Embed Size (px)
Citation preview

16 M A S S A G E & B O DY WO R K • O C T O B E R / N O V E M B E R 2 0 0 3
B y B e n B e n j a m i n
There are manyapproaches to thetreatment of pain and
injury problems. Before wetreat a person it is best to havea full and clear understandingof what the problem is. In thisarticle I will outline some of theprinciples that are essential to atherapist’s overall understanding of theinjury process, and I will demonstrate how toapply these principles to two common knee injuries.
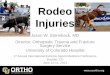
Medialcollateralligament
Lateralcollateralligament

001-029_MNB_O/N_03 8/29/03 1:16 PM Page 17

Introduction
Ihad worked as a therapist for 14years before I truly understood the
injury process. In my world, muscletissue and chronic muscle tensionwere the keys to understanding painand injury. Then, while obtainingmy Ph.D. in sports medicine, I metDr. James Cyriax and Dr. MilneOngley. Together they changed myworldview forever.
After studying and testing Cyriax’stheories on several hundred people, Irealized that much of what I hadbelieved to be true was in fact incor-rect. I had to put aside many of myassumptions and long-cherishedbeliefs. Muscles, muscle injuries andmuscle tension were only one smallpart of understanding the pain andinjury process. When I learned theessential principles of the injuryprocess, it revolutionized my think-ing and my approach to the body.
The first important fact I learnedwas that the formation of adhesivescar tissue in the tendons, ligamentsand joints is often the primary cul-prit in long-term pain. Althoughmuscles get injured most frequently,they also heal more easily on theirown. Tendons, ligaments and joints,on the other hand, often takemonths or years to heal and oftenstay injured for a lifetime.
From my studies I learned thatthere were hundreds of discreteinjuries to muscles, tendons, liga-ments, bursas, nerves and jointsthat could be precisely assessed, andunderstood and successfully treated.I learned an effective hands-on tech-nique called friction therapy, whichcan be used to break down adhesivescar tissue in muscles, tendons, liga-ments and fascia.
Therapists who work with pain and injury problems must gain anunderstanding of what I term theEssential Principles — the underlyingprinciples which govern effectiveassessment and treatment. If you
master this information you will be able to understand the mostinscrutable symptoms, conditions and pain patterns presented by yourclients, including the most difficultpain cases. It took me two decades tograsp these essentials. What followsare some of these important conceptsthat will help you understand the bodyand its pain in a new way. I will use as
an example two common knee injuries— the lateral and medial collateral lig-aments — to show how the applica-tion of these Essential Principles canhelp you clearly assess and effectivelytreat your clients.
PRINCIPLE: The Nature of InjuryAn injury, often called in medi-
cine a “lesion,” is present when
18 M A S S A G E & B O DY WO R K • O C T O B E R / N O V E M B E R 2 0 0 3

there is tissue damage. The damage could manifest as aswelling in a bursa or a joint; pinching of a nerve or atendon; micro-tears in a muscle, tendon, ligament or fas-cia; or a major disruption of tissue like a broken bone ora ruptured tendon. When there is an injury, a part ofthe body has lost its structural integrity and is broken insome way.
APPLICATION: Injuries to the Collateral Ligaments ofthe Knee
The collateral ligaments of the knee hold the leg togeth-er by connecting the femur to the lower leg at the medialand lateral sides of the knee. These ligaments are veryimportant because together they prevent the knee frombuckling inward and outward and keep it on track forforward-backward movement. A person can have a mildsprain of these ligaments, where only a few fibers aredamaged; a moderately severe sprain, where many fibersare torn; or an extremely severe one, where the ligamenttears more extensively or ruptures completely in half.
The medial collateral ligament of the knee is injuredmore frequently than the lateral collateral ligament. Themedial ligament goes from the femur to the tibia whilethe lateral ligament attaches the femur to the fibula.With either of these ligament sprains, some of the fibershave torn either in the middle or near the ends of the lig-ament at the attachments.
