Embed Size (px)
Citation preview
CODING AND BILLING UPDATE
Indiana Osteopathic Association 32nd Annual Winter Update
December 8, 2013
2014 Update
Presented byJoy Newby, LPN, CPC, PCS
Newby Consulting, Inc.5725 Park Plaza CourtIndianapolis, IN 46220Voice: 317.573.3960Fax: 317.705.0131
E-mail: [email protected]
This presentation was current at the time it was created and is intended to provide useful information in regard to the subject matter covered. Newby Consulting, Inc. believes the information is as authoritative and accurate as is reasonably possible and that the sources of information used in preparation of the presentation are reliable, but no assurance or warranty of completeness or accuracy is intended or given, and all warranties of any type are disclaimed.The information contained in this presentation is a general summary that explains certain aspects of the Medicare Program, but is not a legal document. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings.Any five-digit numeric Physician's Current Procedural Terminology, Fourth Edition (CPT) codes, service descriptions, instructions, modifiers, and/or guidelines are copyright 2012 (or such other date of publication of CPT as defined in the federal copyright laws) American Medical Association.For illustrative purposes, Newby Consulting, Inc. has selected certain CPT codes and service/procedure descriptions to be used in this presentation. The American Medical Association assumes no responsibility for the consequences attributable to or related to any use or interpretation of any information or views contained in or not contained in this publication.
CPT Copyright 2013 American Medical Association
4
2014 CPT Code Changes
• New vs. Established Patient– When advanced practice nurses and physician assistants
are working with physicians, they are considered as working in the exact same specialty and exact same subspecialties as the physician
5
Transitional Care Management Services - Update• Codes 99495 and 99496 are used to report transitional care
management services for new or established patients• The discharge service may not constitute the required face-
to-face visit• For Medicare patients, if the patient dies before day 30, TCM
may not be billed
CPT Copyright 2013 American Medical Association
6
Transitional Care Management Reminders
• Transitional Care Management (TCM)
– Covered and paid by Medicare
– Other insurers should also reimburse, but will depend on contract
CPT Copyright 2013 American Medical Association
7
Transitional Care Management Reminders Cont’d• The transition in care is from:
– an inpatient hospital setting (acute care, rehab, LTAC)– partial hospital– observation status in a hospital– skilled nursing facility/nursing facility
• To the patient’s community setting:– home– domiciliary– rest home– or assisted living
CPT Copyright 2013American Medical Association
8
Transitional Care Management Reminders Cont’d• 99495 Transitional Care Management Services with the
following required elements:– Communication (direct contact, telephone, electronic)
with the patient and/or caregiver within 2 business days of discharge
– Medical decision making of at least moderate complexity during the service period
– Face-to-face visit, within 14 calendar days of discharge
CPT Copyright 2013 American Medical Association
9
Transitional Care Management Reminders Cont’d• 99496 Transitional Care Management Services with the
following required elements:– Communication (direct contact, telephone,
electronic) with the patient and/or caregiver within 2 business days of discharge
– Medical decision making of high complexity during the service period
– Face-to-face visit, within 7 calendar days of discharge
CPT Copyright 2013 American Medical Association
10
Transitional Care Management Reminders Cont’d• The required contact with the patient or caregiver, as
appropriate, may be by the physician or qualified health care professional or licensed clinical staff – Within two business days of discharge is Monday through
Friday except holidays without respect to normal to normal practice hours or date of notification of discharge
– Contact may be• Direct (face-to-face)• Telephonic, or by • Electronic means
CPT Copyright 2013 American Medical Association
11
Transitional Care Management Reminders Cont’dNon-face-to-face services provided by licensed clinical staff, under the direction of the physician or other qualified health care professional, may include:• Communication (with patient, family members, guardian or
caretaker, surrogate decision makers, and/or other professionals) regarding aspects of care
• Communication with home health agencies and other community services utilized by the patient
• Patient and/or family/caretaker education to support self-management, independent living, and activities of daily living
• Assessment and support for treatment regimen adherence and medication management
• Identification of available community and health resources• Facilitating access to care and services needed by the patient
and/or familyCPT Copyright 2013
American Medical Association
12
Transitional Care Management Clarifications• The 30-day period for the TCM service begins on the day of
discharge and continues for the next 29 days. The reported date of service should be the 30th day
• The place of service reported on the claim should correspond to the place of service of the required face-to-face visit
• Providers practicing in rural health clinics (RHC) and federally qualified health clinics (FQHC) cannot report TCM codes
CPT Copyright 2013 American Medical Association
13
Transitional Care Management Clarifications Cont’d• If patient is readmitted during the 29-day TCM period, TCM
cannot be billed because a full 29-day period has not occurred.
