Embed Size (px)
Citation preview

Oxidative Medicine Revisited
By Dr. Michael A. Prytula ND and staff

Include Ozone, UVB, Hydrogen Peroxide, Hyperbaric Oxygen and by mechanism of action….
Ascorbic Acid in high dosages
Oxidative Therapies
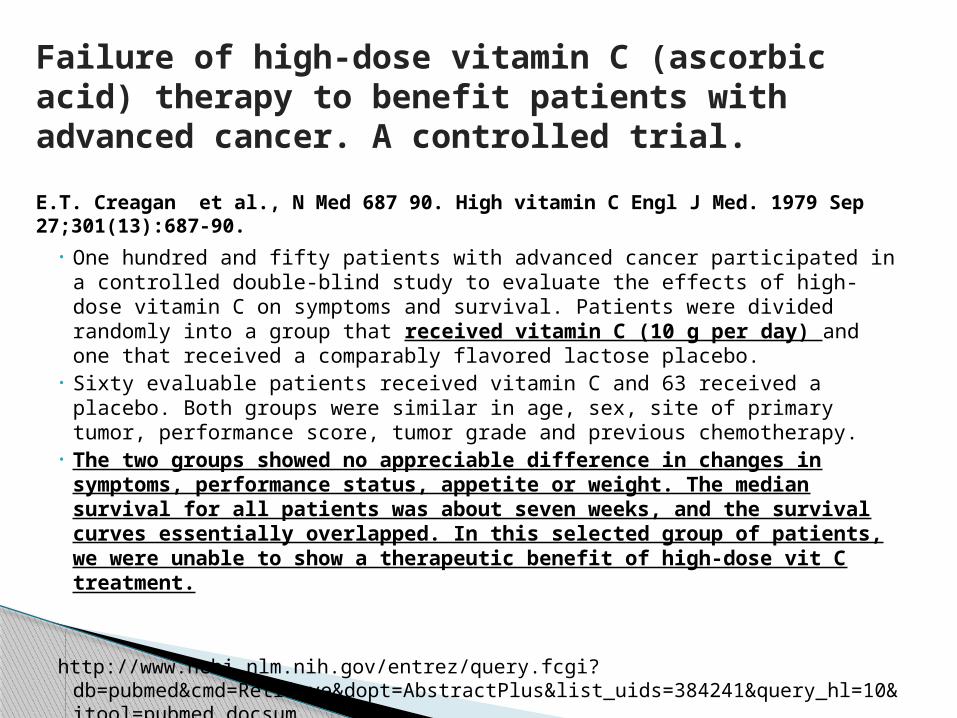
• One hundred and fifty patients with advanced cancer participated in a controlled double-blind study to evaluate the effects of high-dose vitamin C on symptoms and survival. Patients were divided randomly into a group that received vitamin C (10 g per day) and one that received a comparably flavored lactose placebo.
• Sixty evaluable patients received vitamin C and 63 received a placebo. Both groups were similar in age, sex, site of primary tumor, performance score, tumor grade and previous chemotherapy.
• The two groups showed no appreciable difference in changes in symptoms, performance status, appetite or weight. The median survival for all patients was about seven weeks, and the survival curves essentially overlapped. In this selected group of patients, we were unable to show a therapeutic benefit of high-dose vit C treatment.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=384241&query_hl=10&itool=pubmed_docsum
Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer. A controlled trial.
E.T. Creagan et al., N Med 687 90. High vitamin C Engl J Med. 1979 Sep 27;301(13):687-90.

Tight Control of Ascorbic Acid Plasma Concentrations as a Function of Oral Dose
Fasting Steady State Concentrations in Plasma in Men (○) and Women (●):

Predicted Plasma Concentrations IV vs Oral

Intravenously administered vitamin C as cancer therapy: three casesSebastian J. Padayatty, Hugh D. Riordan, Stephen M. Hewitt, Arie Katz, L. John Hoffer, Mark Levine
CMAJ • March 28, 2006; 174 (7).
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1405876/pdf/20060328s00017p937.pdf

Early clinical studies showed that high-dose vitamin C, given by intravenous and oral routes, may improve symptoms and prolong life in patients with terminal cancer. Double-blind placebo-controlled studies of oral vitamin C therapy showed no benefit. Recent evidence shows that oral administration of the maximum tolerated dose of vitamin C (18 g/d) produces peak plasma concentrations of only 220 μmol/L (.220 mM) , whereas intravenous administration of the same dose produces plasma concentrations about 25-fold higher. Larger doses (50–100 g) given intravenously may result in plasma concentrations of about 14 000 μmol/L (14 mM). At concentrations above 1000 μmol/L, vitamin C is toxic to some cancer cells but not to normal cells in vitro. We found 3 well-documented cases of advanced cancers, confirmed by histopathologic review, where patients had unexpectedly long survival times after receiving high-dose intravenous vitamin C therapy. We examined clinical details of each case in accordance with National Cancer Institute (NCI) Best Case Series guidelines. Tumour pathology was verified by pathologists at the NCI who were unaware of diagnosis or treatment. In light of recent clinical pharmacokinetic findings and in vitro evidence of anti-tumour mechanisms, these case reports indicate that the role of high-dose intravenous vitamin C therapy in cancer treatment should be reassessed.
Abstract

Pharmacologic ascorbic acid concentrations selectively kill cancer cells: Action as a pro-drugto deliver hydrogen peroxide to tissues
Qi Chen, Michael Graham Espey, Murali C. Krishna, James B. Mitchell, Christopher P. Corpe, Garry R. Buettner, Emily Shacter, and Mark Levine
PNAS September 20, 2005 vol. 102 no. 38 13604-13609
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1224653/pdf/pnas-0506390102.pdf
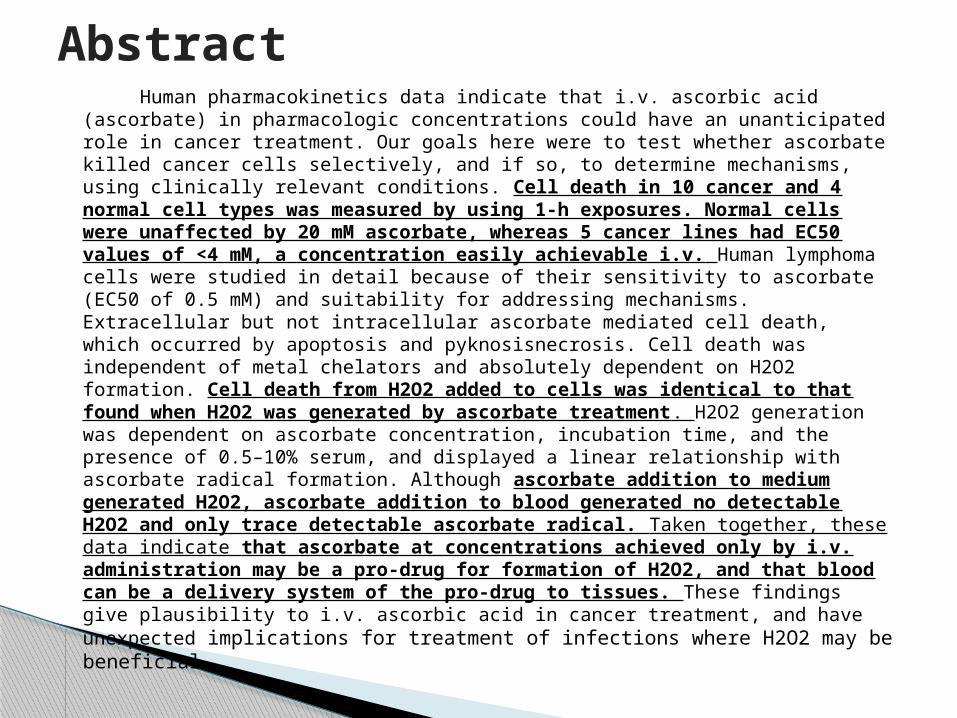
Human pharmacokinetics data indicate that i.v. ascorbic acid (ascorbate) in pharmacologic concentrations could have an unanticipated role in cancer treatment. Our goals here were to test whether ascorbate killed cancer cells selectively, and if so, to determine mechanisms, using clinically relevant conditions. Cell death in 10 cancer and 4 normal cell types was measured by using 1-h exposures. Normal cells were unaffected by 20 mM ascorbate, whereas 5 cancer lines had EC50 values of <4 mM, a concentration easily achievable i.v. Human lymphoma cells were studied in detail because of their sensitivity to ascorbate (EC50 of 0.5 mM) and suitability for addressing mechanisms. Extracellular but not intracellular ascorbate mediated cell death, which occurred by apoptosis and pyknosisnecrosis. Cell death was independent of metal chelators and absolutely dependent on H2O2 formation. Cell death from H2O2 added to cells was identical to that found when H2O2 was generated by ascorbate treatment. H2O2 generation was dependent on ascorbate concentration, incubation time, and the presence of 0.5–10% serum, and displayed a linear relationship with ascorbate radical formation. Although ascorbate addition to medium generated H2O2, ascorbate addition to blood generated no detectable H2O2 and only trace detectable ascorbate radical. Taken together, these data indicate that ascorbate at concentrations achieved only by i.v. administration may be a pro-drug for formation of H2O2, and that blood can be a delivery system of the pro-drug to tissues. These findings give plausibility to i.v. ascorbic acid in cancer treatment, and have unexpected implications for treatment of infections where H2O2 may be beneficial.
Abstract
Physiologic (0.1mM) and pharmacologic
concentrations (0.3~20mM), adjusted to pH 7
1~2 hours exposure 43 cancer cell lines and 5 types of normal
cells Assays to check survival: MTT, Alamar blue,
nuclear staining, colony formation
Conditions were chosen tomimic clinical intravenous use

