Embed Size (px)
Citation preview

1
We have New Zealand programmes which incorporate these favoured practices. We even have a national strategy for reducing family violence and a national strategy for children which has the reduction of violence near the top of its priorities. They sputter along without real political backing.
What is lacking is the courage, will and persistence to make fi rm, adequately-funded implementation plans, based on the best evidence, sell them to the public and relentlessly pursue them as was done in the case of the road toll. Let’s make it a public issue. The politicians seem already to be in electioneering mode. Let’s not be distracted by talk of how diffi cult it is or unpopular with some sections of the public. Our treatment of some of our children is a disgrace.
Contact:Dr Ian HassallInstitute of Public PolicyAuckland University of TechnologyTel (09) 917 9999 ext 8466Email: [email protected]
Inside...Injury Prevention Strategy 2
Deliberate Self-harm 3
Alcohol and Drugs 4
Safe Waimakariri 6
Playground Safety Standard 8
Domestic Violence Centre Programme 9
Open Fire Safety 10
Looking for Information? 11
Te Pukapuka Arai Hauata o Aotearoa
August 2004ISSUE NO. 30 ISSN 1172-8159
Why don’t we tackle New Zealand’s appalling rate of child maltreatment deaths?
by Ian Hassall
Ian Hassall works at the Institute of Public Policy at AUT. He was New Zealand’s fi rst Commissioner for Children.
In a recent Listener article Denis Welch asks why a national effort of the kind that halved our road
toll couldn’t be applied to reducing child deaths from abuse and neglect. Good question. Twenty-one of our fellow OECD countries have a lower abuse death rate than us and six have a rate less than half ours. Our twelve deaths a year are not an immutable fact of human nature.
We know we have a problem. We have been reading and being sickened by details of the lives and deaths of these children for the last twelve years. We know their names. Are the individual and societal factors that lead to lethally violent relationships more intractable and inaccessible than those that lead to lethally violent driving? Probably. But they are no less amenable to change. If we had the will could we bring about the change?
We are not bereft of ideas. In spite of the inherent diffi culty of proving prevention we have promising clues from the world literature for the effectiveness of some interventions.
Dr Ian Hassall
InjuryNEW ZEALAND
C O N T R O O L LCC OO NN TT RR O O L L
BULL
ETIN

2
Communication and strong partnerships “critical” for NZIPS
In June 2003 the New Zealand Injury Prevention Strategy (NZIPS) was launched by the
Minister for ACC. This strategy was developed to provide a framework for injury prevention as it was acknowledged that, while there was a high level of injury prevention work occurring throughout government, non-government and community organisations, there was not enough collaboration or co-ordination between these groups. The strategy is an expression of the Government’s commitment to working with organisations in the wider community to improve the country’s injury prevention performance.
To assist with achieving the strategy’s vision of “a safe New Zealand, becoming injury free” a secretariat has been established within ACC to lead and co-ordinate injury prevention work under the strategy’s 2004/05 Implementation Plan. This plan sets out key activities and expected results for each of the strategy’s objectives.
The secretariat, in consultation with advisory groups, has identifi ed several key focus areas for implementation. The fi rst of these is communication, as the strategy covers a wide range of government agencies and community groups and the fl ow of information and new ideas is critical to the overall success of the strategy. The links between the community and government agencies needs be strengthened to provide a strong partnership to advance injury prevention initiatives. The secretariat has redesigned and launched the NZIPS website www.nzips.govt.nz and
is producing a quarterly newsletter to disseminate information to a wide audience. The focus of both the newsletter and website is a forum for all groups to share information on effective initiatives, best practice and lessons learnt when developing new programmes. The secretariat is also exploring a project to undertake regional forums or speaking at other events to explain how the strategy can assist communities achieve their injury prevention goals and visions.
With the assistance of the Injury Prevention Research Centre (IPRC) at the University of Auckland, the secretariat has begun a stocktake to gauge the extent of injury prevention activity currently being conducted in New Zealand. This stocktake has been grouped into government and non-government organisations and once the results have been analysed there will be a clearer idea about where the gaps exist in injury prevention in New Zealand. It is expected the results of this work will be available after October 2004.
Objective 2 of the strategy is to “strengthen injury prevention capacity and capability”. Achieving this objective is seen as critical to the success of the strategy. The
secretariat has been working closely with the Injury Prevention Network Aotearoa New Zealand (IPNANZ) to address this issue. Work is currently underway to appoint a workforce development co-ordinator within IPNANZ to advance training and educational opportunities for injury prevention providers.
Other tasks the secretariat has been working on is the monitoring of work progressed in the six national priority areas of falls, assault, drowning and near drowning, workplace injuries, motor vehicle traffi c crashes and suicide and deliberate self-harm. The secretariat is also working to establish an evaluation framework for the strategy.