– NCI recommends
• Reporting any billable service related to the first hospitalization
• Start a new TCM period when the patient is discharged from the 2nd admission
CPT Copyright 2013 American Medical Association
14
Surgery – Integumentary System
• There is a new Classification Method Table for Burn Estimations on page 86 of the Professional Edition of the CPT
• It is broken down by different body areas by age groups– Birth to 1 year– 1-4 years– 5-9 years– 10-14 years– 15 years– Adult
CPT Copyright 2013 American Medical Association
15
Burns, Local Treatment• 16000 - Initial treatment, first degree burn, when no more than local
treatment is required (refers to the initial treatment of first-degree burns. Follow-up treatment(s) for first-degree burns is uncommon)– Work RVUs 0.89– Non-facility Total RVUs 2.05
• 99213– Work RVUs 0.97– Non-facility Total RVUs 2.14
• 99212– Work RVUs 0.48– Non-facility Total RVUs 1.29
**2013 RVUs used in this example
CPT Copyright 2013 American Medical Association
16
1st Degree Burns
• Clinical Example CPT – 99201
– Initial office visit for a patient with a small area of sunburn requiring first aid (Dermatology)
CPT Copyright 2013 American Medical Association
17
Dressings and/or Debridement of Partial Thickness Burns• 16020 Dressings and/or debridement of partial-
thickness burns, initial or subsequent; small (less than 5% total body surface area)– Work RVUs 0.71– Total Non-facility RVUs 2.45
• 16025 Dressings and/or debridement of partial-thickness burns, initial or subsequent; medium (eg, whole face or whole extremity, or 5% to 10% total body surface area)– Work RVUs 1.74– Total Non-facility RVUs 4.41
CPT Copyright 2013 American Medical Association
18
Dressings and/or Debridement of Partial Thickness Burns Cont’d• 16030 Dressings and/or debridement of partial-thickness
burns, initial or subsequent; large (eg, more than 1 extremity, or greater than 10% total body surface area)– Work RVUs 2.08– Total Non-facility RVUs 5.50
CPT Copyright 2013 American Medical Association
19
Breast Lesion Biopsy
• Significant revisions to introductory language and 6 new codes
• Specific guidelines to direct users regarding codes for:– Breast biopsies without image guidance– Breast biopsy with imaging guidance• Imaging is bundled (not separately billable)
– Image-guided breast biopsy with placement of localization device
CPT Copyright 2013 American Medical Association
20
Musculoskeletal SystemIntroductory Guidelines• Excision of subcutaneous soft connective tissue tumors
(including simple or intermediate repair) involves the simple or marginal resection of tumors confined to subcutaneous tissue below the skin but above the deep fascia
– These tumors are usually benign and are resected without removing a significant amount of surrounding normal tissue
CPT Copyright 2013 American Medical Association
21
Musculoskeletal SystemIntroductory Guidelines Cont’d• Code selection is based on the location and size of the
tumor. It is determined by measuring the greatest diameter of the tumor plus the most narrow margin required for complete excision of the tumor, based on the physician’s judgment
• The measurement of the tumor plus margin is made at the time of the excision
CPT Copyright 2013 American Medical Association
22
Musculoskeletal SystemIntroductory Guidelines Cont’d• Extensive undermining or other techniques to close a defect
created by skin excision may require a complex repair which should be reported separately
• Dissection or elevation of tissue planes to permit resection of the tumor is included in the excision
• For excision of benign lesions of cutaneous origin see 11400-11446
CPT Copyright 2013 American Medical Association
23
Radical Resection of Soft Connective Tissue Tumors Cont’d• Although these tumors may be confined to a specific layer
(eg, subcutaneous, subfascial), radical resection may involve removal of tissue from one or more layers
• Radical resection of soft tissue tumors is most commonly used for malignant connective tissue tumors or very aggressive benign connective tissue tumors
• The term “malignant neoplasm” was ambiguous– Changed to “sarcoma” which is more refined and specific
CPT Copyright 2013 American Medical Association
24
Radical Resection of Soft Connective Tissue Tumors Cont’d• Code selection is based on size and location of the tumor
**Size is determined same as on previous slide• For radical resection of tumor(s) of cutaneous origin (eg,
melanoma), see 11600-11646
CPT Copyright 2013 American Medical Association
25
Digestive System - Endoscopy
• Significant coding changes in the endoscopy section CPT 2014
• Purpose of Changes– CMS request for review of physician work and practice
expense– Reflect technology, devices, and techniques used in
current practice– Standardize language across all three sections
CPT Copyright 2013 American Medical Association
26
Auditory System-External Ear
• 69210 Removal impacted cerumen requiring instrumentation, unilateral– Requires use of instrumentation and generally
magnification (eg, otoscope, operating microscopy to physically remove the cerumen
– Report E/M service codes when cerumen is not impacted or removal does not require instrumentation (eg, for irrigation only)
CPT Copyright 2013 American Medical Association
27
Auditory System-External Ear Cont’d
CPT Assistant April 2003, page 9 – Copyright AMA• If any one or more of the following are present, cerumen
should be considered ‘impacted’ clinically:– Visual considerations: Cerumen impairs exam of clinically
significant portions of the external auditory canal, tympanic membrane, or middle ear condition
– Qualitative considerations: Extremely hard, dry, irritative cerumen causing symptoms such as pain, itching, hearing loss, etc.
