BY HOSSAM HASSAN DEM CONSULTANT AND ASSISTANT PROFESSOR
Slide 2
History Taking
Slide 3
Introduction As with any part of the physical exam, a complete
cardiac exam should begin with a detailed cardiac history. A good
historian should be able to predict the physical exam findings
before attempting the actual physical exam. A thorough cardiac
history should include investigating for the following cardiac (8)
symptoms.
Slide 4
Chest pain Where is the pain (s)? When did the pain first start
(t)? How long does it last (t)? Does the pain radiate, if so where
? How often do you have the pain ? How would you describe the pain
- burning, pressing, stabbing, crushing, dull, aching, throbbing,
sharp, constricting ? Does the pain occur at rest, with exertion,
with stress, after eating, when moving your arms, or during
intercourse ? Do you have any other symptoms with the pain such as
shortness of breath, palpitations, nausea, vomiting, coughing,
fever, leg pain (as)?
Slide 5
Cyanosis (bluish color skin) Where is the bluish color skin?
How long have you noticed it? Did it seem to happen suddenly or
gradually? What type of work do you do? Does anyone else in your
family has this condition? What makes the bluish skin color better
or worse? Have you had any chest pain, cough, or bleeding
associated with the bluish color skin?
Slide 6
Dyspnea (shortness of breath) How long have you been short of
breath? Did the shortness of breath occur suddenly or gradually? Do
you ever wake up at night feeling short of breath (paroxysmal
nocturnal dyspnea)? How many pillows do you sleep on at night? How
far can you walk before you become short of breath? Have you notice
swelling in your legs associated with your shortness of breath?
Have you had any chest pain associated with your shortness of
breath?
Slide 7
Edema (dependent) Do you have swelling in your legs? When did
you first notice the swelling? Did it appear suddenly or gradually?
Is the swelling worse in the morning or evening? Does the swelling
decrease after a night's sleep? Do your shortness of breath
associated with the swelling? Have you noticed any change in your
weight? Does elevating your feet make the swelling go down? Do you
have pain in your legs associated with the swelling? Do both legs
swell equally? Are you taking any medications, if so, which
ones?
Slide 8
Fainting (syncope) How often do you faint (or feel like you are
going to faint)? What are you doing when you faint (or feel like
you are going to faint)? Have you ever lost consciousness? Does the
fainting (of feeling like you are going to faint) occur suddenly?
In what position were you when you fainted (or felt like you were
going to faint)? periods?
Slide 9
Fainting (syncope) Have you noticed anything that seem to be
associated with the fainting (feeling like you are going to faint),
for example, chest pain, irregular heart beat, nausea, confusion,
hunger, tingling, or numbness? Do you have any black, tarry bowl
movements after the fainting episode.
Slide 10
Fatigue How long have you felt fatigued? Did the fatigue come
on suddenly or gradually? Do you feel tired all day or only in the
morning and/or evening? Do you feel more tired at home or at work?
Is your fatigue relieved by rest? When do you feel least
tired?
Slide 11
General Have you ever had any problems with your heart? Have
you ever had angina or a heart attack? Have you ever had a cardiac
catheterization or heart surgery? Do you have high blood pressure?
Have you ever been told you had a heart murmur or had rheumatic
fever? Have you ever had phlebitis (pain) or swelling in your
legs?
Slide 12
Hemoptysis (coughing up blood) How long have you been coughing
up blood? How often do you cough up blood? Do you have chest pain
when you cough up blood? How much blood do you cough up
Slide 13
Irregular Heart Beat Do you have any problems with irregular
heart beat or palpitations (when you can feel your heart beating
fast or irregular)? How long have you had the irregular heart
beats? When did you first notice the irregular heart beats? How
long did the irregular heart beats last? What did the irregular
heart beats feel like? Did anything you do stop the irregular heart
beats? Did the irregular heart beats stop abruptly? Could you count
your pulse during the episode?
