you currently receiving child support?
4a. How much?5. Do you have medical insurance? 6. Do you need dental and/or prescription assistance?7. Has anyone in your home been physically or emotionally hurt by another household member?
1. Do you receive Food Stamps?1a. How much?
2. Do you know who to contact for emergency? (food, shelter, etc..)
24. Can you afford to make home repairs as needed?25. Do you have someone who can help you if needed?
19. Have you ever been incarcerated? Does not affect eligibility.20. Are you interested in the Case Management Program?
21. Who manages your finances?22. Do you receive Meals on Wheels? 23. Do you attend a Senior Citizen Center?
14a. How long?15. Are you currently attending school?
17. Do you have a Degree or certification?17a. In what?
18. Do you have reliable transportation?
Page 5 of 10 Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
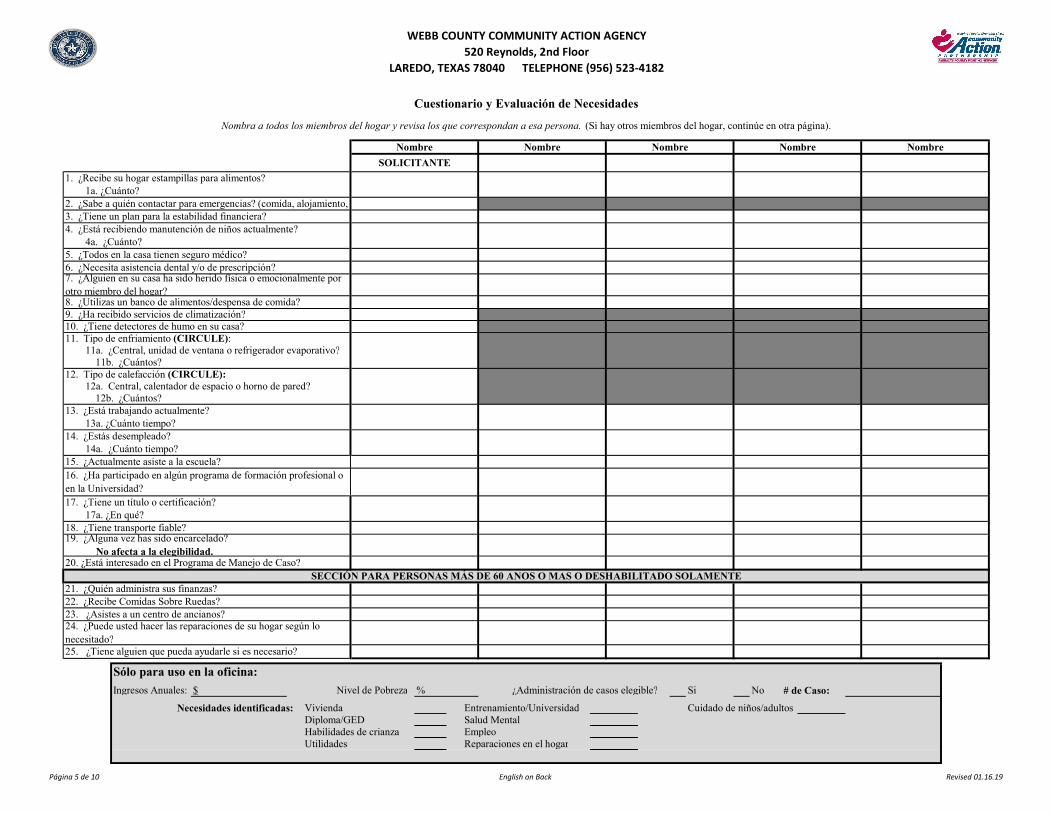
Sólo para uso en la oficina:
Ingresos Anuales: $ Nivel de Pobreza % ¿Administración de casos elegible? Si No # de Caso:
Necesidades identificadas: Vivienda Entrenamiento/Universidad Cuidado de niños/adultosDiploma/GED Salud Mental Habilidades de crianza EmpleoUtilidades Reparaciones en el hogar
23. ¿Asistes a un centro de ancianos?22. ¿Recibe Comidas Sobre Ruedas?
