Embed Size (px)
Citation preview
Eating Disorders
B Y : M O N I K A S O C H A , K E L S I M A Y & S A R A H S I M P S O N
What is an Eating Disorder?
A range of psychological disorders characterized by abnormal or
disturbed eating habits.
Different Types Binge Eating Disorder:Frequent episodes of consuming very large amount of food but without behaviours to prevent weight gain, such as self-induced vomiting.
Eating Disorder Not Otherwise Specified (EDNOS): A feeding or eating disorder that causes significant distress or impairment, but does not meet the criteria for another feeding or eating disorder.
Night-Eating Syndrome: A relatively new eating disorder, "night-eating syndrome," characterized by a lack of appetite in the morning & overeating at night with agitation & insomnia.
Orthorexia: An obsession in which the sufferer systematically avoids specific foods in the belief that they are harmful.
Pica:an eating disorder typically defined as the persistent eating of nonnutritive substances for a period of at least 1 month at an age in which this behaviour is developmentally inappropriate.
Rumination:the voluntary or involuntary regurgitation and re-chewing of partially digested food that is either re-swallowed or expelled.
Nocturnal Sleep-Related Eating Disorder:thought to be a type of sleep disorder in which people eat while seeming to be sound asleep.
Anorexia Athletica: a condition where people over-exercise due to the fact they believe this will control their bodies and give them a sense of power, control and self-respect.
Anorexia
An eating disorder in which a person (most commonly adolescent females) maintains a starvation diet despite being significantly, 15 percent or more, underweight. Anorexia nervosa has the highest mortality rate of all psychiatric conditions.
Anorexia Nervosa:
Key Factors of Anorexia
Research suggests that a genetic predisposition to anorexia may run in families. If a girl has a sibling with anorexia, she is 10 to 20 times more likely than the general population to develop anorexia herself.
Some people have a genetic tendency toward perfectionism, sensitivity and perseverance, all traits associated with anorexia.
People often develop anorexia as a result of depression, loneliness, insecurity, pressure to be perfect, or feeling out of control. They may believe that dieting or weight loss can cure these feelings.
SYMPTOMS Physical Symptoms:o Weakness o Slowed thinkingo Brittle nailso Thinning hair o Constipation and bloatingo Dizziness, fainting, and headacheso Growth of fine hair all over the body and
faceo Absence of menstruation o Heart Palpitationso Low blood pressure; slowed heart rate o Bruises o Get cold easily o Swelling of arms or legs o Discoloration of the fingers
Emotional and Behavioral Symptoms: o Refusal to eat (around others, in public
places or at all )o Following a severely restricted diet despite
being thin o Obsession with counting calorieso Lying about eating o Preoccupation with food o Rigid meal or eating ritualso Feeling fat, despite being underweighto Fixation on body imageo Concern over tiny fluctuations in weighto Denial of being too thin Social withdrawal o Lack of emotion o Excessive exercise o Severe mood swings o Anxiety and anger
CAUSES
Anorexia is a complex condition that arises from a combination of many social, emotional, and biological factors.
Although our culture’s idealization of thinness plays a powerful role, there are many other contributing factors, including family environment, emotional difficulties, low self-esteem, and traumatic experiences in the past that can increase the chance of developing anorexia.
DIAGNOSIS o Detecting the problem early as well as early admission
improves prognosis.
o Target groups for screening should include young women with low BMI (body mass index), patients consulting with weight concerns who are not overweight, women with menstrual disturbances, patients with gastrointestinal symptoms, patients with physical signs of starvation, and children with poor growth.
o One or two simple screening questions can be used. For example: “Do you think you have an eating problem?” or “Do you worry excessively about your weight?”.
o The SCOFF questionnaire is a useful tool to come to a diagnosis along with an assessment of apparent symptoms.
Prognosis: the likely course of a disease or ailment.
Gastrointestinal: of or relating to the stomach and the intestines.
o Mild anorexia nervosa (BMI above 17) can be managed in primary care with support and monitoring. However, if patients don't respond within eight weeks, they should be referred to specialist services.
o Patients with moderate anorexia nervosa (BMI 14-17) should be referred non-urgently to specialist services.
o Patients with severe anorexia nervosa (BMI less than 14), rapid weight loss, or evidence of system failure should be urgently referred to specialist services, or a medical unit if the physical status of the patient is life-threatening.
