-
7/27/2019 CA Endometrial e Hiisteroscopia
1/5
O N C O L O G Y
The risk of diagnostic hysteroscopy
in women with endometrial cancerJennifer E. Soucie, MD, MSc;
Pamela A. Chu, MD, MBA; Sue Ross, PhD;
Tom Snodgrass, BSc (Hons); Stephen L. Wood, MD, MSc
OBJECTIVE : We sought to evaluate whether hysteroscopy in
patients
with endometrial cancer had an effect on disease stage or
mortality.
STUDY DESIGN: This was a retrospective cohort analysis of data
linked
between a registry of women diagnosed with endometrial cancer
and
physician billing data on hysteroscopy.
RESULTS: A 99.8% match rate was obtained. Eighty-five percent
of
cases had complete data on staging. Of these 1972 cases, 672
(34.1%) hadundergone hysteroscopy. There wasno difference in
stage
III disease between the hysteroscopy (7.1%) vs no hysteroscopy
(6.5%)
group (P .38). There was also no difference in death rates,
13.2% vs
15.2% (P .25), or in the proportion of women dying of female
genital
organ cancer, 46.1% vs 42.1% (P .53), respectively.
CONCLUSION: Hysteroscopy is not associated with a higher rate
of
stage III disease or mortality. It allows for accurate diagnosis
with direct
visualization and biopsy, and should be considered a safe
diagnostic
tool.
Key words: endometrial cancer, hysteroscopy, mortality,
stage
Cite this article as: Soucie JE, Chu PA, Ross S, et al. The risk
of diagnostic hysteroscopy in women with endometrial cancer. Am J
Obstet Gynecol
2012;207:71.e1-5.
Hysteroscopy is widely used for thediagnosis of endometrial
hyper-plasia or carcinoma. The sensitivity has
been estimated to be 86.4%.1 In compar-
ison, Pipelle endometrial biopsies have
been reported to have a sensitivity of 67-
83.5%.2,3 It has also been shown that
hysteroscopically guided curettage hashigher accuracy than
dilatation and cu-
rettage (D&C)alone.4However, concern
exists that the introduction of high-pres-
sure gas or fluid into the uterine cavity,
to produce distension, could facilitate
the dissemination of malignant cells in
patients with endometrial cancer. It has
been found that the distention medium
can begin draining transcervically and
transtubally when pressures reach ap-
proximately 100-150 mm Hg. Thus, in
the patient with endometrial cancer,
there is the theoretical possibility that
malignant cells might be dispersed intothe fallopian tubes and
the abdominal
cavity following hysteroscopy.5 The evi-
dence associating peritoneal dissemina-
tion with hysteroscopy and ultimately its
possible effect on endometrial cancer
mortality outcomes is inconclusive.6-16
This study was undertaken to evaluate
whether preoperative hysteroscopy per-
formed in patients with endometrial
cancer had an effect on subsequent sur-
gical staging, and ultimately mortality. It
is a retrospective cohort analysis of data
on women who had been diagnosed with
endometrial cancer over a period of 10years (1997 through
2006).
MATERIALS AND METHODS
Sources of data for this study were the
Alberta Cancer Registry and physician
billing data from Alberta Health and
Wellness. The Alberta Cancer Registry
captures data on all patients diagnosed
with a cancer that is identified by the In-
ternational Classification for Diseases for
Oncology. Data on women with endome-trial cancer were retrieved
from the reg-
istry from Jan. 1, 1997, through Dec. 31,
2006. This start time was chosen princi-
pally because the Alberta Cancer Regis-
try had undergone a number of coding
changes prior to this time period. It was
not until 1997 that endometrioid adeno-
carcinoma was differentiated from other
more aggressive nonadenocarcinoma
histologic types, such as, clear cell and
papillary serous. A second benefit to this
time period was the introduction of newstaging criteria for
endometrial cancer
From the Departments of Obstetrics and Gynecology (Drs Soucie,
Chu, Ross, and Wood),Community Health Sciences (Drs Ross and Wood),
and Family Medicine (Dr Ross), Faculty ofMedicine, University of
Calgary, and Cancer Care-Alberta Health Services (Mr
Snodgrass),
Calgary, Alberta, Canada.Received Jan. 28, 2012; revised March
21, 2012; accepted April 25, 2012.