25. ¿Tiene alguien que pueda ayudarle si es necesario?
24. ¿Puede usted hacer las reparaciones de su hogar según lo necesitado?
SECCIÓN PARA PERSONAS MÁS DE 60 ANOS O MAS O DESHABILITADO SOLAMENTE21. ¿Quién administra sus finanzas?
20. ¿Está interesado en el Programa de Manejo de Caso?
19. ¿Alguna vez has sido encarcelado? No afecta a la elegibilidad.
18. ¿Tiene transporte fiable?
17. ¿Tiene un título o certificación?17a. ¿En qué?
16. ¿Ha participado en algún programa de formación profesional o en la Universidad?
15. ¿Actualmente asiste a la escuela?
14. ¿Estás desempleado?14a. ¿Cuánto tiempo?
13. ¿Está trabajando actualmente?13a. ¿Cuánto tiempo?
12. Tipo de calefacción (CIRCULE): 12a. Central, calentador de espacio o horno de pared?
12b. ¿Cuántos?
11. Tipo de enfriamiento (CIRCULE):11a. ¿Central, unidad de ventana o refrigerador evaporativo?
11b. ¿Cuántos?
10. ¿Tiene detectores de humo en su casa? 9. ¿Ha recibido servicios de climatización?8. ¿Utilizas un banco de alimentos/despensa de comida?
7. ¿Alguien en su casa ha sido herido física o emocionalmente por otro miembro del hogar?
6. ¿Necesita asistencia dental y/o de prescripción?5. ¿Todos en la casa tienen seguro médico?
4. ¿Está recibiendo manutención de niños actualmente? 4a. ¿Cuánto?
3. ¿Tiene un plan para la estabilidad financiera?2. ¿Sabe a quién contactar para emergencias? (comida, alojamiento,
Cuestionario y Evaluación de Necesidades
Nombra a todos los miembros del hogar y revisa los que correspondan a esa persona. (Si hay otros miembros del hogar, continúe en otra página).
Nombre Nombre Nombre Nombre Nombre
1a. ¿Cuánto?
SOLICITANTE
1. ¿Recibe su hogar estampillas para alimentos?
Página 5 de 10 English on Back Revised 01.16.19
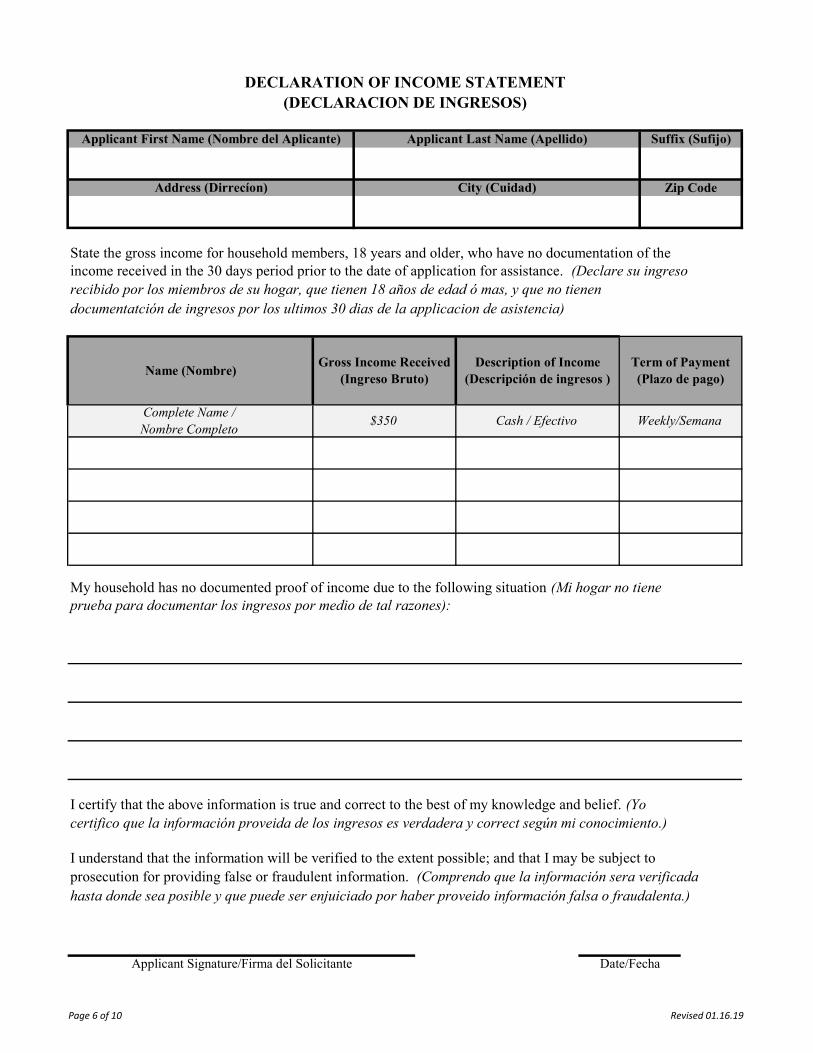
DECLARATION OF INCOME STATEMENT(DECLARACION DE INGRESOS)
Applicant First Name (Nombre del Aplicante) Suffix (Sufijo)Applicant Last Name (Apellido)
Address (Dirrecíon) City (Cuidad) Zip Code
Complete Name / Nombre Completo
Cash / Efectivo$350