The medial collateral ligament is actually attached tothe inner aspect of the joint capsule of the knee and isconnected to another important ligament in the knee, themedial coronary ligament. Medial collateral and coronaryligament tears therefore often accompany each other andare sometimes confused with one another. The lateralcollateral ligament is not contiguous with the joint andtherefore causes less or no swelling when injured.
PRINCIPLE: Pain as a SignalPain is the signal that something has gone wrong in
the body. When the body speaks it is good to listen. Ifthe pain diminishes and disappears within a few days,there is usually nothing to worry about. If the pain per-sists for more than several days, becomes more frequentor hurts with less and less activity then the body is giv-ing the person an important message: “Pay attention!”
The sooner appropriate healing begins, the better are theperson’s chances of full recovery. Early warning signals aretoo frequently ignored and often result in more severeinjuries, which may incapacitate the person for months oryears. Curtailing activities or resting for a few days may beall that is needed. In other circumstances it may be neces-sary for the person to be treated by a physician or hands-on health care practitioner (see box on page 27).
APPLICATION: Pain Signals at the Medial and LateralKnee
In a medial or lateral collateral knee injury, regardlessof where along the ligament the lesion is, pain is feltdirectly on the medial or lateral side of the knee.
A collateral ligament sprain generally arrives in oneof two ways. Suddenly, as if hit by lightning, a personfinds herself on the ground. She fell or was tackled, andthe knee buckled inward (medial collateral) or outward(lateral collateral). Perhaps the person heard a snappingsound, but more likely it was missed in the confusion ofthe fall. The person’s knee hurts everywhere, and shehobbles off trying not to bend it. Over the next fewhours the knee swells, feels hot to the touch, and con-tinues to ache. With the passing hours, the knee stiff-ens, making bending and straightening it difficult, andby the next day the pain begins to concentrate on theinner or outer side of the knee. Activity automaticallybecomes limited because walking is painful and any-thing more strenuous is impossible.
In the second case, a person might start feeling atwinge of pain now and then while playing tennis, run-ning or hiking. After a few weeks the pain settles onthe inside of the knee and is more constant. There maybe slight swelling or maybe not. The person begins tonotice pain as he begins an activity; then the pain goesaway; and an hour or so after finishing the activity ithurts again. The pain mysteriously disappears in themidst of activity because the ligament warms up(warmed-up ligaments don’t hurt). Eventually the per-son can no longer do certain strenuous activities with-out pain.
In both these cases the problem is the same: A tornmedial or lateral collateral ligament. This mysteriousinjury has many personalities. It can come on quicklywith mild, moderate or severe pain; or, it can comemore slowly, building as it goes, and be either mild ormoderately painful. No matter how it starts, it oftenlingers for a long time, causing confusion by coming andgoing. The medial collateral ligament injury usuallyprompts the phrase “my bum knee,” for the pain has ahabit of appearing and disappearing mysteriously. Whenthe injury results from trauma, it’s easy to understandwhat caused it. When it appears slowly, the causes aresubtle and often interlocking: poor leg alignment withknees turned-in or out; excess muscle tension, whichleads to early fatigue; or loose or stretched-out ligamentscaused by old sprains or poor stretching exercises.
PRINCIPLE: Scar Tissue as the Secret of Chronic PainSometimes the acute pain of an injury disappears
completely and you are never bothered by it again.
e s s e n t i a l p r i n c i p l e s
O C T O B E R / N O V E M B E R 2 0 0 3 • M A S S A G E & B O DY WO R K 19
001-029_MNB_O/N_03 9/5/03 9:40 AM Page 19

e s s e n t i a l p r i n c i p l e s
20 M A S S A G E & B O DY WO R K • O C T O B E R / N O V E M B E R 2 0 0 3
Sometimes, however, pain becomesa chronic problem. Most people donot realize that the cause of mostchronic pain from soft tissueinjuries is the initial poor healing of the injury. Adhesive scar tissueforms, binding the originally dam-aged tissue to the adjacent soft tis-sues. Scar tissue formation is normalwhen soft tissue injuries are repair-ing. When scar tissue forms in theappropriate places, it is the biologi-cal glue that holds torn fiberstogether. However if this healingprocess occurs in a random fashion,the scar tissues forms a jumbledmass of adhesions, which tear onnormal movement.