Contact:Geoff WilsonManager, NZ Injury Prevention StrategyTel (04) 918 7480Email: [email protected]: www.nzips.govt.nz
The NZIPS team, from left: Geoff Wilson, Megan Bly, Gill Myers, Bhama Rajiv Kumar

3
One in Eight Young Adults Have Deliberately Harmed Themselves
“[I] felt so unimportant, I’m not even a speck of dust; cutting myself made this feeling go away for days - a release of psychological pressure”
A fi lm entitled Thirteen, released here last month, will describe the day-to-day life
of a thirteen-year-old girl, including scenes in which she and her friends engage in what may be considered non-suicidal self-harmful behaviours. Our high youth suicide rates highlight that young adulthood is a high risk period for self-harm and a recent study showed that one in eight young people had deliberately harmed themselves.
The study was conducted by the Injury Prevention Research Unit (IPRU) at the University of Otago. It surveyed 966 participants aged 26 years, who were enrolled in the Dunedin Multidisciplinary Health and Development Study, and asked about participants’ self-harmful behaviours to deal with emotional pain. Self-harm included self-battery, self-biting, and self-wounding, which are known as “other” self harm, and methods such as cutting, which are specifi ed by International Classifi cation of Diseases (ICD) external codes for self-infl icted injury or suicide (ICD-self-harm). Questions included those on intoxication to deal with emotional pain.
“We fi rst asked about behaviours and then enquired about suicidal intent, to encourage reports of self-harm that were not necessarily suicidal in intent,” said Dr Shyamala Nada-Raja of the IPRU.
Self-harm was relatively common. Of the 472 women, about one in fi ve
reported “other” self-harm and one in seven ICD self-harm, in their lifetime. The comparable fi gures for men were about one in three and one in nine, respectively. Intoxication by substances to deal with emotional pain was common for about 35% of women and 41% of men. Most episodes of self-harm in the year prior to the interview were considered by the study participants to involve no suicidal intent, even for ICD self-harm. For the latter, 4% of the women’s episodes and 16% of the men’s episodes resulted in an injury. Most in the ICD self-harm group also reported “other” self-harm. Just over half in the ICD self-harm group and one-fi fth in the “other” self-harm group had sought professional help. Counsellors, psychologists and general practitioners were the most common sources of help and were rated favourably by most who had sought help from these sources. Attitudinal barriers were the most common reason given for not seeking help for self-harm or related behaviours.
“These results suggest that future studies of self-harm include a wide range of self-harm behaviours, and examine the associations between non-suicidal and suicidal self-harm. It may be necessary to identify ways to reduce attitudinal barriers to encourage help-seeking for self-harm
by young adults, especially by young men in this high risk age group.”
The self-harm study was funded by the Health Research Council of New Zealand and the Community Trust of Otago.
Contact:Dr Shyamala Nada-RajaInjury Prevention Research Unit (IPRU)University of OtagoTel (03) 479-8518Fax (03) 479-8337Email: [email protected]
The movie Thirteen opened in Auckland and Wellington last month.

4
Local Government – What is its Role in Dealing with Alcohol and Drug Issues?
The role of councils in dealing with alcohol and drug issues derives from a range of infl uences. At
a governance level councils offer a forum in which community concerns and desires can be described. If these concerns involve alcohol and drug issues councillors will be keen to examine ways they might assist their community to resolve them.
At another level councils have been prescribed responsibilities via a number of statutes that compel them to think about potential issues and to seek to manage these before they arise. Further to that the Local Government Act 2002 (LGA) tells councils their purpose is to work for community wellbeing.
Each of the pertinent statutes (The Liquor Act, The LGA, The [Public] Health Act 1956, the Resource Management Act 1991, Hazardous Substances and New Organisms Act) infl uences the way councils react to emerging problems and plans to
avoid their eventuality. Responses can range from very proactive to strongly interventionist and will depend on the nature of the problem.
Councils’ role in dealing with an irresponsible manager of a licensed premise or one which disturbs its neighbours is quite different to its role in dealing with youth gathering in the street to party, its role in closing down a tinny house, cleaning up a P lab as a contaminated site, or its role in planning for the appropriate distribution, density, size and modus operandi of licensed premises in a particular area.
Addressing the causes of drug and alcohol issues and seeking to mitigate their infl uence on at-risk communities is a more effective approach to addressing concerns than dealing with symptoms (the problem). However being proactive requires collaboration between the community and government to deliver comprehensive strategies able to interrupt social patterns leading to alcohol and drug issues.
Some councils have successfully taken up this challenge and have developed inter-sectoral alcohol strategies which involve the active participation of other parties to deliver particular initiatives. For example a number of agencies and local authorities are collaborating at both national and local levels to agree who will do what to deal with P in their communities, from minimizing supply and educating at-risk groups to who cleans up contaminated premises.
Councils do have a wide range of roles to play. Importantly there is considerable discretion as to how they give effect to each role. That is a crux of local governance that recognizes diversity of New Zealand communities and provides that they develop an approach that fi ts them.