State the gross income for household members, 18 years and older, who have no documentation of the
documentatción de ingresos por los ultimos 30 dias de la applicacion de asistencia)recibido por los miembros de su hogar, que tienen 18 años de edad ó mas, y que no tienenincome received in the 30 days period prior to the date of application for assistance. (Declare su ingreso
Name (Nombre)Description of Income
(Descripción de ingresos )Gross Income Received
(Ingreso Bruto)
Date/FechaApplicant Signature/Firma del Solicitante
certifico que la información proveida de los ingresos es verdadera y correct según mi conocimiento.)
I understand that the information will be verified to the extent possible; and that I may be subject toprosecution for providing false or fraudulent information. (Comprendo que la información sera verificadahasta donde sea posible y que puede ser enjuiciado por haber proveido información falsa o fraudalenta.)
I certify that the above information is true and correct to the best of my knowledge and belief. (Yo
prueba para documentar los ingresos por medio de tal razones):My household has no documented proof of income due to the following situation (Mi hogar no tiene
Weekly/Semana
Term of Payment(Plazo de pago)
Page 6 of 10 Revised 01.16.19
THIS PAGE
INTENTIONALLY
LEFT BLANK /
ESTA PÁGINA SE DEJÓ
INTENCIONALMENTE
EN BLANCO
Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
*****AGENCY WILL CONTACT EMPLOYER TO VERIFY EMPLOYMENT/AGENCIA CONTACTARÁ CON EL EMPLEADOR PARA VERIFICAR EL EMPLEO *****
Company Name, & Address
Employer's Signature Employer's Printed Name Date
Phone Number Fax Number E-Mail
Additional remarks:
Other Pay (Tips, bonus, commissions)
If the employee's work is seasonal or occasional, please indicate the layoff period(s):
# of HoursGross Pay
Date Pay Period Ended
Date Employed Received Paycheck
Date of First Employed: Last Day of Employment:
On the chart below, list wages received by this employee 30 days prior to signature of application
EMPLOYMENT VERIFICATION
EMPLOYEE NAME: Job Title:
Yes NoPresently Employed?
