Embed Size (px)
Citation preview

CLINICAL ARTICLE -NEUROSURGICAL TECHNIQUES
C2 root nerve sheath tumors management
Mohamed H. El-Sissy & Mostafa Mahmoud
Received: 7 December 2012 /Accepted: 18 February 2013 /Published online: 14 March 2013# Springer-Verlag Wien 2013
AbstractBackground Upper cervical nerve sheath tumors (NST)arising mainly from C2 root and to lesser extent from C1 rootare not uncommon, they constitute approximately 5-12% ofspinal nerve sheath tumors and 18-30% of all cervical nervesheath tumors, unique in presentation and their relationship toneighbouring structures owing to the discrete anatomy at theupper cervical-craniovertebral region, and have atendency forgrowth reaching large-sized tumors before manifesting clini-cally due to the capacious spinal canal at this region; accord-ingly the surgical approaches to such tumors are modified.The aim of this paper is to discuss the surgical strategies forupper cervical nerve sheath tumors.Methods Eleven patients (8 male and 3 females), age range28–63 years, with C2 root nerve sheath tumors were oper-ated upon based on their anatomical relations to the spinalcord. The magnetic resonance imaging findings were uti-lized to determine the surgical approach. The tumors hadextra- and intradural components in 10 patients, while in onethe tumor was purely intradural. The operative approachesincluded varied from extreme lateral transcondylarapproach(n=1) to laminectomy, whether complete(n=3) aor hemilaminectomy(n=7), with partial facetectomy(n=7),and with suboccipital craniectomy(n=2).
Results The clinical picture ranged from spasticity (n=8,72,72 %), tingling and numbness below neck (n=6,54,54 %), weakness (n=6, 54,54 %), posterior column in-volvement (n=4, 26,36 %), and neck pain (n=4, 36,36 %).The duration of symptoms ranged from 1 to 54 months, totalexcision was performed in 7 patients; while in 3 patients anextraspinal component, and in 1 patient a small intraduralcomponent, were left in situ. Eight patients showed im-provement of myelopathy; 2 patients maintained theirgrades. One poor-grade patient was deteriorated.Conclusion The surgical approaches for the C2 root nervesheath tumors should be tailored according to the relationshipto the spinal cord, determined by magnetic resonance imaging.
Keywords Cervical nerve sheath tumors . Craniovertebraljunction . Laminectomy . Extreme lateral transcondylarapproach
Introduction
Upper cervical nerve sheath tumors arising mainly from C2root are not uncommon, as all spinal nerve sheath tumors,they originate from the sensory roots and can extend via theintervertebral foramina to achieve a dumbbell shape [1]. Theupper cervical NST have certain characteristic features notshared by its counterparts in the other regions of the verte-bral column [2, 3]. The relatively large size of these lesionsat the C1-2 level which is explained by the spacious spinalcanal at this level. The mean sagittal diameters at the levelsof the atlas and axis are 23 and 20 mm, respectively, while inthe subaxial spine, the average diameter is only 15 mm. Thecervical bulge of the spinal cord also begins below the axis.At the occipitocervical and atlantoaxial levels, the facetalpillars lie anterior to the nerve roots exiting through theintervertebral foramina. This also permits an exuberantgrowth of the lesion outwards since there is no posterior
Abbreviations used in this paper: NST=nerve sheath tumors;C1=atlas vertebra; C2=axis vertebra; MRI=magnetic resonanceimaging; CVJ=craniovertebral junction; CSF=cerebrospinal fluid;NF-1= neurofibromatosis type 1; roots of C5, D1, D6, L1, S1, andS5=roots of 5th cervical, 1st dorsal, 6th dorsal, first lumbar, firstsacral and 5th sacral spinal segment.
M. H. El-Sissy (*)Neurosurgery Department, Kasr Al Aini Hospital,Cairo University, Cairo, Egypte-mail: [email protected]
M. MahmoudRadiology Department, Aldemerdash Hospital,Ain Shams University, Cairo, Egypt
Acta Neurochir (2013) 155:779–784DOI 10.1007/s00701-013-1659-3

bony obstruction to its growth at the C1-2 levels [4]. Thereis often a delay in the development of clinical symptomsuntil these tumors attain a fairly large size [4, 5]. The highertendency for extradural extension when compared to otherlevels within the spine; according to George et al. [3] 83 %of C1-2 nerve sheath lesions having an extradural extension,while, the total incidence of extradural extension of NST atother levels within the spine is only 16 %. The anatomicallocation with respect to the spinal cord mainly and nerveroots; the extent of its extra-dural and extra-spinal exten-sion; the relationship of the tumor to the vertebral artery; thepresence of multiple NST in the cervical spine; the uniqueosseous anatomy and the biomechanical features of thisregion define the surgical approach for management [4–10].
