Embed Size (px)
Citation preview
BVS in bifurcations, techniques, acute and long-term outcome
Maciej Lesiak Department of Cardiology
University Hospital in Poznan, Poland
Potential conflicts of interest
Speaker's name: Maciej Lesiak
I have the following potential conflicts of interest to report:
Consulting, speaker bureau: Abbott Vascular, AstraZeneca, B Braun,
Boston Scientific, Tryton Medical
Bifurcation stenting & scaffold limitations
Device’s profile crossing through the struts of the side of the stent (SB scaffolding)
Dilatation limits fractal geometry of bifurcation
Struts’ thickness double / triple layers (overlapping stents, crush technique)
Struts’ fragility strut fracture (radial strength, floating struts…)
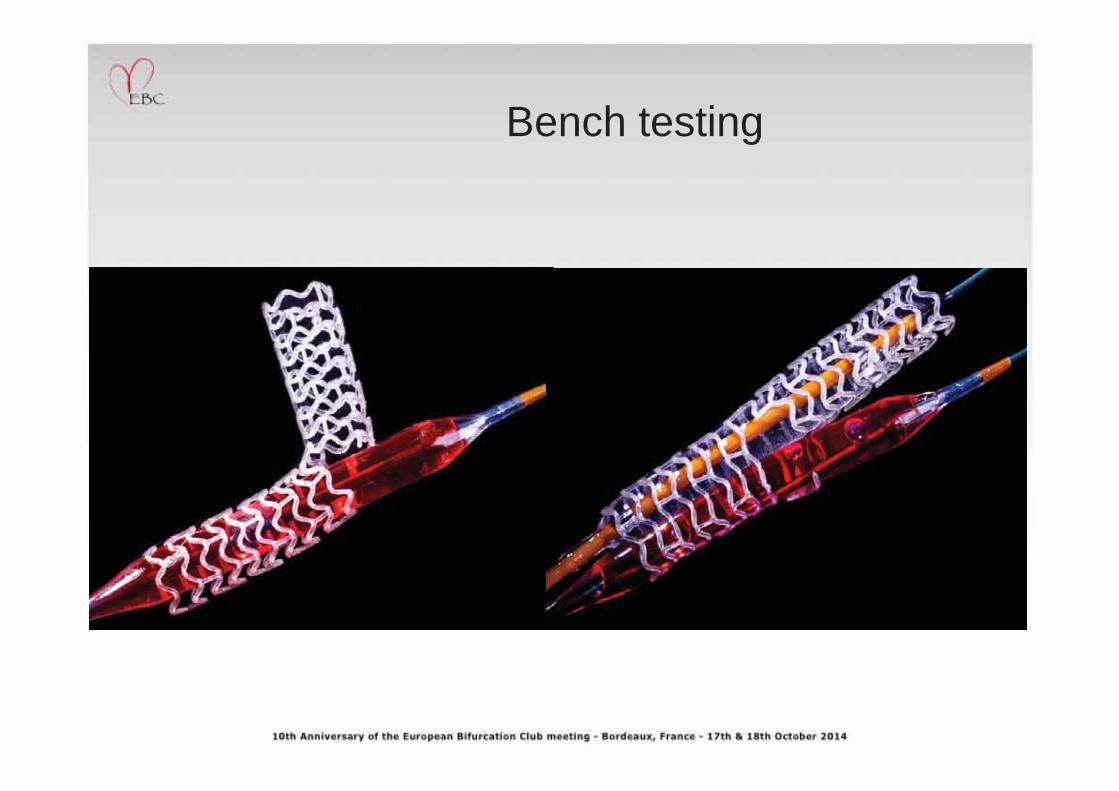
Bench testing
Ormiston, TCT 2013
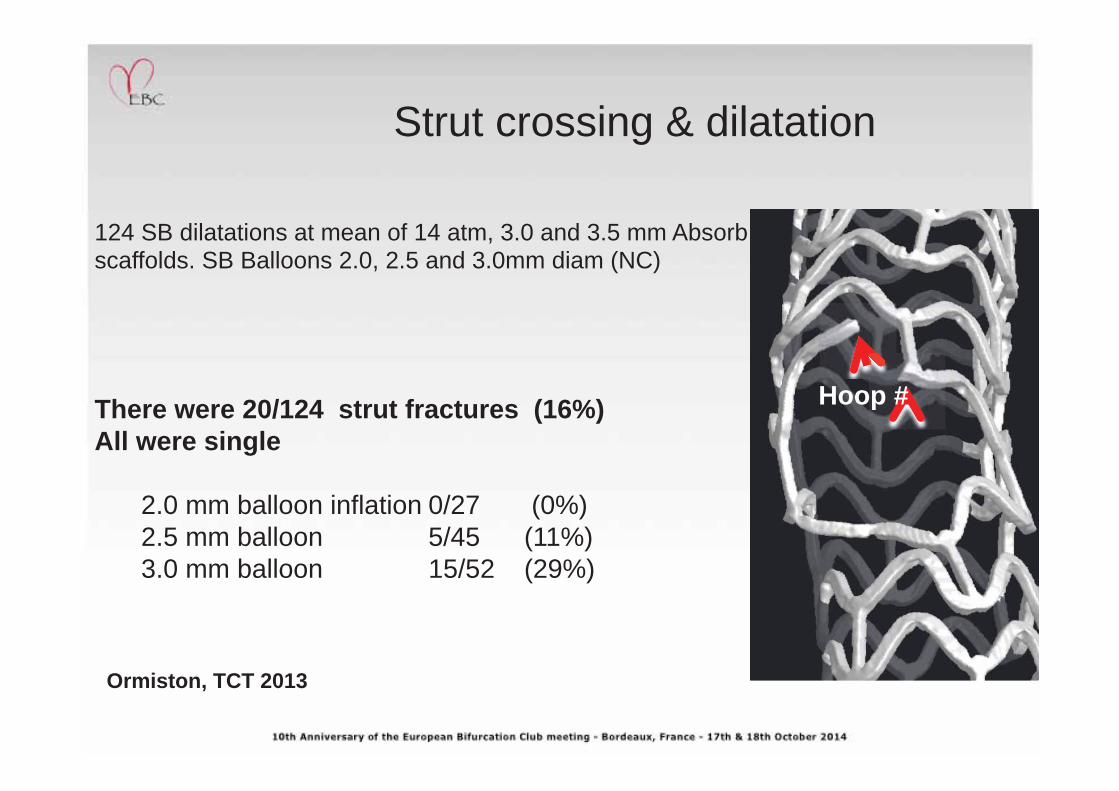
124 SB dilatations at mean of 14 atm, 3.0 and 3.5 mm Absorb scaffolds. SB Balloons 2.0, 2.5 and 3.0mm diam (NC)
There were 20/124 strut fractures (16%) All were single
2.0 mm balloon inflation 0/27 (0%) 2.5 mm balloon 5/45 (11%) 3.0 mm balloon 15/52 (29%)
Hoop #
Strut crossing & dilatation
Poznan Bifurcation BVS Registry
Consecutive bifurcation cases treated with BVS
Informed consent
Any indication to PCI (stable or ACS)
Any Medina type
No excessive calcium & tortuosity
Inclusion / exclusion criteria
General stenting strategy
• Provisional technique – the treatment of choice
• Avoiding complex techniques with high probability of scaffold struts’ fractures (Crush, Culotte)
• Recommended complex techniques: T or TAP
Provisional technique
• Pre dilatation – MV only
• Scaffold sizing according to proximal MV RD (low pressure impl.)