– Inflammatory considerations: Associated with foul odor, infection, or dermatitis
– Quantitative considerations: Obstructive, copious cerumen that cannot be removed without magnification and multiple instrumentations requiring physician skills”
CPT Copyright 2013 American Medical Association
28
Diagnosis Code ChangesEffective October 1, 2013• In preparation for implementation of ICD-10, no changes
were made in ICD-9 codes for fiscal year 2014• Continue working towards implementation of ICD-10 by
including complete diagnostic statements in the assessment portion of your progress notes– ICD-10 Implementation Date Remains
October 1, 2014
29
Documentation Timeliness
• Physicians/practitioners may not submit a claim to Medicare until the documentation is completed. Until the physician/practitioner completes the documentation for a service, including signature
• Physician/practitioners are expected to complete the documentation of services "during or as soon as practicable after it is provided in order to maintain an accurate medical record
– WPS interpretation “no more than a couple of days away from the service itself”
30
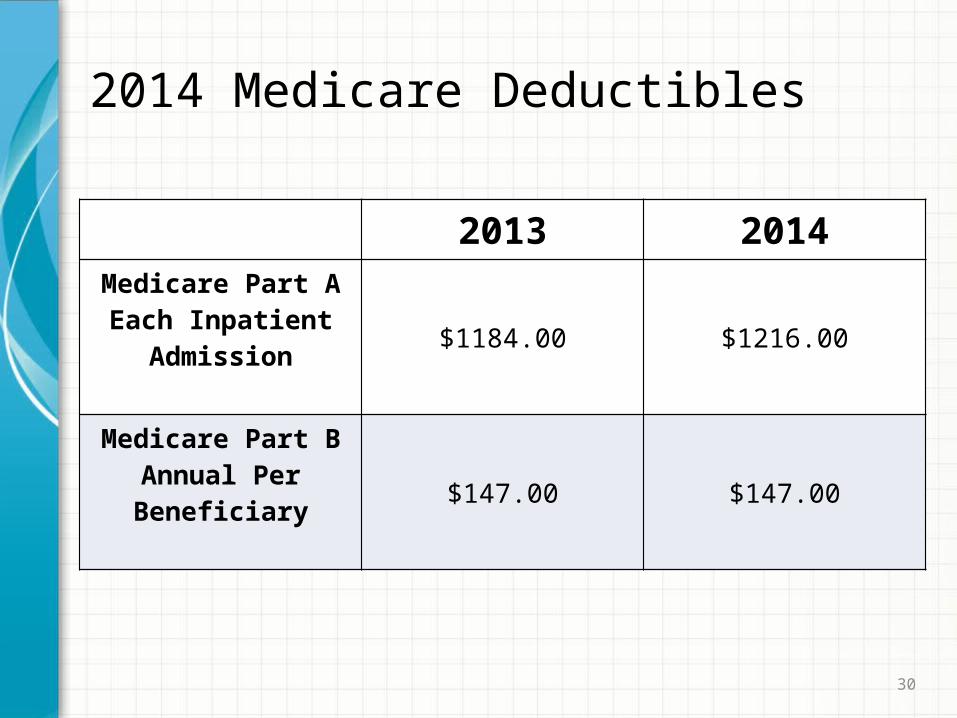
2014 Medicare Deductibles
2013 2014Medicare Part A Each Inpatient
Admission$1184.00 $1216.00
Medicare Part B Annual Per Beneficiary $147.00 $147.00
31
Medicare – 2014 Physician Fee Schedule
• Without a change in the law, the conversion factor will be reduced by 20.1 percent for services in 2014 – The CY 2014 conversion factor is $27.2006• CY 2013 conversion factor is $34.023
• The President’s budget calls for averting these cuts and finding a permanent solution to this problem
32
Ultrasound Screening Abdominal Aortic Aneurysm• An eligible beneficiary, for purposes of this covered service,
is an individual that meets the following criteria:– Has not been previously furnished AAA screening under
the Medicare program; and Is included in at least one of the following risk categories: • has a family history of an abdominal aortic aneurysm
or• is a man aged 65 to 75 who has smoked at least 100
cigarettes in his lifetime
33
Outpatient Based Clinics
• When a service is furnished in a hospital-based office, Medicare pays the hospital a “facility fee” and a payment for the physician portion of the service, which is a lower payment than if the service would have been furnished in a physician’s office – Although the physician payment is lower when the
services are furnished in a hospital, the total payment (facility fee and physician fee) is generally more than the Medicare payment if the same service was furnished in a freestanding clinic or physician office
CPT Copyright 2013 American Medical Association
34
Outpatient Based Clinics Cont’d
• In 2014, CMS will pay flat rates for Medicare visits to outpatient clinics instead of payments that vary with the severity of the patient's condition– Regardless of the “office and other outpatient E/M code”
(99201-99215) used, hospitals will only receive one flat rate for its facility fee
CPT Copyright 2013 American Medical Association
35
Primary Care Incentive Payment
• Primary care providers who provide primary care services (on or after January 1, 2011, and before January 1, 2016) will be paid, quarterly, an amount equal to 10 percent of the payment amount for such services paid under the Physician Fee Schedule– 08 (family practice)– 11 (internal medicine)– 37 (pediatrics)– 38 (geriatrics)– 50 (nurse practitioner)– 89 (certified clinical nurse specialist)– 97 (physician assistant)
CPT Copyright 2013 American Medical Association
36
Primary Care Incentive Payment Cont’d
• PCIP eligible primary care services must account for at least 60 percent of the allowed charges under Part B (excluding hospital inpatient care and emergency department visits) based on a prior two-year claims history– Office and Outpatient – 99201-99215– Nursing Facility – 99304-99340– Home Visits – 99341-99350
CPT Copyright 2013 American Medical Association
37
Primary Care Incentive Payment Cont’d
• If you are newly enrolled in Medicare (with no claims data from 2 years prior to the PCIP payment year), your PCIP eligibility will be determined using the prior year’s available claims data with no minimum time period in which you must have been enrolled in Medicare
• Due to the lag time required to process claims data, PCIP eligibility determinations for newly enrolled primary care practitioners will be delayed until after the end of the third quarter of the PCIP payment year
CPT Copyright 2013 American Medical Association
38
Primary Care Incentive Payment Cont’d
• PCIP payments will ultimately be made for all primary care services the eligible practitioners furnished throughout the full PCIP payment year, but the timing of eligibility determination will result in a single cumulative PCIP payment for newly enrolled primary care practitioners based on eligible services rendered from January 1 through December 31 of the payment year that will be made following the fourth quarter of the incentive payment year
CPT Copyright 2013 American Medical Association
39
Primary Care Incentive Payment Cont’d
• For example, for CY 2014, if you were newly enrolled in Medicare in CY 2013, Medicare will use your available claims data from CY 2013 to determine PCIP eligibility and you will receive a single cumulative PCIP payment for 1/1/2014-12/31/2014 in early 2015
40
Physician Compare Website• Currently, users can view information about approved
Medicare professionals such as – Name– Primary and secondary specialties– American board of medical specialties (ABMS) board
certification information – Practice locations– Medicare assignment status– Education, languages spoken
41
Physician Compare Website Cont’d– Satisfactorily report under the PQRS– Successful electronic prescribers– PQRS maintenance of certification incentive– Individuals that successfully participate in the medicare
EHR incentive program– Group affiliations – Hospital affiliations that link to the hospital’s profile on
hospital compare as available• For group practices, users can also view group practice
names, specialties, practice locations, Medicare Assignment status, and affiliated professionals
42
Physician Compare Website Cont’d
• Some time in 2014 CMS will begin publicly reporting Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) data for – group practices of 100 or more eligible professionals
reporting data in 2013 under the GPRO – ACOs participating in the Shared Savings Program.
