Embed Size (px)
Citation preview

DYSPNEA In Advanced Lung Cancer Patients
By: Cindy Stegman RN BSNAlverno College MSN 621
Spring [email protected]

How to navigate this tutorial:To advance to next slide click on box
To advance to previous slide click on box
To return to MAIN MENU click on box
If you see the return button click on it to return to
QUESTION slide.
Hover over the underlined text for an explanation/definition

To educate RNs and LPNs on the pathophysiology of advanced lung cancer
associated with dyspnea
At the end of the tutorial the learner will be able to:
• Identify pathophysiology of advanced lung cancer associated with dyspnea • Discuss key assessment components of the advanced lung cancer patients experiencing dyspnea
• Describe evidence-based interventions for the advanced lung cancer patients experiencing dyspnea
PURPOSE & OUTCOMES

Clip art, 2010
Pathophysiology of advanced lung cancer
Anatomy of normal lung function
Causes of dyspnea
Mechanisms of dyspneaGenetic relationship
Evidence-Based Nursing Interventions
Stress & Immune/Inflammatory response
Nursing assessment
Case Study Nursing-Sensitive Outcomes
Content of TutorialAt any time during tutorial you may click to come to this screen and select next topic.
Let’s get started… taking a DEEP breath and relax!

Anatomy ofNormal Lung Function
Click each circle in the diagram to recognize the
anatomy of the lungs 1
2
3
5
4
Trachea: Is the tube that runs from your larynx to just above
your lungs. The trachea divides into TWO large
branches called the bronchi.Bronchi: Entering the lung, the bronchi divide into the left and right side of lung. They continue to branch & divide
into smaller bronchi. Bronchioles: Smallest
conducting airways at the terminal end of the bronchi.
At the most distal end gas exchange takes place.
Pleura: A thin serous membrane that lines the
thoracic cavity & cushions the lungs.
Alveolar sacs: Cup-shaped structures which are the
smallest functional unit of the lungs.Porth, 2005

Physiology of Normal Breathing:-Automatic, quiet
- Movement that control ventilation are integrated by neurons located in:
- Medulla & Pons (Respiratory Center)
GOAL of Breathing: Oxygenation of the blood and removal of Carbon dioxide.
Scroll across each picture
Porth, 2005)

What Stimulates your respiratory
system to increase breathing?
ReceptorsClick on star to
receive answer

1)Chemoreceptors - Peripheral chemoreceptors: Located in the
carotid and aortic bodies
- Central chemoreceptors: Located in the Respiratory center in the Medulla & pons
2) Lung & Chest wall Receptors
- Stretch (smooth muscle)
- Irritant (Airway of epithelial cells)
- Juxtacapillary or J receptors (alveolar wall)
Jantarakupt, P. & Porock, D. (2005).

A nurse walks into a room and observes a patient breathing rapid and shallow. Respiratory rateis 32 breaths/min and pulse ox at 80% on room
air. What receptors alerted the respiratory center to turn ON ?
Incorrect.These receptors are located in the medulla & pons and stimulate the resp. center when there are high levels
of carbon dioxide in the blood.
Central Chemoreceptors
Incorrect.These receptors are
located in smooth muscle and do not stimulate the respiratory center when there is LOW oxygen in
the blood.
IncorrectIn this situation because
this scenario did not mention crackles in the
lungs that would suggest pulmonary edema.
Correct!!These receptors alert the respiratory center when there is LOW oxygen in
the blood
J Receptors
Stretch Receptors
Peripheral Chemoreceptors

What Causes Lung Cancer?Repeated
EXPOSURE to
Carcinogens
Transforms: Normal cell into
Malignant
Clip Art, 2010Hoffman, A. & Gift, A. (2007)
Cells in the respiratory membrane that line the
bronchi become THICK &HARDEN
Cilia become
Stiff (Unable to sweep debris away)
Genetic Damage

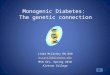
Lung Cancer Cell Dividing
- Lung cancer cells are highly invasive & may extend into the mediastinum or pleural cavity- Lung network is highly vascular and metastasis occurs early- Distant metastasis may occur in the brain, liver, bones, or kidneys Hoffman, A., & Gift, A. (2007)
Permission from http://images.wellcome.ac.uk/

