Embed Size (px)
Citation preview


Bypasses for a Billion: improving healthcare availability for allLearnings from India
Bypasses for a Billion: improving healthcare availability for allLearnings from India
Managing DirectorHealthBridge Advisors Pvt. Ltd, India
Dr. Adheet Gogate
Learnings from IndiaLearnings from India

CONTENTS
Overview of healthcare in India
The Indian hospital free market
Winning strategies
Implications for South Africa

Overall Healthcare market
In Billion US $; 2012E
Total
80
Others
13
Pharma
10
Health delivery
57
THOUGH INDIA IS LARGE, ITS HOSPITAL INDUSTRY IS RELATIVELY SMALL…
The 2nd populous country in the world with the 7th largest area
• Population: 1.21 billion• Population growth rate: 1.3%• Sex ratio: 943• Population density: 382 per sq.km
2011
GEOGRAPHICAL AREA - 3, 287, 263 sq.km
DEMOGRAPHICS
delivery
Care delivery sector
In Billion US $
2020(E)
160
2012
57
2002
18
Source: Census india 2011, : IDFC Securities Hospital Sector November 2010, Hospital Market – India by Research on India, Aranca Research; World Bank data 2012; HBA Analysis
• GDP – 1.842 trillion US $• GDP/ Capita – 1489.24 US $• Purchasing Power Parity adjusted per
Capita – 3876 US $
• Population density: 382 per sq.km
2012ECONOMYHBA estimates

THE GROWTH IN INDIA’S HOSPITAL INDUSTRY IS DRIVEN BY STRONG, RESILIENT FACTORS
GDP growth
Trillion US $ 5.6
2020(E)2011
1.7
2001
0.5
Rise in NCDs
Multiple drivers creating a positive tide….
Prevalence rate as percentage of population
3.3
5
2.8
3.72005
2015(E)
Growing middle class
Income group in percent
6%
13%
34%
2009-10
2020(E)
Too little capacity
Beds per 10,000 population
China
36
S.Africa
28
USA
30
13
35
India WHO std
Source: Census india 2011, Macro economic outlook 2020, KPMG report, McKinsey report, IDFC Securities Hospital Sector November 2010, Hospital Market – India by Research on India, Aranca Research; PWC report; HBA Analysis;
India will have to build between 1.5 – 3
million beds in the next decade
India will have to build between 1.5 – 3
million beds in the next decade
CHD Diabtetes
3.32.8
0.20
Cancer
0.18
2015(E)
2001-02
2010

