Embed Size (px)
Citation preview

By Elizabeth W. Woodcock, MBA, FACMPE, CPC

2015©
2
Elizabeth W. Woodcock, MBA, FACMPE, CPC
Speaker, Author, Trainerwww.elizabethwoodcock.com� MBA, Wharton School of Business, University of Pennsylvania
� BA, Duke University
� Fellow, American College of Medical Practice Executives
� Certified Professional Coder
� Author, 15 textbooks and more than 500 Articles
� Founder and Principal, Woodcock & Associates
� Former Consultant, Medical Group Management Association; Group
Practice Services Administrator, University of Virginia Health Services
Foundation; Former Senior Associate, Health Care Advisory Board
©2

2015©
3
� Federal Government� New Payer in the Market� Meaningful Use
� ICD10� PQRS
� VBPM� Penalties � Future

2015©
4
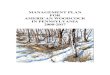
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Law
Actual
Exception - 2014Q1 had a 0.5% rate increase
-0.77%

2015©
5
CARC CO253Adjustment code for mandated Federal, State
or Local law/regulation
CARC=Claim adjustment reason code

2015©
6
CPT Descriptor2015
wRVU
Proposed
2016 wRVU
Final
Work RVU
Final % Change
45330 Flexible sigmoidoscopy 0.96 0.77 0.84 -13%
45378 Colonoscopy 3.69 3.29 3.36 -9%
45380 Colonoscopy w/ Biopsy 4.43 3.59 3.66 -17%
45382 Colonoscopy w/ Control of Bleeding 5.68 4.76 4.76 -16%
45388Colonoscopy, Flexible with Ablation 5.86 4.98 4.98 -15%
Revaluing of the lower GI
endoscopy codes, including…
Pathology – 8% Increase

2015©
7
Average cuts based on claims processed under the taxonomy
code associated with the specialty; represents RVU changes
only. Includes physician specialties only. All other specialties
0% impact.
Review Your Appendix
Pathology 8% Gastroenterology -4%
Interventional Radiology 1% Radiation Oncology -2%
Dermatology 1% Neurosurgery -1%
Plastic Surgery 1% Neurology -1%
Colorectal Surgery -1%
Nuclear Medicine -1%
Ophthalmology -1%
Physical Medicine & Rehab -1%
Vascular Surgery -1%

2015©
8
99497 Advance care planning including the explanation and discussion of
advance directives such as standard forms (with completion of such
forms, when performed), by the physician or other qualified health professional; first 30 minutes, face-to-face with the patient, family
member(s) and/or surrogate
+ Add-on 99498 … each additional 30 minutes
CPT Work RVU
99497 1.50
99498 1.40
Subject to Cost-Sha
ring
except when billed w
ith
an AWV
•Modifier -33
•Separately payable
AWV = Annual Wellness Visit (Medicare) 8

2015©
9
99490 Chronic Care Management Services
99495 and 99496 Transitional Care Management
DOS: Date of the E/M Visit
[in contrast to the final day of the
30-day period post-discharge]
“Direct”supervision is
required

2015©
10
Supervising = Billing

2015©
11
“…we continue to seek a better understanding regarding the growing trend toward hospital acquisition of physicians’ offices and how the subsequent treatment of
those locations as off-campus provider-based outpatient departments affects payments under PFS and beneficiary cost-sharing.”
-CMS 2015 Medicare Physician Fee Schedule Final Rule (11/14)
-22 – On-C[mpus
-19 – Off-C[mpus
Effective January 1, 2016
New Place of Service CodesHospital Outpatient Departments (OPDs)
250 Yards

2015©
12
• Halted all Provider-based
Billing Site Differential
Payments Made to Off-
Campus Hospital Outpatient Departments (OPDs) as of
January 1, 2017. All OPDs
that were in place as of
November 2, 2015 are exempt (grandfathered)
• Extended Sequestration for
One More Year – through
December 31, 2025

2015©
13
Primary Care Incentive Program (PCIP)
2011-2015*
Medicare reimbursement: Bonus of 10% of payments
for selected codes, paid quarterly
•Primary care (IM, FP, Peds, Geriatrics; Physicians, NPs,
PAs and CNSs) for whom primary care services account
for at least 60% of allowed charges – based on the
definition, may include advanced practice providers
working with a specialist
©
*Dates of service January 1, 2011 through December
31, 2015
HPSA Surgical Incentive
Payment (HSIP)

2015©
14
69209the removal of impacted cerumen using irrigation/lavage
(unilateral)
99415-6 Prolonged, face-to-face clinical staff services under direct
supervision
99406-9 Behavior change intervention can be reported with a -25 modifier
in addition to preventive services
Changes
Also… Vaccines | Radiology | Respiratory | Urinary… and

2015©
15

2015©
16
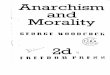
Commercial
Government
Self 100%
<5%
50%
5%
35%
60%
32%32%32%32%
Source: Woodcock & Associates analysis of professional fee receivables, 2015.
Patient Financial
Responsibility