Materials and methods
This study includes 11 patients (8 male and 3 females), agerange 28–63 years, with C2 root nerve sheath tumors oper-ated upon in Kasr Al Aini Hospital, Cairo University, Egypt,and Doctor Soliman Fakeeh Hospital, Jeddah, Kingdom ofSaudi Arabia, between June 2004 and 31 April 2012. Thepatients were evaluated using cervical lateral andanteroposterior radiographs, computed tomography, andmagnetic resonance imaging (MRI) of the craniovertebraljunction (CVJ). The surgical approach was tailoredaccording the tumor relation to the spinal cord (Fig. 1),
ranging from extreme lateral transcondylar approach foranteriorly located lesions (single case), to complete orhemilaminectomy without or with partial facectomy (pre-serving 2/3 of the facet joint), without or with suboccipitalcraniectomy according to the tumor extension.
Results
The analysed cases were 11 patients with C2 root NST,8 males and 3 females, with age range from 28 to 63 years.The symptoms at the onset of illness (Table 1) were spas-ticity (n=8, 72,72 %), tingling and numbness below neck (n=6, 54,54 %), weakness (n=6, 54,54 %), posterior columninvolvement (n=4, 26,36 %), and neck pain (n=4, 36,36 %).The duration of symptoms ranged from 1 to 54 months. Inour series, only one patient had a purely intradural tumor(single case with anteriorly located schwannoma), while therest had both intra-and extradural components. For preoper-ative planning, the relationship of the tumor with the cordwas determined with the help of MRI and classified intothree types (Table 2)—anterior (1 case), anterolateral (7cases), posterolateral (3 cases). On T1-weighted MR se-quences, the lesions were hypointense in five cases andisointense in six cases. They were heterogeneouslyhyperintense in all patients on T2 sequences. Five(45,45 %) had hyperintense signal changes of the cord atthe level of the tumor. The plain radiographs of the cervical
A B
CD
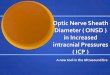
Fig. 1 a & b Sagittal and axialT1-weighted image with contrastshowing homogenouslyenhancing nerve sheath tumorintra/extraspinal; c Axial T1-weighted image with contrastshowing complete tumorresection; d (HE 20) spindleshaped tumor cells of aneurofibroma
780 Acta Neurochir (2013) 155:779–784

spine revealed scalloping of vertebral bodies in three, wid-ening of interlaminar space in two, and both in two cases.The plain radiographs were normal in six patients.Regarding the surgical approach, one patients with anterior-ly located tumor, total excision could be achieved using theextreme lateral transcondylar approach [11–15]. The mostcommon location was the anterolateral one (seven cases). Inthese patients all, addition of partial facetectomy tohemilaminectomy(six cases) or to complete laminectomy(one case) provided an oblique access to the tumor. T-shaped dural incision in order to connect the intra- andextradural components. Excision of the denticulate ligamenthas facilitated access to the part of the lesion located anteriorto the cord within the intradural space. The posterolaterallylocated lesions (three cases) were approached by completelaminectomy (two cases) or hemilaminectomy (one case). Intwo patients, where lesions were extending above the fora-men magnum, a suboccipital craniectomy was alsoperformed. One or more rootlets were sacrificed in all cases.In five cases, the entire nerve root from which the tumor wasarising was sacrificed. A patch graft was used to close thedura in five cases with anterolateral lesions, who underwenthemilaminectomy and partial facetectomy with a ‘T’ inci-sion of the dura. Total excision was achieved in sevenpatients, while subtotal excision could be achieved in fourpatients, three of them were anterolaterally placed and singleposterolaterally placed lesions. In three of these patients, apart of the tumor extending far laterally beyond the confinesof the spinal canal (extraspinal part) was not removed, and
in one patient with an anterolaterally placed lesion, a smallpart of it, located anterior to the cord that did not have aclear arachnoid plane of cleavage, was left in situ.Regarding the clinical assessment performed at the time ofdischarge, eight of the 11 patients showed improvement(spasticity in five cases and spasticity with motor power inthree cases) while two patients clinical examinationremained stationary. A single quadreparetic patient with ananterolaterally located NST, which was totally excised, de-veloped complete quadriplegia postoperatively, mechanicalventilator dependence, bronchopneumonia, and death12 days postoperative. Two patients from the five cases,where a patch dural graft was placed, developed CSF leakfrom the operative incision and they could be managed bylumbar drainage. Pathological examination revealedschwannomas in eight cases and neurofibromas in threecases.