What we know increases risk for
development of Lung Cancer• Active tobacco exposure
• Passive smoke exposure (Second hand)• Shared environment
• Asbestos (school, home, work, person-person)
• Environmental exposure (Radon & heavy metals)• Nickel, arsenic
National Cancer Institute, 2010
Clip Art, 2010
Clip Art, 2007
Clip Art, 2007
Clip Art, 2007

Research in the works…Study produced by:
• National Cancer Institute• National Human Genome Research Institute• National Institutes of health
Study that was printed in 2004 in the American Journal of Human Genetics
Study involved: -52 families with a minimum of Three 1st-degree family members affected by either lung, throat, or laryngeal cancer
-Used 392 known genetic markers & compared the alleles of each affected and non-affected family member
National Cancer Institute, 2010

Research in the works Cont…Discovered:
A region on Chromosome 6 (susceptibility to Lung caner)
WORK is needed to:Look closer in this
REGION to find the exact GENE that causesthis susceptibility National Cancer Institute, 2010
Clip Art, 2010

Mechanisms of Dyspnea
•Divided into 3 pathologies:
• Chemical Stimulation
• Neural Stimulation
• Emotional Stimulation Clip Art, 2007

Chemical Stimulation
Central respiratory
chemoreceptor
s
Peripheral respiratory
chemoreceptors
PaCO2
PaO2
Eliminate Carbon Dioxide
American Thoracic Society. (1998).
Clip Art, 2007
Clip Art, 2007
Jantarakupt, P. & Porock, D. (2005)

Neural StimulationNeural Pathways for breathing receive signals from receptors in:
- Lungs- Skin- Muscles- Joints
These receptors are called “Mechanoreceptors”
- Stretch receptors in (trachea, bronchi) are stimulated with lung expansion
- Irritant receptors (epithelium of airways) stimulated by smoke, pollens, fungi, cold air, & mold
- Movement of lower and upper extremities stimulate receptors in muscles & joints
- Painful stimuli will elicit mechanoreceptors within the skinJantarakupt, P. & Porock, D. (2005)
Once mechanoreceptors are stimulated they
will cause an individual to
breathe faster

Emotional Stimulation• Emotional distress
• Anxiety• Anger• Depression
THE CAUSE & EFFECT relationship is unclear but…
Emotional changes CAN stimulate the respiratory center, which in turn AFFECTS the
Individual’s breathing pattern
Clip art, 2007
Jantarakupt, P. & Porock, D. (2005).

Dyspnea is a distressing and debilitating symptom that
cancer patients may experience.
- It is SUBJECTIVE (what the patient says)- An uncomfortable, frightening experience
(
Clip art, 2007Dyspnea is estimated to occur in 15-55% at the time of diagnosis
and up to 18-79% during the last week of life
Oncology Nursing Society. (2010).

Stress and Dyspnea: What’s the CONNECTION?
Stress response or General Adaptation Syndrome (GAS)
is meant to protect an individual
during ACUTE episodes stress. If the GAS is
continually stimulated by chronic stressors,
this can be a threat to an individual’s homeostasis.
Porth, C., (2005)
Clip Art, 2010

Stress and DYSPNEA Cont…
Dyspnea: Acute or Chronic
Advanced Lung CancerPATIENT
Physical & Psychological Stress
ALERT: STRESS
RESPONSE

Stress and Dyspnea Cont…Results: In release of catecholamines (such as epinephrine and norepinephrine) and cortisol, which:
- Increases heart rate- Dilates the bronchioles
Stress causes Vasoconstriction to…
- Skin: which becomes Pallor and cold- GI tract: which causes nausea, No bowel sounds, & digestion stops- Kidneys: which decreases urinary output
Porth, C., (2005))
Inflammatory and Immune response stops!