2015©
17
1st
Year
Meaningful Use Annual Incentive Payments
2011 2012 2013 2014 2015 2016 [….] TOTAL
2011 MCR $18,000 $12,000 $8,000 $4,000 $2,000 $0 $0 $44,000
MCD $21,250 $8,500 $8,500 $8,500 $8,500 $8,500 $0 $63,750
2012 MCR $18,000 $12,000 $8,000 $4,000 $2,000 $0 $44,000
MCD $21,250 $8,500 $8,500 $8,500 $8,500 $8,500 $63,750
2013 MCR $15,000 $12,000 $8,000 $4,000 $0 $39,000
MCD $21,250 $8,500 $8,500 $8,500 $17,000 $63,750
2014 MCR $12,000 $8,000 $4,000 $0 $24,000
MCD $21,250 $8,500 $8,500 $25,500 $63,750
2015 MCR $0 $0 $0 $0
MCD $21,250 $8,500 $34,000 $63,750
2016 MCR $0 $0 $0
MCD $21,250 $ 42,500 $63,750
MCR = Medicare; MCD = Medicaid. MCD participants must begin participation by 2016.

2015©
18
CMS Final RuleOctober 16, 2015
[Last Day to Start in Order to Get the
90 Days in]

2015©
19
Eliminated!!• Patients who secure electronic
message• Patients who download, view online or
transmit to a third party their health
information electronically
Stages are Collapsed = “Modified Stage Two”

2015©
20
1. Protect Electronic Health Information2. Clinical Decision Support (CDS)– 5 rules for 4+ CQMs or high priority
health conditions; drug-drug and drug-allergy interaction checks3. CPOE – 60% meds; 30% lab and radiology orders4. ePrescribing – 50% queried for drug formulary and transmitted
electronically5. Summary of Care – create and transmit for 10% transitions of care and
referrals
6. Patient-specific education – 10% of all unique patients7. Medication reconciliation – 50% of all transitions of care
8. Patient electronic access – 50% provided access within 4 business days; one patient views, downloads or transmits
9. Secure electronic messaging – [Y or N] – capability?
10. Public Health/Clinical Data Registry Reporting

2015©
21
Based on Using “Exceptions” –
1.Protect Electronic Health Information
2.CDS – 1 rule relevant to specialty/high clinical priority
3.CPOE – 30% medications only4.ePrescribing – 40% transmitted electronically
5.Patient electronic access – 50% provided access
within 4 business days6.Public Health/Clinical Data Registry Reporting –
same as Modified Stage Two

2015©
22
[EHR Incentive Programs] If an EP, eligible hospital or Crit ical Access Hospital (CAH) is unable to
effectively plan for a report ing period in 2015 due to the timing of the publication of the 2015 through
2017 Modificat ions final rule, can they apply for a hardship exception?Yes, if a provider is unable to meet the requirements of meaningful use for an EHR report ing period in
2015 for reasons related to the timing of the publication of the final rule, a provider may apply for a
hardship exception under the "extreme and uncontrollable" c ircumstances category. Each hardship
exception application will be reviewed on a case-by-case basis, as required by law.In the past, CMS has considered these applications seriously and, in fact, has approved over 85% of
hardship exemptions.
(FAQ 12845)
Source: https://questions.cms.gov/faq.php?id=5005&faqId=12845

2015©
23
� First, EPs scheduled to be in Stage 1 may attest to only 1 public health
measure instead of 2...
� Second, we will allow providers to claim an alternate exclusion for a
measure if they did not intend to attest to the equivalent prior menu
objectiveSource: CMS https://questions.cms.gov/faq.php?id=5005&faqId=12985
Examples:
Rheumatology Informatics System for Effectiveness (RISE)
GIQuIC Colonoscopy Quality Registry
Digestive Health Recognition Program Registry
DataDerm™ registry
State Cancer Registry -
http://epi.grants.cancer.gov/registries.html#state
Not meant to be an exhaustive list

2015©
24
•Transmitted via email
•Review the audit request – complete? limited (to one measure)?
•Retain documentation for 6 years
•CMS – and (2015) OIG
http://go.cms.gov/1J6buIshttp://bit.ly/1dB9eg3
Audit InformationGovernment Sample

2015©
25
DATE OF SERVICE
2015
“The Secretary of Health and Human
Services may not, prior to October 1,
2015, adopt ICD–10
code sets as the standard for code
sets…”
Source: Protecting Access to Medicare Act, April 1, 2014

2015©
26
V91.07XD
Burn due to water-skis
on fire, subsequent
encounter
Denials??CO11 - The diagnosis is inconsistent w ith the procedure. (…or Age, Gender or Provider Type)CO16 - Claim/service lacks information or has submission/billing error(s) w hich is needed for adjudication.
CO50 - These are non-covered services because this is not deemed a 'medical necessity' by the payer.CO146 - Diagnosis w as invalid for the date(s) of service reported.
CO15 - The authorization number is missing, invalid, or does not apply to the billed services or provider.
ICD10 - The code is wrong.