Discussion
Upper cervical nerve sheath tumors arising mainly from C2root and to lesser extent from C1 root are not uncommon,they constitute approximately 5-12% of spinal nerve sheathtumors and 18-30% of all cervical nerve sheath tumors.They usually occur between 25 and 50 years of age andare rare in the paediatric population [1, 16]. Spinal nervesheath tumors are usually benign and are classified as eitherschwannomas or neurofibromas. Schwannoma is composedof differentiated neoplastic schwan cells and it is encapsu-lated, while neurofibroma can be solitary or as a part of VonRecklinghausen’s disease, it is composed of schwan cells,perineural cells and fibroplasts, it has no capsule and caninfiltrate the nerve fascicles. The growth of these tumors canbe constricted at two sites along the nerve root and theintervertebral foramen, and this may be the reason for theirdumbbell configuration [20]. Such a configuration is seen inapproximately 10 % of spinal neuromas arising from thespinal nerve in the foraminal or extraforaminal region [1]. Ina series of 176 spinal nerve sheath tumors in 149 patientsreported by Jinnai et al., purely intradural tumors composedonly 8 % of the tumors of the first two cervical nerve roots,
Table 1 Clinical picture
Presenting features Number of patients
Spasticity 8
Weakness 6
Spinothalamic tract involvement 6
Neck pain 4
Posterior column involvement 4
Neck muscle wasting 3
Neck swelling 1
Horner’s syndrome 1
Table 2 Tumor relation to thespinal cord and surgicalapproach
Location N ofcases
Surgical approach
Extremelateraltrancondylar
Laminectomy Hemilaminectomy Partialfacetectomy.
+/− Suboccipitalcraniectomy
Anterolateral 7 − 1 6 7 −
Posterolateral 3 − 2 1 − 1
Anterior 1 1 − − − 1
Acta Neurochir (2013) 155:779–784 781

and the percentage of these tumors increased gradually fromthe cervical to the dorsolumbar region [20]. In contrast, thepercentage of strictly extradural tumors gradually decreasedfrom the rostral to caudal portion. Similarly, the percentageof tumors extending outside the spinal canal decreased fromthe rostral to the caudal position. These facts were explainedby Soullie et al., who reported that the length of the posteriorroots within the dural sac progressively increases from cra-nial to caudal direction [21]. They noted the lengths of theposterior intradural roots of C5, D1, D6, L1, S1, and S5 as20, 29, 45, 91, 185, and 262 mm, respectively. Spinalneurofibromas present with neck pain [22] and may havepyramidal tract signs, as in our patients whose complaintwas neck pain (four cases) and had spasticity (eight cases) orweakness (six cases). Some patients may have features ofNF-1, as noted by Goel in a study of 60 cases with C2neurofibromas, nine patients had features of NF-1 [22],which we did not encounter in our study. Preoperativeimaging revealed no single definitive sign or combinationof signs allows the definitive differentiation of neurofi-bromas from schwannomas, in the presence of the targetsign caused by central fibrocollagenous tissue and peripher-al myxomatous tissue, was described on T2-weighted im-ages or central enhancement favors the diagnosis of aneurofibroma, whereas a fascicular appearance, a thinhyperintense rim, or diffuse enhancement suggests aschwannoma [23]. The magnetic resonance imaging find-ings were utilized to determine the surgical approach,according to the tumor relationship to the cervical cord,the difference in pathology schwannoma versus neurofibromadid not make change in the way of approaching the tumor. Theposterolaterally and the anterolaterally located lesions wereaccessed using a complete or hemilaminectomy, plus or minuspartial facetectomy. The intra-tumoral decompression of thelateral part of the tumor provided an oblique trajectory toaccess the part of the lesion situated in close proximity tothe cord anteriorly. Sectioning of the denticulate ligament[24], tilting the operating table 15 to 30°, with sectioning theposterior nerve roots, as suggested by Bucci et al., [2] in allanterolateral lesions, aided in gently mobilizing the tumorfrom the contact-surface of the cord. Placement of a “T”shaped dural incision, with the horizontal limb of the “T”connecting the intra- and extra-dural components of the tumoralso facilitated access. In the case of dumb-bell tumors, ini-tially an intratumoral decompression was performed. Then,the intradural portion of the lesion was removed maintainingarachnoidal planes in the tumor-cord interface to avoid trac-tion on the cord during the handling of the extradural portion.The use of operative microscope and neurophysiologicalmonitoring facilitate tumor excision with minimal cord ma-nipulation or damage. In the present series, the anatomicalconstraints posed by the posterior approach in accessinganterolaterally located lesions were overcome by extending