UNUSUAL FOR A COUNTRY OF THIS SIZE AND DIVERSITY, HEALTHCARE IS LARGELY PAID FOR OUT OF POCKET
Total healthcare spend very low…
% of GDP
17.9
9.7
Public
Private
2011
… with most people uninsured
13%
2%
Private insurance
Uninsured
Public insuranceImpact
% of Services delivered by value
80%
Public
Private
Percent; 2012
100% = 1.2 Billion people
Source: World Bank data, PWC report, Economic & Political Weekly 2004, HBA analysis, Centrum Healthcare sector October, 2010, KPMG analysis
USA China
1.2
India
3.95.2
2.3
2.92.7
8.2
85%2012
20%
Ability to access & consume Healthcare
dependant on the ability to pay
Ability to access & consume Healthcare
dependant on the ability to pay
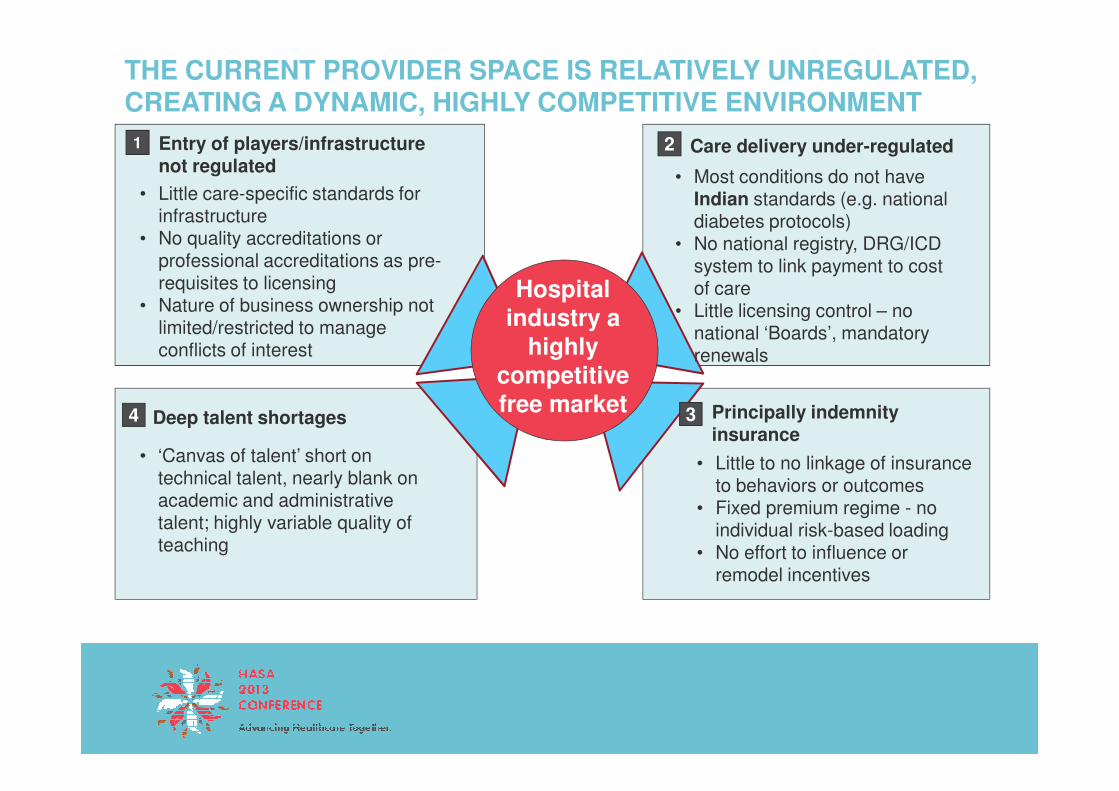
THE CURRENT PROVIDER SPACE IS RELATIVELY UNREGULATED, CREATING A DYNAMIC, HIGHLY COMPETITIVE ENVIRONMENT
Hospital industry a
highly competitive free market
Entry of players/infrastructure not regulated
1
• Little care-specific standards for infrastructure
• No quality accreditations or professional accreditations as pre-requisites to licensing
• Nature of business ownership not limited/restricted to manage conflicts of interest
Care delivery under-regulated2
• Most conditions do not have Indian standards (e.g. national diabetes protocols)
• No national registry, DRG/ICD system to link payment to cost of care
• Little licensing control – no national ‘Boards’, mandatory renewals
free market Principally indemnity insurance
3
• Little to no linkage of insurance to behaviors or outcomes
• Fixed premium regime - no individual risk-based loading
• No effort to influence or remodel incentives
Deep talent shortages4
• ‘Canvas of talent’ short on technical talent, nearly blank on academic and administrative talent; highly variable quality of teaching
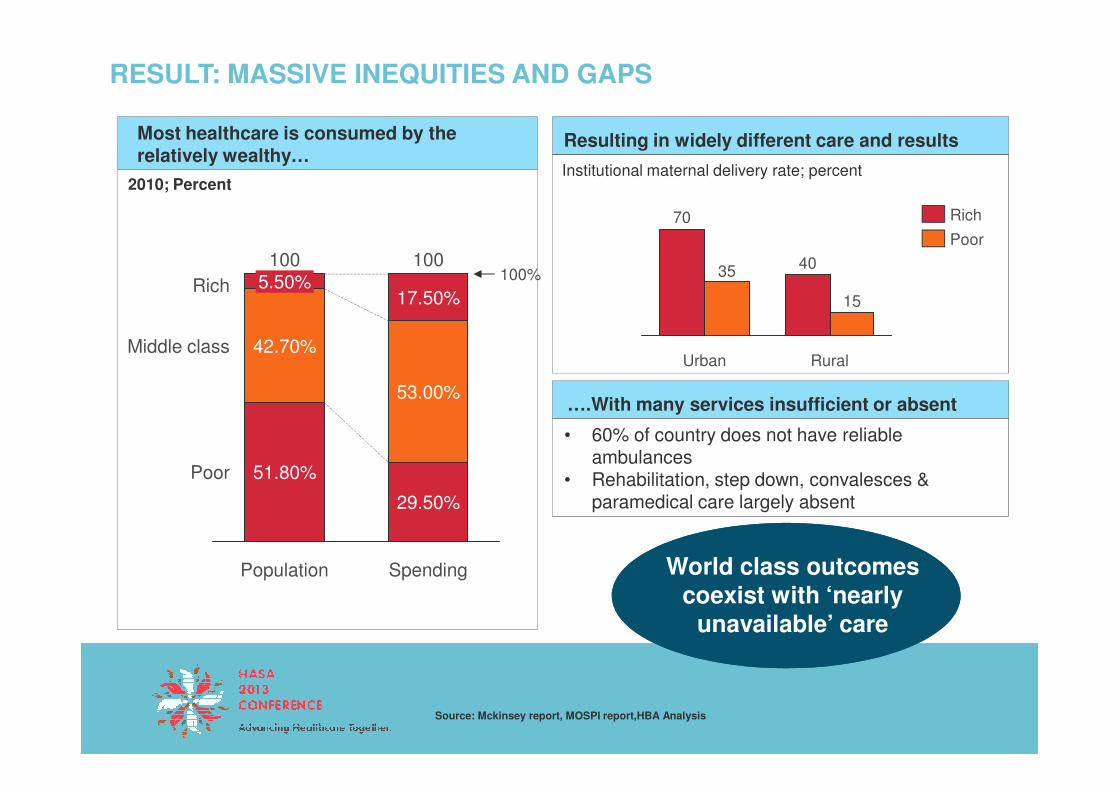
RESULT: MASSIVE INEQUITIES AND GAPS
….With many services insufficient or absent
Most healthcare is consumed by the relatively wealthy…
2010; Percent
Resulting in widely different care and results
Rural
15
40
Urban
35
70
Poor
Rich
Institutional maternal delivery rate; percent
Rich
Middle class 42.70%
5.50%100
100%100
17.50%
53.00%
Source: Mckinsey report, MOSPI report,HBA Analysis
….With many services insufficient or absent
• 60% of country does not have reliable ambulances
• Rehabilitation, step down, convalesces & paramedical care largely absent
World class outcomes coexist with ‘nearly
unavailable’ care
Population Spending
Poor 51.80%
29.50%
53.00%