**Recovery takes years, not weeks or months**
Treatments
Bulimia
An eating disorder in which a person alternates binge eating (usually of high calorie foods) with purging (by vomiting or laxative use), or fasting.
Bulimia Nervosa:
Key Factors of BulimiaPeople with bulimia are more likely to have parents with a substance abuse problem or psychological disorder.
People with bulimia have trouble managing emotions in a healthy way. Eating can be an emotional release or defence mechanism and as a result, it is not surprising that people binge and purge when feeling angry, depressed, stressed, or anxious.
Women with bulimia appear to have a higher incidence of sexual abuse.
People who suffer from bulimia are NOT typically underweight. Men and women with bulimia are usually normal weight or slightly overweight.
Research suggests that people who have a close relative who has or has had bulimia are four times more likely to develop it than those who do not have a relative with the condition

SYMPTOMSPhysical Symptoms:
• Calluses on the knuckles or hands
• Swollen cheeks, hands and feet
• Discolored teeth, tooth decay and mouth sores
• Frequent fluctuations in weight
• Abdominal pain
• Bloating
• Chronic sore throat
• Broken blood vessels in the eyes
• Weakness and dizziness
• Acid reflux or ulcers
• Loss of menstrual periods
• Chronic constipation from laxative abuse
Emotional and Behavioral Symptoms:• Preoccupation with body shape and weight• Living in fear of gaining weight• Feeling out of control of eating behavior• Eating until the point of discomfort or pain• Eating much more food in a binge episode
than in a normal meal or snack• Forcing oneself to vomit or exercise too
much• Misusing laxatives, diuretics or enemas
after eating• Using dietary supplements or herbal
products for weight loss
• Wanting to eat in privacy
CAUSESo Low self-esteem – if you have an eating disorder, you may have a low
opinion of yourself and see losing weight as a way of gaining self-wortho Depression – you may use binging as a way of coping with
unhappiness, but purging does not relieve this depression and the cycle continues
o Stress – for example, you may develop the condition after dealing with a traumatic experience, such as a death or divorce, or during the course of important life-changing events, such as getting married or leaving home
o Some people with bulimia have experienced a difficult childhood, with family problems, arguments and criticism.
DIAGNOSIS When doctors suspect bulimia, they typically perform:oA complete physical examoBlood and urine testsoA psychological evaluation, including a discussion of your
eating habits and attitude toward foodoMay also request an X-ray to check for broken bones,
pneumonia or heart problems and an electrocardiogram (EKG) to look for heart irregularities.
To be diagnosed with bulimia, these criteria must be met:oRepeatedly binge, eat an abnormally large amount of food, and
feel out of control of their eating.oGet rid of the extra calories from bingeing by vomiting,
excessive exercise, fasting, or misuse of laxatives, diuretics, enemas or other medications.
oBinge and purge at least twice a week for at least three months.oBody shape and weight influence feelings of self-worth too
much.oDo not carry out extremely restrictive eating behaviors.
Electrocardiogram: a record or display of a person's heartbeat produced by electrocardiography.
Enema: procedure in which liquid or gas is injected into the rectum, typically to expel its contents.

Treatments o Antidepressants may help reduce the symptoms of bulimia when used along
with psychotherapy.
o If patient has a severe form of bulimia and serious health complications, they may need treatment in a hospital.
o Some eating disorder programs may offer day treatment, rather than inpatient hospitalization.
o Dietitians can design an eating plan to help achieve a healthy weight, normal eating habits and good nutrition.
**Recovery takes years, not weeks or months**
Connection to the Brain
Eating disorders are strongly connected to the reward responses in the brain.
For instance – a dog will do anything for a treat. This is a similar act for people as well. When sugar touches the taste buds, the reward center is excited.
A new study shows that individuals with eating disorders do not react to sweet flavours the same way healthy people do.
A team of psychiatrists at U.C. San Diego researched 14 individuals who had suffered from anorexia, 14 individuals who had suffered form bulimia and 14 healthy individuals, with the same age and weights. After fasting overnight, the individuals consumed a modest breakfast. They were then fed small tastes of sugar every 20 seconds while there brains were scanned.o The women who suffered from anorexia showcased less
activity than healthy women in the reward center of the brain. o The women who suffered from bulimia showed more activity
than healthy women in the reward center of the brain. o These findings suggest that genetic and biological factors
underline most cases of eating disorders.