the surgical corridor laterally by adopting a posterolateraltrajectory via a laminectomy and partial facetectomy, as pro-posed by Bartolomei and Crockard [6]. This approach is alsoadvantageous in gaining an early control of the vertebral artery[6]. Regarding the hazards of cervical instability followinglaminectomy with partial facetectomy [10, 25, 26], in the twoseries by George and Lot [3, 18] of cervical NST, as well asthe study by Bartolomei and Crockard [6] of bilateral C2neurofibromas, none of the patients have required fusion forcervical instability after laminectomy and partial facetectomy.At the level of C1–C2, the anterior ligaments confer an addi-tional stability to the cervical spine with less structural contri-bution from the posterior spinal column [6]. The partialpreservation of bilateral articular facets between C1 and C2also confers stability. According to Welling et al., [4]. C1–C2lateral joints have a capsule that is lax on the medial side. Mostof the movement occurs along a synovial fold present medi-ally. Removal of this part, therefore, does not lead to instabil-ity. In our patients with anterolaterally placed NST, only aunilateral partial facetectomy with preservation of more thantwo-thirds of the joint surfaces and capsule was performed andthe contralateral joint was left completely intact. Thus, nospinal fusion was required. For anterolaterally placed lesions,Verbeist [27] and George et al. [3] use an approach thatpartially removes the anterior portion of the vertebral bodyand transverse foramen but preserves the facet. The vertebralartery is mobilized from the foramen transversarium and theextraspinal tumor can also be safely excised. However, theextensive drilling and the risk of vertebral artery mobilizationfor resecting essentially the extraspinal component of thebenign lesion (that was unlikely to cause spinal cord compres-sion even in the distant future) made this approachunfavourable. In patients with lesions situated mainly anteriorto the cord (single schwannoma case in our study), the ex-treme lateral transcondylar approach was used [11–13].Though an early control of the vertebral artery, a direct visu-alization of the cervicomedullary junction and the cord-tumorinterface from a lateral aspect, and a field of view above andbelow the foramen magnum were obtained, the extensivebony and soft tissue dissection were the major deterrents toits frequent use in all dumb-bell, anteriorly placed lesions. Theextrapharyngeal approach to the upper cervical spine may bean alternative approach [14]. The transoral approach for mid-line, anterior, intradural NST [28, 29] has the risk of infectiondue to traversing through a potentially infected oral cavity[30], and is unable to access tumors extending laterally fromthe midline. During resection of the spinal NST, preservationof the anatomical integrity of the involved nerve root, al-though desirable, cannot always be achieved. This is especial-ly true in cases of large tumors where the nerve rootlets arediffusely involved by the pathological tissue, and when thetumor extends beyond the proximal pole of the dorsal rootganglion, where the roots are devoid of the arachnoidal sheath
782 Acta Neurochir (2013) 155:779–784

that usually separates them from the tumor tissue [5, 31, 32].Occasionally, the posterior sensory nerve root may be sacrificedin order to gain access to the anteriorly located tumor. In ourseries, one or more rootlets were sacrificed in every case, whilein five cases, the entire nerve root, from which the tumor arose,was sacrificed (all neurifibroma cases and 2 schwannoma cases).As C2 nerve roots are nonappendicular and therefore relativelynon-eloquent, this was not associated with any significant neu-rological deficit except an occasional mild hypoaesthesia in thesuboccipital region [16, 31, 33]. In case of eloquent nerves in thesubaxial spine, Lot and George [18] minimized postoperativedeficits by intraoperative nerve stimulation. When a responsewas recorded, the functional root was preserved even at the costof leaving some residual lesion. This procedure was not requiredin our study, since the resection of C2 root is usually notassociated with any significant sensory or motor radicular symp-toms. In three patients, a part of the extraspinal tumor extendingfar laterally beyond the intervertebral foramen was not removed.Usually this part of the tumor has neither clinical recurrence nora tumor regrowth into the spinal canal proven during outpatientclinic follow-up. Preserving the nerve roots at the cost of asubtotal tumor removal is also not associated with increasedrecurrence rates [7]. Seppala, et al. [34, 35] have reported thatof the 187 patients treated for spinal NST, in the 20 in whom lessthan total tumor excision was performed to avoid root injury, 18did not have a symptomatic recurrence even after a medianperiod of 19 years after surgery. In the patients with neurofibro-matosis, the recurrence rates in the cases of partial tumor exci-sion are higher [16, 34, 35]. We did not encounterneurofibromatosis cases in our study.