43
Electronic Prescribing Incentive
• Electronic Prescribing Incentive– 1.0% in 2011 – Paid 3rd quarter 2012– 1.0% in 2012 – Paid 3rd quarter 2013– 0.5% in 2013 – Paid 3rd quarter 2014
• Successful prescriber– 2011 – Submitted at least 25 e-Rx events in 2011– 2012 – Submits at least 25 e-Rx events in 2012– 2013 – Submits at least 25 e-Rx events in 2013– 2014 – Submits at least 25 e-Rx events in 2014
44
e-Rx Payment Adjustments
• Physicians who did not successfully report the e-Rx measure in 2012 (25) or during the first 6 months of 2013 (10) will receive a 2.0 percent penalty for all payments made on the physician fee schedule for 2014 dates of service– Some exceptions apply, but had to have been requested
no later than 6/30/2013• No eRx payment adjustments are scheduled past 2014
45
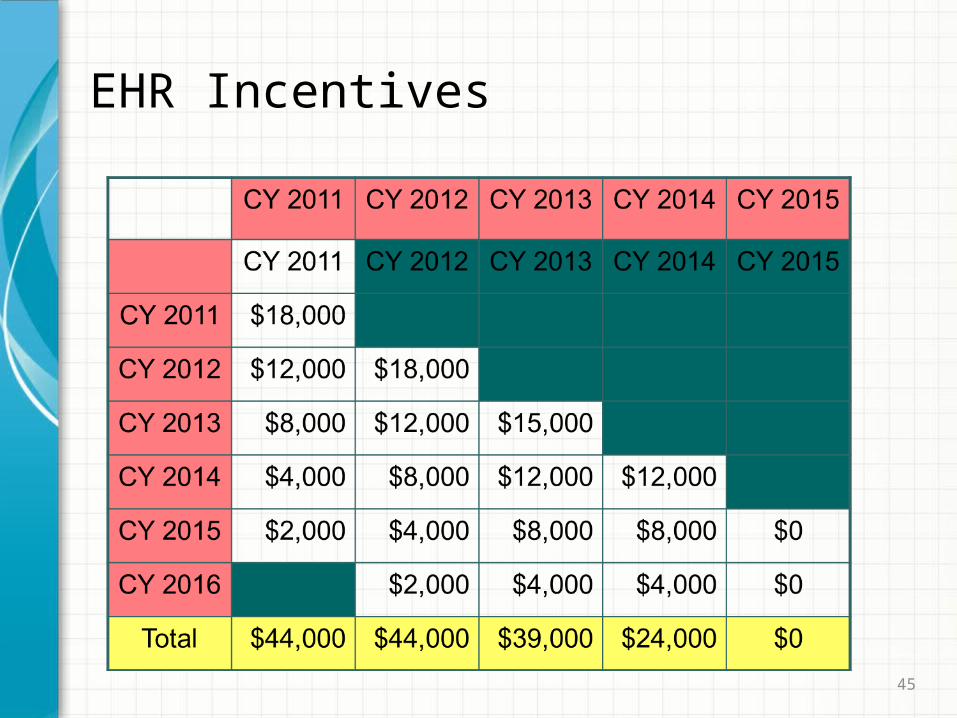
EHR Incentives
46
EHR Payment Adjustments
• ARRA - Physicians who do not adopt/use a certified system will face reduction in their Medicare fee schedule – -1% in 2015
– -2% in 2016
– -3% in 2017 and beyond
– HHS may increase penalties beginning in 2019, but penalties cannot exceed -5%
47
Physician Quality Reporting System
• The Physician Quality Reporting System (PQRS) is a voluntary quality reporting program that provides an incentive payment to practices whose eligible professionals (identified on claims by their individual National Provider Identifier [NPI]) satisfactorily report data on quality measures for covered Medicare Physician Fee Schedule (PFS) services furnished to Medicare Part B Fee-For-Service (FFS) beneficiaries
48
PQRS Incentive and Penalty
• For 2014, eligible professionals may earn an incentive payment of 0.5 percent of their total
• Penalties for not successfully reporting PQRS measures begins in 2015
– 1.5% payment adjustment for 2015 (Based on 2013 reporting)
– 2.0% payment adjustment for 2016 and after (2016 adjustment is based on 2014 reporting)
49
PQRS Reporting
• 2 Measure options– Individual measures– Measures group
• 4 Reporting Options– Claims based – Registry– Direct EHR Vendor
– EHR data submission vendor
50
PQRS Reporting Cont’d
• 2 Reporting Periods– 12 months (January 1, 2014 through December 31, 2014)
Claims must be submitted no later than February 28, 2015
– 6 months (July 1, 2014 through December 31, 2014) Must be submitted no later than February 28, 2015 (Measures Group registry reporting only)
51
PQRS Reporting 2014National Quality Strategy • Effective Clinical Care– Controlling High Blood Pressure: Percentage of patients
18-85 years of age who had a diagnosis of hypertension and whose blood pressure was adequately controlled (<140/90 mmHg) during the measurement period
52
PQRS Reporting 2014National Quality Strategy Cont’d • Patient Safety– Documentation of Current Medications in the Medical
Record: Percentage of visits for patients aged 18 years and older for which the eligible professional attests to documenting a list of current medications using all immediate resources available on the date of the encounter.