CONTENTS
Overview of healthcare in India
The Indian hospital free market
Winning strategies
Implications for South Africa

DESPITE THESE PROBLEMS, THE INDIAN HEALTHCARE SYSTEM IS AN EXTRAORDINARY FREE-MARKET…
Opportunity
Segment
Competitive, diverse provider landscape• Plethora of business philosophies & business models - both
private & public• Variety of players competing in overlapping segments
Providers at (nearly) all price points• Premier hospitals (JCI standards) to low cost players in same
market – even in same neighborhood!• Variety of scale and capabilities
Competitive response
Pop. In Millions
Private spend (US$ Bn)
Poor 624
Year 2010
14.7
• Variety of scale and capabilities• Multiple price-service-quality alternatives at most price points
(‘middle class upwards’)
Supported by made in (and for) India suppliers and business models• Deep bench of domestic providers and manufacturers in all
areas• Innovative business models to keep prices low (e.g. reagent
rental)
Low, middle & upper middle
512 26.5
Rich 66 8.7
Source: McKinsey report, MOSPI report; HBA Analysis

EYE CARE : AS A RESULT, A RICH DIVERSITY OF PLAYERS HAS EMERGED…
Premium / upscale play
• Smaller, boutique
“For the poor” play
Expertise play
Mid-market+ SCALE play
Eye care system
• Mid to large • Large scale • Standardized • Comprehensive Configu-
Examples
• Smaller, boutique with 3-5 doctors
• Focused capabilities
• Luxury experience
• Mid to large scale with younger doctors
• Varied
• Basic
• Large scale with heavy technology
• World class
• Budget
• Standardized centers
• Focused on profitability
• Budget
• Comprehensive system
• Comprehensive
• Margin on all patients
• Socialized • Cross subsidy • Volume play • Cross subsidy
Configu-ration
Capabilities & Experience
Model

AS AN INDUSTRY, THESE PLAYERS HAVE ACHIEVED VERY IMPRESSIVE RESULTS
Cost at all price points…
… using innovative new techniques
With world-class results
Cataract surgery price; US$
SE/ Aravindfolding
300
SE/ Aravind Conventional
100
• Lowest cost surgeries done indigenously developed SICS techniques that have a far shorter learning curve
% complication rates for senior surgeons
Conventional Low cost SICS
1.0 1.1
USA 3500
TypicalNHS
1200
Vasan ’package’
550
curve
• Ability to do truly difficult surgeries. eg: vitrectomies, oculoplasties, prematurity retinopathy
Source: International federation of health plans, comparative price report; British Journal of Ophthalmology; Web reportsBr J Ophthalmol 2005;89:1073–1074. doi: 10.1136/bjo.2005.068213J Cataract Refract Surg 2012; 38:1360–1369 Q 2012 ASCRS and ESCRS
Conventional phaco
Low cost SICS technique
• SICS failure rates for younger surgeons less than a third for phaco – due to far shorter learning curve
• Very low infection rates, over 95% restoration of visual acuity to 6/18 or above