PhysicalBehavior
al
ADAPT to
ACUTE STRESS
WHAT factors AFFECT our ability to ADAPT
to STRESS??
Endocrine-Neurotransmitter pathway… PRODUCE
CHANGES

Click on each circle
Severe emotional distress often
disrupts physiological
function and limits an individuals ability to make
appropriate choices related to adaptive needs. If a dyspnea
is present, this is causing emotional
distress and affecting their ability to enjoy
daily activities due to the stress of not
being able to breathe.
Sleep-Wake Cycles
Hardiness
Mental Health Status
NutritionSleep is the
most restorative function in
which tissues are
regenerated. If an
individual cannot sleep at night, due to dyspnea,
this is affecting
their ability to restore
their energy.
Malnutrition is one of the most
common causes of immunodeficiency.
Most advanced lung cancer
patients have major issues with nutrition due to
loss of appetite & weight loss from treatment &/or disease process
itself.
A personality characteristic
which includes: A sense of
purpose in life and to view
stressors as a challenge rather than a threat. If
dyspnea is affecting their hardiness, the individual will
see this stressor as a threat and slowly become susceptible to
sadness.
Porth, C. (2005)

What happens if DYSPNEA continues to stimulate
our Stress Response??

Exhaustion OCCURS!Coping mechanisms
are depleted.
WEAR & TEAR on the System
Chronic stress will occur & LEAD to:
Loss of AppetiteSleep disturbance
Depression
What does this mean for an advanced lung cancer patient if this
cycle continues ?Porth, C., 2005
Clip Art, 2007

Immune & Inflammatory responses diminish
which means:
The advanced lung cancer patient is at an increased risk for infections
The AGING advancedlung cancer patient hasless ability to adapt to
environmental stressors
Decreases their immune
responsiveness &
abilityto heal wounds
Porth, C., 2005
Clip Art, 2007

Aging can be viewed as a low-grade chronic inflammatory state which is termed as “
inflammaging”
Porth, C. 2005 & Franceschi, C. & Bonafe, M. 2003
If the GAS is constantly stimulated, what does this mean for the
aged advanced lung cancer patient?
Due to the thymus decreasing in size as we age , this affects
T-Cell function within the body.
Ultimately, compromises the immune system
responsiveness to heal wounds.
Due to inflammaging, this can cause
chronic activation of inflammatory responses.
Eventually, leads to the infiltration of
macrophages, lymphocytes, &
fibroblasts, which causes persistent swelling and scar
formation to occur.
Click on ARROW twice

Cancer-Related Causes of DYSPNEA:
1)Direct cause of the cancer
2)Indirect result of the cancer
3)Result of cancer treatment
4) Other

DIRECT -Primary or metastatic cancer to lung
- Pleural tumor
- Pericardial effusion
- Ascites
Permission from http://images.wellcome.ac.uk/
Tyson, L. (2006)
INDIRECT-Anemia
-Pneumonia
- Pulmonary emboli
- Cachexia

Dyspnea from Treatment 1) Surgery
2) Radiation (which can cause)- - Pulmonary Pneumonitis - - Pulmonary fibrosis
Polovich, M., Whitford, J., & Olsen, M. (2009).
Clip Art, 2007
3) Chemotherapy agents that can either cause:
- Pulmonary EdemaCytoxan, Gemzar, Methotrexate, Mitomycin
- Pulmonary Pneumonitis/FibrosisCytoxan (later development), Gemzar (later sign of fibrosis), Bleomycin (Pneumonitis), Methotrexate, Carmustine

- Obesity- Age - Asthma- CHF or COPD
Co-Morbidities that cause
Dysnpea
Clip art, 2007
Other: - Anxiety
DiSalvo, W., at el., (2008)

Oncology Nursing Society (ONS)
In 2003, ONS developed their own definition of oncology nursing-sensitive
patient outcomes(NSPO’s), which focused around:
Oncology Nursing Society, 2003
-Patient’s problems are significantly affected by nursing interventions.
-Interventions developed within the scope of nursing practice; are sensitive to nursing care and represent the consequences or effects of nursing interventions
-Result in changes in patients' symptom experience, functional status, safety, psychological distress, and/or cost

NSPO’s forDyspnea:
1)Symptom Management- Decrease in patient’s perception of breathlessness- Patient maintains activity level within capabilities- Respiratory rate remains at comfortable level- Patient is able to manage episodes of dyspnea
2) Psychosocial Distress- Promoting relaxation and stress reduction- Education and support to patients and their families
Crowley. (2005) & ONS PEP, (2008)