THIS SECTION TO BE COMPLETED BY EMPLOYER IF MISSING CHECK STUBS OR NO EMPLOYER/EMPLOYEE INFORMATION ON CHECK STUBS / ESTA SECCIÓN SERÁ COMPLETADA
POR EL EMPLEADOR SI FALTA TALONES DE CHEQUES O NO HAY INFORMACIÓN DEL EMPLEADOR/EMPLEADO EN TALONES DE CHEQUES
WCCAA Page 7 of 10 Revised 01.16.19
THIS PAGE
INTENTIONALLY
LEFT BLANK /
ESTA PÁGINA SE DEJÓ
INTENCIONALMENTE
EN BLANCO
Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
4
6
5
2
3
1
Amount of Child Support
Date of BirthFrequency (Weekly,
monthly, yearly)Name of Child(ren)
VOLUNTARY CHILD SUPPORT AGREEMENT
Signature of Client
I hereby certify that the above statements are true and correct to the best of my knowledge. I understand that a false statement may disqualify me for benefits. I am aware that I am subject to prosecution for
providing false, fraudulent or purposely omitting information for qualifying purposes.
I acknowledge that the children below are receiving the following in lieu of child support:
Phone Number of Non-Custodial Parent:
Name of Non-Custodial Parent:
Address of Non-Custodial Parent:
City/State of Non-Custodial Parent:
Date:Client Name:
Name of Custodial Parent (If different from Client Name:)
Page 8 of 10 Español al Reverso Revised 01.16.19
WEBB COUNTY COMMUNITY ACTION AGENCY520 Reynolds, 2nd Floor
LAREDO, TEXAS 78040 TELEPHONE (956) 523-4182
Por la presente certifico que las declaraciones anteriores son verdaderas y correctas a conocimiento. Entiendo que una declaración falsa puede descalificarme a los beneficios. Soy consciente de que
estoy sujeto a juicio por proporcionar falsa, fraudulenta o deliberadamente omitir información para fines de clasificación.
Reconozco que los niños a continuación están recibiendo lo siguiente en lugar de manutención de los hijos:
Monto de Manutención
Nombre del Niño (s)
Firma del Cliente
Nombre del Cliente: Fecha:
Nombre del Padre Custodial (si es diferente del nombre del cliente:)
Número de Teléfono del Padre No-Custodial:
5
6
3
4
1
2
ACUERDO VOLUNTARIO DE MANUTENCIÓN INFANTIL
Fecha de Nacimiento
Frecuencia (Semanal, mensual, anual)
Nombre del Padre No-Custodial:
Dirección del Padre No-Custodial:
Ciudad/Estado del Padre No-Custodial:
Page 8 of 10 English on Back Revised 01.16.19
To add additional household members, use another copy of this form.
Applicant's Signature Date
See Form Instructions for section details
I AM AWARE THAT I AM SUBJECT TO PROSECUTION FOR PROVIDING FALSE OR FRAUDULANT INFORMATION.
TEXAS DEPARTMENT OF HOUSING AND COMMUNITY AFFAIRS
Systematic Alien Verification for Entitlements (SAVE) SystemApplicant Certification Form for WAP and CEAP
The program for which you are applying requires verification that you are a U.S. citizen, a non-citizen national, or a legal resident of the United States. Documentation of your status is required. This agency uses the Systematic
Alien Verification for Entitlements (SAVE) System to verify the status of non-citizens.
Household MemberUS Citizen (Born or Naturalized)
or U.S. NationalQualified Alien Documentation Provided
Page 9of 10 Español al Reverso
Para agregar miembros adicionales del hogar, utilice otra copia de este formulario.
SOY CONSCIENTE DE QUE ESTOY SUJETA A ENJUICIAMIENTO POR PROPORCIONAR INFORMACIÓN FALSA O FRAUDULENTA.
Firma del Solicitante Fecha
Consulte las instrucciones del formulario para detalles de la sección
DEPARTAMENTO DE VIVIENDA Y ASUNTOS COMUNITARIOS DE TEXAS
Sistema de verificación sistemática de extranjería para derechos (SAVE)Formulario de Certificación del Solicitante para WAP y CEAP
El programa para el cual usted está aplicando requiere la verificación que usted es un ciudadano de los E.E.U.U., un nacional del no-ciudadano, o un residente legal de los Estados Unidos. Se requiere documentación de su estado. Esta agencia utiliza el
sistema de verificación sistemática de Extranjería (SAVE) para verificar el estatus de los no ciudadanos.