– This list must include• ALL known prescriptions, over-the-counters, herbals,
and vitamin/mineral/dietary (nutritional) supplements• AND must contain the medications’ name, dosage,
frequency and route of administration.
53
National Quality Strategy Cont’d
• Community/Population Health– Preventive Care and Screening: Tobacco Use:– Screening and Cessation Intervention: Percentage of
patients 18 years and older who were screened for– tobacco use one or more times within 24 months AND– who received cessation counseling intervention if
identified as a tobacco user
54
National Quality Strategy Cont’d
• Communication and Care Coordination– Closing the referral loop: receipt of specialist report:
Percentage of patients with referrals, regardless of age, for which the referring provider receives a report from the provider to whom the patient was referred
55
National Quality Strategy Cont’d
• Person and Caregiver-Centered Experience and Outcomes– Urinary Incontinence: Plan of Care for Urinary
Incontinence in Women• Aged 65 Years and Older: Percentage of female
patients aged 65 years and older with a diagnosis of urinary incontinence with a documented plan of care for urinary incontinence at least once within 12 months
56
National Quality Strategy Cont’d
• Efficiency and Cost Reduction– Antibiotic Treatment for Adults with Acute Bronchitis:
Avoidance of Inappropriate Use: Percentage of adults 18 through 64 years of age with a diagnosis of acute bronchitis who were not prescribed or dispensed an antibiotic prescription on or 3 days after the episode
57
PQRS Reporting in 2014 – Individual Physician• Claims - For the 12-month 2014 PQRS incentive reporting
period– Report at least 9 measures covering at least 3 National
Quality Strategy domains, and report each measure for at least 50 percent of the Medicare Part B FFS patients seen during the reporting period to which the measure applies
58
PQRS Reporting in 2014 – Individual Physician Cont’d• Qualified Registry – For the 12-month 2014 PQRS incentive reporting period• Report at least 9 measures covering at least 3 of the
National Quality Strategy domains report each measure for at least 50 percent of the eligible professional’s Medicare Part B FFS patients seen during the reporting period to which the measure applies• Report at least 1 measures group and report each
measures group for at least 20 patients, a majority of which much be Medicare Part B FFS patients
59
PQRS Reporting in 2014 – Individual Physician Cont’d• Qualified Registry– For the 6-month 2014 PQRS incentive reporting period,
report at least 1 measures group and report each measures group for at least 20 patients, a majority of which much be Medicare Part B FFS patients
60
PQRS Reporting in 2014 – Individual Physician Cont’d• EHR Direct Product– For the 12-month 2014 PQRS incentive reporting period,
report 9 measures covering at least 3 of the National Quality Strategy domains• If an eligible professional's certified EHR technology
(CEHRT) does not contain patient data for at least 9 measures covering at least 3 domains, then the eligible professional must report the measures for which there is Medicare patient data
61
PQRS Reporting in 2014 – Individual Physician Cont’d• EHR Data Submission Vendor– For the 12-month 2014 PQRS incentive reporting period,
report 9 measures covering at least 3 of the National Quality Strategy domains • If an eligible professional's CEHRT does not contain
patient data for at least 9 measures covering at least 3 domains, then the eligible professional must report the measures for which there is Medicare patient data. An eligible professional must report on at least 1 measure for which there is Medicare patient data
62
PQRS Reporting in 2014 – Group Practice
• Reporting mechanisms for group practices. With the exception of a group practice who wishes to participate in the PQRS using the certified survey vendor mechanism (as specified in paragraph (h)(4)(v) of this section), a group practice must report information on PQRS quality measures identified by CMS in one of the following reporting mechanisms– Web interface. For 2013 and subsequent years, reporting
PQRS quality measures to CMS using a CMS web interface in the form and manner and by the deadline specified by CMS
63
PQRS Reporting in 2014 – Group Practice Cont’d• Web interface
– For 2014 and subsequent years, reporting PQRS quality measures to CMS using a CMS web interface in the form and manner and by the deadline specified by CMS• For the 12-month 2014 PQRS incentive reporting period, for a
group practice of 25 to 99 eligible professionals, report on all measures included in the web interface and populate data fields for the first 218 consecutively ranked and assigned beneficiaries in the order in which they appear in the group’s sample for each module or preventive care measure
• If the pool of eligible assigned beneficiaries is less than 218, then report on 100 percent of assigned beneficiaries
64
PQRS Reporting in 2014 – Group Practice Cont’d• Web interface
– For the 12-month 2014 PQRS incentive reporting period, for a group practice of 100 or more eligible professionals, report on all measures included in the web interface and populate data fields for the first 411 consecutively ranked and assigned beneficiaries in the order in which they appear in the group’s sample for each module or preventive care measure