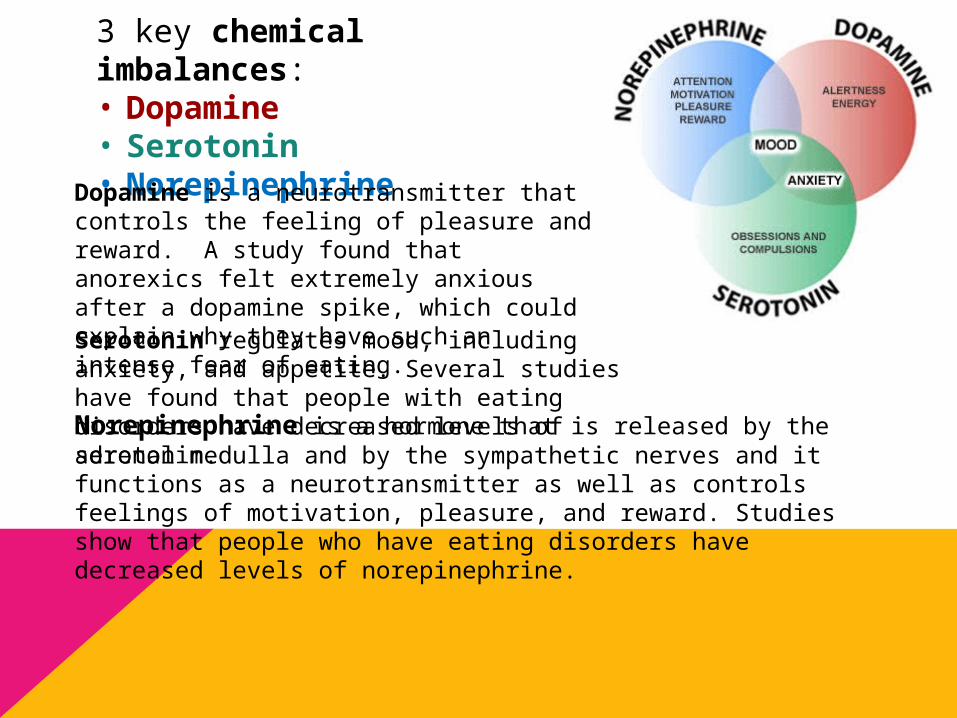
3 key chemical imbalances: • Dopamine • Serotonin • Norepinephrine
Dopamine is a neurotransmitter that controls the feeling of pleasure and reward. A study found that anorexics felt extremely anxious after a dopamine spike, which could explain why they have such an intense fear of eating. Serotonin regulates mood, including anxiety, and appetite. Several studies have found that people with eating disorders have decreased levels of serotonin.Norepinephrine is a hormone that is released by the adrenal medulla and by the sympathetic nerves and it functions as a neurotransmitter as well as controls feelings of motivation, pleasure, and reward. Studies show that people who have eating disorders have decreased levels of norepinephrine.
Connections to Parts of the BrainAmygdala: oThe center of the limbic emotional brain, constantly alert to
things needed for survival such as emotional reactions (anger and fear).
Frontal lobe: oResponsible for decision making as it organizes responses to
complex problems and planning steps to serve an objective or purpose, searches memories for relevant information and guides behaviour.
oIts orbitofrontal circuit manages emotional impulses in socially appropriate ways for productive behaviors.
Cerebrum:oResponsible for one’s reasoning behind their behaviours.
Hypothalamus:oRegulates food intake, hunger and controlling body weight. oReceives signals from the hormonal system.
Pituitary Gland: oProduces and distributes hormones that control growth, sexual
drive and hunger.
CASE STUDY
BoysGirls
vs.
Body Obsessed Boys- Dr. Phil:
http://www.youtube.com/watch?v=DHE5BTPjd3k
The Worst Case of Anorexia and Bulimia You’ll Ever See-Dr. Phil:
http://www.youtube.com/watch?v=iy_RPP2eIfk
Video
Quiz
Body Obsessed Boys
1) According to Dr. Phil, how many Americans are affected by eating disorders?
