Embed Size (px)
Citation preview

By:
Case Report
General data
• P.P.
• 72 y/o
• Married
• Quezon City
• Roman Catholic

Chief Complaint
• Post-menopausal vaginal spotting x 4-5months

Past Medical History
• (+) Hypertension x 20 years, controlled– On Amlodipine 10 mg, 1 tab OD– Combizar, 5mg
• Dyslipidemia– Simvastatin, 40mg

Past Medical History
• s/p thyroidectomy (1977)
• s/p dilatation and curretage (1976)
Family History
• (-) hypertension, DM, asthma, thyroid disease, cancer

Menstrual History
• Menarche: at the age of 10
• Interval: regular, monthly
• Duration: 5 days
• Amount: 3-4 ppd, moderately soaked
• (-) dysmenorrhea
• LMP: 1995 (55 y/o), menopause x 15 years

OB History
• G0P0
• Married nulligravid

Gynecologic History
• Coitarche: at the age of 22
• # of sexual partner: 1
• (-) OCP or HRT use
• Last PAP Smear: (-)
• (-) vaginal discharge
• (+) vaginal spotting x 4-5 months

History of present illness
5 months PTA (+) vaginal spotting, 1-2ppd
(-) abdominal pain / mass
(-) bladder / bowel habit changes
(-) weight loss (+) Consult
USG: uterus slightly enlarged for age

History of present illness
3 mos. PTA (+) vaginal spotting, persistent
(-) abdominal mass
(-) bladder or bowel habit changes
(-) weight loss

History of present illness
1 mo. PTA (+) vaginal spotting, persistent
Consult SLMC Endometrial Biopsy
Secretory carcinoma, endometrium

Review of Systems
• General: no to minimal weight loss (-)loss of appetite and body weakness
• Skin: No rash and active skin lesions• Hair: No abnormal loss or growth• Nails: No color changes, brittleness and clubbing • Eye: No blurring of vision, redness, discharges • Ear: No pain and ear discharge• Nose: No discharge, obstruction and itching • Mouth: No bleeding gums and sores • Throat: No soreness and swollen tonsils• Neck: No mass and cervical lymphadenopathies

Review of Systems
• Pulmonary: No dyspnea, cough and shortness of`breath• Cardiac: No chest pains, palpitations, easy fatigability,
syncope• Gastrointestinal: No masses or tenderness• Genito-urinary: see HPI• Musculo-skeletal: No joint swelling and abnormal
posture• Hematopoietic: No pallor and easy bruisability• Neurologic: No headache, altered sensorium, numbness
and motor dysfunction

Physical Examination
• General survey– Conscious, coherent, ambulatory, not in CP distress
• Vital signs– BP 110/80 PR 80 RR 20 Temp 36.9°C– Wt: 50kg Ht: 155cm BMI: 20.8 (normal)
• Skin – No lesions, hyper/hypopigmentations

Physical Examination
• HEENT– Normocephalic, anicteric sclerae, pink palpebral conjunctivae,
patent ear canal, TM intact,
no nasal discharge, tonsils not enlarged
• Neck– No neck vein engorgement, no masses,
no CLADs
• Breast exam– No skin color changes, nipple retraction or discharge, no
masses, no axillary lymphadenopathies

Physical Examination
• Chest and lung– Symmetrical chest expansion, no retractions, clear
breath sounds
• Heart– Adynamic precordium, PMI at 5th LICS MCL,
regular rate and rhythm– No thrills, heaves and murmurs
• Abdomen– Globular, normoactive bowel sounds, soft, non-
tender

Physical Examination
• Internal exam: – cervix is short and closed– uterus palpable, nontender – no adnexal mass or tenderness
• Extremities– full and equal pulses, no cyanosis and edema

Salient Features
• 72 y/o• Married nulligravid
• Menarche: 10 y/o
• Menopause: 55 y/o
• No history of OCP or HRT use
• Hypertensive
• Dyslipidemic
Salient Features
• NO family history of Cancer
• Vaginal spotting x 4-5 months
• (-) hypogastric pain
• Normal BMI (20.81)
• TVS: uterus slightly enlarged for age
Assessment
• Secretory carcinoma, endometrium; s/p endometrial biopsy (3/8/10)
• Hypertension, dyslipidemia, s/p thyroidectomy (1977), s/p dilatation and curettage (1976)
• Married nulligravid x 37 years