– If the pool of eligible assigned beneficiaries is less than 411, then report on 100 percent of assigned beneficiaries. In addition, for the 12-month 2014 PQRS incentive reporting period, the group practice must report all CG CAHPS survey measures via a CMS-certified survey vendor, and report at least 6 measures covering at least 2 of the National Quality Strategy domains using a qualified registry, direct EHR product, or EHR data submission vendor
65
PQRS Reporting in 2014 – Group Practice Cont’d• Registry– For 2013 and subsequent years, reporting on PQRS
quality measures to a qualified registry in the form and manner and by the deadline specified by the qualified registry selected by the eligible professional
– The selected registry must submit information, as required by CMS, for covered professional services furnished by the eligible professional during the applicable reporting period to CMS on the eligible professional’s behalf
66
PQRS Reporting in 2014 – Group Practice Cont’d• Registry– For the 12-month 2014 PQRS incentive reporting period,
for a group practice of 2 or more eligible professionals, report at least 9 measures, covering at least 3 of the National Quality Strategy domains and report each measure for at least 50 percent of the group practice’s Medicare Part B FFS patients seen during the reporting period to which the measure applies
67
PQRS Reporting in 2014 – Group Practice Cont’d• Direct EHR product– For 2014 and subsequent years, reporting PQRS quality
measures to CMS by extracting clinical data using a secure data submission method, as required by CMS, from a direct EHR product by the deadline specified by CMS for covered professional services furnished by the eligible professional during the applicable reporting period
– For the 12-month 2014 PQRS incentive reporting period, for a group practice of 2 or more eligible professionals, report 9 measures covering at least 3 of the National Quality Strategy domains
68
PQRS Reporting in 2014 – Group Practice Cont’d• Direct EHR product– If a group practice's CEHRT does not contain patient data
for at least 9 measures covering at least 3 domains, then the group practice must report the measures for which there is Medicare patient data. A group practice must report on at least 1 measure for which there is Medicare patient data
69
PQRS Reporting in 2014 – Group Practice Cont’d• EHR data submission vendor– For 2014 and subsequent years, reporting PQRS quality
measures to CMS by extracting clinical data using a secure data submission method, as required by CMS, from an EHR data submission vendor product by the deadline specified by CMS for covered professional services furnished by the eligible professional during the applicable reporting period
70
PQRS Reporting in 2014 – Group Practice Cont’d• EHR data submission vendor– For the 12-month 2014 PQRS incentive reporting period,
for a group practice of 2 or more eligible professionals, report 9 measures covering at least 3 of the National Quality Strategy domains. If a group practice's CEHRT does not contain patient data for at least 9 measures covering at least 3 domains, then the group practice must report the measures for which there is Medicare patient data. A group practice must report on at least 1 measure for which there is Medicare patient data
71
PQRS Reporting in 2014 – Group Practice Cont’d• Certified survey vendors– For 2014 and subsequent years, reporting CAHPS survey
measures to CMS using a vendor that is certified by CMS for a particular program year to transmit survey measures data to CMS. Group practices that elect this reporting mechanism must select an additional group practice reporting mechanism in order to meet the criteria for satisfactory reporting for the incentive payments
72
PQRS Reporting in 2014 – Group Practice Cont’d• Certified survey vendor– For the 12- month 2014 PQRS incentive reporting period,
for a group practice of 25 or more eligible professionals, report all CG CAHPS survey measures via a CMS-certified survey vendor, and report at least 6 measures covering at least 2 of the National Quality Strategy domains using a qualified registry, direct EHR product, EHR data submission vendor, or GPRO web interface
73
Maintenance of Certification Program Incentive• Physicians who are incentive eligible for 2014 PQRS can receive
an additional 0.5% incentive payment when Maintenance of Certification Program Incentive requirements have been met
• This physician-only incentive will be paid at the same time as the 2014 PQRS incentive for those physicians who qualify
• Physicians cannot receive more than one additional 0.5% Maintenance of Certification Program Incentive, even if they complete a Maintenance of Certification Program in more than one specialty
• Maintenance of Certification Program entities will manage the program as well as submit 2014 information on behalf of physicians by February 27, 2015
74
Value Based Payment Modifier
• §3007 of the Affordable Care Act mandated that, by 2015, CMS begin applying a value modifier under the Medicare Physician Fee Schedule (MPFS).
• Applicable to groups with primary care providers with a total of 100 or more physicians
– Groups of 100 or more without PCPs – must report PQRS
• By 2017, the Value-based Payment Modifier is to be applied to all physicians who bill Medicare for services provided under the physician fee schedule.