Supported by McClure Memorial Cancer Endowment, University of
Calgary (J.E.S.).
This study is based in part on data provided by Alberta Health
and Wellness. The interpretationand conclusions contained herein
are those of the researchers and do not necessarily representthe
views of the Government of Alberta. Neither the government nor
Alberta Health and Wellnessexpresses any opinion in relation to
this study.
The authors report no conflict of interest.
Presented at the 40th Global Congress of Minimally Invasive
Gynecology, American Association ofGynecologic Laparoscopists,
Hollywood, FL, Nov. 6-10, 2011, and the 40th annual meeting,
Association of Academic Professionals in Obstetrics and
Gynecology of Canada, Toronto,Ontario, Canada, Dec. 2-4, 2011.
Reprints not available from the authors.
0002-9378/$36.00 2012 Mosby, Inc. All rights reserved.
http://dx.doi.org/10.1016/j.ajog.2012.04.026
Research www.AJOG.org
JULY 2012 American Journal of Obstetrics &Gynecology
71.e1
http://dx.doi.org/10.1016/j.ajog.2012.04.026http://dx.doi.org/10.1016/j.ajog.2012.04.026
-
7/27/2019 CA Endometrial e Hiisteroscopia
2/5
that took place in 1989. Staging after that
change included surgical observations.17
Besides diagnosis, the Alberta Cancer
Registry provided further information
on pathology (histologic cell type and
staging) and vital statistics. Loss to fol-
low-up within the Alberta Cancer Regis-try is minimal, as each
month linkage is
made to Alberta Vital Statistics to iden-
tify those cancer patients who have died
and the causeof death. In addition, there
is a link made annually with the Cana-
dian National Mortality database. How-
ever, patients who die outside Canada
could be potentially missed.
Cases were selected from the Alberta
Cancer Registry based on the diagnosis
of endometrial cancer as defined by a
positive biopsy. Staging was reported bythe treating physician.
In Alberta, pelvic
washings are considered the standard of
care. The majority of cases would have
also included pelvic lymph node sam-
pling. For the few cases missing node
sampling, the performance of pelvic
washings alone would have dictated the
classification of stage IIIa disease based
on the International Federation of Gyne-
cology and Obstetrics (FIGO) 1989 stag-
ing criteria.17
A thorough review of this dataset wasthen performed to eliminate
transcrip-
tion errors and to clarify staging. When
staging information within the dataset
was missing or not interpretable, cross-
reference to other variables (ie, text en-
tered by the physician) in the wider elec-
tronic database allowed for clarification
in many cases. Finally, any staging based
on the American Joint Committees
Cancer TNM staging manual (fifth and
sixth editions) was translated to the FIGO
1989 staging criteria.17
Alberta Health and Wellness adminis-
ters a universal health care plan that cov-
ers all Albertans, and through this, phy-
sicians are reimbursed for all procedures
performed in the province. The Alberta
Health and Wellness dataset provided
information on diagnostic hysteroscopy
(specifically by fee code 80.81) and patient
characteristics(age). This code would have
captured hysteroscopy performed in both
the office setting and operating room.When hysteroscopy was not
performed,
diagnoses would have been made by either
office endometrial biopsy or D&C.
The cases from the cancer registry
were then linked to the Alberta Health
and Wellness dataset. Information on
whether a diagnostic hysteroscopy was
performed for each patient was ab-stracted. Data linkage went
back as far as
January 1996, to include information on
cases that were pulled from the Alberta
CancerRegistry forthe year of 1997. This
would represent hysteroscopy that had
been performed within 1 year, isolating
that which was used for the diagnosis of
endometrial cancer. Data linkage was
performed using at least 2 patient-spe-
cific variables within each dataset, and allidentifying
information was removed
from the linked dataset before release foranalysis.
Women with stage IV disease were ex-
cluded, since diagnosis with an endome-
trial sample may not have been required,
as disease may have been more clinically
apparent at presentation. As the survival
in this group is also close to 0,this would
have affected our analysis by dispropor-
tionably decreasing the survival for
women who had not had hysteroscopy.