• POT – short NC bal. max. 0.5 mm larger than the reference, high
pressure
• End of procedure if a SB ok (DS ≤ 75% & TIMI 3)
• Otherwise rewire and FKB with minimal protrusion with two short
NC balloons at maximum 8 ATM, +/- 2nd POT
• Bailout SB stenting if needed using T or TAP
Complex techniques
Only T or TAP technique used
In TAP metallic DES instead of BVS in case of difficulty with delivering BVS through the struts of a scaffold
Using Crush or Culotte strongly discouraged
OCT in complex cases strongly recommended
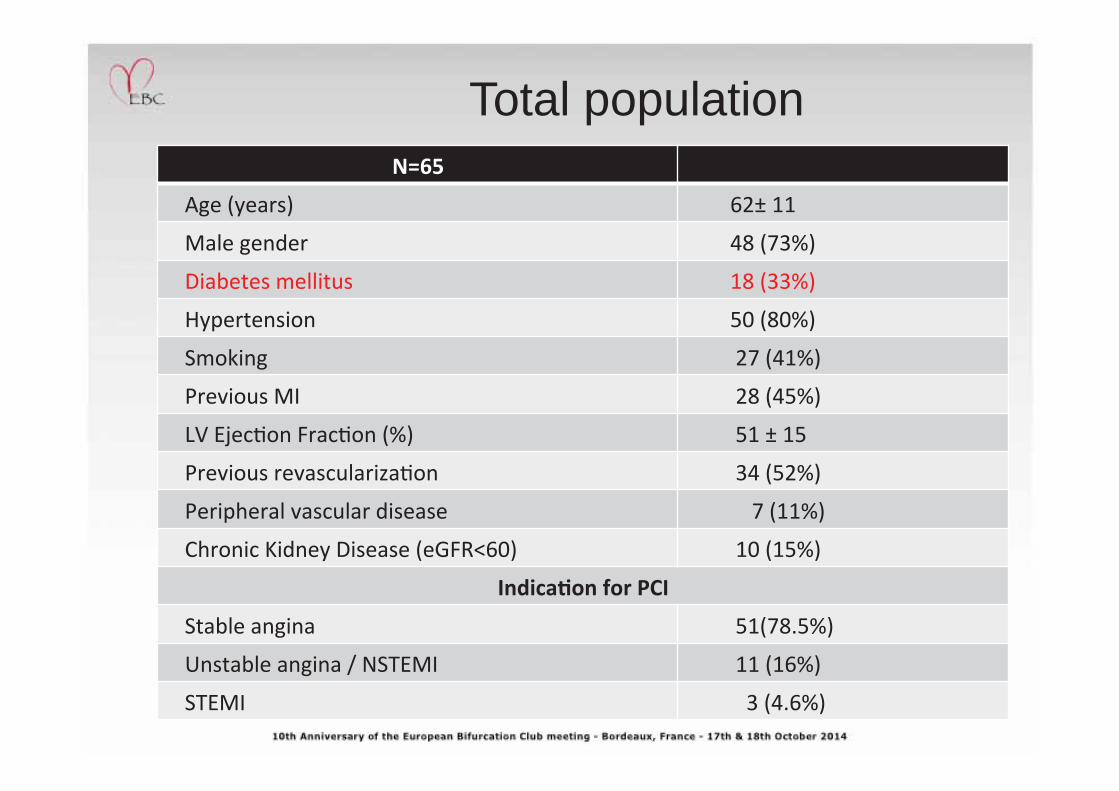
Total population
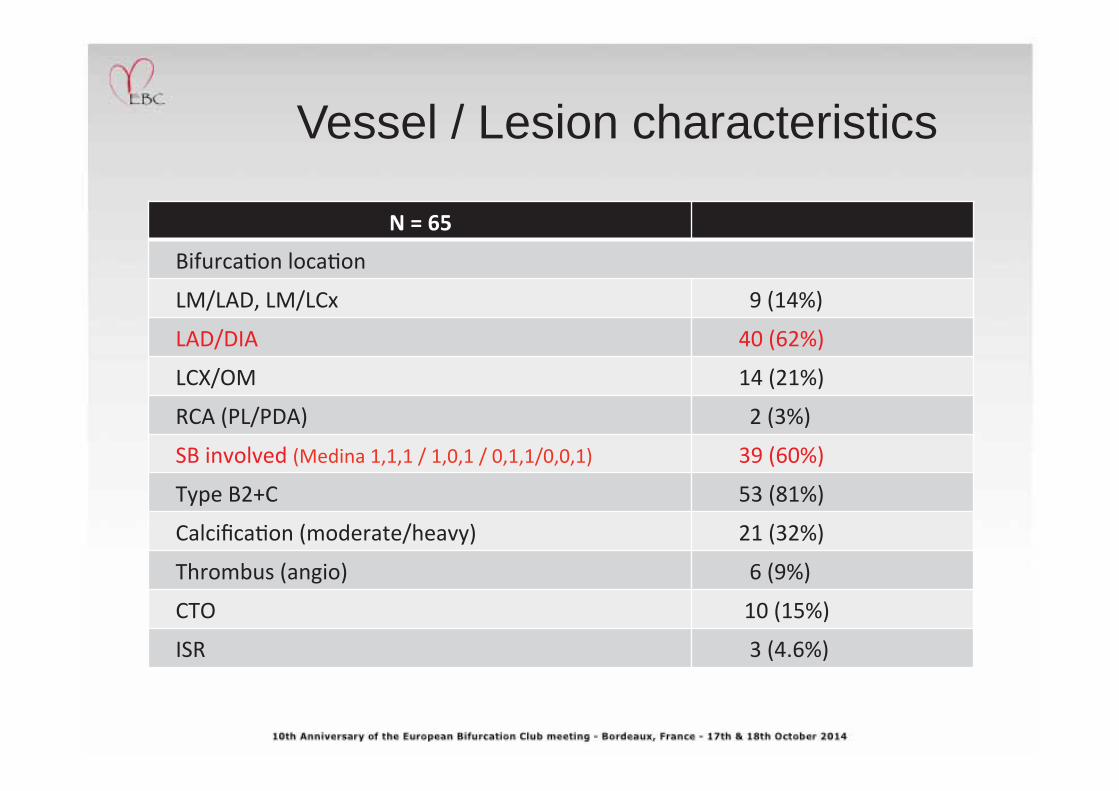
Vessel / Lesion characteristics
