Embed Size (px)
Citation preview

Case ReportC2 Solitary Bone Plasmacytoma Curettage and VertebralAugmentation in an 83-Year-Old Female: Case Report andReview of Surgical Treatment Approaches in the Spine
Matthew J. Yousif,1,2 Taha A. Faruqi,1,2 Rakesh Ramakrishnan,1,2 and Nilesh M. Patel2
1Beaumont Hospital Farmington Hills, Farmington Hills, MI, USA2Beaumont Hospital Oakwood Dearborn, Dearborn, MI, USA
Correspondence should be addressed to Taha A. Faruqi; [email protected]
Received 27 June 2017; Accepted 1 November 2017; Published 17 December 2017
Academic Editor: Ali F. Ozer
Copyright © 2017 Matthew J. Yousif et al. ,is is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Surgically, solitary bone plasmacytoma (SBP) of the craniocervical junction (CCJ) is typically treated with cement augmentation andoccipital-cervical stabilization (OCS). In the orthopedic spine literature, various surgical treatment options have been described forSBP, but only a few studies exist describing SBP of the CCJ with treatment involving cement augmentation alone. We report the caseof an 83-year-old female found to have C2 SBP that was successfully treated with curettage and cement augmentation alone.
1. Introduction
Solitary bone plasmacytoma (SBP) is a localized plasmacell tumor accounting for 2–5% of plasma cell malignancies.,e median age of SBP is 55. When compared to multiplemyeloma, SBP occurs more frequently in younger patientsand has a much better prognosis [1, 2]. SBP has a 2-3 timeshigher incidence in males compared to females, whereasmultiple myeloma displays an equal gender incidence [3].Patients typically present with severe neck pain with move-ment before the onset of neurologic symptoms [2, 4]. Oncomputed tomography (CT), SBP usually presents as a large,well-demarcated, cyst-like lesion [1]. Criteria for diagnosis ofSBP include a radiographic lytic lesion, monoclonal plasmacell inBltration on biopsy, histologically normal bone marrowaspirate, absent or low concentration of serum and urineprotein on electrophoresis, and absence of anemia, hyper-calcemia, or renal impairment [1, 5].
Plasma cell neoplasms of the craniocervical junction(CCJ) are rare. When they do occur, early recognition isimportant as they can lead to cervical spine instabilityand sudden death. ,ey often respond to radiation therapyand, however, can also be managed surgically. Lesions ofthe cervical spine are typically operated on if there is evidenceof spinal instability, algesia, or neurologic compromise [5].
Surgical treatment guidelines do not currently exist forplasma cell neoplasms of the CCJ [2, 5]. Surgically, SBPof the spine is treated based on location, degree of in-volvement of vertebrae, and preference of surgeon. Varioustreatment approaches discussed in the literature includevertebroplasty, occipitocervical stabilization (OCS), lam-inectomy, the use of intraoperative MRI, and two stagedsurgeries, amongst others [6–9].
Few cases of plasmacytoma of the cervical spine treatedsuccessfully with cement augmentation alone without fur-ther spine stabilization have been reported. To our knowl-edge, there is no report of an elderly female treated withcement augmentation alone for a C2 plasmacytoma withoutsubsequent cervical instability in the orthopedic literature.,is case demonstrates the possibility of favorable outcomesin elderly patients with plasmacytoma treated with cementaugmentation alone, as opposed to cement augmentationwith further spinal stabilization, which may pose additionalmorbidity and mortality.
2. Case
An 83-year-old woman presented to the emergency de-partment with a one-day nocturnal history of cervicalgia,dysphagia, and right scapular pain. She also complained of
HindawiCase Reports in OrthopedicsVolume 2017, Article ID 5692402, 3 pageshttps://doi.org/10.1155/2017/5692402

limited range of motion of the neck, and cervicalgia exac-erbated by movement. She did not admit to any history offalls, numbness or tingling, or systemic complaints. Physicalexam yielded tenderness to palpation in the cervical region.No sensory or motor neurological deBcits were noted. Vitalssigns, metabolic panel, and complete blood count werewithin normal limits. In the emergency department, CT ofthe cervical spine showed a large C2 lytic lesion with corticalbreakthrough in the inferior plate, as well as anteriorly.,ere was no vertebral height loss or collapse, and the C1-C2articulations were intact.