Cases were also excluded if histology in-
dicated a nonadenocarcinoma type ofcancer, such as squamous,
clear cell, pap-
illary serous, and/or undifferentiated car-
cinoma. This eliminated advanced dis-
ease that was likely due to the inherent
disease process of a more aggressive tu-
mor type, rather than the diagnostic
technique used.
There were 2 primary outcomes in
this study: staging and overall survival.
Staging IIIa would indicate that thecarcinoma had extended out
of the
uterus. If peritoneal dissemination viathe fallopian tubes
occurs during hys-
teroscopy, staging should indicate at
least stage III. Therefore, the study hy-
pothesis was that hysteroscopy would
be associated with an increased fre-
quency of stage III disease and endo-
metrial cancerrelated deaths.
Review of the literature suggested that
10% of those women with endometrial
cancerwho undergo hysteroscopyfor di-
agnostic purposes and 5% of those who
do not undergo hysteroscopy will havestage III disease.12 From
this, it was cal-
culated that a sample size of 387 and 581
women who have and have not under-
gone hysteroscopy, respectively, would
be needed to detect a difference in stag-
ing with a power of 80% and an alpha
error of 0.05. These numbers were easily
attained from the provincial registries.Data were summarized
using propor-
tions for categorical variables, and bothmean and median for
continuous vari-
ables. Bivariate analyses were performed
to compare the hysteroscopy groups in
regard to staging and other possible
prognostic risk factors. Comparisons
were made using Pearson 2 test for cat-
egorical variables. Mantel-Haenszel 2
test was used to identify trends in pro-
portions. A Student t test was used to
compare continuous variables if theywere normally distributed;
otherwise,
the Wilcoxon rank sum test was used.
P .05 was considered to be statistically
significant. All statistical calculations
were performed using the SAS program
package (SAS Institute, Cary, NC).
Data were managed according to the
Alberta Privacy Legislation. Data linkage
between Albertas Cancer Registry and
the Health and Wellness dataset was per-
formed by Alberta Health and Wellness.
Thisprocess did not compromise patientconfidentiality as only
anonymous datawere received by the research team. Eth-
ical approval was obtained from the
Conjoint Health Research Ethics Board
at the University of Calgary (Ethics Re-
view Board no: E-20934).
RESULTS
The initial data request from the Alberta
Cancer Board had provided 2331 cases
that met both inclusion and exclusioncriteria. A 99.8% match
rate was ob-
tained when linkage was performed with
the Alberta Health and Wellness claims
data. Approximately 85% of these cases
had complete and appropriate data on
staging (350 were missing staging com-
pletely, while 5 had staging complicated
by coexistent cancer, a different type of
cancer, or a benign condition). Of these
1972 cases with complete staging, 672
(34.1%) had undergone hysteroscopy.
There wasan increase in the utilizationof hysteroscopy over the
study period,
Research Oncology www.AJOG.org
71.e2 American Journal of Obstetrics &Gynecology JULY
2012
-
7/27/2019 CA Endometrial e Hiisteroscopia
3/5
and in the number of cases diagnosed. In
1997, 40 hysteroscopies were performed
in 154 women who were diagnosed with
endometrial cancer (26.0%), whereas, in
2006, 95 hysteroscopies were performed
in 232 women (40.9%).
The mean age was 62.0 and 60.7 years,respectively, for women who
had under-gone hysteroscopy and those who had
not (Wilcoxon rank sum, P .01).
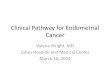
The frequencies of FIGO stages in the
2 groups are shown in Table 1. The rates
of stage III disease did not differ statisti-
cally between those who had and did not
have hysteroscopy (relative risk, 1.16;
95% confidence interval [CI], 0.831.62;
P .38).
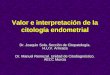
There was also no statistically signifi-
cant difference found in death rates forthose who had a
hysteroscopy (13.2%)
compared to those who had not (15.2%)
(relative risk, 0.87; 95% CI, 0.691.10;
P .25) (Table 2). The mean years of
follow-up for each group were 4.0 (0.03-
9.97) and 4.4 (0.02-10.67), respectively.
Survival analysis was not possible be-
cause of the relatively fewer numbers of
deaths, resulting in high censor rate in
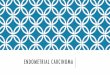
the analysis. When evaluating only those
women who had died, statistically signif-
icant differences were found neither inthe proportion of stage
III disease (P
.10), nor in the proportion of women dy-
ing of female genital organ cancer be-
tween hysteroscopy groups (P .53)
(Table 3).