Pharmacologic ascorbic acid concentrationskill some cancer cells but not normal cells

Concentration dependence of cell death: humanlymphoma (JLP119) vs normal lymphocytes & monocytes

Lymphoma cell death: dependent on extracellular ascorbate extracellular, not intracellular

Mechanism is via H2O2

Inhibition of H2O2 formation in blood:Ascorbate radical formation is minimal
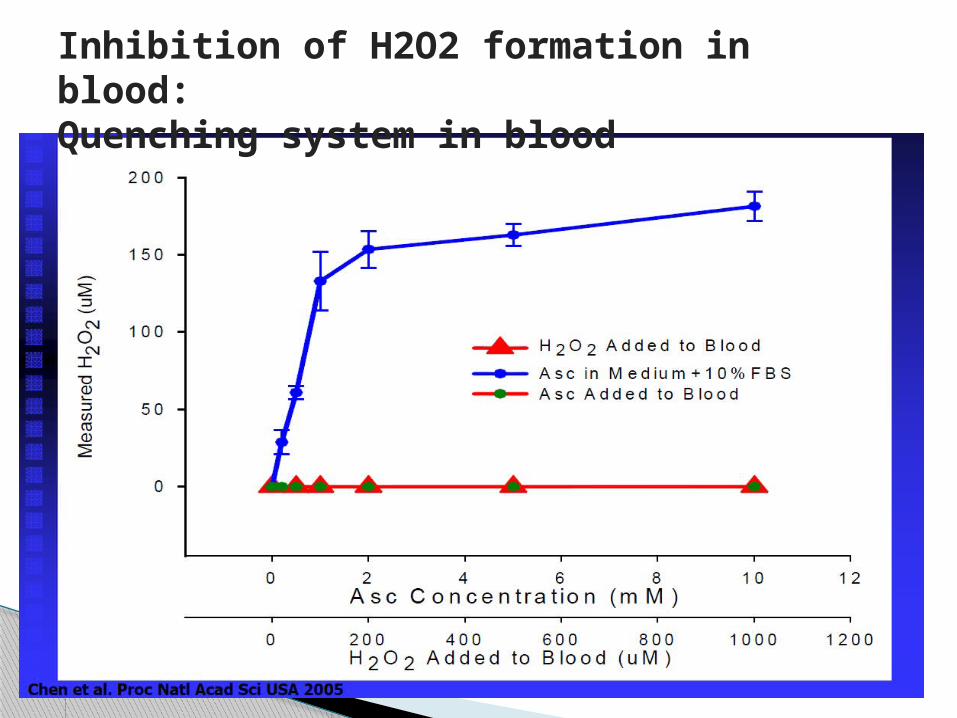
Inhibition of H2O2 formation in blood:Quenching system in blood

Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo
Qi Chen, Michael Graham Espey, Andrew Y. Sun, Je-Hyuk Lee, Murali C. Krishna, Emily Shacter, Peter L. Choyke, Chaya Pooput, Kenneth L. Kirk, Garry R. Buettner, and Mark Levine
PNAS May 22, 2007 vol. 104 no. 21 8749-8754
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1885574/pdf/zpq8749.pdf

Ascorbate (ascorbic acid, vitamin C), in pharmacologic concentrations easily achieved in humans by i.v. administration, selectively kills some cancer cells but not normal cells. We proposed that pharmacologic ascorbate is a prodrug for preferential steady-state formation of ascorbate radical (Asc) and H2O2 in the extracellular space compared with blood. Here we test this hypothesis in vivo. Rats were administered parenteral (i.v. or i.p.) or oral ascorbate in typical human pharmacologic doses (0.25–0.5 mg per gram of body weight). After i.v. injection, ascorbate baseline concentrations of 50–100 M in blood and extracellular fluid increased to peaks of >8 mM. After i.p. injection, peaks approached 3 mM in both fluids. By gavage, the same doses produced ascorbate concentrations of <150 M in both fluids. In blood, Asc concentrations measured by EPR were undetectable with oral administration and always <50 nM with parenteral administration, even when corresponding ascorbate concentrations were >8 mM. After parenteral dosing, Asc concentrations in extracellular fluid were 4- to 12-fold higher than those in blood, were as high as 250 nM, and were a function of ascorbate concentrations. By using the synthesized probe peroxyxanthone, H2O2 in extracellular fluid was detected only after parenteral administration of ascorbate and when Asc concentrations in extracellular fluid exceeded 100 nM. The data show that pharmacologic ascorbate is a prodrug for preferential steady-state formation of Asc and H2O2 in the extracellular space but not blood. These data provide a foundation for pursuing pharmacologic ascorbate as a prooxidant therapeutic agent in cancer and infections.
Abstract
Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice
Qi Chen, Michael Graham Espey, Andrew Y. Sun, Chaya Pooput, Kenneth L. Kirk, Murali C. Krishna, Deena Beneda Khosh, Jeanne Drisko, and Mark Levine
PNAS August 12, 2008 vol. 105 no. 32 11105–11109
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2516281/pdf/zpq11105.pdf

Ascorbic acid is an essential nutrient commonly regarded as an antioxidant. In this study, we showed that ascorbate at pharmacologic concentrations was a prooxidant, generating hydrogenperoxide- dependent cytotoxicity toward a variety of cancer cells in vitro without adversely affecting normal cells. To test this action in vivo, normal oral tight control was bypassed by parenteral ascorbate administration. Real-time microdialysis sampling in mice bearing glioblastoma xenografts showed that a single pharmacologic dose of ascorbate produced sustained ascorbate radical and hydrogen peroxide formation selectively within interstitial fluids of tumors but not in blood. Moreover, a regimen of daily pharmacologic ascorbate treatment significantly decreased growth rates of ovarian (P < 0.005), pancreatic (P < 0.05), and glioblastoma (P < 0.001) tumors established in mice. Similar pharmacologic concentrations were readily achieved in humans given ascorbate intravenously. These data suggest that ascorbate as a prodrug may have benefits in cancers with poor prognosis and limited therapeutic options.
Abstract

Ascorbic acid as a function of time in blood, extracellular fluid, and tumors with 4 g/kg i.p. ascorbate

• IV or IP ascorbate administration creates pro-oxidant ascorbate radical and H2O2 in extracellular fluids but not in blood, consistent with their roles as tumor cytotoxic effectors.
• IV or IP administration achieves pharmacologic concentrations of ascorbic acid, generating ascorbate radical and H2O2 in tissues, with anti cancer effects, and may have effects on diseases that H2O2 or ROS have therapeutic roles, such as infections.
Vit C: Prooxidant!