ASSESSMENT
1)SUBJECTIVE (Pt’s own description, feeling, of breathlessness)
- At rest- With activity- Assess dyspnea with a Visual Analog scale
- Number Scale (1-10)- Mild-Moderate-Severe
2) VITAL SIGNS- Respiratory rate (Rate, Irregular, Depth)- Weight
Clip Art, 2007
Clip Art, 2007

Assessment Cont…3) CARDIOPULMONARY:
- Accessory Muscle use- Edema - Tachycardia
- Underlying cause (fever, etc.)
- Auscultation -Wheezes, crackles, cough
- Secretions (amount, consistency)
4) INTEGUMENTARY:- Pallor (Anemia)
- Cyanosis (Low oxygen, hypoxia) Itano, J. & Taoka, K. (2005)
Clip Art, 2007

Assessment Cont…5) MENTAL STATUS
- Restlessness- Confusion- Memory Difficulties
6) PSYCHOSOCIAL Distress:- Depression- Anxiety- Fear
Clip art, 2007

G. S. is a 65 year-old man diagnosed with Stage IV Lung cancer in October 2009
- His presenting symptom at the time of diagnosis is rib pain.- During the next few weeks, G.S has received several radiation treatments to his ribs.- After his radiation treatment, G.S has also received system chemotherapy.
(Up to this point, G.S. has tolerated this treatment fairly well)
December of 2009 (post radiation/chemotherapy tx) G.S had a PET scan that showing worsening enlargement of primary tumor.
January 2010 G.S. was switched to salvage Taxotere chemotherapy regimen
Over the next few weeks to months G.S. is seen in the clinic with increased weakness, hypotension, nausea, and dehydration.
Continued

Today March 2010, G.S is seen in the clinic:
- G.S. is looking frail & ashen in color- Knees down bilateral has +3 pitting edema- Oxygen saturation measuring at 87% on room air- No appetite- Lost of five pounds since February - Denies any pain- C/o of shortness of breath with activity- Uses a walker to assist with ambulation- C/O of insomnia, due to trouble breathing at night- On auscultation: fine wheezes heard throughout bases of lungs
HOME MEDICATION:
- MS Contin 30 mg BID- Fluconazole 200 mg- Ativan 0.5-1 mg every 8 hrs PRN- Oxycodone 5 mg (1-3) every 2 hrs PRN

These are all possible Nursing Interventions to help relieve G.S’s DYSPNEA.
Click on all the buttons at the bottom to understand WHY?A) Suggest to G.S to get a prescription of Morphine Sulfate in an immediate release
capsules to help relieve his dyspnea
B) On assessment, heard audible wheezes in upper lung fields. Suggest an albuterol inhaler treatment
C) Suggest to G.S to take his Ativan before strenuous activities & before sleep to help relieve his anxiety
D) G.S. oxygen saturation on room air was 87%. Supplement oxygen to help relieve his dyspnea.
E) Due to the edema (swelling) in his legs, ask his physician for an order of lasix
F) Suggest to his wife to place a fan on G.S’s face and nose, as this might help relieve his dyspnea or use breathing techniques to slow down his breathing during periods of dyspnea.
G) Educate G.S on relaxation techniques & encourage G.S to sleep in his recliner to keep upper body at least at 45-90 degree angel to help with sleep.
A B C D E F G

Opioids on Cancer-RelatedDyspnea
• Immediate-release oral agents
• Parenteral
RECOMMENDED for Practice:
• Morphine (most common)• Hydromorphone (Dilaudid)
WHEN OXYGEN OR REST DO NOTRELIEVE DYSPNEA
NCCN, 2010, DiSalvo, W., Joyce, M., Tyson, L., Culkin, A., & Mackay, K., 2008, & Oncology Nursing Society, 2008.

Theory of OPIATES
Act at central/periphe
ral opioid receptors sites
& central nervous
system (Respiratory
center)
Respiratory
drive at rest and activity
Block respiratory responses to hypoxia
& hypercapni
a
Wickham, R. (2002) & Gift, A. & Hoffman, A. (2007)
MORPHINE
Opioids have a depressant effect on the central nervous system, which alleviate dyspnea by blocking the neural signals to hypoxia &
hypercapnia.