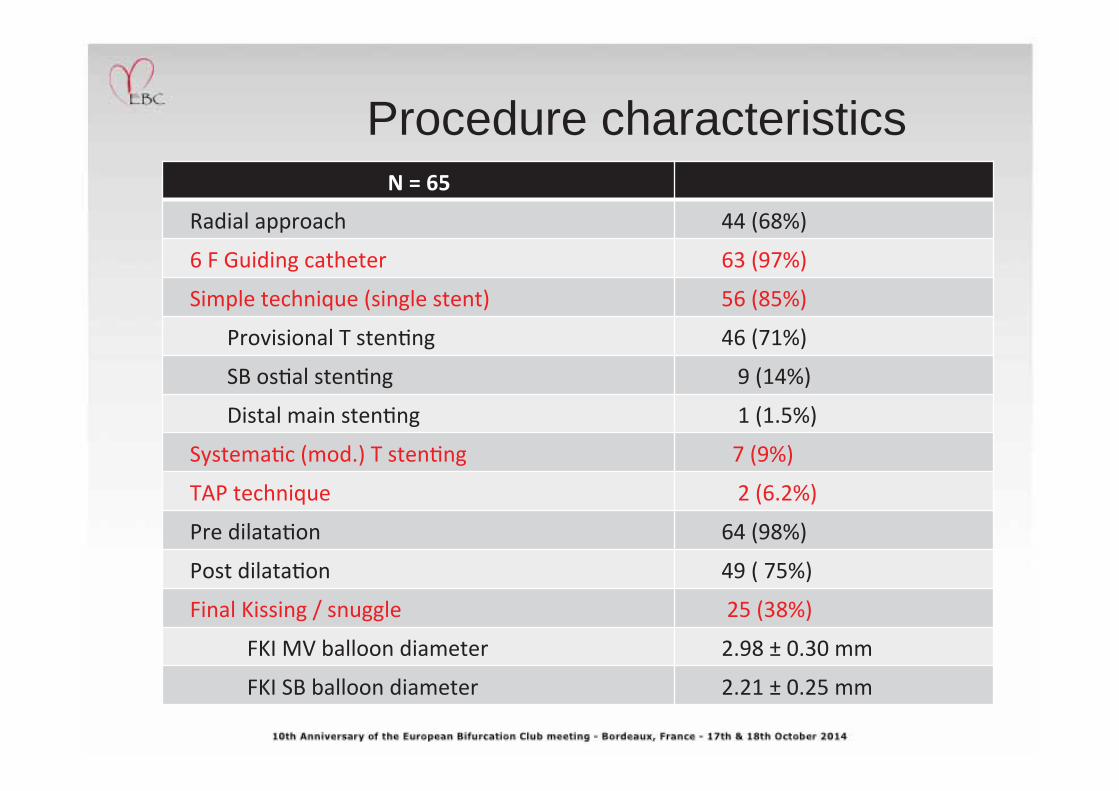
Procedure characteristics
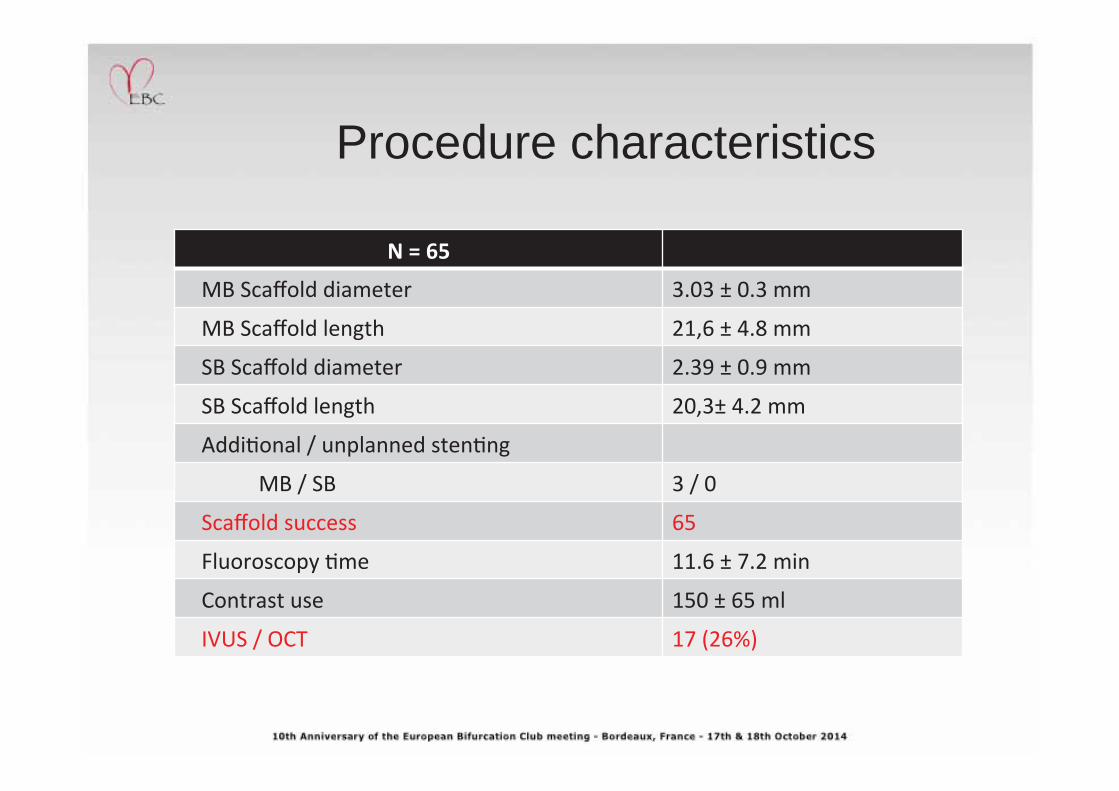
Procedure characteristics
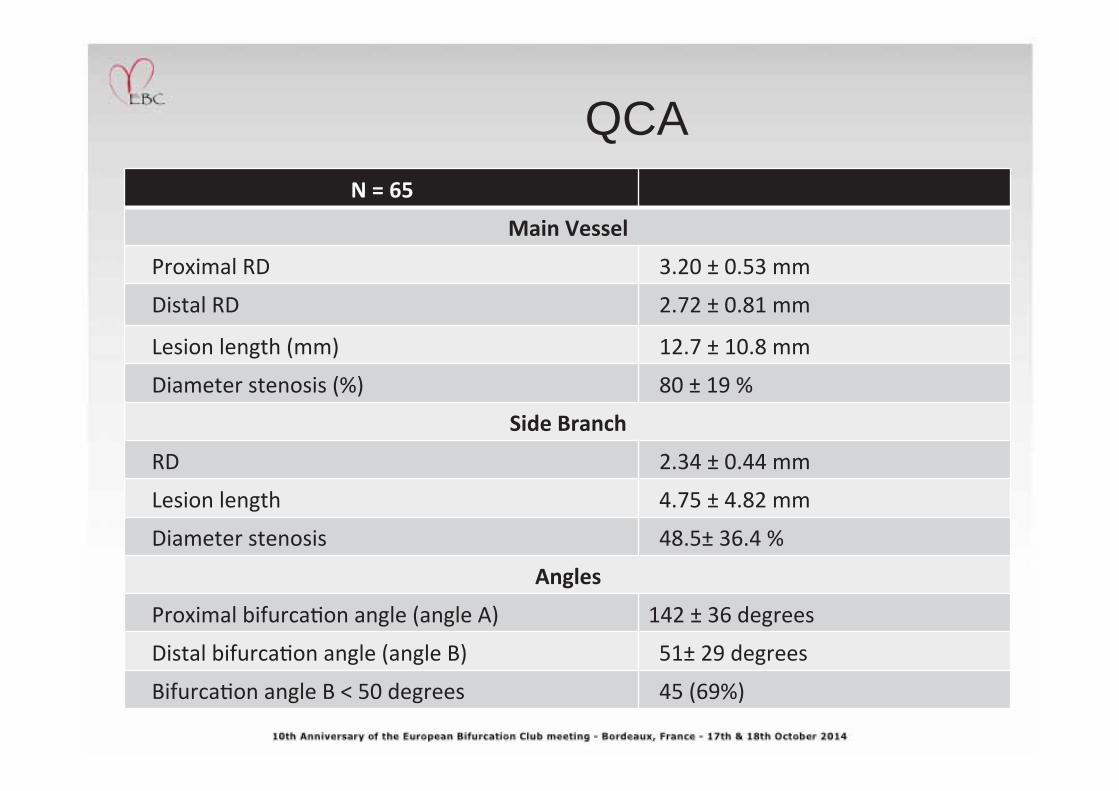
QCA
DAPT @ Discharge
Initial strategy ASA 75–100mg + Clopidogrel 75mg recommended for 12 months Since December 2013 Clopidogrel resistance testing (Multiplate) In patients