Book: Hope, Medicine & Healing
by Francisco Contreras, MD & Daniel E. Kennedy, MC
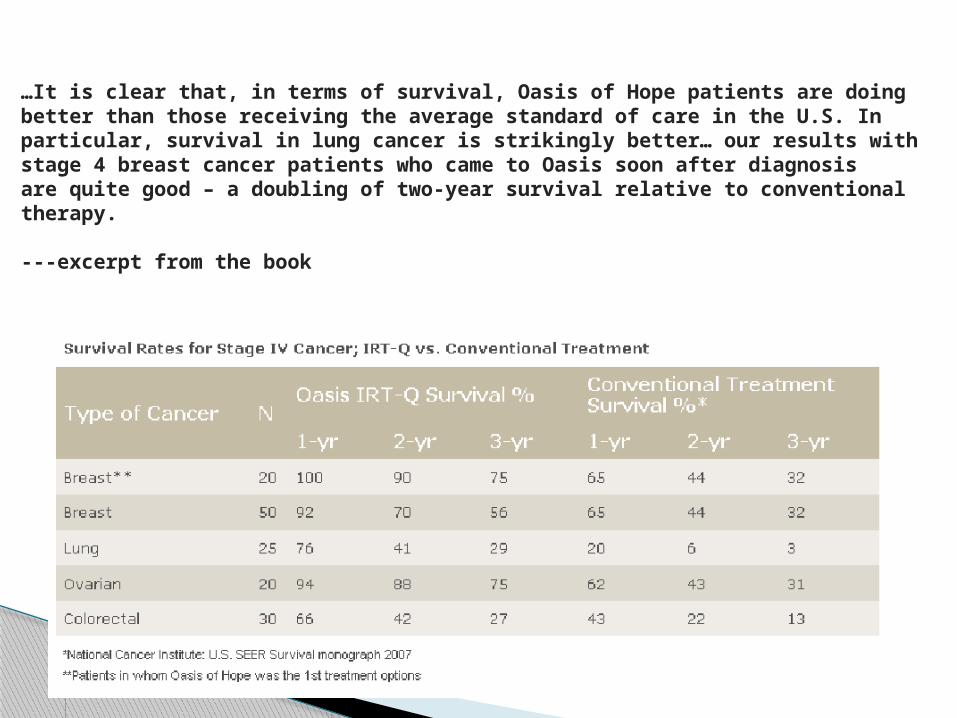
…It is clear that, in terms of survival, Oasis of Hope patients are doingbetter than those receiving the average standard of care in the U.S. Inparticular, survival in lung cancer is strikingly better… our results withstage 4 breast cancer patients who came to Oasis soon after diagnosisare quite good – a doubling of two-year survival relative to conventional therapy.
---excerpt from the book

Hazardous Waste and Hazardous Materials Chemical Oxidation Technologies: Ultraviolet Light/Hydrogen Peroxide, Fenton's Reagent, and Titanium Dioxide-Assisted Photocatalysis
RAJAGOPALAN VENKATADRI, ROBERT W. PETERS.
Hazardous Waste and Hazardous Materials. Spring1993, 10(2): 107-149.doi:10.1089/hwm. 1993.10.107. Published in Volume: 10 Issue 2: April10, 2009 Mary Ann Liebert, Inc. Publishers
http://www.liebertonline.com/doi/abs/10.1089/hwm.1993.10.107

The application status and potential of three chemical oxidation treatment methods which generate powerful oxidants (hydroxyl radicals): ultraviolet light (UV)/hydrogen peroxide (H2O2) process, Fenton's reagent treatment, and titanium dioxide (TiO2)-assisted photocatalytic degradation, are described and discussed. These oxidation methods are known to effectively degrade and, in several cases, mineralize contaminants ranging from inorganic compounds (such as cyanides) to chlorinated aliphatic compounds and complex aromatic compounds in reaction times on the order of a few minutes to a few hours. Of the three oxidation systems discussed, the technology for the UV/H2O2 process is the most advanced, with numerous successful full-scale treatment units already in existence. Applications of both the Fenton's reagent and TiO2-assisted photodegradation processes are currently being developed, with the concepts proven in numerous laboratory-scale studies for a wide range of contaminants. However, both of these processes have only been studied at the pilot/field scale to a limited extent. The application of Fenton's reagent as a pretreatment step prior to biological treatment for industrial wastes and contaminated soils appears promising. Improved system configuration and quantum efficiency of photoreactors are likely to improve the economics of TiO2-assisted photodegradation for groundwater treatment, especially with the use of solar illumination.
Abstract

Degradation of Endocrine Disrupting Chemicals by Ozone/AOPs
BO NING; GRAHAM Nigel; YANPING ZHANG; NAKONECHNY Maureen; MOHAMED GAMAL EL-DIN
Published in: Ozone: Science & Engineering, Volume 29, Issue 3 May 2007 , pages 153 – 176
http://www.informaworld.com/smpp/content~db=all~content=a779407475?words=ozone|cancer&hash=3509892760

The presence of endocrine-disrupting compounds (EDCs) in the aqueous environment is of increasing concern due to their adverse impact on aquatic life, and potential risk to human health. Among the EDCs of concern are steroidal estrogenic hormones such as estrone (E1), 17β-estradiol (E2), estriol (E3), and 17 -ethinylestradiol (EE2), which have a high environmental prevalence and strong estrogenic activity. In addition, the extensive use of alkylphenol ethoxylates (APnEOs), bisphenol A (BPA) and phthalate compounds have resulted in an environmental presence at significant concentrations, although they appear to have a lower estrogenic activity than the steroidal hormones. As water and wastewaters are some of the primary routes of exposure to EDCs, it is important to determine at what levels EDCs are found in these media and how these levels may be reduced. Hence, it is necessary to understand the fate of EDCs in conventional water and wastewater treatment plants, as well as the efficacy of more specialized treatment methods, such as adsorption and oxidation. This paper is a summary of the latest information on the degradation of prominent EDCs by ozone and ozone-based advanced oxidation processes (AOPs). From this review, it is clear that ozone and AOPs are effective in degrading these EDCs, with the possible exception of phthalates, which are relatively stable to ozone oxidation. Knowledge of the formation of reaction products from the treatment by ozone and AOPs is relatively poor at present, particularly for the non-steroid compounds.
Abstract

Ozone Therapy in Cancer Treatment: State of the Art
Silvia Menndeza; Janet Ceperob; Luis Borregoc
Published in: Ozone: Science & Engineering, Volume 30, Issue 6 November 2008 , pages 398 - 404
http://www.informaworld.com/smpp/content~db=all~content=a905990487?words=ozone|cancer&hash=3509892760