CENTERS OF EXCELLENCE SUCH AS TATA MEMORIAL(CANCER) CENTER ALSO EXIST IN THE PUBLIC SECTOR
Tata Memorial Centre: a first among equals
A unique business model
• 60 year old, 550 bedded cancer treatment & research hospital
• Among the first hospitals to move to a Disease Management Group(DMG) approach for treatment
• Provides own teaching, research
• Patients in higher payment classes subsidize poorer ones; telescopic pricing used to spread benefits in all departments
• “Business + economy” OPD with shared ICU/ OT’s keeps operating costs low
Source: TMH Annual Report
• Provides own teaching, research and care opportunities with full-suite, in-house services
• Pioneer in the field of tissue banking in India & is the only hospital in India to have an ISO 9001:2000 certified tissue bank .
• Part socialized – part paid/; staff + capex government paid; consumables charged
• Rigorous cost control (e.g. re-using consumables)
Nearly 70% of patients are
treated totally for free or at
subsidized prices
Nearly 70% of patients are
treated totally for free or at
subsidized prices
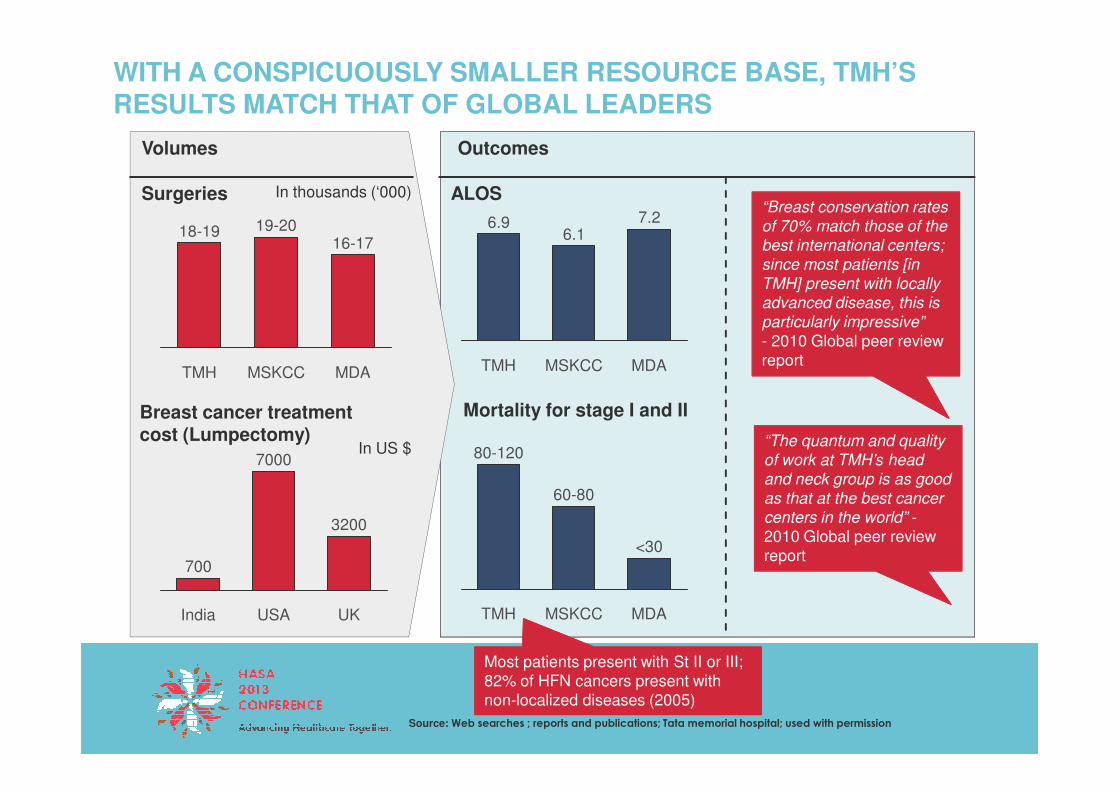
WITH A CONSPICUOUSLY SMALLER RESOURCE BASE, TMH’S RESULTS MATCH THAT OF GLOBAL LEADERS
Volumes
Surgeries
Outcomes
ALOS
16-17
MSKCC
19-20
TMH
18-19
MDA MDA
7.2
MSKCC
6.1
TMH
6.9
In thousands (‘000)“Breast conservation rates
of 70% match those of the
best international centers;
since most patients [in
TMH] present with locally
advanced disease, this is
particularly impressive”
- 2010 Global peer review report
Breast cancer treatment cost (Lumpectomy)
Mortality for stage I and II
700
7000
USA
3200
UKIndia
In US $
Source: Web searches ; reports and publications; Tata memorial hospital; used with permission
MDA
<30
MSKCC
60-80
TMH
80-120
Most patients present with St II or III; 82% of HFN cancers present with non-localized diseases (2005)
“The quantum and quality
of work at TMH’s head
and neck group is as good
as that at the best cancer
centers in the world” -2010 Global peer review report
ACROSS A VARIETY OF SPECIALTIES, INDIA HAS CREATED INSTITUTIONS THAT HAVE DE-HYPHENATED QUALITY OF CARE FROM HIGH COST
Clinical Area
Cancer
Cardiac
Low cost ‘Premier’
Several regional players
Exceptional Outcomes
• Dozens of hospitals now regularly do bypasses off-pump, on the beating heart. 5-year survival rates at several Indian hospitals at or above global benchmarks
Neurology
Limitations
1) Scalability still a challenge due to deep talent constraints
2) Managing chronic conditions still tough
• Several practices delivering replacement and prosthesis results at or global levels
• Niches created in unusual areas (e.g. pediatric cardiac care at Amma Hospital, Cochin)