Scar tissue within the musculo-skeletal system forms primarily in lig-aments, tendons, muscles, fascia andjoint capsules. When scar tissue formsin the fascial tissue, it often binds theskin to its underlying fascia, limitingthe movement of the skin. If thisabnormal scar tissue is placed undertension, the nerve endings in the skinand the underlying fascia are stimulat-ed, producing pain. Fascia also liesdeep in the body, where its purpose isto envelope and to provide a glidingsurface for muscles, tendons, liga-ments and other structures. Puttingtension on this scar tissue in the deep-er fascia again stimulates local nerveendings and produces pain. Methodsof fascial release can be employedwith beneficial results. However, untilall the abnormal adhesive scar tissueis removed from all of the affectedstructures, a pain-free state cannot beachieved.
Movements that excessively stressthe damaged tissue result in re-injury.This re-injury results in the forma-tion of more adhesive scar tissue.Understanding how to encourage thecorrect healing of tissues preventsthese complications. Breaking thecycle of tearing and re-tearing ofadhesive scar tissue is the key toeffective treatment.
APPLICATION: Scar Tissue andChronic Pain at the Medial and Lateral Knee
A complication of torn collateralligaments is the “bum-knee” syn-drome. In one way or another, theligament has been sprained, andthough there are brief reprieves, theperson begins to think, “It’s gone,I’ve beaten the problem.” Then thepain mysteriously returns. It canrecur with what was seemingly a
simple activity such as helping afriend move some boxes up a flightof stairs, squatting for five minuteswhile doing a quick weeding in thegarden, running a mile every otherday for two weeks, or making ablock-long dash to catch the bus.Troublesome adhesive scar tissuethat keeps re-tearing is the key tounderstanding this mystery.
When the knee bends and straight-ens, the collateral ligaments normally➝

22 M A S S A G E & B O DY WO R K • O C T O B E R / N O V E M B E R 2 0 0 3
move freely across the bone on the medial and lateralsides of the knee. If a collateral ligament is injured andheals properly, the scar tissue that’s formed within theligament does not interfere with its free movement.However, if the injury doesn’t heal well, scar tissue mayform a matted scar within the ligament or between theligament and the bone where it's not supposed to beattached. This scar tissue often acts like glue, adheringthe ligament to the bone so that its free-sliding move-ment becomes more limited. If activities are strenuousand jarring, or involve twisting, the scar tissue does nothold and tears repeatedly. When a ligament warms upduring activity, pain often diminishes or disappearstemporarily. An hour or two later, when the ligamenthas cooled down, the pain intensifies or returns. Thiscycle of poor healing and scar tissue re-tearing can hap-pen hundreds of times over many months or years. Inits most extreme form the ligament completely rupturesin half, and the knee becomes unstable. This event onlyoccurs in very serious accidents or severe falls. If itoccurs, the person should see a doctor immediately.
PRINCIPLE: Injury Verification through Resisted andPassive Testing
A therapist should begin the assessment of a client byobtaining a complete history of the injury, including adescription of the location of the pain, any traumaticevent that led to the injury, and any factors that aggra-vate or relieve the pain. The therapist can further verifythe injury through palpation and by applying a series ofsimple tests to the region. These tests will help the ther-apist pinpoint the location of injured structures, evalu-ate the severity of the injury, and develop a rationale fora treatment plan.
A resisted test is an isometric contraction againstresistance that does not moved through space. This typeof test primarily tests for injury to muscles and tendons,those structures which initiate movement. It also testsfor weakness when there is disc pressure on the nerve.