Erhlich Ascitic Tumor and Sarcoma 37 were implanted in mice and afterward the animals were treated with ozone (rectally). A significant decrease in the number of metastasis was obtained. In another study, ozone was applied intraperitoneally, before Lewis' lung carcinoma inoculation. A delayed effect in the tumor development kinetics and in the increase rate of tumor volume in the ozone groups was observed. With regard to the clinical trial, patients with prostatic cancer were treated with cobalt-60 therapy and ozone (rectally), decreasing the presence of side effects (due to radiation treatment) and the prostatic specific antigen figures. However, further investigations are necessary to be performed, in order to be considered the ozone therapy as complementary therapy for cancer.
Abstract

• inorganic oxidants: hyperbaric oxygen (O2), singlet oxygen (O2), ozone (O3), hydrogen peroxide (H2O2), magnesium peroxide (MgO2), zinc peroxide (ZnO2), chlorine dioxide (ClO2), chlorite (ClO2-), nitrate ( NO3-), permanganate ( MnO4-), iodine ( I2)
• organic oxidants: organic ozonides (RO3R'), organic peroxides (ROOR'), quinones (Q), alphaketoaldehydes RCOCHO), imidazoles, methylene blue
• sulfur compounds: disulfides (RSSR'), sulfoxides (RSOR'), disulfide monoxides (RSSOR')
• utraviolet light• Ascorbates (in high doses)
A list of clinically useful medicinaloxidants:

1. Withdraw 5cc blood into syringe. Attach to special UVI cuvette.
2. Pass blood into cuvette, but do not remove syringe.
3. Insert cuvette, syringe attached, into receptacle in machine.
4. Turn on timed cycle.5. When cycle complete, withdraw blood into
syringe , remove from cuvette.6. Attach needle and inject IM
UV - IM Technique

• Antibodies have the capacity, on their own, to generate ozone. Investigators found oxidation reactions that could only be attributed to the presence of ozone.
• They believed the raw material source was singlet oxygen generated by activated neutrophils, which provides the energy needed for the antibodies to manufacture ozone
• Hence, ozone is a natural substance produced by the body.
Antibodies Generate Ozone!!Science News, December 2002

Investigating antibody-catalyzed ozone generation by human neutrophils
Bernard M. Babior,, Cindy Takeuchi§, Julie Ruedi, Abel Gutierrez, and Paul Wentworth Jr
Departments of Molecular and Experimental Medicine, Immunology, Chemistry, and The Skaggs Institute for Chemical Biology, The Scripps Research Institute, 10550 North Torrey Pines Road, La Jolla, CA 92037 Contributed by Bernard M. Babior, January 14, 2003
PNAS | March 18, 2003 | vol. 100 | no. 6 | 3031-3034 From the Cover Chemistry / Biochemistry

• Recent studies have suggested that antibodies can catalyze the generation of previously unknown oxidants including dihydrogen trioxide (H2O3) and ozone (O3) from singlet oxygen (1O2) and water. Given that neutrophils have the potential both to produce 1O2 and to bind antibodies, we 2 considered that these cells could be a biological source of O3.
• We report here further analytical evidence that antibody-coated neutrophils, after activation, produce an oxidant with the chemical signature of O3. This process is independent of surface antibody concentration down to 50% of the resting concentration, suggesting that surface IgG is highly efficient at intercepting the neutrophil-generated 1O2
• Vinylbenzoic acid, an orthogonal probe for ozone detection, is oxidized by activated neutrophils to 4-carboxybenzaldehyde in a manner analogous to that obtained for its oxidation by ozone in solution. This discovery of the production of such a powerful oxidant in a biological context raises questions about not only the capacity of O3 to kill invading microorganisms but also its role in amplification of the inflammatory response by signaling and gene activation
Abstract

A. Seda Artis, S. Aydogan & M. Gokhan Sahin. Clin Hemorheol Microcirc. 2010;45(2-4):329-36.
• Erythrocyte deformability, aggregation and osmotic fragility were determined from blood samples at the end of each treatment period.
• The study showed an improvement in deformability, a decrease in aggregation and an increase in fragility following a 15 day ozone treatment.
• With longer ozone application the changes in aggregation and fragility returned back to control levels, however its effect on deformability sustained. Therefore, more than two weeks ozone insufflation may induce adaptation to changes induced by ozone suggesting its systemic effects.
The effects of colorectally insufflated oxygen-ozone on red blood cell rheology in rabbits.
D. Guanche, Z. Zamora, F. Hernádez, K. Mena, Y. Alonso et al. Toxicol Mech Methods. 2010 Jan;20(1):25-30.
• Ozone doses administered to rabbits did not cause adverse effects and mortality did not show significant changes relative to tissue damages and they increased enzymes activities belonging to the first line antioxidant defences. The results demonstrate that ozone/oxygen mixture administered by rectal insufflations is innocuous and it is able to increase the antioxidant defense of the organism.
Effect of ozone/oxygen mixture on systemic oxidative stress and organic damage.

V. Bocci, N. Di Paolo. Blood Purif. 2009;28(4):373-6. Epub 2009 Sep 10
• Ozone therapy is particularly useful in cardiovascular disorders and tissue ischemia. In chronic viral infections, it is unable to eliminate the viremia but it may display supportive help by stimulating the immune system. Recently, its use has been successfully extended to the herniated disk pathology and therapy of primary caries in children.
Oxygen-ozone therapy in medicine: an update
V.A. Neronov. Vopr Kurortol Fizioter Lech Fiz Kult. 2009 Nov-Dec;(6):14-7.
• Patients treated with the use of ozone exhibited better biochemical, virological, and functional characteristics compared with their counterparts managed by standard methods. The results of the study suggest a higher efficiency of combined therapy and reduced risk of development of cholelithiasis.
Experience with the use of ozone for the treatment of chronic viral hepatitis
O.A. Bitkina, T.V. Kopytova, K.N. Kontorshchikova, A.P. Bavrina. Klin Lab Diagn. 2010 Apr;(4):13-6.
• Eighty patients with different clinical types of rosacea were examined; the parameters of primary and intermediate products of lipid peroxidation, superoxide dismutase, plasma total antioxidative activity, and protein oxidative modification were studied. Based on the findings, oxidative therapy options for rosacea, treatment with an ozone-oxygen mixture in particular, are proposed.
Oxidative stress level in patients with rosacea and a rationale for the therapeutic use of an ozone-oxygen mixture

V.M. Kopchak, I.V. Khomiak, A.V. Duvalko, A.A. Stasenko, V.A. Dieiev. Klin Khir. 2008 Oct;(10):28-31.
• Examination and treatment of 32 patients was done, in whom an acute necrotic pancreatitis was diagnosed. In 16 patients (the main group) ozonotherapy, according to scheme, elaborated in the clinic, was added to conventional treatment. The ozonotherapy application had permitted to reduce the rate of performance of "open" operative interventions. The cellular, humoral and local immunity improvement and biochemical indices normalization were noted. The stationary treatment duration was 21.4 days at average in the main group and 34.5 -- in a control one. The relaparotomy performance rate in the main group was lesser than in a control one.
Application of ozone therapy in complex treatment of patients with acute necrotizing pancreatitis

B. Uysal, M. Yasar, N. Ersoz, O. Coskun, A. Kilic et al. Pancreas. 2010 Jan;39(1):9-15.
• Forty Sprague-Dawley rats were divided into sham-operated, acute necrotizing pancreatitis (ANP), ANP + hyperbaric oxygen (HBO), and ANP + ozone therapy (OT) groups.
• Serum amylase/lipase and neopterin levels and tissue oxidative stress parameters were similar to sham's values in both the ANP + HBO and the ANP + OT groups. Histopathologic injury scores were significantly lower in the treatments groups than in the ANP group.
• Hyperbaric oxygen and OT reduce the severity and the mortality in the experimental rat model of ANP, and a greater benefit was received for OT comparing with HBO.
Efficacy of hyperbaric oxygen therapy and medical ozone therapy in experimental acute necrotizing pancreatitis