COMMENT
Our results indicate that hysteroscopy in
patients with endometrialcancer is not as-
sociated with a higher rate of subsequent
stage III disease. There was no statisticaldifference in death
rates between hysteros-
copy groups. Additionally, among those
who had died, there was no statistical dif-
ference in stage III disease between hyster-
oscopy groups.
Previous studies have published con-
flicting results about the effect of hyster-
oscopy on peritoneal dissemination of
malignant cells and upstaging of disease
in women who have endometrial cancer.
The first of the reports providing evi-
dence against hysteroscopy was by Ober-mair et al.8 Their group
performed a
multicenter, retrospective cohort analy-sis of 113 consecutive
patients with en-
dometrialcancer limited to theinner half
of the myometrium, who underwent
D&C either with or without prior diag-
nostic hysteroscopy. They found that the
only factor significantly associated with
positive peritonealcytology was a history
of hysteroscopy (12.2% vs 2.5%, P
.04).
Zerbe et al6 reviewed the charts of 222
patients with endometrial cancer and
evaluated the peritoneal dissemination
of malignant cells during hysteroscopy.They found a difference
in positive peri-
toneal cytology in those who had hyster-
oscopy vs those who had not (odds ratio,
2.6; 95% CI, 1.026.63; P .05).
Bradley et al15 reviewed 256 charts of
women with endometrial cancer. In all,
204 cases were diagnosed by endometrial
biopsy or D&C, whereas 52 were diag-
nosed withhysteroscopy. A nonsignificant
lower proportion of patients (6.9%) had
malignant orsuspicious cytology intheen-
dometrial biopsy or D&C group, com-
TABLE 1
Stage of disease by hysteroscopy
Hysteroscopy
Stage
Yesn 672
No. (%)
Non 1300
No. (%) Statistical testStageIII 621 (92.9) 1215 (93.5) 2 P
.38..............................................................................................................................................................................................................................................
Stage III 51 (7.1) 85 (6.5) RR, 1.16; 95% CI,
0.831.62..............................................................................................................................................................................................................................................
Details of FIGO
stage.....................................................................................................................................................................................................................................
FIGO 0 1 (0.2) 3
(0.2).....................................................................................................................................................................................................................................
FIGO Ia 67 (10.0) 112
(8.6).....................................................................................................................................................................................................................................
FIGO Ia 133 (19.8) 265
(20.4).....................................................................................................................................................................................................................................
FIGO Ib 182 (27.1) 447
(34.4).....................................................................................................................................................................................................................................
FIGO Ic 116 (17.3) 201
(15.5).....................................................................................................................................................................................................................................
FIGO IIa 2 (0.3) 19
(1.5).....................................................................................................................................................................................................................................
FIGO IIa 49 (7.3) 55
(4.2).....................................................................................................................................................................................................................................
FIGO IIb 71 (10.6) 113
(8.7).....................................................................................................................................................................................................................................
FIGO IIIa 1 (0.2) 3
(0.2).....................................................................................................................................................................................................................................
FIGO IIIa 21 (3.1) 54
(4.2).....................................................................................................................................................................................................................................
FIGO IIIb 3 (0.5) 5
(0.4).....................................................................................................................................................................................................................................
FIGO IIIc 26 (3.9) 23
(1.8)..............................................................................................................................................................................................................................................
CI, confidence interval; FIGO, International Federation of
Gynecology and Obstetrics; RR, relative risk.
a Substaging was not available.
Soucie. Riskof hysteroscopy in endometrial cancer. Am J Obstet
Gynecol 2012.
TABLE 2
Vital statistics by hysteroscopy
Hysteroscopy
Vital statisticsYes n 672No. (%)
No n 1300No. (%) Statistical test
Alive 583 (86.8) 1103 (84.8) 2 P
.25..............................................................................................................................................................................................................................................
Dead 89 (13.2) 197 (15.2) RR, 0.87; 95% CI,
0.691.10..............................................................................................................................................................................................................................................
CI, confidence interval; RR, relative risk.