Subsequent serum and urine protein electrophoresisindicated possible monoclonal gammopathy with serumimmunoBxation. Bence-Jones proteins were present. Bonesurvey indicated signiBcant bone demineralization andarthritic changes with repeat demonstration of the lyticlesion at C2. No lesions of the right scapula or proximal ribswere noted.
It was decided, based on the patient’s age, poor bonequality, and multiple comorbidities, a C1–C3 fusion wouldpose excess risk to the patient. ,us, it was decided toperform intralesional curettage and cement augmentation.,e patient was informed that if cement augmentation wereto fail, a fusion could still be necessary later on.
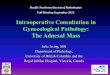
Intraoperatively, an anterior cervical approach was used.,en a small cortical window was made on the inferioraspect of the C2 vertebra. ,e tumor was suctioned andcuretted and Blled with iohexol contrast agent to conBrm theabsence of posterior leakage. Next, 2.5 mL of methylmethacrylate and bone Bller were inBltrated into the ver-tebra. Intraoperative and postoperative AP and lateralX-rays conBrmed no cement had extravagated posteriorly(Figures 1 and 2). Final pathologic diagnosis of the lesionand a bone marrow core biopsy revealed plasma cell mye-loma with kappa restriction.
At 9 months post-op, the patient’s neck and scapularpain was 100% improved and fully resolved. She progressedwell without any evidence of complication or looseningaround cement augmentation or cervical instability. At thattime, she was to follow up on a PRN basis only and continuehome exercises including isometrics and ROM.
3. Discussion
SBP in the CCJ is a rare entity that typically occurs inyounger males, and is responsive to radiation. Whensurgical intervention is needed, cement augmentation withfurther stabilization is routinely recommended to avoidinstability of the CCJ. ,ose treated with cement aug-mentation alone have previously been reported to developcervical instability and need future stabilization and fusionprocedure [6].
To our knowledge, this is the Brst case in the spineliterature of an elderly female successfully treated with ce-ment augmentation alone for a C2 plasmacytoma withoutsubsequent cervical instability. Our case is unique as SBPwas treated with cement augmentation alone in an elderlywoman with favorable outcome. At 9-month follow-up,she had no signs of cervical instability, and her cervicalgia
was completely resolved. ,is case illustrates how cementaugmentation alone may serve to limit morbidity andmortality in elderly individuals when compared to combinedcement augmentation with fusion. We will brieHy reviewtreatment modalities described for SBP of the spine cited inthe literature.
In a systemic review and proposed treatment algorithm,Ahmadi et al. describe a series of four patients with a meanage of 58 with cervical plasma cell neoplasms. One lesionwas present at C1, while the others were found at C2.Two patients received vertebroplasty and radiotherapy as
Figure 1: Lateral extended view showing bone Blter and meth-ylmethacrylate Blled into C2 curettage.
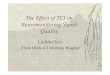
Figure 2: AP view with black/white reversal.
2 Case Reports in Orthopedics

primary management, and the others received occipito-cervical stabilization (OCS). ,e patients who receivedvertebroplasty alone developed secondary instability of theCCJ, requiring OCS at 5 and 12 months, while patients whounderwent OCS alone did not require any further surgicalintervention. Given these results and a review of the liter-ature, OCS for SBP in the CCJ was stated to be the favoredsurgical treatment option [6].
Lourbopoulos et al. described an unusual presentation ofplasmacytoma presenting as a C4–7 epidural mass causingprogressive upper and lower extremity weakness andnumbness in a 45-year-old male. ,e patient’s ascendingparalysis initially led to a misdiagnosis of Guillain-Barresyndrome, which was then correctly diagnosed as a cervicalepidural plasmacytoma. He was then treated with C4–7laminectomy alone. At 9- and 13-month follow-up visits,he was in complete remission, was able to ambulate withunilateral assistance, and continued to gain strength [7].
,ree cases of transoral resection of axial lesionsaugmented by intraoperative MRI have also been reported.Each case demonstrated diLerent lesions involving theCCJ. Intraoperative MRI was used to determine adequacyof decompression. In one case, intraoperative MRI ledto a change from the planned surgical approach. Intra-operative MRI did not adversely aLect operating timesor neurosurgical technique including instrumentationrequirements [8].