E.V. Sin’kov. Vestn Otorinolaringol. 2009;(3):34-5.
• Methods of clinical application of gaseous ozone and ozonated solutions for treatment of patients with acute and chronic suppurative middle ear diseases. Results of otoscopy, microbiological and cytological studies confirm therapeutic efficiency of the above techniques as accelerating recovery of patients with this pathology. It is recommended to include ozonotherapy as an additional method in the combined treatment of acute and chronic suppurative otitis media.
Treatment of patients with acute and chronic suppurative middle ear diseases using ozone preparations

V. Bocci, V. Travagli, I. Zanardi. Cardiovasc Hematol Disord Drug Targets. 2009 Jun;9(2):78-85.
• In an aging population vascular disorders well exemplified by the chronic limb ischemia, chronic heart failure, cerebral ischemia and age-related macular degeneration represent a serious medical and socio-economical problem. All of these diseases are characterized by ischemia, chronic inflammation and tissue degeneration. Here it is proposed to associate the approach of ozonated autohemotherapy as a modifier of the biological response capable to block the pathological progress
May oxygen-ozone therapy improves cardiovascular disorders?

MATERIAL AND METHODS: September, 1995, to April, 1997, we treated more than 1000 patients with intradiscal ozone infiltration. We prospectively analyzed the first 50 patients, with 6 months' follow-up at least; all of them were preliminarily submitted to clinical examination, electromyography, CT and MRI. After local anesthesia, we injected the disk, with 18-20 G needles and under CT or fluoroscopic guidance, with 12 ml of a mixture of oxygen and ozone at a concentration of 20-30 micrograms/ml. The treatment was repeated two or three more times at intervals of 3, 15 or, when necessary, 30 days. After each treatment, CT follow-ups were carried out and the final follow-up was made 3 months later.
Ozone therapy in lumbar sciatic pain M.D'Erme et al. Radiol Med. 1998 Jan-Feb;95(1-2):21-4.
RESULTS: We divided our results into clinical and instrumental. As for clinical response, we had 68% positive results (40% excellent, 28% good) and 32% negative results (10% of patients underwent surgery and 22 are under medical and physical treatment). As for CT response, we had 82% positive results (36% excellent, 46% good), while no major changes between pre- and post-treatment CT findings in the remaining 18% of cases.
CONCLUSIONS: Ozone therapy, thanks to its ease of execution and noninvasiveness, permits the successful outpatient treatment of lumbar sciatic pain. Moreover, the lack of major complications and the good results obtained compared to other methods, such as chemonucleolysis, percutaneous automated discectomy, microsurgery and conventional surgery, suggest that ozone therapy can be considered the treatment of choice for lumbar sciatic pain and a valid alternative to surgery in many cases.
METHODS: Six hundred patients were treated with a single session of oxygen-ozone therapy. All presented with clinical signs of lumbar disk nerve root compression, with CT and/or MR evidence of contained disk herniation. Three hundred patients (group A) received an intradiscal (4 mL) and periganglionic (8 mL) injection of an oxygen-ozone mixture at an ozone concentration of 27 micro g/mL. The other 300 patients (group B) received, in addition, a periganglionic injection of corticosteroid and anesthetic. Therapeutic outcome was assessed 6 months after treatment by using a modified MacNab method. Results were evaluated by two observers blinded to patient distribution within the two groups.
Minimally invasive oxygen-ozone therapy for lumbar disk herniation.C.F. Andreula et al., AJNR Am J Neuroradiol. 2003 May;24(5):996-1000
RESULTS: A satisfactory therapeutic outcome was obtained in both groups. In group A, treatment was a success (excellent or good outcome) in 70.3% and deemed a failure (poor outcome or recourse to surgery) in the remaining 29.7%. In group B, treatment was a success in 78.3% and deemed a failure in the remaining 21.7%. The difference in outcome between the two groups was statistically significant (P <.05).
CONCLUSION: Combined intradiscal and periganglionic injection of medical ozone and periganglionic injection of steroids has a cumulative effect that enhances the overall outcome of treatment for pain caused by disk herniation. Oxygen-ozone therapy is a useful treatment for lumbar disk herniation that has failed to respond to conservative management.

M. Muto, C. Andreula, M. Leonardi. J Neuroradiol. 2004 Jun;31(3):183-9
MATERIAL: We report our experience between May 1996 and May 2003 with 2200 patients affected by low back pain or sciatica due to herniated disk treated by intradiscal and intraforaminal oxygen-ozone injection. The patients received medical and physical therapy before treatment for at least 2 months; the patients with conus-cauda syndrome and hyperalgesic sciatica were excluded. We never performed discography before the treatment that was performed under CT guidance or fluoroscopy. CT provided monitoring of gas distribution in the disk and epidural space.
RESULTS: No side effects were recorded at short and long-term follow-up. Clinical results were evaluated with the modified McNab method showing an 80% success rate and 20% failure rate in 1750 patients followed up to 6 months while the success rate dropped down at 75% and failure increased at 25% in 1400 followed up to 18 months. CT showed reduction in the size of the herniated disk in only 63% of the followed patients (420 patients). The failure has been mostly related to: calcified herniated disk; spinal canal stenosis; recurrent herniated disk with epidural fibrosis; small descending herniated disk at the level of the lateral recess.
Treatment of herniated lumbar disc by intradiscal and intraforaminal oxygen-ozone (O2-O3) injection

G. Das, S. Ray, S. Ishwarari, M. Roy, P. Ghosh. Interv Neuroradiol. 2009 Sep;15(3):330-4. Epub 2009 Nov 4.
• Pain intensity was significantly reduced following treatment (Visual Analog Score baseline 7.58-/+0.86, after three weeks 2.75-/+1.42 and after two years 2.64-/+2.14).
• Oswestry disability index showed a remarkable improvement in the functional status of the patients (p<0.05).
• Oxygen-ozone treatment is highly effective in relieving low back pain due to lumber disc herniation.
Ozone nucleolysis for management of pain and disability in prolapsed lumber intervertebral disc. A prospective cohort study.

M. Paoloni, L. Di Sante, A. Cacchio, D. Apuzzo, S. Marotta et al. Spine (Phila Pa 1976). 2009 Jun 1;34(13):1337-44.
• A significant difference between the 2 groups in the percentage of cases who had become pain-free (61% vs. 33%, P < 0.05) was observed at 6 months. Patients who received O2O3 had a lower mean pain score than patients who received simulated therapy throughout the observation period. A significant improvement was observed in LBP-related disability in the study group patients when compared with the control group patients. Active O2O3 therapy was followed by a significantly lower number of days on nonsteroidal anti-inflammatory drugs at 15 days, 30 days and by a lower number of days at 2 weeks. No adverse events were reported.
• O2O3 intramuscular lumbar paravertebral injections, which are minimally invasive, seem to safely and effectively relieve pain, as well as reduce both disability and the intake of analgesic drugs in low back pain and sciatica.
Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: a multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection.