Soucie. Riskof hysteroscopy in endometrial cancer. Am J Obstet
Gynecol 2012.
www.AJOG.org Oncology Research
JULY 2012 American Journal of Obstetrics &Gynecology
71.e3
-
7/27/2019 CA Endometrial e Hiisteroscopia
4/5
pared to the hysteroscopy group (13.5%)(P .15). However, after
controlling for
stage and grade, the odds ratio for positive
cytology after hysteroscopy was 3.88 (95%
CI, 1.1113.6; P .03).
The final study providing evidence
against the use of hysteroscopy was per-
formed by Takac and Zegura.16 In their
review of 146 women with endometrial
cancer diagnosed with either D&C or of-
fice hysteroscopy, they found suspicious
or positive peritoneal cytology was pres-
ent in 1.6% (2/122) after D&C and12.5% (3/24) after
hysteroscopy (P
.05).
Evidence in support of the use of hys-
teroscopy has also been published. Gu et
al9 found that of 23 patients who were
diagnosed by D&C with hysteroscopy,
17 had abnormal peritoneal washings
(13.0%). Of 177 patients diagnosed by
either endometrial biopsy or D&C with-
out hysteroscopy, again 17 had abnor-
mal peritoneal washings (9.6%). The
rates were not different statistically.Similarly, Selvaggi et
al7 evaluated pa-
tients with endometrial cancer and
found that 52 had a diagnosis made only
by D&C, 56 underwent D&C and then
hysteroscopy, and 39 had only hysteros-
copy. Peritoneal cytology was positive in
9 patients, and 21 had microscopic intra-
peritoneal dissemination; neither was
significantly associated with hysteros-
copy (P .07).
Juhasz-Boss et al14 took a novel ap-
proach to evaluating the effects of hyster-oscopy.Whensentinel
lymph node biopsy
is performed, a second hysteroscopy isnecessary for technetium
injection. Ju-
hasz-Boss et al14 took this factor into con-
sideration in their analysis, and examined
whetherthe number of hysteroscopiesand
the time interval between hysteroscopy
and surgery had an effect on cytology. The
rate of positive cytology was 18.2% (4/22)
in those without hysteroscopy vs 1.9% (2/
104) and 7.1% (5/70) for those with 1 and
2 hysteroscopies, respectively (P .008).
Furthermore, positive cytology was notre-
lated to the timeintervalbetween preoper-ative hysteroscopy and
definitive surgery.Kudela and Pilka10 prospectively re-
viewed 134 women diagnosed with hys-
teroscopy and 61 diagnosed with D&C.
Positive or suspect cytology in fluid from
lavage was present in 30.3% for those
with hysteroscopy, compared to 33.9%
in those who underwent a D&C. Both
groups were comparable for stages of
disease.
Ben-Arie et al11 reported on a cohort of
392 women diagnosed with endometrialcancer with endometrial
biopsy (25.3%),
uterine curettage (49.2%), and hysteros-
copy (25.5%). In this series, poor histo-
logic types, including serous papillary,
clear cell, and small cell cancer were in-
cluded in the analysis. Peritoneal cytol-
ogy was positivein only1 case, thus com-
parison could not be made. However, no
statistic difference in the survival rate
was found between diagnostic methods.
There have been 2 randomized con-
trolled trials evaluating the effects of hys-teroscopy on
peritoneal cytology. Sainz
de la Cuesta et al12 examined 50 consec-
utive patients with endometrial cancer.
Patients were randomized 3:2 to have or
not to have fluid hysteroscopy biopsy
performed just prior to surgery. There
were 3 patients (10%) with positive
washings in the hysteroscopic groupcompared to 1 (5%) among the
controls
(P .64). This difference was not statis-
tically significant; however, the small
sample size only allowed for a statistical
power of20%. Median follow-up was
34 months, and all patients but 1 (de-
ceased due to unrelated cause) were alive
with no evidence of disease. The authors
concluded that fluid hysteroscopy and
directed biopsies may have a small risk of
upstaging early endometrial cancer but
does not seem to influence prognosis.Cicinelli et al13
randomized 140 women
to undergoor notundergodiagnosticfluid
minihysteroscopy before surgical staging.
There was no difference in peritoneal cy-
tology between those who had hysteros-
copy (5.7%) vs those who did not (8.5%).