with high on-treatment platelet reactivity -ticagrelor/prasugrel instead of clopidogrel Since March 2014 Ticagrelor 2 x 90 mg for 12 months after procedure
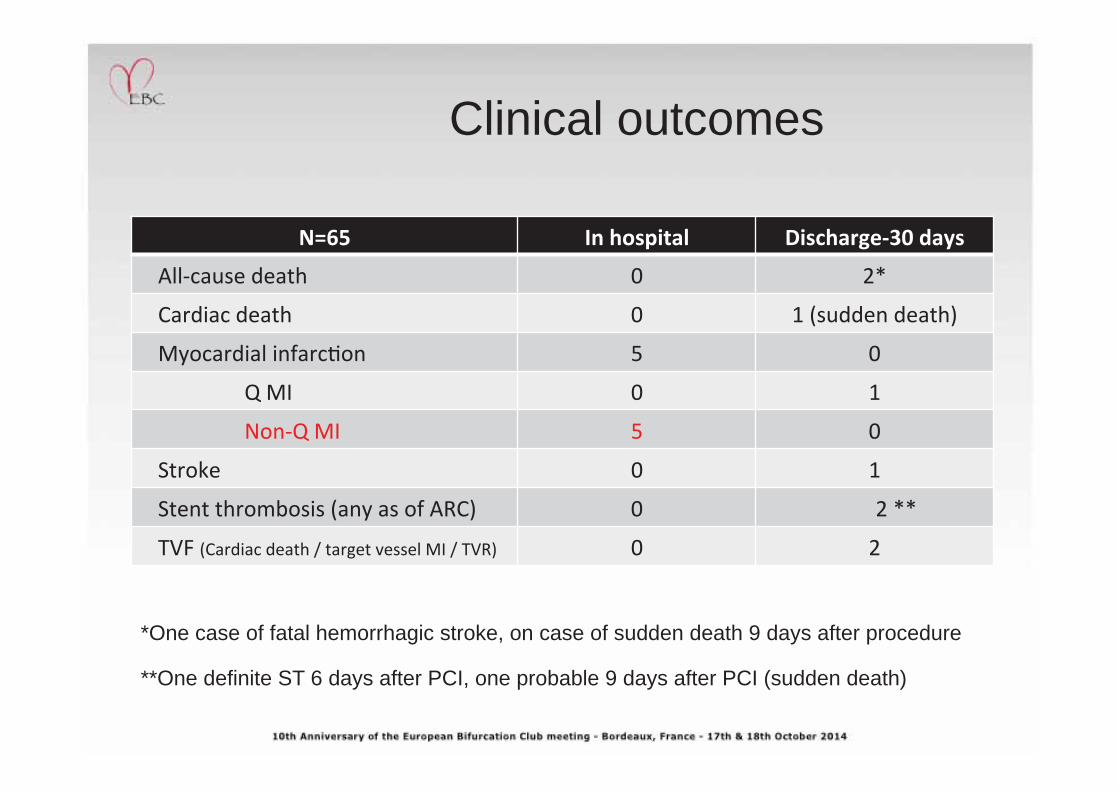
Clinical outcomes
*One case of fatal hemorrhagic stroke, on case of sudden death 9 days after procedure