J.B. Staal, R.A. de Bie, H.C. de Vet, J. Hildebrandt, P. Nelemans. Spine (Phila Pa 1976). 2009 Jan 1;34(1):49-59.
• METHODS: We updated the search of the earlier systematic review and searched the Cochrane Central Register of Controlled Trials, MEDLINE, and EMBASE databases up to March 2007 for relevant trials reported in English, French, German, Dutch, and Nordic languages. We also screened references from trials identified. RCTs on the effects of injection therapy involving epidural, facet, or local sites for subacute or chronic low back pain were included. Studies that compared the effects of intradiscal injections, prolotherapy, or ozone therapy with other treatments were excluded unless injection therapy with another pharmaceutical agent (no placebo treatment) was part of one of the treatment arms. Studies about injections in sacroiliac joints and studies evaluating the effects of epidural steroids for radicular pain were also excluded.
Injection therapy for subacute and chronic low back pain: an updated Cochrane review

• RESULTS: Eighteen trials (1179 participants) were included in this review. The injection sites varied from epidural sites and facet joints (i.e. intra-articular injections, peri-articular injections and nerve blocks) to local sites (i.e. tender-and trigger points). The drugs that were studied consisted of corticosteroids, local anesthetics, and a variety of other drugs. The methodologic quality of the trials was limited with 10 of 18 trials rated as having a high methodologic quality. Statistical pooling was not possible because of clinical heterogeneity in the trials. Overall, the results indicated that there is no strong evidence for or against the use of any type of injection therapy.
• CONCLUSION: There is insufficient evidence to support the use of injection therapy in subacute and chronic low-back pain. However, it cannot be ruled out that specific subgroups of patients may respond to a specific type of injection therapy.
S. Gautam, V. Rastogi, A. Jain, AP. Singh. Pain Pract. 2010 Jul 19. [Epub ahead of print]
• Visual analog scale (VAS) scores for pain and Oswestry disability index (ODI) were significantly decreased by both ozone and ozone-PIRFT when compared with the baseline values
• Ozone-PIRFT produced a significant reduction in the VAS scores and ODI when compared to ozone at 2 weeks, 1 month, 3 months, 6 months, and 1 year follow-up. Ozone-PIRFT also resulted in a significant change in pain relief, reduction of analgesic consumption, and patient's satisfaction at all points of follow-up, as compared with the ozone group.
• Ozone-PIRFT is more efficacious than ozone alone in reducing pain scores, analgesic consumption, improving functional outcome, and satisfaction of patients with contained lumbar disc herniation
Comparative Evaluation of Oxygen-Ozone Therapy and Combined Use of Oxygen-Ozone Therapy with Percutaneous Intradiscal Radiofrequency Thermocoagulation (PIRFT) for the Treatment of Lumbar Disc Herniation

J. Steppan, T. Meaders, M. Muto, K.J. Murphy. J Vasc Interv Radiol. 2010 Apr;21(4):534-48. Epub 2010 Feb 25.
• Metaanalyses were performed on the oxygen/ozone treatment results for almost 8,000 patients from multiple centers. The mean improvement was 3.9 for Visual Analog Scale and 25.7 for Oswestry disability index. The likelihood of showing improvement on the modified MacNab scale was 79.7%. The means for the VAS and ODI outcomes are well above the minimum clinically important difference and the minimum (significant) detectable change. The likelihood of complications was 0.064%.
• Oxygen/ozone treatment of herniated discs is an effective and extremely safe procedure. The estimated improvement in pain and function is impressive ranging in age from 13 to 94 years with all types of disc herniations. Pain and function outcomes are similar to the outcomes for lumbar discs treated with surgical discectomy, but the complication rate is much lower (<0.1%) and the recovery time is significantly shorter.
A metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs.

V. Bocci., E. Borrelli, V. Travagli. I Zanardi. Med Res Rev. 2009 Jul;29(4):646-82.
• After five decades characterized by empiricism and several pitfalls, some of the basic mechanisms of action of ozone in pulmonary toxicology and in medicine have been clarified. The present knowledge allows to understand the prolonged inhalation of ozone can be very deleterious first for the lungs and successively for the whole organism. On the other hand, a small ozone dose well calibrated against the potent antioxidant capacity of blood can trigger several useful biochemical mechanisms and reactivate the antioxidant system. In detail, firstly ex vivo and second during the infusion of ozonated blood into the donor, the ozone therapy approach involves blood cells and the endothelium, which by transferring the ozone messengers to billions of cells will generate a therapeutic effect. Thus, in spite of a common prejudice, single ozone doses can be therapeutically used in selected human diseases without any toxicity or side effects. Moreover, the versatility and amplitude of beneficial effect of ozone applications have become evident in orthopedics, cutaneous, and mucosal infections as well as in dentistry.
The ozone paradox: ozone is a strong oxidant as well as a medical drug

B. Cassileth. Oncology (Williston Park). 2009 Nov 30;23(13):1182.
• Oxygen therapies are unproven alternatives promoted as a cure for cancer, acquired immune deficiency syndrome (AIDS), and other degenerative diseases. Proponents claim that many diseases, including cancer, are caused by oxygen deficiency and that oxygenation can restore health by destroying cancer cells, eliminating pathogens, stimulating metabolism, and by producing "oxidative detoxification." There is no scientific evidence to support any of these claims. Oxygen therapies include: (1) hydrogen peroxide therapy involving intravenous infusion, ingestion, colonic administration, or soaking in hydrogen peroxide solution; (2) ozone colonies and ozone autohemotherapy, in which blood is withdrawn and treated with ozone before reinfusion, and (3) "oxygenated" water, pills, and solutions. The use of oxygen therapies has resulted in serious adverse events and several deaths. Oxygen therapies should not be confused with those commonly used in respiratory care.
Oxygen therapies

• TGF-B activates cartilage cells to produce matrix proteins, and improves matrix protein arrangement, modulates surface integrity, modulates the ratio between protease and protease inhibitors.
• Rising ozone in the blood promotes an increase in serum TGF-B
• TGF-B is released from macrophages and platelets under ozone influence, and from cartilage cells
• Intrarticular ozone may promote antiinflammation through TGF-B induction, SOD induction and cytokine induction
• Check out research on TGF-B: if we can use it and its affordable say goodbye to PRP (Expensive) and maybe even prolozone (dirt cheap).
Prolozone

• Release of Il-10 and TGF-B1 is able to suppress excess immunostimulation, thus resulting in an orderly programming of immune response
• The rise increases at the lower concentrations reaching optimum( IFN-g) at 40-60 ug), and inverses at the higher concentrations.
Prolozone

• Il-6 accelerated antibody synthesis and acute phase proteins GM-CSF factor produces leukocytosis interferons, prevent viral replication and modulate the immune system with Il-2 and TNF-a
• Il-2 andTNF-a produce: an activation of: cytotoxic CD-8 cells, macrophages, neutrophiles, eosinophils, NK cells and activation of antibody-dependent cellular cytotoxicity (important for killing off neoplastic cells, infected cells, and microorganisms)
Prolozone

R. A. Hauser & M. A. Hauser. Journal of Prolotherapy. 2009;3:184
PRP involves the application of concentrated platelets, which release growth factors to stimulate recovery in non-healing injuries.
PRP causes a mass influx of growth factors, which exert their effects of fibroblasts causing proliferation and thereby accelerating the regeneration of injured tissues.
Specifically PRP enhances the fibroblastic events involved in tissue healing including chemotaxis, proliferation of cells, proteosynthesis, reparation, extracellular matrix deposition, and the remodeling of tissues.
Bottom line here is that PRP helps the healing process.
Platelet Rich Plasma (PRP) Injection Technique

Growth Factor Role
Transforming Growth Factor-betaTGF-β
Regulates balance between fibrosis and myocyte regeneration; Stimulates undifferentiated mesenchymal cell proliferation; Regulates collagen synthesis; Stimulates angiogenesis; Stimulates endothelial chemotaxis; Inhibitsmacrophage proliferation; Regulates mitogenic effects of other growth factor.
Platelet Derived Growth FactorPDGFa-b
Stimulates cell replication; Stimulates angiogenesis; Regulates collagen synthesis; Mitogenic for fibroblast/glial/smooth muscle cells; Mitogenetic for mesencymal cells and osteoblasts; Stimulates macrophage and neutrophil chemotaxis.
Vascular Endothelial Growth FactorVEGF
Stimulates angiogenesis; Increases vessel permeability; Mitogenetic for endothelial cells.
K. S. Tate & D. M. Crane. Platelet Rich Plasma Grafts In Musculoskeletal Medicine Journal of Prolotherapy. 2010;2(2):371-376.