After a mean duration of follow-up of 62
months, overall survival and disease-free
survival werenot significantly different for
the 2 groups.
From the literature, it is evident that
there is no firm conclusion as to whetherhysteroscopy leads to
peritoneal dissem-
ination of malignant cells in women who
have endometrial cancer. Prior to this
publication, and not including the 2 ran-
domized controlled trials, a metaanalysis
indicated that hysteroscopy is associated
with a small risk of peritoneal spread, and
by direct extension, higher disease upstag-
ing. However, they note that greater num-
bers are needed to clarify the effect on
prognosis.18Thesamplesizesofthestudies
to date have been small to moderate with
limited follow-up intervals to adequately
evaluate survival differences. Our study
provides more informationas it includeda
large sample, with a cohort spanning over
10 years. The results indicate clearly that
hysteroscopy is not associated with higher
stagingof endometrialcancer.From this, it
suggests that hysteroscopy does not im-
pose a significant risk of dissemination.
Most importantly, there was no difference
in death rates, and more specifically, thecause of death from
female genital organ
TABLE 3
Staging and cause of death by hysteroscopy among women who
died
Hysteroscopy
StagingYes n 89No. (%)
No n 197No. (%) 2 Pvalue
StageIII 70 (78.7) 170 (86.3)
.10..............................................................................................................................................................................................................................................
Stage III 19 (21.3) 27
(13.7)..............................................................................................................................................................................................................................................
Cause of
death.....................................................................................................................................................................................................................................
Noncancer death cause 25 (28.1) 62 (31.5)
.53a.....................................................................................................................................................................................................................................
Female genital organ cancer 41 (46.1) 83
(42.1).....................................................................................................................................................................................................................................
Other cancer 15 (16.9) 37
(18.8).....................................................................................................................................................................................................................................
Primary unknown death cause not coded 8 (9.0) 15
(7.6)..............................................................................................................................................................................................................................................a2
comparing female genital organ cancer vs all other causes of
death.
Soucie. Riskof hysteroscopy in endometrial cancer. Am J Obstet
Gynecol 2012.
Research Oncology www.AJOG.org
71.e4 American Journal of Obstetrics &Gynecology JULY
2012
-
7/27/2019 CA Endometrial e Hiisteroscopia
5/5
cancer did not differ significantly between
the groups.
There are a few limitations to this study,
the main limitation being that positive
peritoneal cytology could not be directly
evaluated, as the information was not
available in either of the electronic data-bases. To retrieve
this information, indi-
vidual patient charts at each regional
health authority would have to have been
reviewed, and this was not possible. In-
stead, disease stage was evaluated, with the
hypothesisthatanyupstagingofdiseasere-
sulting from hysteroscopy should have
been evident in our analysis. It should also
be noted that FIGO did replace their stag-
ing criteria in 2009, with positive perito-
neal cytology not included as it was not
considered to have an independent effecton survival.19
Nonetheless, all staging in
this cohort was based on the previous cri-
teria, and thus peritoneal cytology would
have been captured by this older classifica-
tion system.
This study was also a retrospective co-
hort study, and therefore by design is
subject to several possible biases, namely
reporting and selection bias. It would be
ideal if all cases of endometrial cancer
were reported to the cancer registry;
however, this is unlikely and thus, somedegree of reporting bias
may be evident.
It would be impossible to know whether
there were differences in reporting for
those who had hysteroscopy vs those
who had not. However, the Alberta Can-
cer Registry has an overall calculated
capture rate of 95%, and thus a differ-
ence in reporting was likely minimal.
Finally, 15% of our sample was miss-
ing staging data, and this is a common
problem with administrative databases.
Every effort was made to ascertain miss-
ing data from the larger database when
available.
Ourlarge study covering a periodof 10
years of endometrial cancer manage-
ment offers valuable evidence to guide
clinical practice. Our results clearly indi-cate that
hysteroscopy, which allows for
direct visualization and directed biopsy,
should be considered a safe diagnostic
tool in women suspected of having en-
dometrial cancer. f
REFERENCES
1. Clark TJ, Voit D, Gupta JK, Hyde C, Song F,Khan KS. Accuracy
of hysteroscopy in the di-agnosis of endometrial cancer and
hyperplasia:a systematic quantitative review. JAMA
2002;288:1610-21.