Recommendations:Treating COUGH/DYSPNEA/ or AIR HUNGER
- 2-10 mg Morphine orally every 4 hr prn- 1-4 mg Morphine IV every 4 hr prn
1) RE-ASSESS patient
2) SIDE EFFECTS: dysphoria, dizziness, drowsiness, urinary retention, constipation.
Re-assure patient: Opiates will help them rest without the feeling of “suffocation”
REMEMBER!!
Naïve Vs
Tolerant
LOWER dose of
Morphine used to treat
Dyspnea, BUT
Action of Morphine
for dyspnea is shorter
than its analgesic effects!
Jantarakupt, P. & Porock, D. (2005), NCCN, 2010, & Wickham, R. (2002).
NCCN, 2010

Patient/Family MYTHS & FEARS about OPIOIDs
1)ADDICTION- Reassure patient they are taking opioids to relieve their
cancer-related dyspnea. Dyspnea can change from day to daydepending on the progression of their disease state. As nurse providers, reassure patient that the dosage may increase in the future due to repeated administration of that opioid dose. The body will eventually build up a tolerance for that dose of opioids and the individual will not be receiving the desired effect.
2) Over SEDATION- Reassure patient we will be monitoring them while receiving opioids- This is for palliative treatment of dyspnea, so titrating the opioid dosage may be necessary to get the desired effect.- As the individual transitions from palliative care to hospice…
Retain increased amounts of carbon dioxide
Causes
Sleep & a comatose state to
occur with the dying patient regardless if opioids are
administered or not
DYING patient’s
breathing is now more rapid & shallow
Wickham, R. (2002) & Johnston, M. (2007).
Clip Art, 2010

QUIZ1)Are extended-release opioids just as
effective as immediate-release?CORRECT!
Immediate-release opioids have been shown to be
effective in practice when treating dyspnea.
Sorry Extended-Release opioids
have NOT been established to show
effectiveness towards treating dyspnea
FALSETRUE
In the case of G.S, immediate-release opioids are an appropriate intervention, because he has already has been exposed to opioids. REMEMBER… he is opioid
tolerant, so G.S. might need to repeat the dose more frequently to treat the DYSPNEA. As nurse providers, we need to console & support G.S. if he has any
fears of using opiods, because sedation & addiction can be a fear patients have with opioid usage. KEEP the patient’s GOAL in mind & reassure G.S. that this intervention
will be able to get him through tough periods of dyspnea to be able to endure certain activities.

Bronchodilators•Inhaled or Nebulized
-B2 –adrengergic agonist
• Albuterol
decreases
WORKLOAD of the lungs
Nebulized Opioids??Believed to “TARGET” stretch and
irritant receptors in
the lungs
SYSTEMIC TOXICITY
Jantarakupt, P. & Porock, D. (2005) & Kallet, R., (2007)
NOT Recommend for Practice
Due to:Insufficient Evidence
Bronchodilators relaxes smooth muscles within
the bronchioles

CORRECT On assessment you heard wheezing throughout lung
fields to suggest vasoconstriction within
bronchioles. An albuterol treatment would be an
appropriate intervention for G.S’s dyspnea.
Sorry Short-Acting bronchodilators are more effective for patient’s who have either air flow obstruction
such as COPD, asthma, or patient’s with lung cancer & is
presenting with wheezing throughout lung fields to suggest
vasoconstriction.
Quiz1) Which option is correct to suggest an albuterol
inhaler to treat G.S’s dyspnea?
G.S complained of shortness of breath
while walking to the bathroom?
On auscultation, you heard wheezes throughout G.S.’s
lung fields
Wickham, R. 2005

Benzodiazepines•Lorazepam
• Diazepam
Recommended Dosages: Ativan: 0.5-1 mg orally or IV q 4 hrs prn
Diazepam: 2 mg po/SQ/IV q 12 hours (NCCN, 2010)
Sedative action ANXIETY that stimulates dyspnea!!
DO NOT WORK
DIRECTLY ON THE LUNGS
Jantarakupt, P., & Porock, D., (2005) & NCCN, (2010). & Wickham, R., (2002)