Contact: Jane JohnstonLocal Government New ZealandEmail: [email protected]: www.lgnz.co.nz
Did you know...> Road traffi c crashes kill 1.2 million
people a year or an average of 3242 people every day globally
> Road traffi c crashes injure or disable between 20 million and 50 million people a year globally
> Road traffi c crashes cost an annual US$518 billion globally
> These fi gures are expected to increase dramatically by 2020 without appropriate action
> An increase in speed of 1km/h typically results in a 3% higher risk of a crash involving an injury, with a
4-5% increase for crashes that result in fatalities
> In Victoria, Australia, poor visibility was a factor in 65% of crashes between cars and motorized two-wheelers, and the sole cause in 21% of them
> In many high-income countries about 20% of fatally injured drivers have excess alcohol in their blood. In low-income countries alcohol is present in between 33% and 69% of fatally injured drivers.
> Non-helmeted users of motorized two-wheelers are three times more likely to sustain head injuries in a
crash compared with those wearing helmets.
> Correctly used seatbelts reduce the risk of death in a crash by approximately 61%.
> The use of child restraints can reduce infant death in car crashes by 71% and toddler deaths by 54%.
Source: The World Report on Road Traffi c Injury Prevention, developed jointly by the World Health Organisation and the World Bank and presented at the 7th World Conference on Injury Prevention and Safety Promotion, held in Vienna in June.

5
Mayor Harvey: Community empowerment, Council leadership
solutions to substance abuseby Bob Harvey
Substance abuse is a social phenomenon. It may manifest itself in crimes but those crimes are primarily only symptoms of a segment of society that is not coping.
If the community does not combine its resources to respond successfully to drug and alcohol abuse, who else can do it? Only the people who know where abuse is occurring can ‘blow the whistle’ and only when the ‘whistle is blown’ can we as a society do something positive.
The Police and many social agencies are geared only to react and respond - not to pre-empt - and unless we prefer to live with the destructive and criminal effects of substance abuse we must help the Police and social agencies wherever we can. The Police do need more resources and we can help just by motivating our own staff and the community to be alert to – and report – signs of abuse and criminal activity.
In Waitakere, we are doing this through a very close working relationship with Police and social agencies and also by calling for new legislation to replace obsolete parts of the Health Act covering the clean up of chemical contaminated properties.
Prevention, however, is always better
than cure. The community doesn’t want substance abuse problems, it wants solutions and therefore the council – as the leader of the community - has a duty to marshal the community’s resources to produce the solutions.
I believe that in Waitakere City - with our holistic approach to city-building-through-community-building - we have begun to grasp this nettle. We, with government assistance, have formed partnerships with communities, specifi cally to empower them to behave as if they are a community and not a jumble of disparate people, who just happen to live next door to each other.
A true community knows best where the negatives in their environment are, and has ideas about how, just by working together and caring for each other, they can replace negatives with positives.
It is when communities care for each other that we will make progress – and a progressive, imaginative council can lead communities to this situation. It is called empowerment and it works.
Contact: Bob HarveyWaitakere CityTel (09) 836 8000Website: www.waitakere.govt.nz
Waitakere City Mayor Bob Harvey

6
Waimakariri recently celebrated fi ve years as an Accredited World Health Organisation
(WHO) Safe Community, with community partners (Waimakariri District Council, Land Transport Safety Authority, Police, Ministry of Health, ACC and Canterbury District Health Board) re-signing their commitment to the WHO Safe Community Criteria at a Waimakariri District Council meeting. The Safe Waimakariri community team is responsible for the delivery of activities around road safety, crime prevention and injury prevention with advisory groups, representative of the community, and organisations and agencies with an interest in these areas supporting the work.
“The WHO Safe Community accreditation has given Waimakariri a framework on which to build our projects with the results being increased participation and ownership of safety initiatives within the community and long term sustainable programmes – in other words a ‘safety culture’ is being built,” said Injury Prevention Waimakariri programme co-ordinator Sandra James. The indicators for WHO Safe Com-munities are available on www.phs.ki.se/scp/criteria.html.
Down the Back Paddock
A new safety resource called Down the Back Paddock is set to be piloted at North Loburn and Loburn Schools in Waimakariri during term three, with a farm safety day planned as part of Kidsafe Week in October. Research commissioned by Injury Prevention Waimakariri highlighted the need to address safety issues for children living and visiting
rural environments including use of ATV bikes, fi re safety, horses, rural road safety, water safety, fi rearms, dog and other animal control and neighbourhood support. It also showed that there were different issues even within the relatively small Waimakariri area, for example lifestyle blocks versus farms. A collaborative group has been working to develop farm safety days. It will bring together agencies and individuals within the community to provide education and information around specifi c safety issues identifi ed by communities, for example, crossing rivers or burning rubbish. Down the Back Paddock is a curriculum resource
Waimakariri – Five years as an accredited WHO Safe Community
which schools will use a term prior to the visit to support the farm safety day visit. Developed by a local deputy principal and principal it is a user friendly, simple to follow resource for teachers and the school as a whole. Other partners in this project are the NZ Fire Service, NZ Police, council road safety, animal control and water safety staff, Neighbourhood Support and a fi rearms safety advisor.