CONTENTS
Overview of healthcare in India
The Indian hospital free market
Winning strategies
Implications for South Africa
LEADING INDIAN PLAYERS HAVE CHALLENGED SEVERAL MYTHS & DOGMAS
• Standards are useful, but they must be challenged if they obstruct the ability to deliver care – innovate constantly
More resources are essential
1
2
Standards are essential and necessary
• More would be good. If not, we will adjust. Trade offs are a part of life
Myth Indian champion’s response
Productivity requires technology3• Technology does not imply productivity
(or results)• Tech innovation must be appropriate
Healthcare is not a business4 • A business like approach critical.“ Will patient pay for this?” “Will we get more patients if we charge less?

INDIAN PLAYERS HAVE INNOVATED RELENTLESSLY, CONSTANTLY CHALLENGING DOGMA AND NORMS
…leading to a service at any price point
Economy
Low costMaternityproviders
83
Price of normal labour; US$
Hospitals at all sizes Calibrated infrastructure
Sq ft per bed
Small200
Nursinghome
120
$ per patient bed
$150
1
Economynursing
home417
1,250
1,667"Birthing
suite"
SuperiorTrust
hospital
Luxuryhospital
1500
Majorhospital
600
Smallhospital
200
Source: Web Reports; client studies
$3500

INDIAN PROVIDERS HAVE TORN DOWN AND REDESIGNED CARE, FOCUSING ON PRODUCTIVITY OVER MARGINS
Physician productivityThe challenge : Deliver a Cataract Surgery for under 100 US $
Raise physician productivity
• Developed new small incision technique which requires less than 5 minutes to remove old lens
• Used Lean processes to raise productivity
Cataract surgeries per day per surgeon
Client A >60
2
CLIENT EXAMPLE
Source: Web Reports
• Create “continuous flow” of patients
Control capital costs
• Developed domestic low cost microscope with 20% fewer features for only 40% of price
• Developed domestic foldable lenses at a fraction of cost
Client B ~40
<20Typical global
number

THEY HAVE SHOWN THAT MUCH CAN BE DONE WITH JUDICIOUS USE OF TECHNOLOGY
The challenge
The plan : ADT @ global standards
Results
• 60 year old Trust hospital facing competitive pressure
• 10 year old basic HIS system
• Rigorously studied total process
• Devised paper & people solutions for all drivers of discharge process
• Piloted, tested, rolled out
From
• 0% planned discharges• 0% e-discharge cards• 5 hours to discharge
CLIENT EXAMPLE
3
• No EMR• No RFID/bar coding• No vacuum tubes
system
• Shallow talent pool
• Used minimal HIS/ IT fixes for electronic discharge summaries
• CEO-led, nurse driven 6 month program
• 80% pre-planned discharges
• 100% e-discharge cards• 45 min “sign to vacate”
USING MULTIPLE STRATEGIES AND BUSINESS MODELS TO ENABLE COST COMPETITIVENESS…
Variety of physician models to attract physicians
• Co-owner with P&L responsibility
• Group practice
• Free – lance consultant
• Salaried with fixed play –
Variety of cost containment and cost distribution strategies
• Extensive use of cross subsidization with telescopic charging (services charged at higher margins by room rent)
• Robust procurement including upstream integration into consumable manufacture
• Set up of EO gas reuse infrastructure to re-
4
• Salaried with fixed play –with or without research/academic duties
• Salaried with value share
• Set up of EO gas reuse infrastructure to re-condition and reuse select consumables
• Creation of ‘pay-as-you-go’ payment models to convert capital expenses into operational expenses (e.g. reagent rental models)