During a passive test, the client behaves like a rag dolland does not assist during the movement that the thera-pist takes the client through. Passive tests primarilycheck for injury to ligaments, joints and bursas, struc-tures that do not initiate movement.
APPLICATION: Verification of Collateral Ligament Knee Injuries
One of the clearest signs of a collateral ligamentinjury in the knee is the location of the pain. If youknow how to palpate these ligaments, you can find theprecise source of the pain. The lateral collateral liga-ment is easy to find. When a person crosses the legs, thelateral collateral becomes taut and sticks right out at the
lateral knee. To find it place your finger on the head ofthe fibula just below the lateral knee while the legs arecrossed and move superiorly until you come to theattachment on the femur. The medial collateral ligamentis a little trickier to find because the ligament is flat-tened against the bone. To find it let the person liesupine and bend the knee so that the foot is on thetable. Now place your finger at the inferior pole of thepatella; this puts you at the joint line. Now slide yourfinger medially in the crevice of the joint line ninetydegrees until you reach the ligament. It is relativelyclose to the skin surface. Injuries to this ligament oftenoccur at the joint line in the middle of the ligament.
Resisted tests should not cause pain in cases of collat-eral ligament injuries, since the resistance tests activestructures such as muscles rather than the ligaments.The following list offers one palpation test and four pas-sive tests to help you assess whether the collateral liga-ments of the knee are injured.
Test 1Heat — Place the back of your hand alternately on
the inner side and then outer side of both knees andcompare their relative heat. If there is active inflamma-tion and swelling in one knee, there is usually a heat differential.
Test 2Passive Flexion of the Knee — Lift the knee slight-
ly toward the chest and gently flex the knee by bringing
the heel toward the buttock. If you reach the buttockwithout pain or limitation, give the foot a slight pushtoward the buttock. If the knee is swollen you will notbe able to bring the heel to the buttock, so do not forceit. If the motion is limited, check the other knee to seethat it is not just the person’s natural structure.

Test 3Passive Extension of the Knee — Place one hand
under the Achilles tendon and the other hand above theknee. Now press down with the hand above the knee,while simultaneously pulling up with the hand underthe Achilles. You are gently, passively trying to straight-en the knee. If the knee is swollen, movement will beslightly limited and/or painful.
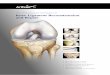
Test 4Valgus (Stressing the Medial Knee) — Standing next
to the knee facing the person’s head, place your outerhand on the lateral aspect of the knee with your fingersjust under the knee. Then, place the palm of your innerhand on the medial ankle as shown in the photograph.Now apply a shearing force in opposing directions tostress the medial knee. In other words push laterallywith the hand on the medial ankle and medially withthe hand on the lateral knee. If there is no pain whenthe knee is taut, give it a slight extra push. If there isstill no pain, slide the leg off the table laterally andrepeat the test with the knee slightly bent (about one inch).
Test 5Varus (Stressing the Lateral Knee) — Facing the
client’s head, place your outer hand on the lateral ankle.Then place your inner hand on the medial knee withyour fingers just under the knee. Now apply a shearingforce in opposing directions to stress the lateral knee,that is, press laterally with the hand on the medial kneeand push medially with the hand on the lateral ankle. If there is no pain when the knee is taut, give it a slightextra push. If there is still no pain, repeat the test withthe knee bent only one inch by slipping the leg off the table.
If the valgus test or the varus test causes pain, you haveverified a strain of the medial collateral or lateral collater-al ligament respectively. It should hurt where the personnormally feels pain. If the injury is severe, you have toexert only a small amount of pressure during the test. If itis mild, you must exert more pressure. If passive flexionand/or passive extension are painful or limited in theability to move through a full range of movement itmeans that there is some swelling accompanying the col-lateral ligament injury. Collateral ligament injuries areoften accompanied by a tear of a ligament that attachesthe meniscus to the tibia (the coronary ligament). Thesetwo ligaments are often injured simultaneously.