**One definite ST 6 days after PCI, one probable 9 days after PCI (sudden death)
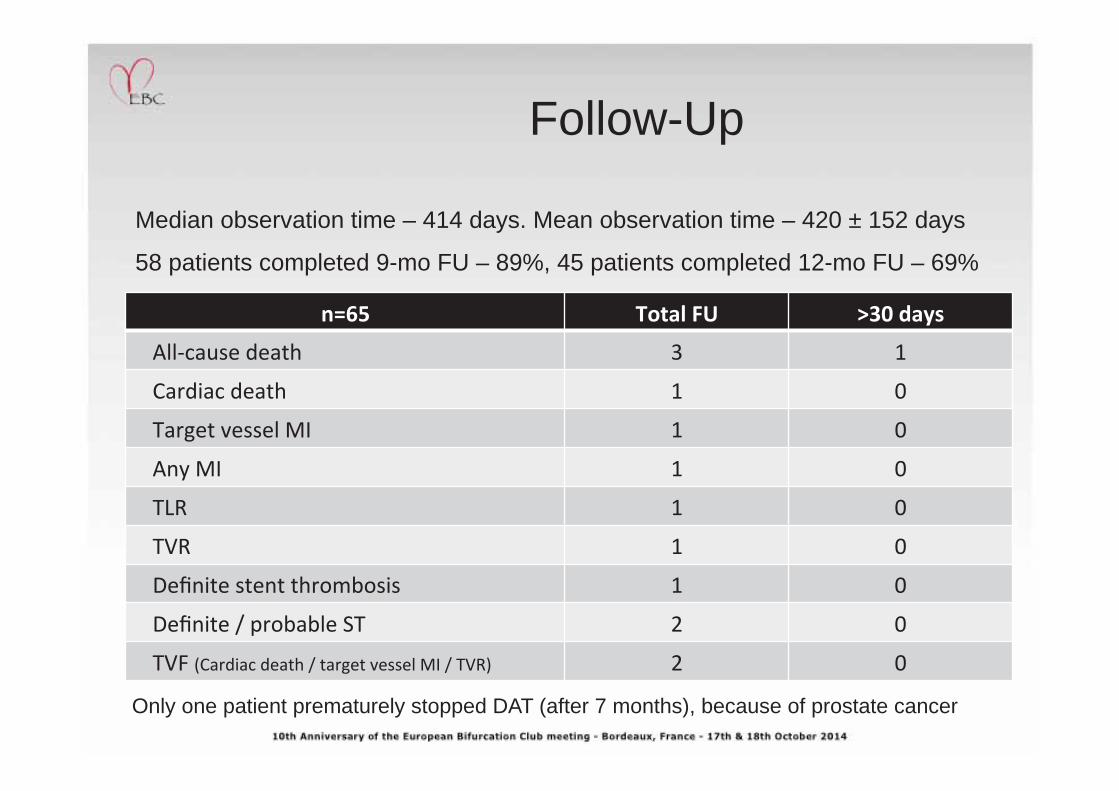
Follow-Up
Median observation time – 414 days. Mean observation time – 420 ± 152 days
58 patients completed 9-mo FU – 89%, 45 patients completed 12-mo FU – 69%
Only one patient prematurely stopped DAT (after 7 months), because of prostate cancer