CONTENTS
Overview of healthcare in India
The Indian hospital free market
Winning strategies
Implications for South Africa

IMPLICATIONS FOR SOUTH AFRICA
Expensive Healthcare ≠ Good Healthcare
Go from using price to determine the market to using the market to set the price
1
2
Don’t make the ‘best’ the enemy of the ‘better’
If you want to change the game, change the rules
3
4
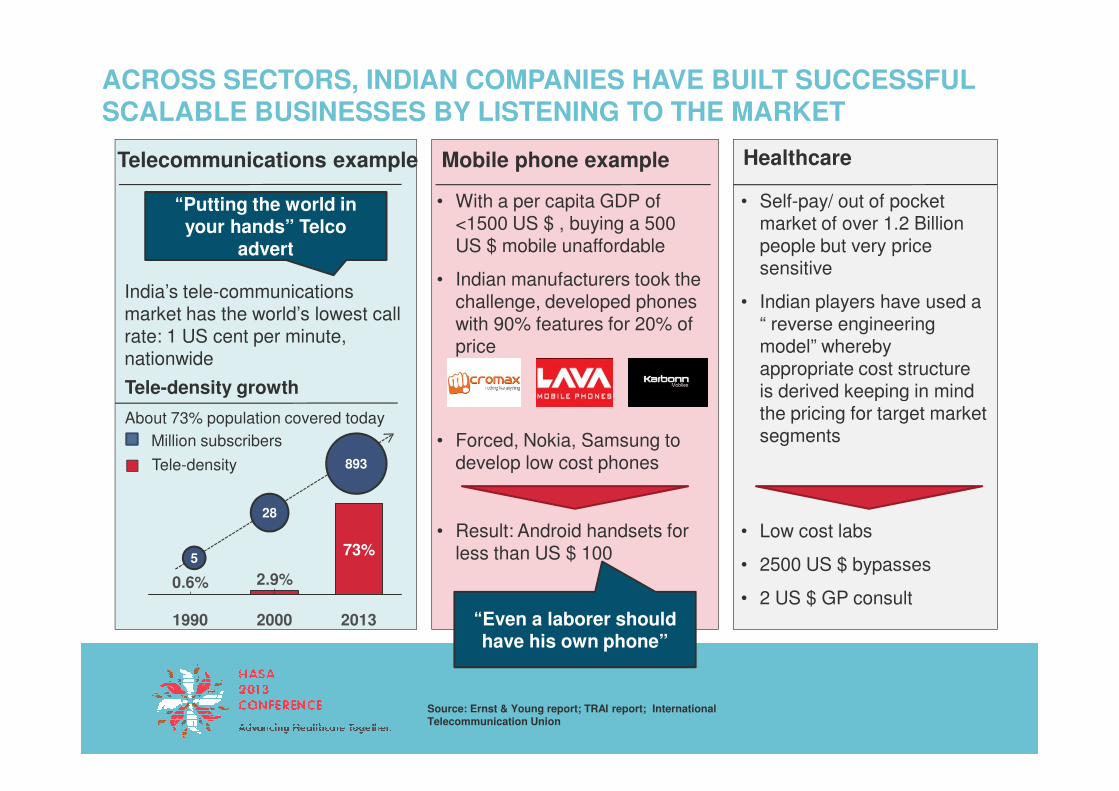
ACROSS SECTORS, INDIAN COMPANIES HAVE BUILT SUCCESSFUL SCALABLE BUSINESSES BY LISTENING TO THE MARKET
Telecommunications example Mobile phone example
• With a per capita GDP of <1500 US $ , buying a 500 US $ mobile unaffordable
• Indian manufacturers took the challenge, developed phones with 90% features for 20% of price
India’s tele-communications market has the world’s lowest call rate: 1 US cent per minute, nationwide
Tele-density growth
“Putting the world in your hands” Telco
advert
Healthcare
• Self-pay/ out of pocket market of over 1.2 Billion people but very price sensitive
• Indian players have used a “ reverse engineering model” whereby appropriate cost structure is derived keeping in mind Tele-density growth
About 73% population covered today
• Forced, Nokia, Samsung to develop low cost phones
• Result: Android handsets for less than US $ 100
“Even a laborer should have his own phone”
is derived keeping in mind the pricing for target market segments
• Low cost labs
• 2500 US $ bypasses
• 2 US $ GP consult2.9%
73%
0.6%
201320001990
Source: Ernst & Young report; TRAI report; International Telecommunication Union
Million subscribers
Tele-density
5
28
893