Contact:Sandra JamesInjury Prevention WaimakaririTel (03) 313 6136Email: [email protected]
Cameron Parr (right), Group Manager of Recreation and Community Services at Auckland City, at the launch of Communities Living Injury Free in June. Rob Charlton of The Improv Bandits team (left) is interviewing Cameron about injury while Wade Jackson is behind Cameron “being his arms”. Communities Living Injury Free was set up to reduce the number and severity of injuries for Auckland city residents from Otahuhu to Avondale and the eastern suburbs. More than 100 members of the community attended the launch, including representatives from SafeKids, the Child Safety Foundation, Plunket, Watersafe Auckland, Age Concern, Alcohol Healthwatch, New Zealand Police, the New Zealand Fire Service and Housing New Zealand. Representatives from primary health organisations, ACC, the Auckland District Health Board, local Maori and Pacifi c Island health providers and new settler groups were also there, as were key researchers and academics who specialise in this area. The Communities Living Injury Free website can be found at www.auckland.govt.nz/injuryfree.
Injury free Auckland City

7
Tai chi programme builds confi dence
A tai chi programme run for older people in the Waimakariri and Christchurch
areas has proven to be great success, both in reducing the number of falls and in enhancing the sense of confi dence and well-being experienced by participants.
“Falls are the leading cause of injury for older people. However the majority of falls can be prevented,” said Pip Nicholl of Presbyterian Support Services. “Tai Chi reduces the number of falls and fall-related injuries by improving strength and balance. Its gentle, fl uid-like movements make it an ideal exercise for older people.”
The 68 participants in the programme completed a questionnaire in which they were asked to assess changes in levels of confi dence and balance. “Almost all participants said they were more aware of the risk of falling, confi dent that tai chi would reduce the likelihood of a fall and were less fearful of a fall. Nearly half said they had improved balance,” said Pip. “More importantly it has changed some people’s lives.”
“Tai chi saved my life both mentally and physically.”
“Since doing tai chi I am more confi dent going down stairs and with my balance generally.”
“I enjoy waking up in the morning and realising today is a tai chi day.”
Results from an annual survey of slips, trips and falls calendars fi lled out by participants in the survey showed a 64% reduction in the number of falls reported.
Mary Guy (above) attends tai chi classes aimed at improving strength and balance and preventing falls.
Contact: Pip NichollPresbyterian SupportTel (03) 366 5472Fax (03) 379 6235Website: www.ps.org.nz/uppersouthisland
8
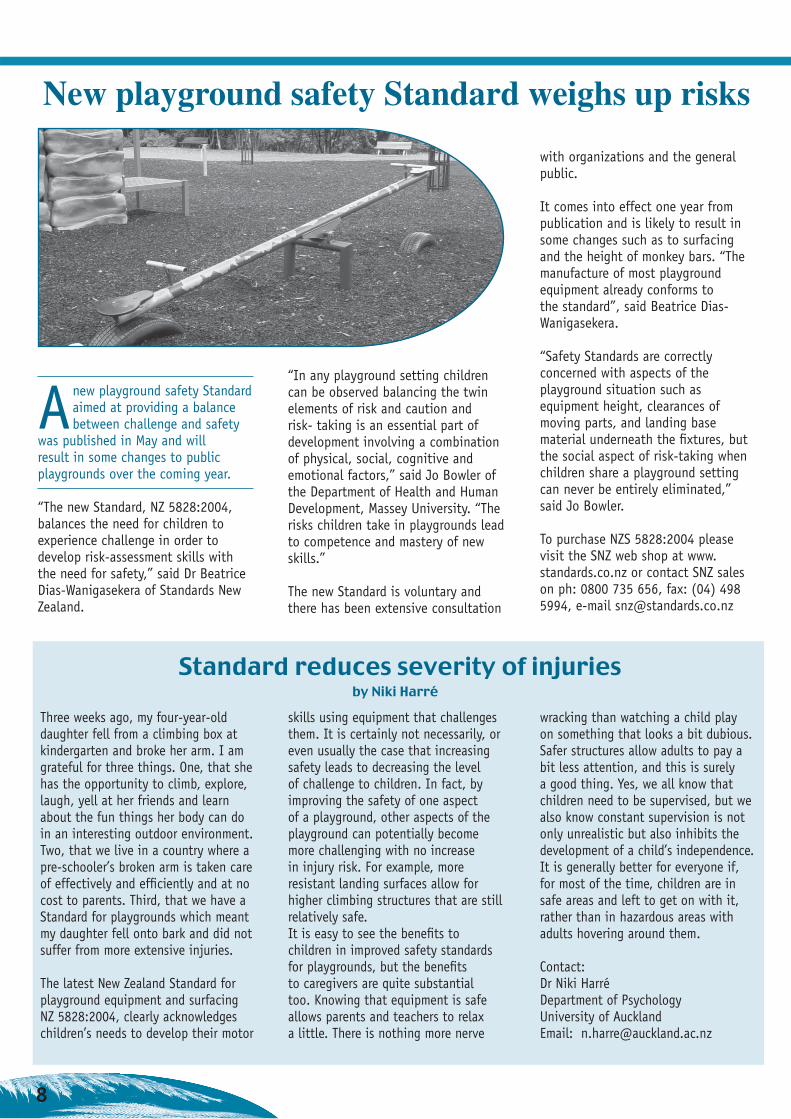
Anew playground safety Standard aimed at providing a balance between challenge and safety
was published in May and will result in some changes to public playgrounds over the coming year.