In 2004, Çolak performed a retrospective review of eightcases with C2 vertebral body neoplastic lesions to determinethe eLectiveness of a two-staged surgery and outcomes.Patients were Brst decompressed via an anterior approachand then stabilized posteriorly at a later time. It was foundthat the staged approach increased patient tolerabilitywithout increasing morbidity [9].
To our knowledge, this is the Brst case in the spineliterature of an elderly female successfully treated with ce-ment augmentation alone for a C2 plasmacytoma withoutsubsequent cervical instability. At 9-month follow-up, shehad no signs of cervical instability, and her cervicalgia wascompletely resolved. ,is case illustrates how cement aug-mentation alone may serve to limit morbidity and mortalityin elderly individuals when compared to combined cementaugmentation with fusion.
Our case represents another treatment option for solitarylesions within the CCJ. Our patient, an elderly female,demonstrated favorable outcome with cement augmentationand curettage for a C2 plasmacytoma without need forfurther stabilization or fusion.
4. Conclusion
SBP is a rare disease whose surgical treatment entailscement augmentation with further stabilization. Our casedemonstrates successful surgical treatment in an elderlyfemale patient with a C2 plasmacytoma utilizing cementaugmentation and curettage without need for furtherstabilization or fusion. ,is may be a potential deBnitivesurgical treatment option in patients with high morbidityand mortality.
Conflicts of Interest
,e authors declare that they have no conHicts of interest.
References
[1] R. Bataille and J. Sany, “Solitary myeloma: clinical and prog-nostic features of a review of 114 cases,” Cancer, vol. 48, no. 3,pp. 845–851, 1981.
[2] S. Voulgaris, M. Partheni, K. Gousias, K. Polyzoidis, andD. Konstantinou, “Solitary plasmacytoma of the upper cervicalspine: therapeutic considerations,” Jounal of NeurosurgicalSciences, vol. 52, no. 2, pp. 55–59, 2008.
[3] H. Singh, S. A. Meyer, and A. L. Jenkins, “Treatment of primaryvertebral tumors,” Mount Sinai Journal of Medicine, vol. 76,no. 5, pp. 499–504, 2009.
[4] H. R. Durr, J.-H. Kuhne, F.-W. Hagena, T. Moser, andH. J. ReBor, “Surgical treatment for myeloma of the bone,”Archives of Orthopaedic and Trauma Surgery, vol. 116, no. 8,pp. 463–469, 1997.
[5] R. Soutar, H. Lucraft, G. Jackson et al., “Guidelines on thediagnosis and management of solitary plasmacytoma of boneand solitary extramedullary plasmacytoma,” Clinical Oncology,vol. 16, no. 6, pp. 405–413, 2004.
[6] S. A. Ahmadi, P. J. Slotty, C. Munoz-Bendix, H.-J. Steiger, andJ. F. Cornelius, “Early surgical occipitocervical stabilization forplasma cell neoplasms at the craniocervical junction: systematicreview and proposal of a treatment algorithm,” Spine Journal,vol. 16, no. 1, pp. 91–104, 2015.
[7] A. Lourbopoulos, P. Ioannidis, I. Balogiannis, P. Stavrinou,T. Koletsa, and D. Karacostas, “Cervical epidural plasmacy-toma presenting as ascending paraparesis,” Spine Journal,vol. 11, no. 5, pp. e1–e4, 2011.
[8] T. Kaibara, R. John Hurlbert, and G. R. Sutherland, “Transoralresection of axial lesions augmented by intraoperative magneticresonance imaging,” Journal of Neurosurgery: Spine, vol. 95,no. 2, pp. 239–242, 2001.
[9] A. Çolak, M. Kutlay, K. Kıbıcı, M. Nusret Demircan, andO. N. Akın, “Two-staged operation on C2 neoplastic lesions:anterior excision and posterior stabilization,” NeurosurgicalReview, vol. 27, no. 3, pp. 189–193, 2003.
Case Reports in Orthopedics 3

Submit your manuscripts athttps://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com