2015©
27
Metrics October 1-27, 2015 Historical Baseline*Total Claims Submitted 4.6 million per day 4.6 million per day
Total Claims Rejected
due to incomplete or invalid information
2.0% of total claims submitted
2.0% of total claims submitted
Total Claims Rejected due to invalid ICD-10
codes
0.09% of total claims
submitted
0.17% of total claims
submitted
Total Claims Rejected
due to invalid ICD-9
codes
0.11% of total claims
submitted
0.17% of total claims
submitted
Total Claims Denied10.1% of total claims
processed
10% of total claims
processed
*Metrics for total ICD-9 and ICD-10 clai ms rejecti ons w ere es ti mated based on end-to- end testing conducted in 2015 si nce CMS has not historically collected this data. Other metrics are based on
historical clai ms submissions.
Source: CMS, https:/ /www.cms.gov/Newsroom/Medi aReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-10-29.html

2015©
28
1. No denials on the basis of specificity (only)
for 12 months.2. Advance payments available.
3. Ombudsman.
Humana and United said… they had
adopted a liberal approach to specificity
as long as the codes made sense…~10/15 MGMA “Town Hall” meeting, as reported by Robert Tennant, senior pol icy adv isor for the Medic al Group Management Association
July 2015

2015©
29
2015 PQRS Implementation
2015 PQRS Implementation Guide: Guide:
http://go.cms.gov/1aI1SXl
http://go.cms.gov/1aI1SXlMeasures:
Measures:
http://go.cms.gov/1ev2vjp
http://go.cms.gov/1ev2vjp
Can also qualify for MU CQMs
2+ Eligible ProfessionalsCan also qualify for MU CQMs
Can report 1 measures group
Not limited to PQRS measures

2015©
30
2016-2%*
281 Measures & 18 in GPRO

2015©
31
Size of
Group
Paymt
Adj’mt
Perf’ce
Year
100+ 2015 2013
10+ 2016 2014
All 2017 2015
Automatic Penalty
1% (2015)*
2% (2016)+
2% for <9 EPs; 4% for >9 (2017)+
*Must have reported through GPRO
+GPRO – or at leas t 50% of the EPs in the TIN must have reported. The exception is
solo practitioners, w ho mus t participate success fully.

2015©
32
Cost measures, including total per capita, condition-specific, and spending per hospital patient
Quality measures, including
hospital admissions for ambulatory care sensitive conditions
and all-cause hospital readmissions
Except M
CR Part
D outp
atient
presc
riptio
n drugs
Exempt if <125 cases

2015©
33
Download your Quality and Resource Use Report Today!
You’ll need an IACS (Individuals Authorized Access
to the CMS Computer Services) user ID and
password
You won’t get one if you participate in the Medicare Shared
Savings Program, the Pioneer ACO Model, or the Comprehensive Primary Care Initiative
http://go.cms.gov/1JjoXvb
Read CMS’ Document “Action for Physicians… to Take In Order To
Earn an Incentive Based on Performance and Avoid the Automatic CY
2017 Downward Payment Adjustment under the VBPM”!
1.1.
2.2.
http://go.cms.gov/1DtymQu

2015©
34
34
Year eRx PQRS EHR VBPM+
Seques-
tration~ Total
2012 -1.0% - - - - -1.0%
2013 -1.5% - - - -2.0% -3.5%
2014 -2.0% - - - -2.0% -4.0%
2015 - -1.5% -1.0% -1.0% -2.0% -5.5%
2016 - -2.0% -2.0% -2.0% -2.0% -8.0%
2017 - -2.0% -3.0% -4.0% -2.0% -11.0%
2018 - -2.0% up to -5% -4.0% -2.0% up to -13%
+\Table reports maximum penalty.~Applies only to Medicare payment, not the allowable
In 2013, the Sequestration cuts started in April of that year.
Applied to all Medicare reimbursement
2015 Performance

2015©
35
However, every eligible professional will be assigned a “composite score”
Will replace PQRS, VBPM and MU!
1. Participate in an
Alternative Payment Model �
2. Low MCR volume
3. New provider
Category Yr 1
(2019)
Yr 2
(2020)
2021 +
Quality 50% 45% 30%
Meaningful Use* 25% 25% 25%
Resource Use 10% 15% 30%
Clinical Practice
Improvement
15% 15% 15%
Max. Reduction (4%) (5%) (7%-9%)
*MU weight can decreas e to 15% if adoption reaches 75%; the weight would then be
redistributed to another category.

2015©
36
� Clinical Practice Improvement?
� Expanded practice access
� Population management
� Care coordination
� Beneficiary engagement
� Patient safety and practice assessment
or "comparable specialty practice"

2015©
37
� Promoting health equality and continuity
� Accepting new Medicaid (MCD) patients
� Service MCD or MCR/MCD patients
� Participating in the ACA exchange
� Underserved populations
� Integration of behavioral health
� Emergency preparedness and response
PROPOSALPROPOSALPROPOSALPROPOSAL
October 2 015
MCD=Medicaid; MCR=Medicare

2015©
38

2015©
39
Question &
Answer
Session

2015©
40
Elizabeth W. Woodcock, MBA, FACMPE, CPC
Woodcock & Associates
Speaker, Trainer, Author
Atlanta, Georgia
404.373.6195
www.elizabethwoodcock.com
These handouts may not be reproduced without the written consent of the speaker.