Slide 14
Irregular Heart Beat Can you tap on the table what the rhythm
felt like? Have you noticed the irregular heart beats during
exercise? Did you experience any sweating, flushing, or headaches
with your irregular heart beats? Are you taking any medications, if
so, which ones? Has anyone ever told you that you had problems with
your thyroid gland? Do you smoke or use any other recreational or
street drugs, if so, how much and how often? How much caffeine do
you drink a day (coffee, tea, soft drinks)? After the irregular
heart beats, do you need to urinate?
Slide 15
EXAMINATION Inspection Like any part of the physical exam a
thorough cardiac exam should begin with inspection. For the cardiac
exam the patient should be supine at 30 degrees, ideally without
any clothes on their chest or just a bra, or at the most a hospital
gown. A thorough inspection for the cardiac exam involves not only
looking at the area of the body in close proximity to the heart
(chest), but also other areas of the body (eyes, mouth, skin),
which although anatomically remote to the heart, give us a window
into the cardiovascular systemchesteyesmouthskin
Slide 16
Neck Look for raised JVP 4-11 cm
Slide 17
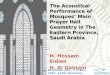
Chest Observe the chest for overall torso contour. Do you see
pectus excavatum (caved-in chest)? Do you see pectus carinatum
(pigeon chest)? Can you see any cardiac motion?
Slide 18
Pectus Exacavatum
Slide 19
Pectus Carinatum
Slide 20
Eyes The presence of yellowish plaques on the eyelids
(xanthelasma) could indicate hyperlipoproteinemia, a risk factor
for hypertension as well as arteriolosclerosis.
Slide 21
Mouth The presence of petechiae (small red or purple spots
containing blood that appears in skin or mucous membrane), shown
here on the skin, but which can also appear on mucous membranes,
especially on the palate, can be a sign of subacute
endocarditis.
Slide 22
Slide 23
Skin Clubbing The presence of clubbing (broadening of the
extremities of the digits, accompanied by nails which are
abnormally curved and shiny) indicates chronic poor oxygen
perfusion to the distal tissues of the hand and feet.
Slide 24
Slide 25
Cyanosis The presence of cyanosis (bluish color) also denotes
chronic poor oxygen delivery to the peripheral tissues of the hands
and feet. Cyanosis can be found in patients with many different
cardiac and pulmonary conditions.
Slide 26
Slide 27
Edema The presence of edema (tissue swelling) can be caused by
several factors, although most commonly is associated with
decreased cardiac function leading to decreased capillary flow.
This decreased flow in turns leads to increased fluid perfusion,
especially in the gravity dependent areas of the body (e.g. arms
and legs) which causes the swelling.
Slide 28
Slide 29
Xanthomas The presence of yellowish plaques under the skin
(non-eruptive) excoriated through the skin (eruptive) could
indicate hyperlipoproteinemia, a risk factor for hypertension as
well as arteriolosclerosis
Slide 30
Slide 31
Palpation Point of Maximal Impact (PMI) The point of maximal
impact (PMI) is the location on the anterior chest wall where the
apex of the heart is felt most strongly. It can be felt in 70% of
individuals in the sitting/standing position or in the left lateral
decubitus position. Palpate for the PMI as follows:
Slide 32
Place the patient's chest so that the heart is thrust
anteriorly either in the upright position (either sitting or
standing) or left lateral decubitus position (NOT in the supine
position). Place your fingertips in the fifth intercostal space and
the left midclavicular line (PMI is normally within 10 cm of the
sternum on the left side). Note the location of the PMI. Note the
size of the PMI (PMI is normally 2-3 Cm in diameter). A large,
laterally displaced, or diffuse PMI generally indicates some form
of cardiomegaly.
Slide 33
Localized Motion Palpate for localized motion as follows: Place
the patient in the supine position. Place your fingertips in each
of the four precordial regions (aortic, pulmonary, tricuspid, and
mitral). Note any impulses felt (e.g. a systolic impulse at the
second left intercostal space could indicate pulmonary
hypertension).
Slide 34
Generalized Motion Palpate for generalized motion as follows:
Place the patient in the supine position. Place the proximal part
of your hand (not fingers) in each of the four precordial regions.
Note any heaves, lifts, or rocks (synonymous words indicating large
cardiac pulsations felt on palpation).