PRINCIPLE: Healing Injured TissuesMost of the body’s healing processes proceed without
our conscious direction. When musculo-skeletal struc-tures are damaged or torn, the body’s wisdom ensuresthat the damage, whenever possible, will be repaired.However, to a large extent the degree and quality of thisrepair depend upon our own participation. The naturalmechanisms of inflammation and wound healing areusually excessive for the job at hand. The body over-compensates when it responds to injury. More plasma,red and white cells, blood platelets and chemical media-tors are released than are actually needed to allow fullhealing to occur. Therefore, additional scar tissue is like-ly to form. This scar tissue often binds together damagedand undamaged structures, resulting in adhesions that,
O C T O B E R / N O V E M B E R 2 0 0 3 • M A S S A G E & B O DY WO R K 23
➝
e s s e n t i a l p r i n c i p l e s

26 M A S S A G E & B O DY WO R K • O C T O B E R / N O V E M B E R 2 0 0 3
as we have seen, can lead to re-injury and to chronic pain.
There are several methods bywhich we can help the body limitthe formation of adhesive scar tis-sue and/or recover from adhesionsthat have already formed. The firstof these methods is friction thera-py. A therapist applies cross-fiberfriction therapy in a controlledmanner to break up specifically tar-geted areas of adhesive scar tissue.When friction therapy is accompa-nied by the second method, “heal-ing in the presence of a full rangeof motion,” healthy tissue can growwithout the re-formation of adhe-sions. This means that in order toheal properly, the body part mustbe regularly moved through its fullrange of movement during thehealing process so that adhesionsdo not form. If the injured personis able to collaborate with thebody's healing processes by ade-quate physical movement, completehealing is more likely. If the personis unable to perform the requiredexercises by him or herself, it isimportant to have a therapist assistthe person in a full range of motionof the injured part.
APPLICATION: Treatment forInjuries to the Collateral Ligaments ofthe Knee
Friction therapy applied to injuredcollateral ligaments, along with fullrange of movement of the knee, canbe a safe and effective treatment forthese injuries. The therapist shouldalso be aware of other treatmentoptions and refer the client to otherpractitioners when necessary. Thesetreatments include:
Deep Massage and Friction TherapyThis is an effective treatment for
medial and lateral collateral kneeligament injuries if done twice aweek for three to four weeks. Itspeeds the healing of the ligament
and prevents scar-tissue formation,especially if done soon after the ini-tial injury. In long-standing cases,treatment may take longer and mayneed to be combined with manipula-tion by a chiropractor or osteopathto free the ligament from the bone.
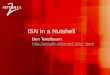
Friction therapy for the medialcollateral ligament. Sit on a stoolnext to the injured knee and placeyour index finger at the lower pole ofthe patella. Now trace the joint linewith a moderate pressure as you movearound the knee toward the table in astraight line medially. Half way downtoward the table you will feel the liga-ment under your finger. It feels abouta quarter of an inch wide and a six-teenth of an inch thick. It isn’t thateasy to find until you know it, likemost things in life. Place your middleor index finger over the ligament and
apply a friction stroke upwards, thenrelax as you bring your hand back toyour original position. Friction five orsix minutes, take a break and repeatagain for five or six minutes. Mostoften the ligament is injured here atthe joint line, but it may be injured aswell at the tibial attachment or at thefemoral attachment. In that case,those areas must be frictioned also.
Friction therapy for the lateralcollateral ligament. Sit on a stoolnext to the injured knee and placeyour thumb on the head of the fibulajust below the lateral knee. Now movesuperiorly toward the condyle of thefemur with a moderate pressure. Halfway toward the femur you will feelthe ligament under your finger. Itfeels like a tight band about a quarterof an inch wide. It is sometimes easierto find if the client crosses the leg,
001-029_MNB_O/N_03 9/5/03 9:44 AM Page 26

placing the ankle of the bad knee just above the oppositeknee. This causes the lateral collateral ligament to protrudeout from the knee. Once you have located the ligament,palpate for where the pain is felt. This is where the pri-mary scar tissue is located. Using your middle or index fin-ger over the ligament, apply a friction stroke upwards, thenrelax as you bring your hand back to your original posi-tion. Friction five or six minutes as described above, take abreak and repeat again. Most often the ligament is injuredhere at the joint line, but it may be injured as well towardthe fibula attachment or toward the femoral attachment. Inthat case, those areas must be frictioned also.