THE TATA NANO EXAMPLE: NOT MAKING THE BEST THE ENEMY OF THE BETTER
The challenge The NANO story
• The vision: A family car for 4 at under (US $ 2,000) “ One lakh”
• Small 2 cylinder engine
• Light, low cost chassis
• Basic equipment, single wiper
The result
• A car for INR 1,20,000
• With low running cost of less than 4 cents per mile
• Providing safe, dignified, affordable transportation to a family of 4
wiper
• Top speed 80 km/hr
• Costly, luxury features removed
• Several sophisticated safety system removed (ABS, ESP, Airbag, Sensor)
• Safe transport for 4
India has over 100,000 road
fatalities annually
Won’t survive on the
Autobahn but better than a
motorbike
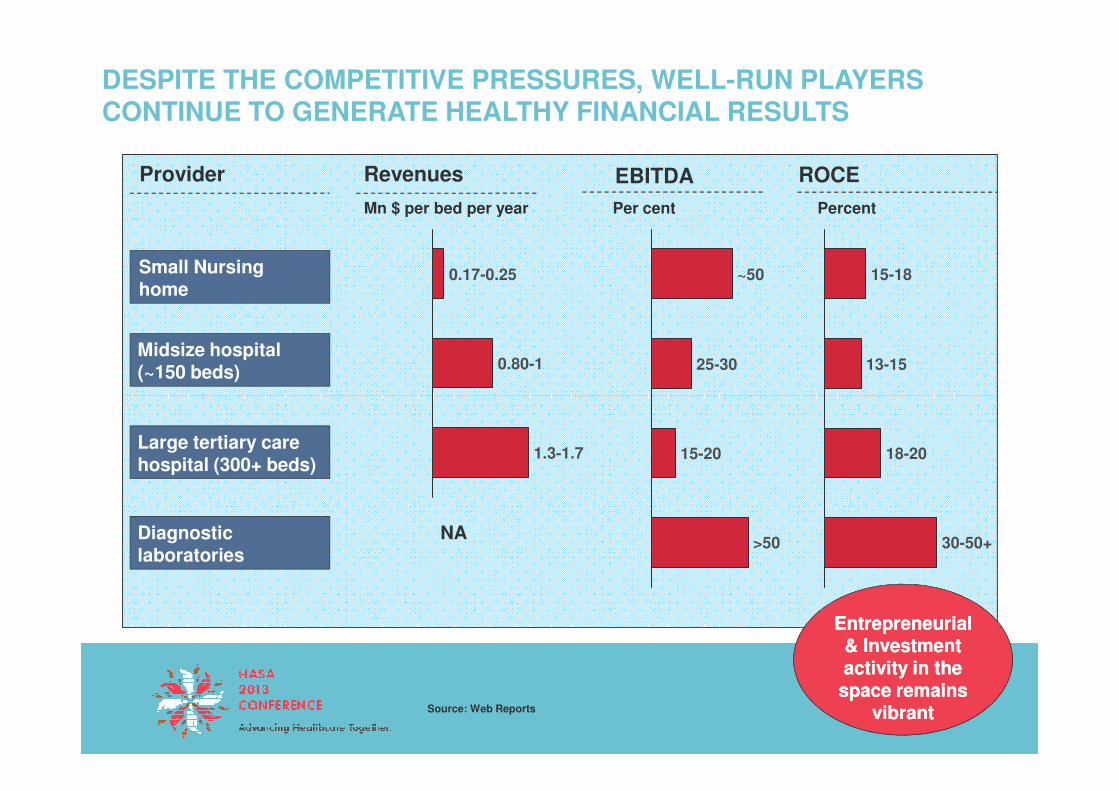
DESPITE THE COMPETITIVE PRESSURES, WELL-RUN PLAYERS CONTINUE TO GENERATE HEALTHY FINANCIAL RESULTS
ROCE
15-18
13-15
Provider Revenues
Small Nursing home
0.80-1
0.17-0.25
PercentMn $ per bed per year
Midsize hospital (~150 beds)
EBITDA
25-30
~50
Per cent
18-20
30-50+
1.3-1.7
Source: Web Reports
Large tertiary care hospital (300+ beds)
Diagnostic laboratories
>50
15-20
NA
Entrepreneurial & Investment activity in the
space remains vibrant
Entrepreneurial & Investment activity in the
space remains vibrant

IN SUMMARY
Policy and incentives have had profound implications for healthcare in India
Several challenges are similar: reducing variability in care outcomes in a nation with a huge spread in the ability to pay
Exposed to the cold-face of payment insecurity and Exposed to the cold-face of payment insecurity and competition, players have risen to the challenge and delivered exceptional performance
Changing the rules to change the game is essential; but the route adopted is as important as the destination

THANK YOU!