Conclusion
Upper cervical nerve sheath tumors mainly arising from C2root are unique when compared to their counterparts in otherregions of the spine in terms of their anatomical relationshipsto neighbouring structures, osseous anatomy, the biomechan-ical features of this region, and their tendency towardextradural and extraspinal spread; the surgical approachesrequired to deal with such lesions is tailored according to theirrelation to the spinal cord determined by preoperative mag-netic resonance imaging.
Conflicts of interest None.
References
1. McCormick PC, Post KD, Stein BM (1990) Intraduralextramedullary tumors in adults. Neurosurg Clin N Am 1(3):591–608
2. Bucci MN, McGillicuddy JE, Taren JA, Hoff JT (1990)Management of anteriorly located C1–C2 neurofibromata.Surg Neurol 33:15–18
3. George B, Lot G (1995) Neurinomas of the first two cervical nerveroots: a series of 42 cases. J Neurosurg 82:917–923
4. Welling B, Park YK, Al-Mefty O (1988) Primary extramedullarytumors of the craniovertebral junction. In: Dickman CA, SpetzlerRF, Sonntag VK (eds) Surgery of the craniovertebral junction, 1stedn. Theime, New York, pp 240–242
5. McCormick PC, Stein BM (1994) Spinal cord tumors in adults. In:Youmans JR (ed) Neurological Surgery, Vol. 4, 4th edn. WBSaunders Company, Philadelphia, pp. 302–323
6. Bartolomei JC, Crockard A (2001) Bilateral posterolateral ap-proach to mirror-image C-2 neurofibromas. Report of four cases.J Neurosurg 94:292–298
7. Klekamp J, Samii M (1998) Surgery of spinal nerve sheath tumorswith special reference to neurofibromatosis. Neurosurgery 42:279–290
8. Smith DA, Schmeidek HH (1980) Tumors of the nerve sheathinvolving the spine. In: Sundaresan N, Schmeidek HH, SchillerA, Rosenthal DM (eds) Tumors of the spine: diagnosis and clinicalmanagement, 1st edn. WB Saunders Company, Philadelphia,pp. 226–227
9. Yasuoka S, Okazaki H, Daube JR, MacCarty CS (1978) Foramenmagnum tumors. Analysis of 57 cases of benign extramedullarytumors. J Neurosurg 49:828–838
10. Zdeblick TA, Zou D, Warden KE (1992) Cervical stability afterforaminotomy. A biomechanical in vitro analysis. J Bone JointSurg (Am) 74:22–27
11. Banerji D, Behari S, Jain VK, Pandey T, Chhabra DK (1999)Extreme lateral transcondylar approach to the skull base. NeurolIndia 47:22–31
12. Pritz MB (1991) Evaluation and treatment of intradural tumorslocated anterior to the cervicomedullary junction by a lateralsuboccipital approach. Acta Neurochir (Wein) 113:74–81
13. Sen CN, Sekhar LN (1990) An extreme lateral approach tointradural lesions of the cervical spine and foramen magnum.Neurosurgery 27:197–204
14. Behari S, Banerji D, Trivedi P, Jain VK, Chhabra DK (2002)Anterior retropharyngeal approach to the upper cervical spine.Neurol India 49:342–349
15. Nittner K (1976) Spinal meningioma, neurinomas and neurofi-bromas and hourglass tumors. In: Vinken PJ, Bruyn GW (eds)Handbook of clinical neurology, Vol. 20. North Holland/AmericaElsevier, New York, pp. 177–322
16. Levy WJ, Latchaw J, Hahn JF, Sawhny B, Bay J, Dohn DF (1986)Spinal neurofibromas: a report of 66 cases and a comparison withmeningiomas. Neurosurg 18(3):331–334
17. Guidetti B, Spallone A (1988) Benign extramedullary tumors ofthe foramen magnum. In: Symon L (ed) Advances and technicalstandards in neurosurgery, Vol. 16. Springer, Wein, pp. 84–120