What is Endometrial Cancer?
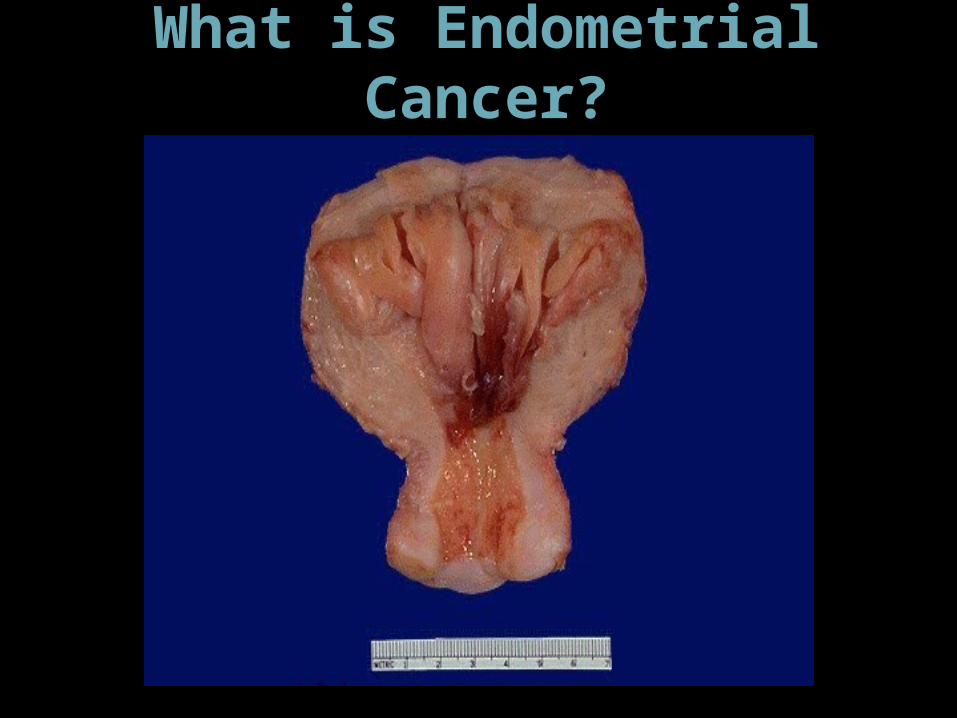
What is Endometrial Cancer?

• The most common gynecologic cancer in developed countries
• 7% of ca in women
• Lifetime incidence ~2-3%
(American Cancer SocietyFemale Cancers: 2000 Statistics)
Lifetime risk
• 5% occur before age 40• Early occurence• Bothersome symptoms, i.e. bleeding early
consultation and diagnosis
• 20-25% before onset of menopause• Perimenopausal women

Cancers of the Uterine Corpus:Histologic Types
• Carcinoma (94%)– Endometrioid (87%)– Adenosquamous (4%)– Papillary Serous* (3%)– Clear Cell* (2%)– Mucinous (1%)– Other (3%)
• Sarcoma (6%)– Carcinosarcoma* (60%)– Leiomyosarcoma* (30%)– Endometrial Stromal Sarcoma (10%)– Adenosarcoma (<1%)
*poor prognosis histology

Endometrial Cancer:Type I/II Concept
• Type I (Obese-type)– Estrogen Related– Younger and heavier patients– Low grade– Background of Hyperplasia– Perimenopausal– Exogenous estrogen
• Type II (Non-obese type: ~10% of total cases)– Aggressive– High grade– Unfavorable Histology– Unrelated to estrogen stimulation– Occurs in older & thinner women
• Familial/genetic (~15% of total cases)• Lynch II syndrome/HNPCC• Familial trend