Approximately 10 million
2) How many of these are men? 1 million
3) How old was Eric when he was diagnosed? 12 (he is now 15)
5) What eating disorder was he diagnosed with? Anorexia
6) Identify symptoms of Anorexia that Eric has: Slowed heart rate, severely
restricted diet despite being thin, obsession with counting calories, preoccupation with food, social withdrawal,
excessive exercise.
7) What method of treatment had Eric received? Hospitalization
Worst Case of Anorexia and Bulimia You’ll Ever See
1) What eating disorders does Amy have? Anorexia and Bulimia
2) How does Amy describe herself?
a) Evil
b) Pretty
c) Fat
d) Thin3) How long has Amy suffered from her eating
disorders? 16 years
4. What symptoms of anorexia and bulimia does Amy have?
Gets cold easily, very thin hair, eats by herself, worst fear is gaining weight, follows a severely restricted diet despite being dangerously thin, preoccupation with food, rigid eating rituals, fixation on body image, social withdrawal, anxiety, discolored teeth and tooth decay, feeling out of control of eating behavior, forcing herself to vomit, eats much more food in a binge episode
than in a normal meal
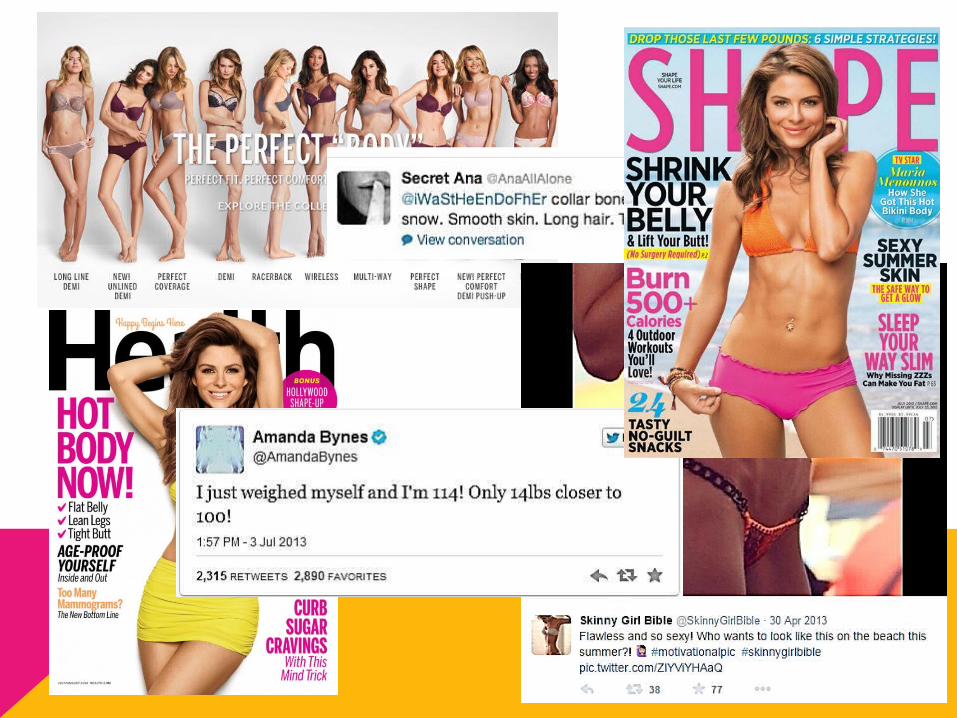
Society’s Impacto The media is covered with images of thin models and actors.
Success and worth often go hand and hand with being thin.
o Peer pressure may help fuel the desire to be thin, particularly among young girls.
o Our culture’s emphasis on thinness and beauty can lead to body dissatisfaction, particularly in young women bombarded with media images of an unrealistic physical ideal.
o Appearance-oriented professions or activities like ballet dancing, modeling, gymnastics, wrestling, running, and acting face a tremendous image pressure and are vulnerable to developing an eating disorder.
o Major life changes: Bulimia is often triggered by stressful changes or transitions, such as the physical changes of puberty, going away to college, or the breakup of a relationship. Binging and purging may be a negative way to cope with the stress.
o It also includes having parents who are overly controlling, who put a lot of emphasis on looks, diet themselves, or criticize their children’s bodies and appearance.

• In North American culture, women are more likely than men to develop an eating disorder.