18. Lot G, George B (1997) Cervical neuromas with extradural com-ponents: surgical management in a series of 57 patients.Neurosurgery 41:813–822
19. Freeman TB, Cahill DW (1996) Tumors of the meninges, caudaequine, and spinal nerves. In: Menezes AH, Sonntag VKH (eds)Principles of spinal surgery, Vol. 2. McGraw-Hill, New York,pp. 1371–1386
20. Jinnai T, Hoshimaru M, Koyama T, Yasargil MG, Hedley-WhyteET, Brotchi J (2005) Clinical characteristics of spinal nerve sheathtumors: analysis of 149 cases. Neurosurg 56(3):510–515
21. Soulié A (1901) Nerfs rachidiens. In: Poirier P, Charpy A (eds)Traite d’anatomie humaine. Masson & Cie, Paris
22. Goel A, Muzumdar D, Nadkarni T, Desai K, Dange K, Chagla A(2008) Retrospective analysis of peripheral nerve sheath tumors ofthe second cervical nerve root in 60 surgically treated patients. JNeurosurg Spine 8(2):129–134
Acta Neurochir (2013) 155:779–784 783

23. Jee WH, Oh SN, McCauley T, Ryu KN, Suh JS, Lee JH, Park JM,Chun KA, Sung MS, Kim K, Lee YS, Kang YK, Ok IY, Kim JM(2004) Extraaxial neurofibroma, versus neurilemmomas:discimination with MRI. AJR 183:629–633
24. Tubbs RS, Salter G, Grabb PA, Oakes WJ (2001) The denticulateligament: anatomy and functional significance. J Neurosurg94:271–275
25. Cusick JF, Yoganandan N, Pintar F (1988) Biomechanics of cer-vical spine facetectomy and fixation techniques. Spine 13:808–812
26. McCormick PC (1996) Surgical management of dumb-bell tumorsof the cervical spine. Neurosurgery 38:294–300
27. Verbiest JH (1986) A lateral approach to the cervical spine-technique and indications. J Neurosurg 28:191–203
28. Crockard HA, Transoral BR (1985) transclival removal of aschwannoma anterior to the craniocervical junction. J Neurosurg62:293–295
29. Crockard HA, Sen CN (1991) Transoral approach for the manage-ment of intradural lesions at the cervicovertebral junction – areview of 7 cases. Neurosurgery 28:88–98
30. Jain VK, Behari S, Banerji D, Bhargava V, Chhabra DK (1999)Transoral decompression for craniovertebral anomalies: perioper-ative management dilemmas. Neurol India 47:188–195
31. Celli P (2002) Treatment of relevant nerve roots involved innerve sheath tumors: removal or preservation? Neurosurgery51:684–692
32. Schultheiss R, Gullotta G (1993) Resection of relevant nerve rootsin surgery of spinal neurinomas without persisting neurologicaldeficit. Acta Neurochir (Wien) 122:91–96
33. Kim P, Ebersold MJ, Onofrio BM, Quast LM (1989) Surgery ofspinal nerve schwannoma: risk of neurological deficit after resec-tion of involved root. J Neurosurg 71:810–814
34. Seppala MT, Haltia MJJ, Sankila RJ, Jaaskelainen JE, Heiskanen O(1995) Long term outcome after removal of spinal neurofibroma.J Neurosurg 82:572–577
35. Seppala MT, Haltia MJJ, Sankila RJ, Jaaskelainen JE, Heiskanen O(1995) Long term outcome after removal of spinalschwannomas. A clinicopathological study of 187 cases.J Neurosurg 83:621–626
784 Acta Neurochir (2013) 155:779–784







![Neurological Disorders - OMICS Publishing Group...Schwannomas are generally benign tumors of the peripheral nerve sheath and account for 8% of all primary intracranial tumors [1,2]](https://img.pdfslide.us/doc/110x75/5f7ff1f90cbb51524d18b287/neurological-disorders-omics-publishing-group-schwannomas-are-generally-benign.jpg)