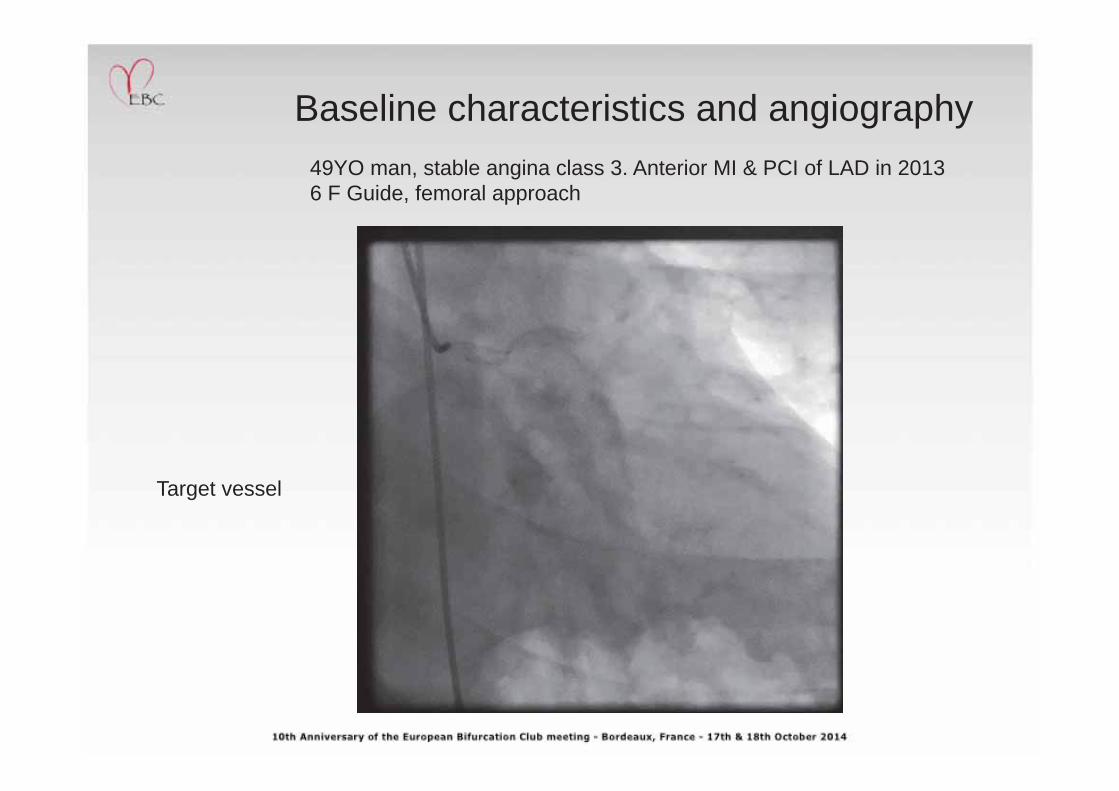
Baseline characteristics and angiography 49YO man, stable angina class 3. Anterior MI & PCI of LAD in 2013 6 F Guide, femoral approach
Target vessel
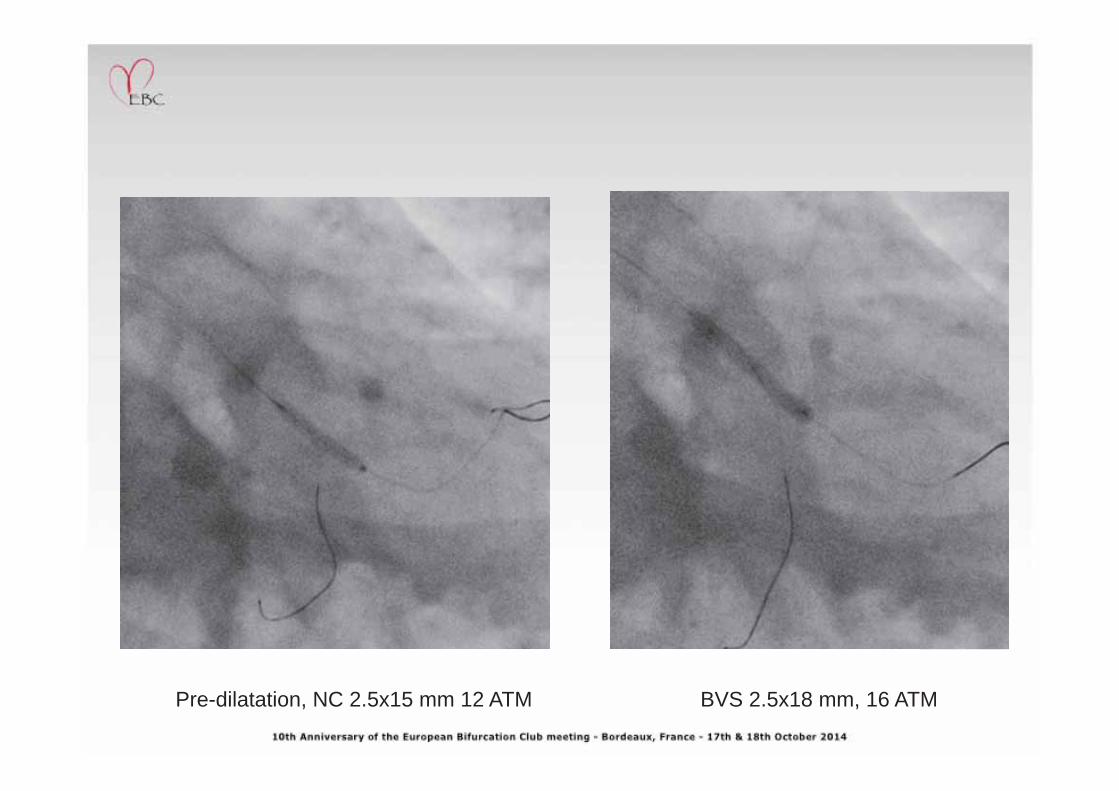
Pre-dilatation, NC 2.5x15 mm 12 ATM BVS 2.5x18 mm, 16 ATM
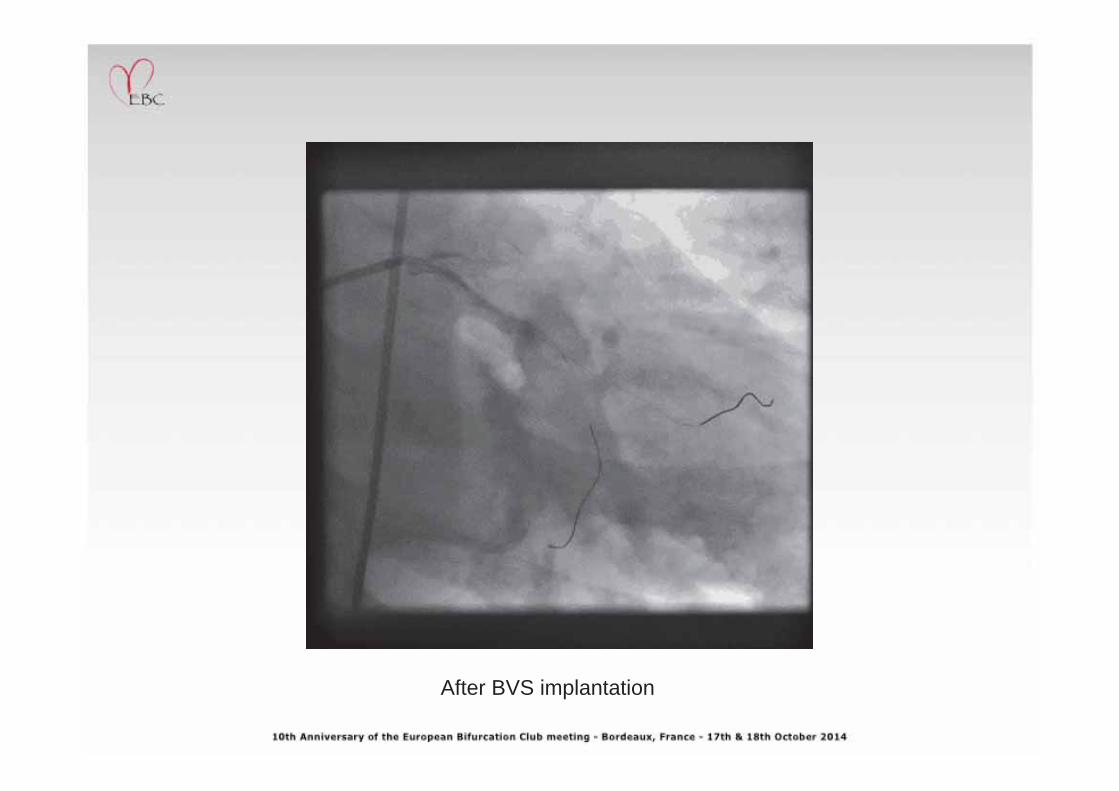