“The new Standard, NZ 5828:2004, balances the need for children to experience challenge in order to develop risk-assessment skills with the need for safety,” said Dr Beatrice Dias-Wanigasekera of Standards New Zealand.
“In any playground setting children can be observed balancing the twin elements of risk and caution and risk- taking is an essential part of development involving a combination of physical, social, cognitive and emotional factors,” said Jo Bowler of the Department of Health and Human Development, Massey University. “The risks children take in playgrounds lead to competence and mastery of new skills.”
The new Standard is voluntary and there has been extensive consultation
Three weeks ago, my four-year-old daughter fell from a climbing box at kindergarten and broke her arm. I am grateful for three things. One, that she has the opportunity to climb, explore, laugh, yell at her friends and learn about the fun things her body can do in an interesting outdoor environment. Two, that we live in a country where a pre-schooler’s broken arm is taken care of effectively and effi ciently and at no cost to parents. Third, that we have a Standard for playgrounds which meant my daughter fell onto bark and did not suffer from more extensive injuries.
The latest New Zealand Standard for playground equipment and surfacing NZ 5828:2004, clearly acknowledges children’s needs to develop their motor
Standard reduces severity of injuries by Niki Harré
with organizations and the general public.
It comes into effect one year from publication and is likely to result in some changes such as to surfacing and the height of monkey bars. “The manufacture of most playground equipment already conforms to the standard”, said Beatrice Dias-Wanigasekera.
“Safety Standards are correctly concerned with aspects of the playground situation such as equipment height, clearances of moving parts, and landing base material underneath the fi xtures, but the social aspect of risk-taking when children share a playground setting can never be entirely eliminated,” said Jo Bowler.
To purchase NZS 5828:2004 please visit the SNZ web shop at www.standards.co.nz or contact SNZ sales on ph: 0800 735 656, fax: (04) 498 5994, e-mail [email protected]
skills using equipment that challenges them. It is certainly not necessarily, or even usually the case that increasing safety leads to decreasing the level of challenge to children. In fact, by improving the safety of one aspect of a playground, other aspects of the playground can potentially become more challenging with no increase in injury risk. For example, more resistant landing surfaces allow for higher climbing structures that are still relatively safe. It is easy to see the benefi ts to children in improved safety standards for playgrounds, but the benefi ts to caregivers are quite substantial too. Knowing that equipment is safe allows parents and teachers to relax a little. There is nothing more nerve
wracking than watching a child play on something that looks a bit dubious. Safer structures allow adults to pay a bit less attention, and this is surely a good thing. Yes, we all know that children need to be supervised, but we also know constant supervision is not only unrealistic but also inhibits the development of a child’s independence. It is generally better for everyone if, for most of the time, children are in safe areas and left to get on with it, rather than in hazardous areas with adults hovering around them.
Contact:Dr Niki HarréDepartment of PsychologyUniversity of AucklandEmail: [email protected]
New playground safety Standard weighs up risks

9
Traumatised children helped by new Domestic Violence Centre programme
Concerns about the poor uptake of therapeutic services by children witnessing violence in the home
led the Domestic Violence Centre (DVC) in Auckland to pilot a new Child Crisis Team intervention. This new service is unique in New Zealand and an evaluation has shown a reduction in problems experienced by these chil-dren as a result of the intervention.
“The service aimed to provide accessible services for children who, although traumatised, may fall below Child Youth & Family Services high priority threshold,” said Jane Drumm, Executive Director of the DVC. “We have found that these children are generally not seen as a priority and may languish on the unallocated list for a very long time. When fi nally seen, it is often a case of too little, too late. The Child Crisis Team (CCT) responds promptly to incidents reported to the police, is proactively offered to families, is free, in their homes and at times convenient to them.”
The CCT programme was designed to be a brief and structured intervention of three visits. The goal of the programme was to reduce the level of repeat violence and stress on children in these homes, by giving families an opportunity to understand the impact on their children. Objectives were to: alleviate stress; help children understand what was happening; assess the level of danger and trauma; provide crisis therapy; develop safety plans; assist parents to understand the impact of violence upon their child; provide support to parents experiencing diffi culties with their children; and be a “front door” into other services such as children’s programmes and Barnardo’s.
The evaluation, funded by The Crime Prevention Unit of the Ministry of Justice and conducted by the Injury Prevention Research Centre (IPRC) at the University of Auckland, included an analysis of 89 family case fi les, involving 226 children. Most of the families reported signs of children displaying physical and behavioural problems at the time of the fi rst visit. These diffi culties included bed wetting, problems at school, nightmares and physically hurting their mother or sibling. By the time of the third visit, the evaluation found that the majority of families reported a reduction in these areas.