Growth Factor Role
Basic Fibroblast Growth FactorbFGF
Stimulates angiogenesis; Stimulates proliferation of myoblasts; Mitogenic for mesenchymal cells, chondocytes and osteoblasts; Promotes growth/differentiation of chondrocytes and osteoblasts.
Epidermal Growth FactorEGF
Stimulates angiogenesis; Stimulates proliferation of myoblasts; Mitogenic for mesenchymal cells, chondocytesand osteoblasts; Promotes growth/differentiation of chondrocytes and osteoblasts.
Connective Tissue Growth FactorCTGF
Promotes angiogenesis and cartilage regeneration; Promotes fibrosis and platelet adhesion.
K. S. Tate & D. M. Crane. Platelet Rich Plasma Grafts In Musculoskeletal Medicine Journal of Prolotherapy. 2010;2(2):371-376.

PRP is done just like any other prolotherapy treatment except the solution used for injection is plasma enriched with growth factors from the patients own blood.
PRP has been used successfully to enhance surgical outcomes in maxillofacial, cosmetic, spine, orthopedic, and podiatric surgery.
In regard to its use today, you will see that the majority of doctors using it apply it onto their current knowledge-base of Prolotherapy. In other words, the doctors doing PRP are using it as a proliferant, much like they use other solutions in Prolotherapy.
In simple terms, PRP is a type of Prolotherapy!
R. A. Hauser & M. A. Hauser. Platlet Rich Plasma (PRP) Injection Technique . Journal of Prolotherapy. 2009;3:184

PRP injection has a potential risk of contamination. PRP with leukocytes may help to lower the risk however the patient is not fully protected.
“The AAOM did a PRP demo on a patient¹sshoulder at one of their meetings, and it caused infection that has resulted in several surgeries, and an ongoing big problem, including law suits.” As told to Dr. Michael A. Prytula
PRP and Risk of Infection

Infectious Agent Comments
Viral Arthritis
Hepatitis B
Rubella
Mumps
Ross River and other togaviruses
parvovirus
Occurs in prodromal period: due to circulating immune complexes
Especially in young women, often follows live virus vaccine
Unusual, mostly in men
Mosquito-transmitted infections in Australia (Ross River) and Africa
May follow adult infection
Reactive Arthritis
Campylobacter, Yersinia, salmonellae, shigellae, Chlamydia trachomatis (reiter’s syndrome*)
‘post-infectious’ arthritis, HLA B27-associated, no bacterial invasion of joint, immune mediated
Arthralgia and Arthritis In Infectious Diseases
*urethritis, arthritis, uvetis ± mucocutaneous lesions; complicates 1-2% of cases of chlamydial urethritis
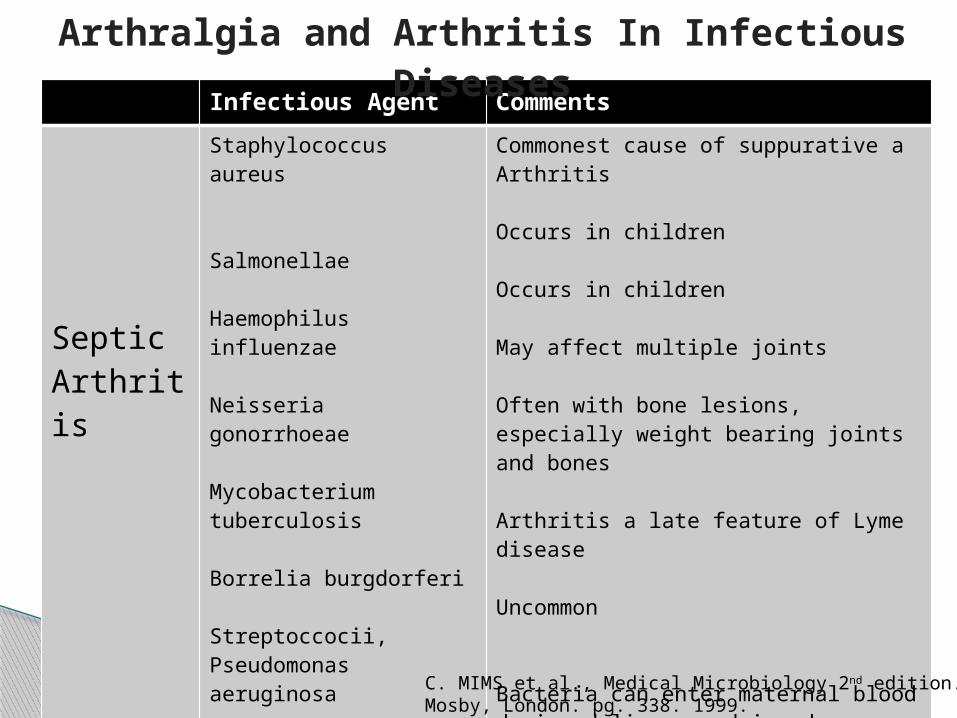
Infectious Agent Comments
SepticArthritis
Staphylococcus aureus
Salmonellae
Haemophilus influenzae
Neisseria gonorrhoeae
Mycobacterium tuberculosis
Borrelia burgdorferi
Streptoccocii, Pseudomonas aeruginosa
Mycoplasma hominis
Sporothrix schenckii
Commonest cause of suppurative aArthritis
Occurs in children
Occurs in children
May affect multiple joints
Often with bone lesions, especially weight bearing joints and bones
Arthritis a late feature of Lyme disease
Uncommon
Bacteria can enter maternal blood during delivery and invade joints; uncommon
Fungal infection of joints
Arthralgia and Arthritis In Infectious Diseases
C. MIMS et al., Medical Microbiology 2nd edition. Mosby, London. pg. 338. 1999.

R.I. Gracer & V. Bocci. Medical hypotheses. 2005;65,(4), 752-759.
• Regenerative injection therapy (RIT), also known as proliferative therapy, has been used for over 30 years in the USA in patients with spinal and peripheral joint and ligamentous pathologies. It involves the injection of mildly irritating medications onto ligaments and tendons, most commonly at origins and insertions. These injections cause a mild inflammatory response which “turns on” the normal healing process and results in the regeneration of these structures. At the same time they strengthen and become less sensitive to pain through a combination of neurolysis of small nerve fibers (C-fibers) and increased stability of the underlying structures.
Can the combination of localized “proliferative therapy” with “minor ozonated autohemotherapy” restore the natural healing process?