75
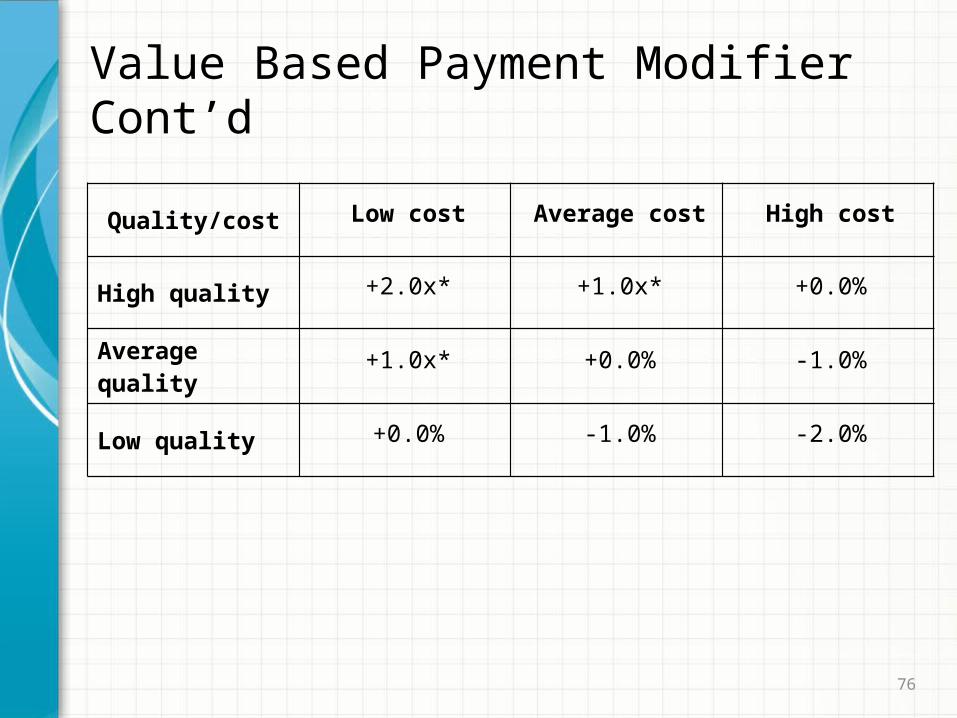
Value Based Payment Modifier Cont’d
• CMS will assess both quality of care furnished and the cost of that care under the Medicare Physician Fee Schedule
• Must develop a quality and cost composite for each group of physicians
• An adjustment to every claim paid under the physician fee schedule
• Must be budget neutral – Negative payment adjustments will be divided among the groups with positive payment adjustments
• * Groups of physicians eligible for an additional +1.0x if reporting Physician Quality Reporting System quality measures and average beneficiary risk score is in the top 25 percent of all beneficiary risk scores.
76
Value Based Payment Modifier Cont’d
Quality/cost Low cost Average cost High cost
High quality +2.0x* +1.0x* +0.0%
Average quality +1.0x* +0.0% -1.0%
Low quality +0.0% -1.0% -2.0%
77
Value Based Payment Modifier Cont’d
• In calendar year 2013, medical practice groups of 100 or more eligible professionals (all of whom file Medicare Fee-For-Service claims under the physician fee schedule using a single tax identification number) must register and participate in PQRS as a group in order to avoid a negative one percent payment adjustment (in 2015) under the value modifier.
78
Value Based Payment Modifier Cont’d
• All physicians who participate in Fee-For-Service Medicare will be impacted by CMS’ emphasis on reporting quality data through PQRS and by 2017 will be affected by the value modifier
79
Chronic Care Management
• CY 2015, CMS will establish a separate payment under the PFS for chronic care management services furnished to patients with multiple chronic conditions that are expected to last at least 12 months or until the death of the patient, and that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline
• Chronic care management services to beneficiaries with multiple (that is, two or more) chronic conditions are not adequately reflected in the existing E/M codes
– Not applicable for patients in nursing facility or receiving hospice services
80
Chronic Care Management Cont’d• Furnishing care management to beneficiaries with multiple
chronic conditions requires multidisciplinary care modalities that involve:
– regular physician development and/or revision of care plans
– subsequent reports of patient status
– review of laboratory and other studies
– communication with other health professionals not employed in the same practice who are involved in the patient’s care
– integration of new information into the care plan; and/or adjustment of medical therapy
81
Chronic Care Management Cont’dCMS will develop standards for furnishing chronic care management services to ensure that the physicians and practitioners who bill for these services have the capability to provide them • The practice must be using a certified Electronic Health Record
(EHR) for beneficiary care that meets the most recent HHS regulatory standard for meaningful use
• Must be able to provide 24-hour- a-day, 7-day- a-week access to address a patient’s acute chronic care needs
• Patient and caregiver would be provided with a means to make timely contact with health care providers in the practice to address the patient’s urgent chronic care needs regardless of the time of day or day of the week
82
Chronic Care Management Cont’d• The practice must employ one or more advanced practice
registered nurses or physicians assistants whose written job descriptions indicate that their job roles include and are appropriately scaled to meet the needs for beneficiaries receiving services in the practice who require chronic care management services furnished by the practice– To bill for “incident to” services, practitioners should
follow all the usual “incident to” requirements except when furnishing services outside of normal business hours under conditions that meet the requirements for the general supervision exception
83
Chronic Care Management Cont’d• All practitioners, including advanced practice registered
nurses or physicians assistants, involved in the furnishing of chronic care management services must have access at the time of service to the beneficiary's EHR that includes all of the elements necessary to meet the most recent HHS regulatory standard for meaningful use. – This includes any and all clinical staff furnishing after
hours care to ensure that the chronic care management services are available with this level of EHR support in the practice or remotely through a Virtual Private Network (VPN), a secure website, or a health information exchange (HIE) 24 hours per day and 7 days a week
84
Chronic Care Management Cont’d
• Continuity of care with a designated practitioner or member of the care team with whom the patient is able to get successive routine appointments
• Care management for chronic conditions including • systematic assessment of patient’s medical, functional,
and psychosocial needs• system-based approaches to ensure timely receipt of all
recommended preventive care services• medication reconciliation with review of adherence and
potential interactions• oversight of patient self-management of medications.