Slide 35
Thrills Thrills are vibratory sensations caused by the heart
and felt on the body surface. Thrills are always associated with
murmurs. Palpate for thrills as follows: Place the patient in the
supine position. Use the proximal part of your hand (not
fingers)and press gently over the anterior chest wall over the
heart. Note any thrills appreciated.
Slide 36
Percussion does have a small role in the cardiac exam, although
its role in the cardiac exam is much less then in other parts of
the physical exam such as the abdominal or pulmonary exam.
Slide 37
Cardiac percussion is performed at the third, fourth, and fifth
intercostal spaces from the left axillary to the right axillary
lines. Normal cardiac percussion should show dullness to percussion
from the sternum to approximately 6 cm lateral to the left of the
sternum.
Slide 38
Auscultation Listening to the heart you can gather information
about the 1)rate and rhythm, 1) 2) value functioning (e.g.
stenosis, regurgitation/insufficiency), and 3) anatomical defects
(e.g. atrial septal defects, ventricular septal defect (VSD),
hypertrophy).
Slide 39
Auscultation In describing and documenting a murmur, you should
be able to characterize 4 properties of an abnormal heart sound:
The location of the heart sound on the chest (i.e. where is it
heard loudest and where you can hear the sound at all). The timing
of the heart sound (i.e. early diastolic, pan systolic, etc.) The
grade or intensity of the heart sound (i.e.1-6 (see table below))
The quality and shape of the heart sound (i.e. musical crescendo,
harsh snap, etc.)
Slide 40
Auscultation Where to place your stethoscope auscultation
should proceed in a logical manner over 4 general areas on the
anterior chest, beginning with the patient in the supine position.
The 4 percordial areas are examined with diaphragm, including:
Aortic region (between the 2nd and 3rd intercostal spaces at the
right sternal border) (RUSB right upper sternal border). Pulmonic
region (between the 2nd and 3rd intercostal spaces at the left
sternal border) (LUSB left upper sternal border). Tricuspid region
(between the 3rd, 4th, 5th, and 6th intercostal spaces at the left
sternal border) (LLSB left lower sternal border). Mitral region
(near the apex of the heard between the 5th and 6th intercostal
spaces in the mid-clavicular line) (apex of the heart).
Slide 41
Auscultation After this initial examination in the supine
positions, several additional maneuvers should be accomplished in
the thorough cardiac exam, as follows: Instruct the patient to turn
onto their left side (left decubitus position) and listen with the
bell of the stethoscope at the apex for mitral stenosis (low
pitched diastolic murmur). Instruct the patient to sit upright and
re-examine the 4 percordial regions, again with the diaphragm of
the stethoscope. Instruct the patient to lean forward, exhale, and
hold their breath. Listen with the diaphragm between the second and
third intercostal spaces at the right sternal (aortic) and left
sternal (pulmonic) areas for aortic regurgitation.
Slide 42
Murmurs Grade 1/6:very faint, only heard in ideal circumstance
2/6:loud enough to be generally hear 23/6:louder than grade
4/6:Louder than grade 3 5/6:heard with stethoscope partially off
chest :Heardwith stethoscope entirely off chest 66/
Slide 43
Murmur Descriptions Description Possible Diagnosis Systolic
ejection murmur Normal, pulmonic, or aortic stenosispulmonicaortic
stenosis Early diastolic murmur Aortic regurgitationAortic
regurgitation Ejection SoundEjection Sound Aortic valve disease
Pansystolic murmur Tricuspid or mitral
regurgitationlTricuspidmitraregurgitationl Late diastolic murmur
Tricuspid or mitral stenosisTricuspidmitral stenosis Systolic click
with late systolic murmur Mitral valve prolapseMitral valve
prolapse
Slide 44
Auscultation Mitral stenosis Opening snap with diastolic rumble
murmur Normal in children and occurs in heart failure s3
Physiological and in various diseas S4
Slide 45
Heart Sounds Normal sinus rhythm (at rates of ~60, ~90, and
~130beats per minutes).~60~90 ~130