• Replaced Clinical Staging 1989• Conceptual rationale
– Better defines extent of disease (metastases, depth of invasion, cervix involvement, etc.)
– Minimizes over/under treatment– Minimally increases perioperative
morbidity/mortality– Decreases overall Rx risks and costs– Better allows comparison of therapeutic results
Uterine Cancer: Surgical Staging

Stage I
(73%)Confined to uterus
Stage II
(11%)Cervix involved
Stage III
(13%)
Uterine serosa, adnexae, positive cytology, vaginal metastases, pelvic/aortic node metastases
Stage IV
(3%)Bladder, bowel, inguinal node, distant metastasis
Endometrial Cancer: FIGO Surgical Stage

• Aggressive Histologic Subtypes (Clear-cell, Serous, poorly differentiated)
• Increasing age (over 65)• Vascular invasion• Aneuploidy• Altered oncogene/tumor suppressor gene
expression ( “molecular staging” concept- p53, PTEN, microsatellite instability, MDR-1, HER2/neu, ER/PR, Ki 67, PCNA, CD 31,EGF-R, MMR genes)
• Race?
Endometrial Cancer: Poor Prognostic Factors

Diagnosis of disease
• History of having symptoms– Postmenapausal bleeding– Menorrhagia– Metrorrhagia– Bloody Discharge
• Endometrial biopsy main diagnostic tool – performed either in the office or via D&C in OR
• D&C is the gold standard sampling method – preoperative D&C will agree with diagnosis at
hysterectomy 94% of the time

• Normal endometrial stripe:• Postmenopausal 4- 8 mm
• Postmenopausal on HRT 4- 10 mm
• U/S for Detection of any uterine pathology
• Sensitivity: 85-95%
• Specificity: 60-80%
Transvaginal Ultrasound Screening

Normal Endometrium

Endometrial Polyp

Diagnosis

Sampling of the Endometrium
• Office biopsy procedures (Pipelle, Vabra aspirator, Karman cannula) will agree with a D&C performed in the OR ~95% of the time
• Office biopsy has a 16% false negative rate when the lesion is in a polyp or the cancer covers less than 50% of the endometrium– Guido et al. J Reprod Med. 1995;40:553
Endometroid carcinoma, Grading
• FIGO- Gr 1 - < 5% solid tumor
- Gr 2 - 6 % - 50% solid
- Gr 3 - > 50% solid tumor• NUCLEAR GRADE
– Size, shape , staining and chromatin, variability, prominent nucleoli.
– High nuclear grade adds one point to FIGO grade

Grade 1 Endometroid Carcinoma
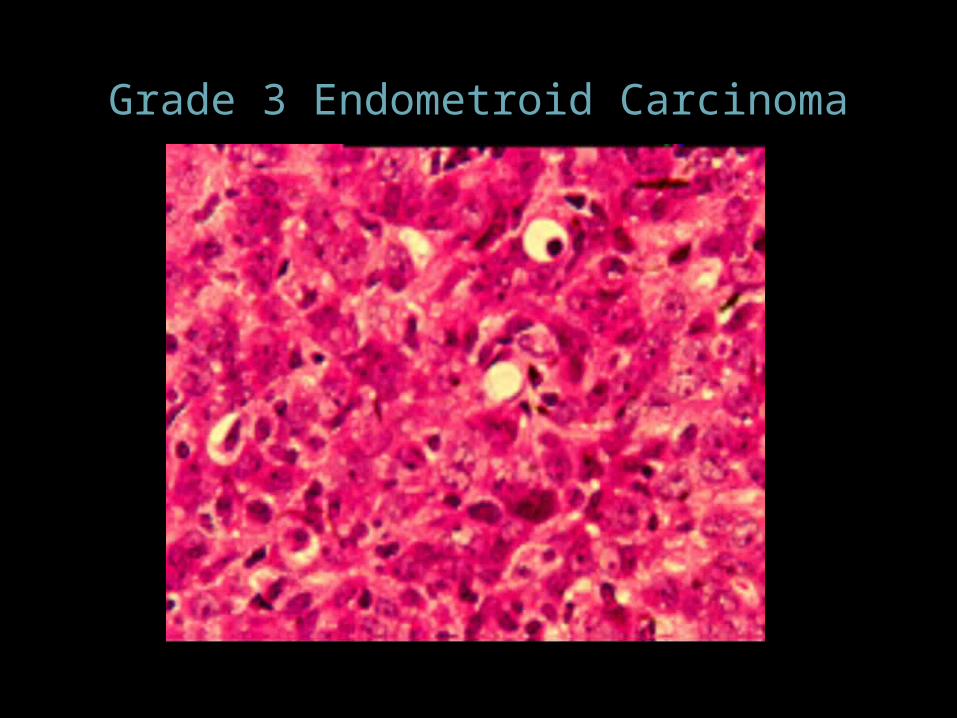
Grade 3 Endometroid Carcinoma