2. Ferry J, Farnsworth A, Webster M, Wren B.Efficacy of the
Pipelle endometrial biopsy in de-tecting endometrial cancer. Aust N
Z J ObstetGynecol 1993;33:76-8.3. Guido RS, Kanbour-Shakir A, Rulin
MC,Christopherson WA. Pipelle endometrial sam-pling: sensitivity in
the detection of endometrialcancer. J Reprod Med 1995;33:76-8.4.
Goldrath MH, Sherman AI. Office hysteros-copy and suction
curettage: can we eliminatethe hospital diagnostic dilatation and
curet-tage? Am J Obstet Gynecol 1985;152:220-9.5. Egarter C,
Krestan C, Kurz C. Abdominaldis-semination of malignant cells with
hysteros-copy. Gynecol Oncol 1996;63:143-4.6. Zerbe MJ, Zhang J,
Bristow RE, GrumbineFC, Abularach S, Montz FJ. Retrograde seed-ing
of malignant cells during hysteroscopy inpresumed early endometrial
cancer. GynecolOncol 2000;79:55-8.7. Selvaggi L, Cormio G, Ceci O,
Loverro G,Cazzolla A, Bettocchi S. Hysteroscopy does notincrease
the risk of microscopic extrauterinespread in endometrial
carcinoma. Int J GynecolCancer 2003;13:223-7.8. Obermair A, Geramou
M, Gucer F, et al.Does hysteroscopy facilitate tumor cell
dissem-ination? Incidence of peritoneal cytology frompatients with
early stageendometrial carcinoma
following dilatation and curettage(D & C) versus
hysteroscopy and D & C. Cancer 2000;88:
139-43.
9. Gu M, Shi W, Huang J, Barakat RR, Thaler
HT, Saigo PE. Association between initial diag-nostic procedure
and hysteroscopy and abnor-
mal peritoneal washings in patients with endo-
metrial carcinoma. Cancer 2000;90:143-7.
10. Kudela M, Pilka R. Is there a real risk in
patients with endometrial carcinoma undergo-ing diagnostic
hysteroscopy (HSC)? Eur J
Gynaecol Oncol 2001;22:342-4.
11. Ben-Arie A, Tamir S, Dubnik S, et al. Does
hysteroscopy affect prognosis in apparent ear-
ly-stage endometrial cancer? Int J GynecolCancer
2008;18:813-9.
12. Sainz de la Cuesta R, Espinosa JA, Crespo
E, Granizo JJ, Rivas F. Does fluid hysteroscopy
increase the stage or worsen the prognosis in
patients with endometrial cancer? A random-
ized controlled trial. Eur J Obstet Gynecol Re-prod Biol
2004;115:211-5.
13. CicinelliE, Tinelli R, ColafiglioG, et al.Risk oflong-term
pelvic recurrences after fluid minihys-
teroscopy in women with endometrial carcino-
ma: a controlled randomized study. Meno-pause 2010;17:511-5.
14. Juhasz-Boss I, Fehm T, Nauth A, et al.
Number of hysteroscopies and the time interval
between hysteroscopy and surgery: influence
on peritoneal cytology in patients with endome-trial cancer.
Anticancer Res 2010;30:2425-30.
15. Bradley WH, Boente MP, Brooker D, et al.
Hysteroscopy and cytology in endometrial can-
cer. Obstet Gynecol 2004;104:1030-3.16. Takac I, Zegura B.
Office hysteroscopy and
the risk of microscopic extrauterine spread inendometrial
cancer. Gynecol Oncol 2007;107:
94-8.
17. International Federation of Gynecology and
Obstetrics. Corpus cancer staging. Int J Gynae-col Obstet
1989;28:190.
18. Polyzos NP, Mauri D, Tsioras S, Messini CI,
Valachis A, Messinis IE. Intraperitoneal dissem-
ination of endometrial cancer cells after hyster-
oscopy: a systematic review and meta-analysis.Int J Gynecol
Cancer 2009;20:261-7.
19. Lewin SN. Revised FIGO staging systemfor
endometrial cancer. Clin Obstet Gynecol 2011;
54:215-8.
www.AJOG.org Oncology Research
JULY 2012 American Journal of Obstetrics &Gynecology
71.e5