“(My daughter) is no longer consumed by sadness … she is able to concentrate better at school and (is) generally much happier.” (mother)
“She had been afraid to talk to me before about her problems but now opens up and there is better communication between us all.” (mother)
Forming age-appropriate safety plans was an important part of the programme. Evaluation evidence indicated that children who had needed to use their safety plan had been able to remember it and put it into action.
“In developing the CCT programme, I was greatly infl uenced by an observation made by a Canadian children’s programme which was that ‘women stay in dangerous relationships because of their children and they leave because of their children too’,” Jane said. “This was found to be the case here with mothers re-evaluating their relationships when they understood
the impact the violence was having on their children.”
“At times I sit there with a crying woman after I’ve started explaining a little bit of what the children are going through. They just absolutely burst into tears because they have no idea. Often it’s a real catalyst for change.” (Advocate)
Mothers and children from all families indicated positive outcomes from the advocate’s visits.
“Yes it was helpful. The explanations about children’s behaviours, the safety plan and children’s rights.” (mother)
“Referring us to counsellors and groups. I mean we didn’t even know that stuff was out there.” (mother)
“Yes it was because we could open ourselves. We learned that we weren’t all wrong, we were actually kind of right.” (teenage male)
“Another thing that is really good about the service is that when it is all happening, they come to you and it is free and available.” (mother)
“They gave me ideas about how to control my anger.” (10 year old female)
A key recommendation, to increase the number of sessions to four, has already been implemented, with this fourth visit being made four to six weeks after the conclusion of the fi rst three.
Contact:Jane DrummDomestic Violence CentreTel (09) 303 3938Website: www.dvc.org.nz
10
From the Editor …
A cosy evening goes up in smoke
It’s great to be back in print after a two-year break. Our thanks go to ACC for their commitment
to funding the NZICB for the coming year. Thanks also to the team of injury prevention experts who have come together to make up the editorial board for the NZICB. We’re fortunate to have back on board the advisors from previous issues, along with a few new names.
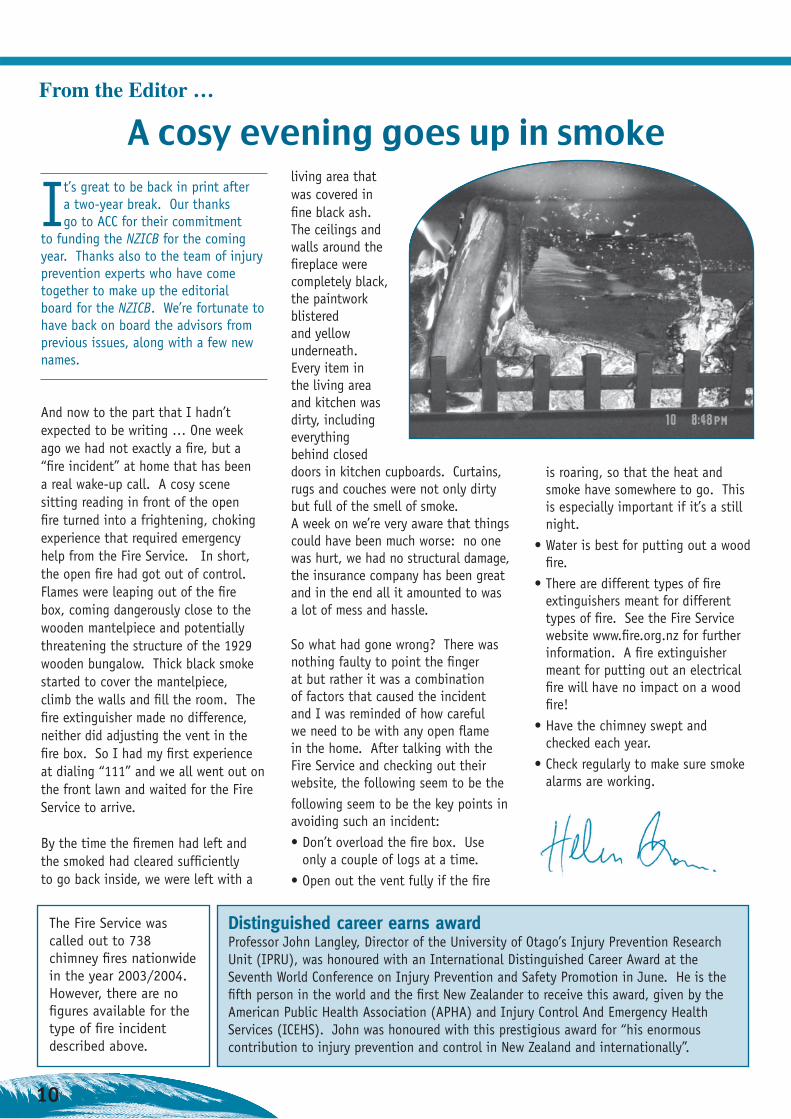
And now to the part that I hadn’t expected to be writing … One week ago we had not exactly a fi re, but a “fi re incident” at home that has been a real wake-up call. A cosy scene sitting reading in front of the open fi re turned into a frightening, choking experience that required emergency help from the Fire Service. In short, the open fi re had got out of control. Flames were leaping out of the fi re box, coming dangerously close to the wooden mantelpiece and potentially threatening the structure of the 1929 wooden bungalow. Thick black smoke started to cover the mantelpiece, climb the walls and fi ll the room. The fi re extinguisher made no difference, neither did adjusting the vent in the fi re box. So I had my fi rst experience at dialing “111” and we all went out on the front lawn and waited for the Fire Service to arrive.