Sorry Benzodiazepines do not directly
work on the lungs to relieve dyspnea. Benzodiazepines are used for their
sedative use to decrease anxiety that is commonly associated with
dyspnea.
QuizTrue or False:
Do benzodiazepines work directly on the lungs to relieve Dyspnea?
TRUE
YES Benzodiazepines
treat anxiety associated with dyspnea and do
not directly treat dyspnea. In G.S’s case, this can help his anxiety & let him be able to
sleep at night with out the fear of
suffocation.
FALSE

OXYGEN- Increase oxygen saturation (SaO2)
- Hypoxia is present
DYSPNEA• Lowers respiratory RATE• Lowers respiratory EFFORT
Non-hypoxic Patients?
FEAR and AnxietyJantaarakupt, P. & Porock, D. (2005)
Patient’s with advanced lung cancer have less ability to remove carbon dioxide or
transport oxygen to other parts of the body due to the physical changes cancer makes
within lung tissue. Patient’s with a history of COPD will be at higher risk of retaining
CO2.
CAUTION!! CO2 Retainers
Click on box
Clip Art, 2007

QuizTrue or False
Oxygen therapy is ONLY for patient’s who are truly hypoxic?
IncorrectOxygen therapy is primarily used for
hypoxic patients, but in cases of advanced lung cancer patient’s who are experiencing dyspnea, oxygen has been proven to help relieve the feeling of shortness of breath.
True
Correct Oxygen therapy can be used for hypoxic & non-hypoxic advanced lung
cancer patient’s experiencing dyspnea. CAUTION should be used when titrating
oxygen if patient is a CO2 retainer. In the case of G.S. he is truly hypoxic
when his oxygen saturation was at 87% on room air. Oxygen therapy would be an appropriate intervention to treat his
dyspnea.
False

OTHER Treatments:Steroids & NSAIDS
Side effects of steroids: Gastric toxicity, fluid retention, hyperglycemiaLasixGiven when a patient is experiencing:
1) Pulmonary congestion2) Lower extremity edema
INFLAMMATION in the LUNGS to
relieve dyspnea
Gift A. & Hoffman, A. (2007).
More effective for patient’s with pre-existing conditions such as COPD
LASIX is given for fluid overload to
Decrease the demand on the
heartJantarakupt, P. & Porock, D., 2005 & Wickham, R. 2005

What is the relationship betweenG.S’s lower extremity edema and
him experiencing DYSPNEA?
In G.S.’s situation, there could be multiple factors causing his lower leg edema, such as malnutrition, medications, and/or worsening of his lung cancer involvement . The edema
is causing his heart to pump harder to compensate for the extra fluid, which is
causing G.S. to have dyspnea at rest &/or with activities. Lasix would be an appropriate short term fix to help with the edema in lower
extremities & relieve dyspnea.
CLICK ON
Hoffman, A. & Gift, A. (2007)

1)Breathing Techniques - Pursed-lip and diaphragmatic breathing
(Shown to optimize lung function, decrease stress, & relaxthe breathing for that patient)
2) Increase airflow (generated by a FAN)
- Face- Nose
(Gives the perception of more airflow to the individual, which may reduce the feeling of dyspnea)
3) Providing COOLER temperatures- Decrease the feeling of dyspneaDiSalvo, W., Joyce, M., & Belansky, H. (2009)
Clip Art, 2007
Clip Art, 2007

4) Positioning
- Sitting up (expansion of lungs)
5) Promoting Relaxation Stress Reduction
- Massage- Reducing external noise
(Decrease anxiety & stress associated with dyspnea)
6) Emotional & Psychosocial Support
(Coaching and support have been shown to decrease the feeling and anxiety associated with
dyspnea)
Clip Art, 2007
Andry, J. (2008) & Tyson, L (2006)

Key Points to REMEMBER:
-Dyspnea is a SUBJECTIVE feeling & a debilitating symptom that patients experience.
- Key ASSESSMENT skills are crucial to help understand the underline cause of the dyspnea and/or the treatment options.
-Be consciously aware of evidence-based interventions that are already incorporated into nursing practice, whether the dyspnea is oncology related or not.
-Dyspnea is a symptom that can CHANGE from day to day. Reassure the patient of this and the multiple interventions we can help to relieve dyspnea.
-Lastly, keep the patient’s GOAL in mind. Are the interventions appropriate and will the patient be able to enjoy certain activities with some of the side effects that may occur. Just remember to communicate & educate patients on theseinterventions and just maybe, we can give them a little relief from their dyspnea!
KEY POINTS TO
REMEMBER