85
Chronic Care Management Cont’d
• In consultation with the patient, caregiver, and other key practitioners treating the patient, the practitioner furnishing chronic care management services should create a patient-centered plan of care document to assure that care is provided in a way that is congruent with patient choices and values
86
Chronic Care Management Cont’d
• A plan of care is based on a – Physical– Mental– Cognitive– Psychosocial– Functional and environmental (re)assessment– An inventory of resources and supports
87
Chronic Care Management Cont’d
• It is a comprehensive plan of care for all health issues. It typically includes, but is not limited to, the following elements: – problem list, expected outcome and prognosis– measurable treatment goals– symptom management– planned interventions– medication management– community/social services ordered, how the services of agencies
and specialists unconnected to the practice will be directed/coordinated
– identify the individuals responsible for each intervention– requirements for periodic review and, when applicable, revision, of
the care plan
88
Chronic Care Management Cont’d
• The provider should seek to reflect a full list of problems, medications and medication allergies in the electronic health record to form the care plan, care coordination, and ongoing clinical care
89
Chronic Care Management Written Protocols• The practice must be able to demonstrate the use of written
protocols by staff participating in the furnishing of services that describe: – The methods and expected “norms” for furnishing each
component of chronic care management services furnished by the practice
– The strategies for systematically furnishing health risk assessments to identify all beneficiaries eligible and who may be willing to participate in the chronic care management services
90
Chronic Care Management Written Protocols Cont’d
– The procedures for informing eligible beneficiaries about chronic care management services and obtaining their consent
– The steps for monitoring the medical, functional and social needs of all beneficiaries receiving chronic care management services
– System based approaches to ensure timely furnishing of all recommended preventive care services to beneficiaries
– Guidelines for communicating common and anticipated clinical and non-clinical issues to beneficiaries
– Care plans for beneficiaries post-discharge from an emergency department or other institutional health care setting, to assist beneficiaries with follow up visits with clinical and other suppliers or providers, and in managing any changes in their medications
91
Chronic Care Management Written Protocols Cont’d
– A systematic approach to communicate and electronically exchange clinical information with and coordinate care among all service providers involved in the ongoing care of a beneficiary receiving chronic care management services
– A systematic approach for linking the practice and a beneficiary receiving chronic care management services with long-term services and supports including home and community-based services
– A systematic approach to the care management of vulnerable beneficiary populations such as racial and ethnic minorities and people with disabilities
92
Chronic Care Management Written Protocols Cont’d– Patient education to assist the beneficiary to self-manage
a chronic condition that is considered at least one of his/her chronic conditions. These protocols must be reviewed and updated as is appropriate based on the best available clinical information at least annually
CPT Copyright 2013 American Medical Association
93
Chronic Care Management Coding and Coverage• If the AMA does not revise the Complex Chronic Care
Coordination Care codes to meet Medicare’s coverage requirements, CMS plans to create a separately payable alphanumeric G-code.– GXXX1 Chronic care management services furnished to
patients with multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient, that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline; 20 minutes or more; per 30 days
• Typically, CMS will expect that the 20 minutes or more of chronic care management services to be provided by clinical staff directed by a physician or other qualified health care professional
94
Chronic Care Management Coding and Coverage– At least 20 minutes of chronic care management services
must be provided during the 30- day period– Time of less than 20 minutes over the 30-day period may
not be rounded up to 20 minutes in order to bill for these services
• For purposes of meeting the 20-minute requirement, the practitioner could count the time of only one clinical staff member for a particular segment of time, and could not count overlapping intervals such as when two or more clinical staff members are meeting about the patient
95
Chronic Care Management Coding and Coverage Cont’d• Chronic care management services would include
transitional care management services (CPT 99495, 99496), home health care supervision (HCPCS G0181), and hospice care supervision (HCPCS G0182). If furnished, to avoid duplicate payment, we proposed that these services may not be billed separately during the 30 days for which GXXX1 is billed
• For similar reasons, we proposed that GXXX1 cannot be billed separately if ESRD services (CPT 90951-90970) are billed during the same 30 days
96
Chronic Care Management Coding and Coverage Cont’d• CMS will pay only one claim for chronic care management
services billed per beneficiary at the conclusion of each 30-day period
• All of CMS’ proposed chronic care management services that are relevant to the patient must be furnished to bill for a 30-day period
• If a face-to-face visit is provided during the 30-day period by the practitioner who is furnishing chronic care management services, we proposed that the practitioner should report the appropriate evaluation and management code in addition to billing for chronic care management
97
Chronic Care ManagementBeneficiary Agreement• Before the practitioner can furnish or bill for these services,
the eligible beneficiary must be informed about the availability of the services from the practitioner and provide his or her written agreement to have the services provided, including agreeing to the electronic communication of the patient’s information with other treating providers as part of care coordination.
98
Chronic Care ManagementBeneficiary Agreement Cont’d• This would include a discussion with the patient, and
caregiver when applicable, about what chronic care management services are, how these services are accessed, how the patient’s information will be shared among other providers in the care team, and that cost-sharing applies to these services even when they are not delivered face-to-face in the practice.
99
Chronic Care ManagementBeneficiary Agreement Cont’d• To bill for the services, the practitioner would be required to
document in the patient’s medical record that all of the chronic care management services were explained and offered to the patient, noting the patient’s decision to accept these services. Also, a written or electronic copy of the care plan is required to be provided to the beneficiary, and the provision of the plan to the patient must also be recorded in the beneficiary’s electronic medical record
CPT Copyright 2013 American Medical Association
100
Chronic Care Management Recommendation• Recommendation for a practitioner to furnish an AWV or
IPPE to a beneficiary prior to billing for chronic care management services furnished to that same beneficiary. As an alternative, a practitioner who meets the practice standards that will be established to bill for chronic care management services may initiate services with an eligible beneficiary as a part of an AWV, an IPPE, or a comprehensive E/M visit
Thanks for inviting me to your meetings for 22 years
It has been a privilege to be a presenter.
Happy Holidays!See you in 2014!