By the time the fi remen had left and the smoked had cleared suffi ciently to go back inside, we were left with a
living area that was covered in fi ne black ash. The ceilings and walls around the fi replace were completely black, the paintwork blistered and yellow underneath. Every item in the living area and kitchen was dirty, including everything behind closed doors in kitchen cupboards. Curtains, rugs and couches were not only dirty but full of the smell of smoke. A week on we’re very aware that things could have been much worse: no one was hurt, we had no structural damage, the insurance company has been great and in the end all it amounted to was a lot of mess and hassle.
So what had gone wrong? There was nothing faulty to point the fi nger at but rather it was a combination of factors that caused the incident and I was reminded of how careful we need to be with any open fl ame in the home. After talking with the Fire Service and checking out their website, the following seem to be the following seem to be the key points in avoiding such an incident:• Don’t overload the fi re box. Use
only a couple of logs at a time. • Open out the vent fully if the fi re
is roaring, so that the heat and smoke have somewhere to go. This is especially important if it’s a still night.
• Water is best for putting out a wood fi re.
• There are different types of fi re extinguishers meant for different types of fi re. See the Fire Service website www.fi re.org.nz for further information. A fi re extinguisher meant for putting out an electrical fi re will have no impact on a wood fi re!
• Have the chimney swept and checked each year.
• Check regularly to make sure smoke alarms are working.
Distinguished career earns awardProfessor John Langley, Director of the University of Otago’s Injury Prevention Research Unit (IPRU), was honoured with an International Distinguished Career Award at the Seventh World Conference on Injury Prevention and Safety Promotion in June. He is the fi fth person in the world and the fi rst New Zealander to receive this award, given by the American Public Health Association (APHA) and Injury Control And Emergency Health Services (ICEHS). John was honoured with this prestigious award for “his enormous contribution to injury prevention and control in New Zealand and internationally”.
The Fire Service was called out to 738 chimney fi res nationwide in the year 2003/2004. However, there are no fi gures available for the type of fi re incident described above.

11
Looking for information? Are you looking for national
injury data, for injury data by district health board (DHB)
or territorial local authority (TLA)? Thanks to the Ministry of Health, the Injury Prevention Research Unit (IPRU) at the University of Otago is able to provide National Injury Query System (NIQS) information on its website, www.otago.ac.nz/ipru, so you can fi nd injury statistics for New Zealand.
NIQS is an interactive system set up so you can select variables such as the years you want information for, whether you want information on deaths or hospitalisations, intent, age group, cause, gender and whether you want national or district health board data. The
information available is from the New Zealand Health Information Service mortality and morbidity dataset. There are also useful summaries of injury statistics in reports and tables. They can be found on the statistics page: www.otago.ac.nz/ipru/Stats .
Can’t fi nd what you want or your question isn’t that simple? Email [email protected] for personal assistance. There is a lot more information available than can be seen on NIQS, so if you can’t fi nd it on the website, ask. For example, the TLA data are not on NIQS at the moment, but they can run a query using TLA boundaries. Dan and Maggie are the IPRU’s data management staff who will work on your requests. Use the inquiry
address to contact them or phone (03) 479 5934, or fax (03) 479 8337.The Ministry of Health funds this service, and queries that do not take more than six hours of staff time are free. We will let you know if your query might be a complex one and needs extra time. We undertake to respond in fi ve working days, and it really helps to know what your time frame or constraints are. Depending on our workload, we may be able to respond more quickly.
Your feedback on this service is most welcome. One of our questions at the moment is what would be most useful if we were going to extend the information available on NIQS. Visit the IPRU Stats page, visit NIQS, and use the feedback page to tell us what would help you in your work.
Strong client focus for new IPRC librarian
The Injury Prevention Research Centre (IPRC) at the University of Auckland recently appointed
Gay Richards as librarian. Gay has a Masters in Library and Information Studies from Victoria University of Wellington and is an active member of the Library and Information Association of New Zealand Aotearoa (LIANZA). Her background includes information management and research in both the business and health sectors.