• Oxygen/ozone therapy is a well established complementary therapy practiced in many European countries. The ozone dissolves in body fluids and immediately reacts with biomolecules generating messengers responsible for biological and therapeutic activities. This results in an anti inflammatory response, which also results in a similar trophic reaction to that of RIT. It is logical to expect that combining these two modalities would result in enhanced healing and therefore improved clinical outcomes. Oxygen/ozone therapy, accomplished by autohemotherapy (AHT), is performed by either administering ozonated blood intravenously (Major AHT) or via intramuscular route (Minor AHT). These procedures result in stimulation of the immune and healing systems. Our concept is that the local injection of this activated blood injected directly to the ligamentous areas that are also being treated with RIT will act as a direct stimulation to the healing process. In addition, combining this with intravenous major AHT should stimulate the immune system to augment and support this process. RIT and oxygen/ozone therapy have been extensively studied separately. We propose a study of lumbosacral ligamentous pain to explore this therapeutic combination. We hope that this paper will stimulate general interest in this area of medicine and result in investigation of the “interface” between these treatment modalities.
RIT and ozone treatment can enhance the cellular anabolic activity and defense mechanisms, thus decreasing chronic inflammation and risk of infection
Prolozone

IV Ozone, Hydrogen Peroxide & UVBI Course: November 27, 28, 2010
It will be held in the meeting room at: Country Inn & Suites By Carlson Calgary Airport, 2481 39th Avenue N.E., Calgary AB T2E 8V8, Canada, Reservations: 1-800-596-2375, US/Canada Toll-free Telephone: (403) 250 – 1800. Room reservations for standard room $139 suite $154 this may go up as we get closer to the date. http://www.countryinns.com/calgaryab
Cost $750 plus GST, I need at least 12 people registered and paid by Nov 12 to hold this course.
For more information on upcoming courses please refer to www.naturomedic.org
Ozone Training and Certification

A. Seda Artis, S. Aydogan & M. Gokhan Sahin. The effects of colorectally insufflated oxygen-ozone on red blood cell rheology in rabbits. Clin Hemorheol Microcirc. 2010;45(2-4):329-36.
B. Cassileth. Oxygen therapies. Oncology (Williston Park). 2009 Nov 30;23(13):1182B. Baibor et al, Investigating antibody-catalyzed ozone generation by human
neutrophils. PNAS March 18, 2003 vol. 100 no. 6 3031-3034 B. Ning et al., Degradation of Endocrine Disrupting Chemicals by Ozone/AOPs. Ozone:
Science & Engineering, Volume 29, Issue 3 May 2007 , pages 153 - 176B. Uysal, M. Yasar, N. Ersoz, O. Coskun, A. Kilic et al. Efficacy of hyperbaric oxygen
therapy and medical ozone therapy in experimental acute necrotizing pancreatitis. Pancreas. 2010 Jan;39(1):9-15.
C.F. Andreula et al., Minimally invasive oxygen-ozone therapy for lumbar disk herniation. AJNR Am J Neuroradiol. 2003 May;24(5):996-1000
C. MIMS et al., Medical Microbiology 2nd edition. Mosby, London. pg. 338. 1999.D. Guanche, Z. Zamora, F. Hernádez, K. Mena, Y. Alonso et al. Effect of ozone/oxygen
mixture on systemic oxidative stress and organic damage. Toxicol Mech Methods. 2010 Jan;20(1):25-30.
E.T. Creagan et al., Failure of high-dose vitamin C (ascorbic acid) therapy to benefitpatients with advanced cancer. A controlled trial. N Med 687 90. High vitamin C Engl J Med. 1979 Sep 27;301(13):687-90.
References
E.V. Sin’kov. Treatment of patients with acute and chronic suppurative middle ear diseases using ozone preparationsVestn Otorinolaringol. 2009;(3):34-5.
G. Das, S. Ray, S. Ishwarari, M. Roy, P. Ghosh. Ozone nucleolysis for management of pain and disability in prolapsed lumber intervertebral disc. A prospective cohort study. Interv Neuroradiol. 2009 Sep;15(3):330-4. Epub 2009 Nov 4.
J.B. Staal, R.A. de Bie, H.C. de Vet, J. Hildebrandt, P. Nelemans. Injection therapy for subacute and chronic low back pain: an updated Cochrane reviewSpine (Phila Pa 1976). 2009 Jan 1;34(1):49-59.
J. Steppan, T. Meaders, M. Muto, K.J. Murphy. A metaanalysis of the effectiveness and safety of ozone treatments for herniated lumbar discs. J Vasc Interv Radiol. 2010 Apr;21(4):534-48. Epub 2010 Feb 25.
K. S. Tate & D. M. Crane. Platelet Rich Plasma Grafts In Musculoskeletal Medicine Journal of Prolotherapy. 2010;2(2):371-376.
M.D'Erme et al. Ozone therapy in lumbar sciatic pain. Radiol Med. 1998 Jan-Feb;95(1-2):21-4.
M. Levine et al, A new recommended dietary allowance of vitamin C for healthy young women. Proc Natl Acad Sci U S A. 2001 August 14; 98(17): 9842–9846, 1996, 2001.
M. Muto, C. Andreula, M. Leonardi. Treatment of herniated lumbar disc by intradiscal and intraforaminal oxygen-ozone (O2-O3) injection J Neuroradiol. 2004 Jun;31(3):183-9
References

O.A. Bitkina, T.V. Kopytova, K.N. Kontorshchikova, A.P. Bavrina. Oxidative stress level in patients with rosacea and a rationale for the therapeutic use of an ozone-oxygen mixtureKlin Lab Diagn. 2010 Apr;(4):13-6.
Q. Chen et al, Pharmacologic ascorbic acid concentrations selectively kill cancer cells: Action as a pro-drugto deliver hydrogen peroxide to tissues. PNAS September 20, 2005 vol. 102 no. 38 13604-13609
Q. Chen et al, Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo. PNAS May 22, 2007 vol. 104 no. 21 8749-8754
Q. Chen et al, Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. PNAS August 12, 2008 vol.105 no. 32 11105–11109.
R. A. Hauser & M. A. Hauser. Platlet Rich Plasma (PRP) Injection Technique . Journal of Prolotherapy. 2009;3:184
R.I. Gracer & V. Bocci. Can the combination of localized “proliferative therapy” with “minor ozonated autohemotherapy” restore the natural healing process? Medical hypotheses. 2005;65, (4), 752-759.
R. Venkatadri & R.W. Peters. Hazardous Waste and Hazardous Materials Chemical Oxidation Technologies: Ultraviolet Light/Hydrogen Peroxide, Fenton's Reagent, and Titanium Dioxide-Assisted Photocatalysis. Hazardous Waste and Hazardous Materials.
Spring1993, 10(2): 107-149.S. Gautam, V. Rastogi, A. Jain, AP. Singh. Comparative Evaluation of Oxygen-Ozone Therapy and
Combined Use of Oxygen-Ozone Therapy with Percutaneous Intradiscal Radiofrequency Thermocoagulation for the Treatment of Lumbar Disc Herniation. Pain Pract. 2010 Jul 19. [Epub ahead of print]
References

S. Menndeza et al, Ozone Therapy in Cancer Treatment: State of the Art. Ozone: Science & Engineering, Volume 30, Issue 6 November 2008 , pages 398 – 404
S.J. Padayatty et al, Intravenously administered vitamin C as cancer therapy: three cases. CMAJ • March 28, 2006; 174 (7).
V.A. Neronov. Experience with the use of ozone for the treatment of chronic viral hepatitis. Vopr Kurortol Fizioter Lech Fiz Kult. 2009 Nov-Dec;(6):14-7.
V. Bocci., E. Borrelli, V. Travagli. I Zanardi. The ozone paradox: ozone is a strong oxidant as well as a medical drug. Med Res Rev. 2009 Jul;29(4):646-82.
V. Bocci, N. Di Paolo. Oxygen-ozone therapy in medicine: an update. Blood Purif. 2009;28(4):373-6. Epub2009 Sep 10
V. Bocci, V. Travagli, I. Zanardi. May oxygen-ozone therapy improves cardiovascular disorders?. Cardiovasc Hematol Disord Drug Targets. 2009 Jun;9(2):78-85.
V.M. Kopchak, I.V. Khomiak, A.V. Duvalko, A.A. Stasenko, V.A. Dieiev. Application of ozone therapy in complex treatment of patients with acute necrotizing pancreatitis. Klin Khir. 2008 Oct;(10):28-31.
References