Miembro del HogarCiudadano Estadounidense (Nacido o Naturalizado) o
Extranjero Calificado Documentación Proporcionada
Página 9 de 10 English on Back
SAVE Certification Form Instructions
Household members who answer "no" to the "US Citizen (Born or Naturalized) or U.S. National" or "Qualified Alien" box or who cannot provide supporting documentation are considered ineligible for CEAP and WAP.
The SAVE Certification Form is not valid without applicant signature
Documentation Provided - List out documentation collected for each member of the household supporting their selected status
Qualified Alien - All household members answering YES to this question must provide documentation to be verified through SAVE. Reference SAVE tutorials and guides for information on acceptable documents to use.
For Household members who select yes to this question with valid supporting documentation, no SAVE verification is required.
Persons born in Puerto Rico, Guam, the US Virgin Islands, American Samoa, Swains Island (or their descendants) are considered citizens.
US Citizen (Born or Naturalized) or U.S. National - Must provide acceptable primary or secondary forms of documentation. Reference the SAVE webinar on the TDHCA website for details on acceptable documentation.
Household Member - All members of the household listed on the application must be accounted for.
Page 10 of 10 Español al Reverso
Las personas nacidas en Puerto Rico, Guam, las Islas Vírgenes de los Estados Unidos, Samoa Americana, Swains Island (o sus descendientes) son consideradas ciudadanas.
Ciudadano de los E.E.U.U. (Llevado o Naturalizado) o Nacional de los E.E.U.U. - Debe proporcionar las formas primarias o secundarias aceptables de la documentación. Haga referencia al webinar de SAVE en el sitio web de TDHCA para obtener más información sobre la documentación aceptable.
Miembro del Hogar - Todos los miembros del hogar enumerados en la solicitud deben ser contabilizados.
Instrucciones para la Certificación de SAVE
Los miembros del hogar que responden "NO " a la "Ciudadano de los EE. UU. (Nacido o Naturalizado) o U.S. nacional " o "Extranjero Calificado " caja o que no pueden proporcionar documentación de apoyo se consideran inelegibles para CEAP y WAP.
El formulario de certificación SAVE no es válido sin la firma del solicitante
Documentación proporcionada - Enumere la documentación entregada para cada miembro del hogar que apoya su estatus seleccionado.
Extranjero calificado - Todos los miembros del hogar que respondan SI a esta pregunta deben proporcionar la documentación que se verificará a través de SAVE. Haga referencia a tutoriales y guías de SAVE para obtener información sobre documentos aceptables para usar.
Para los miembros del hogar que seleccionan SI a esta pregunta con documentación justificativa válida, no se requiere ninguna verificación de SAVE.
Página 10 de 10 English on Back

![Mike Bond · 7KH +D]DUGV RI 6HFXULW\ $3, ’HVLJQ Mike Bond Computer Security Group BCS Advanced Programming Group 10th January](https://img.pdfslide.us/doc/110x75/6019d7e82f117d18fa2ade9b/mike-7kh-ddugv-ri-6hfxulw-3-ahvljq-mike-bond-computer-security-group-bcs.jpg)

![IoT Data Days 21 - gdsd.statistik.uni-muenchen.de · %urdg sruwirolr ri forxg vhuylfhv +\eulg 2shudwlrqv 6hfxulw\ 0dqdjhphqw %dfnxs 6wru6lpsoh $]xuh 6lwh 5hfryhu\ ,psruw ([sruw $]xuh](https://img.pdfslide.us/doc/110x75/5e10775ef3ca9f35435ead8d/iot-data-days-21-gdsd-urdg-sruwirolr-ri-forxg-vhuylfhv-eulg-2shudwlrqv-6hfxulw.jpg)

