After frictioning the ligament, deep massage shouldbe applied to the front thigh and knee area. This willenhance the circulation and speed healing and theremoval of waste products. Don’t neglect working onthe other leg as it is usually doing double work to com-pensate for the injured leg.
Exercise TherapyThe knee must be moved under a little stress so that
adhesive scar tissue does not reform. As a first exercisehave the client sit and swing the leg for two or three min-utes several times a day. After three or four treatmentshave the person lean against a door and do 10 to 20 miniknee squats where the knee bends no more than 45degrees. As the knee improves the squats should deepen sothat the thigh and lower leg are at a 90 degree angle. Theseexercises prevent the reestablishment of adhesive scar tis-sue while building strength in the muscles and ligaments.
ManipulationThis is only effective where there is an external adhesion
to the femur. This occurs with medial collateral ligamenttears only.
Anti-inflammatory InjectionAn anti-inflammatory injection is helpful in stopping
inflammation and pain and preventing internal adhesionswhen friction is not successful. It is also effective in thechronic stage when there are adhesions to the bone. Theinjection, when properly given, ruptures the adhesionsand prevents additional adhesions from forming.
Proliferant InjectionIf the ligament has been excessively stretched and
weakened, massage, exercise, oral medication, manipula-tion, or other methods of treatment cannot, to myknowledge, tighten the ligaments. Proliferant injectionscause the ligaments to tighten and strengthen.
A proliferant is usually composed of dextrose (a sugar),glycerine (which helps the blood congeal), xilocane (thestuff the dentist uses to numb your mouth) and phenol(which acts as a sterilizing agent). The dextrose is themain active substance; it irritates the ligament or tendontissues and tricks the brain into producing (proliferating)many like cells of tissue.
There are three goals of the proliferant treatment pro-cedure: First, to break up adhesive scar tissue, second,to tighten the stretched ligaments, and third to strength-en the weakened ligament fibers.
SurgeryIf the ligament has been completely ruptured, surgical
repair is best performed as soon as possible. After theinitial recovery period, rehabilitative exercise therapyand deep massage aid in the healing process.
Conclusion
In this article I have introduced several of what I considerto be the Essential Principles of the field of orthopedic
massage, and have applied these principles to the specificcase of two common knee injuries. The principles discussedhere not only changed the way I view injury and the heal-ing process, but also changed the ways in which I assess,verify and treat the people who come to me with acute andchronic pain. I hope you have gained a picture of the impor-tance these principles can have in your day-to-day workwith your own clients.
Ben Benjamin holds a doctorate in education and sports medicine. He isthe founder and president of the Muscular Therapy Institute in Cambridge,Mass., and the author of Listen to Your Pain, Are You Tense? andExercise Without Injury. He can be contacted at [email protected].
M&B
It is essential to see a doctor if:1) the pain is severe 2) there is paralysis3) there is numbness or constant pins and
needles in the arms, hands, legs or feet4) the area is swollen5) a snapping sound or tearing sensation
accompanied the injury6) there is weakness of the injured body part7) there is extreme limitation of movement or
inability to use the injured area8) there is malfunction of the bladder or bowel9) there is associated nausea, vomiting or blurred
vision 10) the person is disoriented, dizzy or cannot per-
form normal activities because of the injury
e s s e n t i a l p r i n c i p l e s
O C T O B E R / N O V E M B E R 2 0 0 3 • M A S S A G E & B O DY WO R K 27
001-029_MNB_O/N_03 9/5/03 9:31 AM Page 27