• An estimated 85-95% of people with anorexia or bulimia are female.
• The ideal body type portrayed in media and advertising is possessed naturally by only 5% of Canadian females.
• Females put pressure on themselves as well as other girls to have a very specific body shape that is almost impossible to achieve, such as a flat stomach, long toned legs, and a large derriere and chest.
Females
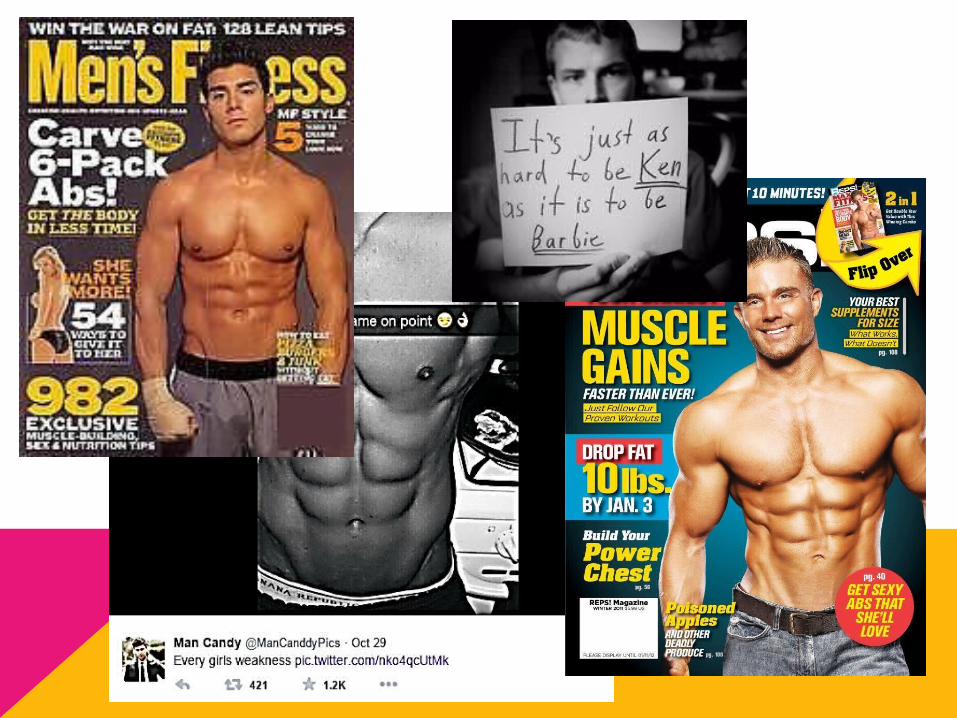
• Between 10 to 20 percent of people diagnosed with eating disorders are men who also feel the pressure to attain what they imagine is physical perfection.
• Girls use social media to portray the physical appearance of their “dream guy”.
• Media, such as magazines, promote extreme exercise and dieting to please women and others rather than promoting a healthy lifestyle for the reader.
• For example: perfect abs, large arms, broad shoulders, defined muscles.
Males
o 42% of first to third grade girls want to be thinner. o Over 50% of teenage girls and over 30% of teenage boys have used
troubling weight control methods like fasting, skipping meals, smoking, vomiting, or taking laxatives.
o 81% of ten year olds are afraid of being fat. o Almost 50% of people with eating disorders meet the criteria for
depression. o Only 1 in 10 men and women with eating disorders receive treatment. o 69% of girls in fifth to twelfth grade reported that magazine pictures
influenced their idea of a perfect body shape. o 20% of people suffering from anorexia will prematurely die from
complications related to their eating disorder, including heart failure, organ failure, malnutrition or suicide.
Interesting Facts
o Having an eating disorder is not something to hide.
o Do not put blame on yourself, as it is not your fault, it’s your brains way of responding to elements that are likely out of your control.
o An eating disorder is classified with the same severity as other mental illnesses, if not more.
o There are many resources available that can lead to the right path of recovery, such as: oCall the National Eating Disorders Association's toll-
free hotline at 1-800-931-2237 (Mon–Fri, 8:30 a.m. to 4:30 p.m. PST).
oThe National Eating Disorder Information Centre (NEDIC) is a Canadian non-profit providing resources on eating disorders and weight preoccupation.
How to Get Help