Endometrial carcinoma:Poor Prognosis Cell Types - Papillary Serous

Endometrial Carcinoma - Poor Prognosis Cell Types Clear Cell
•CA125•Chest X-ray•Mammograms•Colon Evaluation•Others as indicated
Uterine Cancer: Pre-op Evaluation
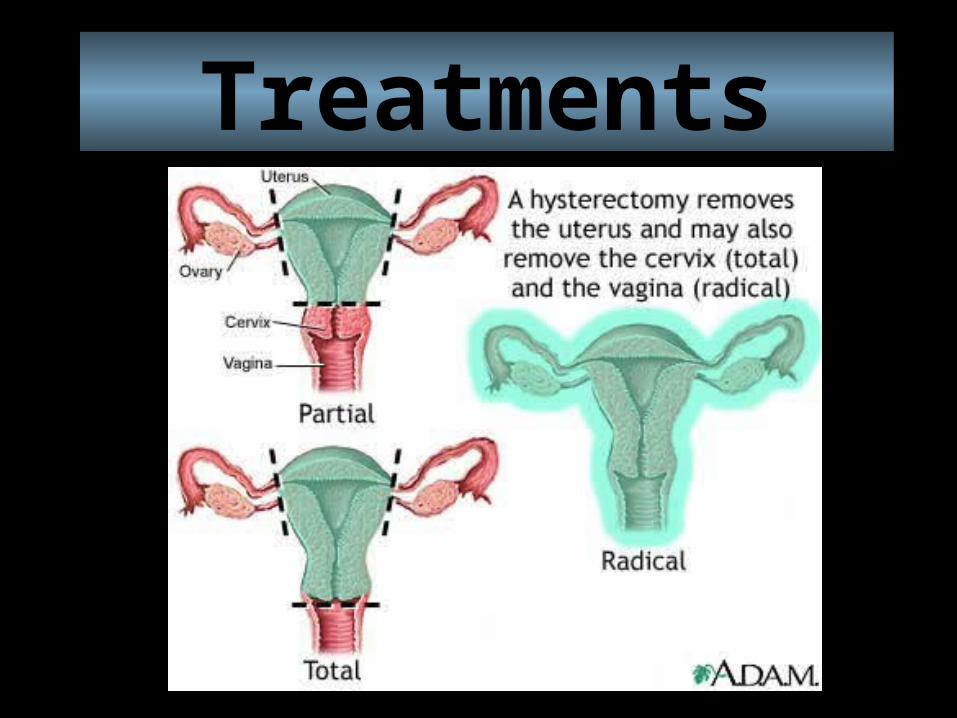
Treatments
Endometrial Cancer: Adjuvant Therapy
• Brachytherapy• External beam radiotherapy• Hormonal therapy• Cytotoxic chemotherapy• Combination therapy

Endometrial Cancer: Recurrence
• Pelvic examination• Pap smears• CA125 (high-risk)• Chest X-ray (high-risk)

Endometrial Cancer: Follow-Up
• 75-95% of recurrences are in first 36 months• 60% of patients have symptoms (pain,
weight loss, vaginal bleeding) • Rare to cure distant recurrences• 50% vaginal recurrences cured
Prevention Early reporting of any abnormal vaginal bleeding
or discharge to the doctor.
Controlling comorbidities: obesity, high blood pressure, and diabetes
Using birth control helps prevent endometrium cancer.
If taking medication that increases/produces estrogen, ask about receiving progesterone.
If you are at risk, get screened regularly.

Thank you!