AS A RESULT, HEALTH CARE OUTCOMES IN INDIA ARE HIGHLY VARIABLE
• CABG results in several institutions that meet or exceed global outcomes
• >95% off-pump rates• > 90% RIMA/LIMA usage
• Presence of large transplant programs –with over 5,000 patients – in the not for profit sector!
….co exist with brillianceDismal healthcare outcome….
1648
5
17
Infant Mortality rate/ 1000 live births
20056
Maternal Mortality rate/ 100000 live births
profit sector!
• Pool of benchmark eye care institutions with deep skill base, benchmark outcomes at low prices
56
1237
15
10825647
TB Prevalence/ 100000 population
India U.K. China Brazil
Source: WHO Health statistics, 2010
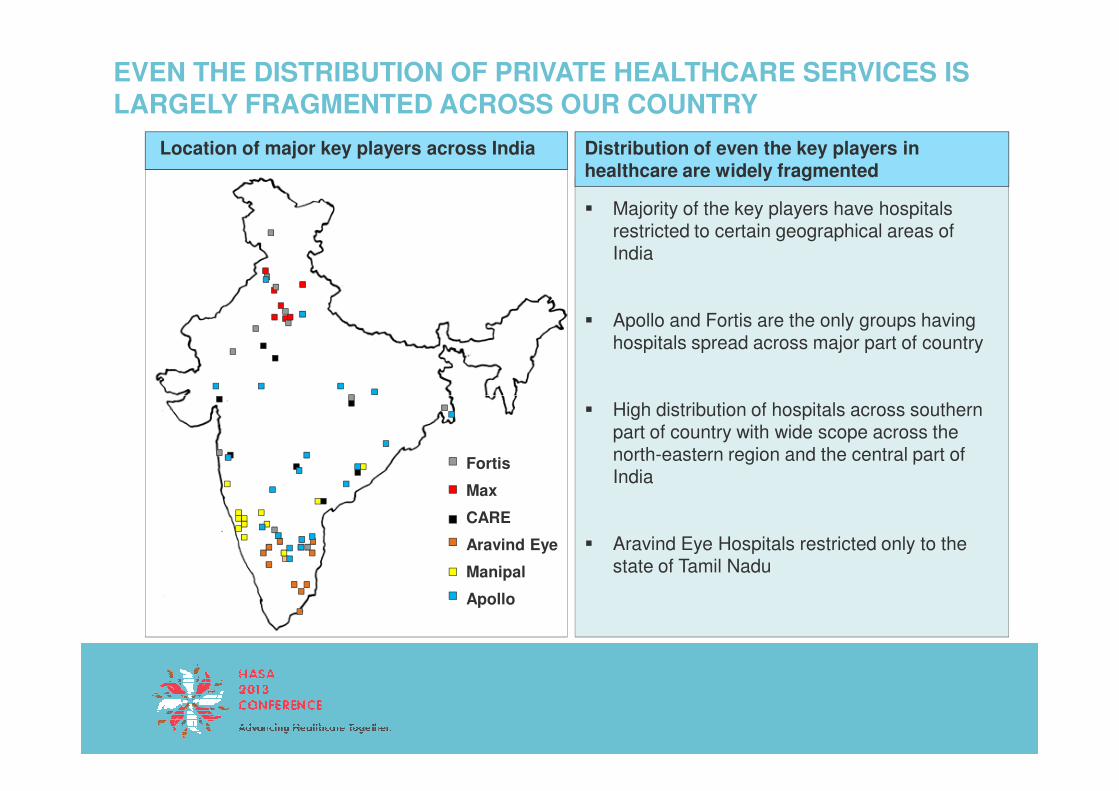
EVEN THE DISTRIBUTION OF PRIVATE HEALTHCARE SERVICES IS LARGELY FRAGMENTED ACROSS OUR COUNTRY
� Majority of the key players have hospitals restricted to certain geographical areas of India
� Apollo and Fortis are the only groups having hospitals spread across major part of country
Distribution of even the key players in healthcare are widely fragmented
Location of major key players across India
Fortis
Max
CARE
Aravind Eye
Manipal
Apollo
� High distribution of hospitals across southern part of country with wide scope across the north-eastern region and the central part of India
� Aravind Eye Hospitals restricted only to the state of Tamil Nadu