REFERENCES:
Guyton, A. & Hall, J. (2006). Blood Cells, Immunity, & Blood Clotting. Schmitt, W. & Gruliow, R. Medical Physiology (11th e.d.) pp. 439-450. PA: Elsevier Inc
DiSalvo, W., Joyce, M., Tyson, L., Culkin, A., & Mackay, K. (2008). Putting Evidence Into Practice: Evidence-Based Interventions for Cancer-Related Dyspnea. Clinical Journal of Oncology Nursing. 12(2) pp. 341-352.
Jantarakupt, P. & Porock, D. (2005). Dyspnea Management in Lung Cancer: Applying the Evidence From Chronic
Obstructive Pulmonary Disease. Oncology Nursing Forum. 32(4), pp. 785-795.
Johnston, M. P. (2007). Oncology Nursing. In Langhorne, M., Fulton, J., & Otto, S. Pain. (5th e.d. pp. 680-693). St. Louis: Elsevier Saunders.
Kallet, R. (2007). The Role of Inhaled Opioids and Furosemide for the Treatment of Dyspnea. Respiratory Care. 52(7): pp. 900-910.
Nation Cancer Institute, Retrieved on March 31, 2o10 from, http://www.cancer.gov/newscenter/pressreleases/lungcancerlocus National Comprehensive Cancer Network Practice Guidelines, Palliative Care, Version 1, 2010. Retrieved on April 22, 2010 from http://www.nccn.org
Oncology Nursing Society, 2003. Retrieved on March 31, 2010 from, http://www.ons.org/Research/NursingSensitive/
Oncology Nursing Society, 2008. Putting Evidence into Practice. Retrieved on April 2, 2010 from, http://www.ons.org/Research/PEP
Crowley, M. (2005). Core Curriculum for Oncology Nursing. In Itano, J. & Taoka, K (Eds.), Supportive Care: Dying and Death. (4th ed., pp. 102-126) St. Louis: Elsevier Saunders
About.Com. (2010). Smoking Cessation. Retrieved April 5, 2010 from, http://quitsmoking.about.com/cs/nicotinepatch/g/carcinogen.htm
American Cancer Society. (2007). Retrieved February 23, 2010 from, http://www.cancer.org/downloads/PRO/LungCancer.pdf
American Thoracic Society. (1998). Dysnpea: Mechanisms, Assessment, & Management. A Consensus Statement. American Journal of Respiratory and Critical Care Medicine. (159) pp 321-340.
Andry, J. (2008). Palliative Practices From A-Z for the Bedside Clinician. In Esper, P. & Kuebler, K. (Eds.). Dyspnea. (2nd ed., pp. 117-122). ONS Publishing Division, PA: Pittsburgh.
Hoffman, A. & Gift, A. (2007). Oncology Nursing. In Langhorne, M., Fulton, J., & Otto, S. Lung Cancer. (5th e.d., pp. 258- 274). St. Louis: Elsevier Saunders.
Franceschi, C. & Bonafe, M. (2003). Centenarians as a model for healthy aging. Biochemical Society Transactions. 31(2) pp: 457-461.

Polovich, M., Whitford, J., & Olsen, M. (2009). Chemotherapy and Biotherapy Guidelines and Recommendations for Practice. Oncology Nursing Society, pp. 234-244.
Stedman’s Medical Dictionary for the Health Professions and Nursing. (2005). (5th e.d.) Baltimore, MD: Lippincott Williams & Wilkins.
Tyson, L. (2006). Dyspnea. Clinical Manual for the Oncology Advanced Practice Nurse. Sorrell-Camp, D. & Hawkins, R. (23) pp. 153-158.
Wickham, R. (2002). Dyspnea: Recognizing and managing an invisible problem. Oncology Nursing Forum, 29, 925-933.
Zerwekh, J. & Claborn, J. (2006). Illustrated Study Guide for the NCLEX-RN Exam. Respiratory System, pp. 281-316. MO: Elsevier Mosby.