Gay is manager of the Information & Resource Unit, which is an integral part of the IPRC. Its role is to collect and catalogue published research and reports on injury prevention issues. These include many reports and conference proceedings which can be diffi cult to fi nd. Research published
by IPRC staff is made available through the IPRC website. Much of this material can now be downloaded by anyone worldwide at no cost. IPRC is committed to the dissemination of injury prevention research to practitioners and researchers in New Zealand and around the world. “I bring a client-focused approach to the provision of information. As examples of how I can help people outside Auckland, I have already helped a nursing student in Nelson complete an assignment on falls, supplied information on suicide prevention to a researcher in the United Kingdom, provided information to a community-based injury prevention practitioner on effective strategies for prevention of home injuries and provided a Wellington consultancy librarian with IPRC research papers,” said Gay. “As
well as contacting me by phone or email, those in the Auckland region are welcome to visit IPRC and use the information resources we have collected.”
The role also involves working closely with researchers and injury prevention practitioners to conduct robust literature reviews conforming as far as practicable to the rigorous requirements of Cochrane Collaboration standards. “For example, I have been working with researchers to develop exhaustive search strategies, executing online searches and gathering information from many other sources including the internet.
Contact:Gay Richards, IPRC email: [email protected]: (09) 373 7599 x84640 Website: www.auckland.ac.nz/ipc

12
ICB EDITORIAL BOARDHelen Borne, IPRC, University of AucklandMarilyn Brewin, IPRC, University of AucklandSue Campbell, Royal NZ Plunket SocietyCarolyn Coggan, IPRC, University of AucklandMargaret Devlin, Safe WaitakereLaurie Gabites, Wellington City CouncilRussell Hendry, ACCJohn Langley, IPRU, University of OtagoShyamala Nada-Raja, IPRU, University of OtagoVal Norton, IPNANZGeoff Wilson, NZIPS Secretariat, ACC
MEETINGS & CONFERENCES17th International Conference on Alcohol, Drugs and Traffi c Safety Glasgow, United Kingdom, August 8-13, 2004 http://www.icadts2004.com/
10th European Symposium On Suicide And Suicidal BehaviourCopenhagenAugust 25-28,2004http://www.suicideprevention.dk/
7th Australian Injury Prevention Conference 2nd Pacifi c Rim Safe Communities ConferenceMackay, QueenslandSeptember 15-17, 2004Contact: Maria Lamari, conference secretariatFax +617 3847 2148Website: www.nisu.fl inders.edu.au/aipnconference2004
3rd World Conference on the Promotion of Mental Health and prevention of Mental and Behavioural DisordersAucklandSeptember 15-17, 2004Contact: (09) 300 7010Fax (09) 300 7020Email: [email protected]
IASP Asia-Pacifi c 2004Suicide prevention through collaboration: Asian Pacifi c perspectivesBangkok, ThailandOctober 6-8, 2004
http://www.iaspbangkok.org/iasp2004/main/index.html
17th International Symposium on Epidemiology in Occupational Health Melbourne, AustraliaOctober 13-15, 2004 Email: [email protected]: http://www.med.monash.edu.au/epidemiology/epicoh/index.html
Suicide Prevention Australia 2004 National ConferenceSydney, Australia October 29-31, 2004http://www.suicidepreventionaust.org/new_conference.htm
2nd International Symposium on Concussion in SportPrague, Czech RepublicNovember 5-6, 2004 http://www.iihf.com/education/pdf/
APSAD 2004 National ConferenceFremantle, Western AustraliaNovember 14-17, 2004Contact: APSAD Conference SecretariatTel 07 3846 5858Fax 07 3846 5859Email: [email protected]
Global Forum for Health Research Forum 8 Mexico City, MexicoNovember 16-20, 2004http://www.globalforumhealth.org
Bold Perspectives, Shared Objectives Injury Prevention and Rehabilitation ConferenceAuckland
March 21-23, 2005Contact: Gillian Boyes, conference organizerTel (029) 200 8985Email: [email protected]
8th World Conference on Injury Prevention and Safety Promotion Johannesburg, South AfricaMarch 19-22, 2006Conference secretariat: Tel +27 (0)12-481 2094Fax +27 (0)12-481 2112Email: [email protected]
American Association of Suicidology 2005 Annual ConferenceBroomfi eld, Colorado April 13-16, 2005
14th International Safe Communities ConferenceBergen, Norway June 13-15, 2005Email:[email protected]@vesta.noWebsite: www.safebergen.com
1st World Congress on Sports Injury Prevention Oslo June 23-25, 2005 http://www.ostrc.no/
XXIII Congress of the International Association for Suicide PreventionScaling the Summit: Suicidal Behaviour in Diverse CulturesDurban, South AfricaSeptember 12-16, 2005http://www.interaction.nu.ac.za
Funding for the New Zealand Injury Control Bulletin (NZICB) is provided by the Accident Compensation Corporation (ACC), Wellington, New Zealand. Views expressed in the NZICB are those of its contributors. They do not necessarily represent the opinion or position of the members of the bulletin’s editorial board, the Injury Prevention Research Centre (IPRC) or the ACC.
Editor:Helen Borne Injury Prevention Research Centre, School of Population HealthUniversity of Auckland, Private Bag 92019, AucklandTel (09) 373 7599 ext 82377, Fax (09) 373 7057 Email [email protected] Website: http://www.auckland.ac.nz/ipc