After BVS implantation
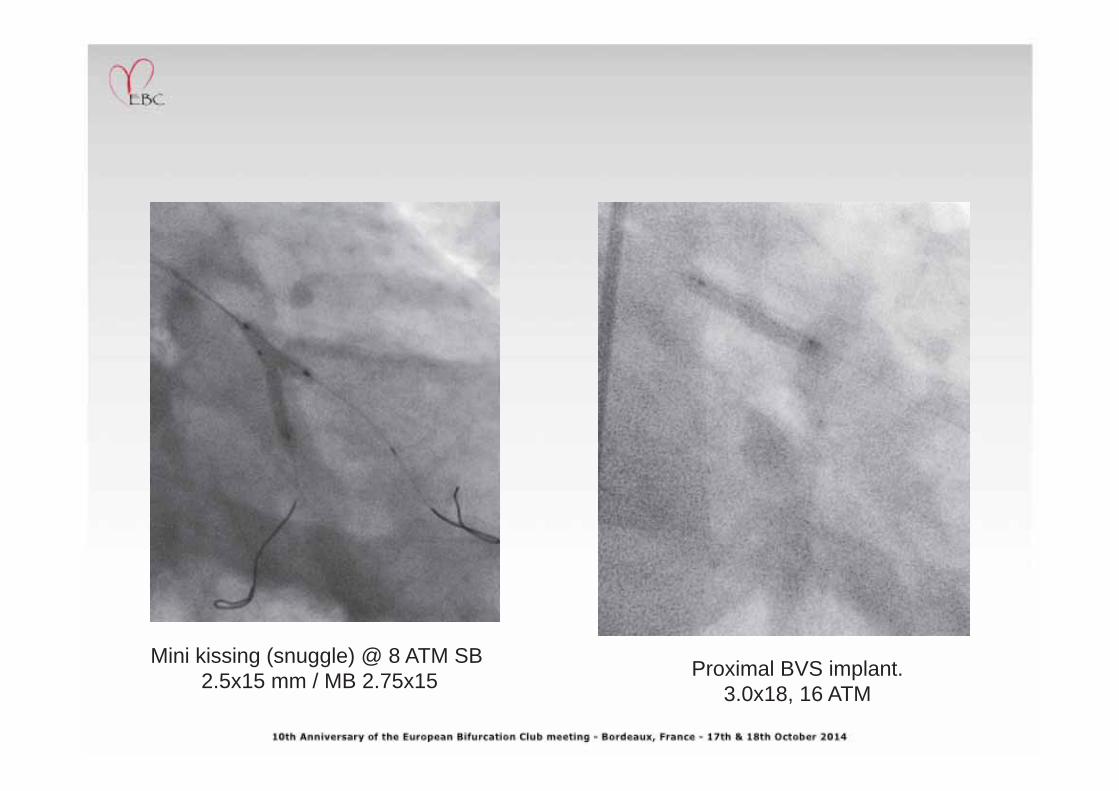
Proximal BVS implant. 3.0x18, 16 ATM
Mini kissing (snuggle) @ 8 ATM SB 2.5x15 mm / MB 2.75x15
Final result
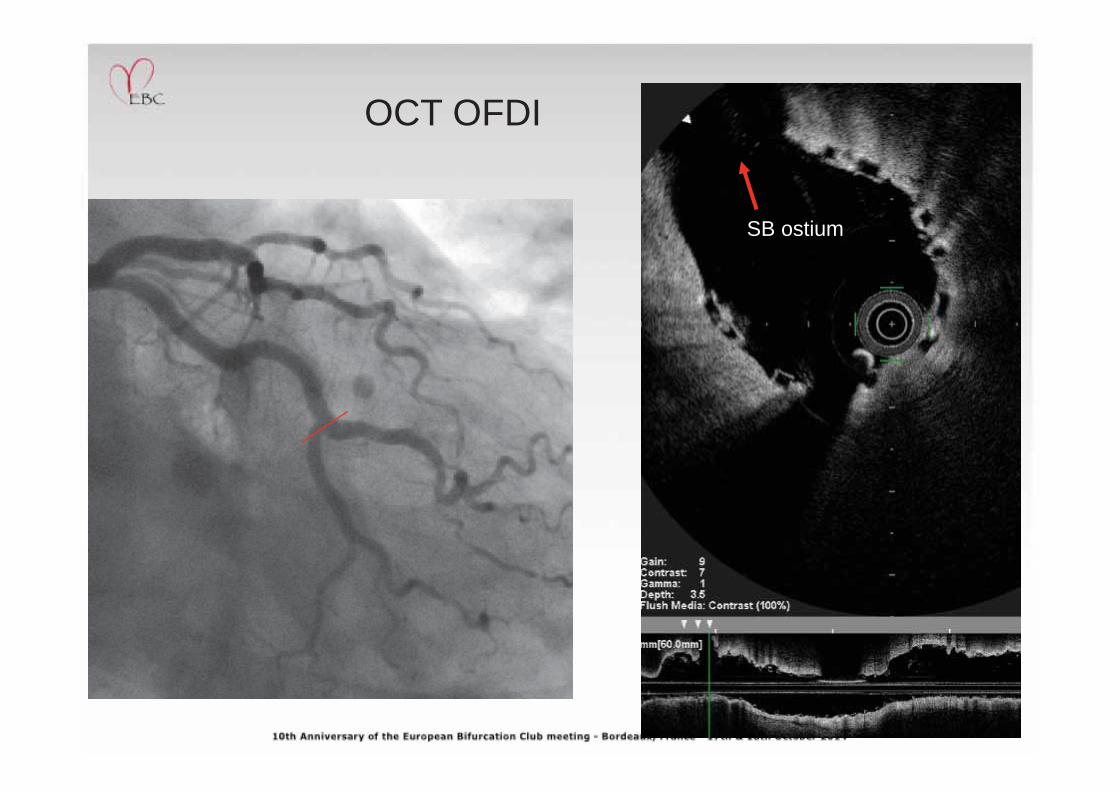
OCT OFDI
SB ostium
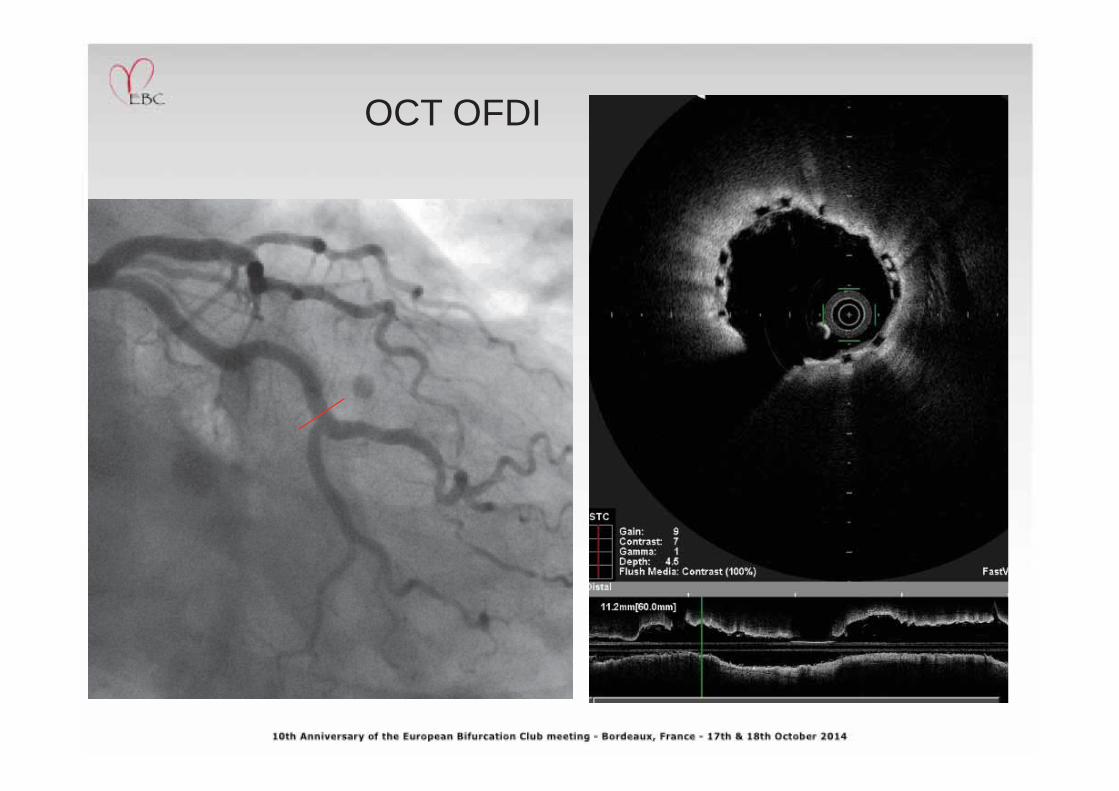
OCT OFDI
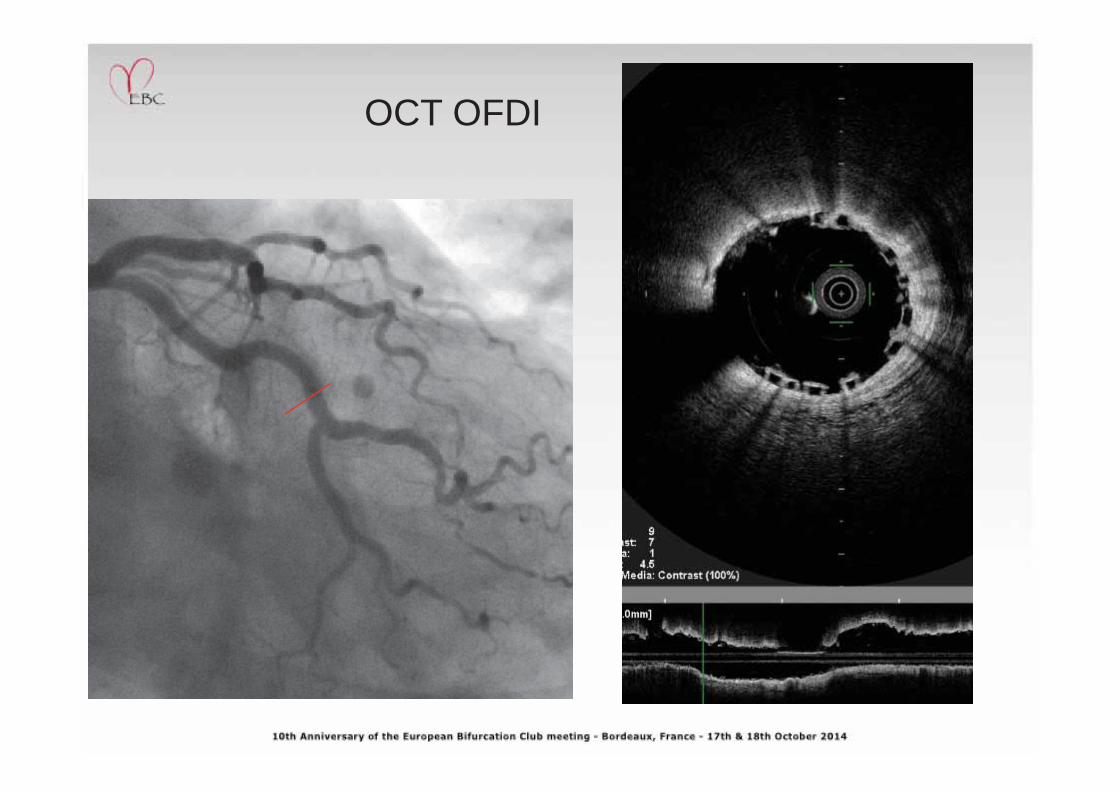
OCT OFDI
10-Month FU
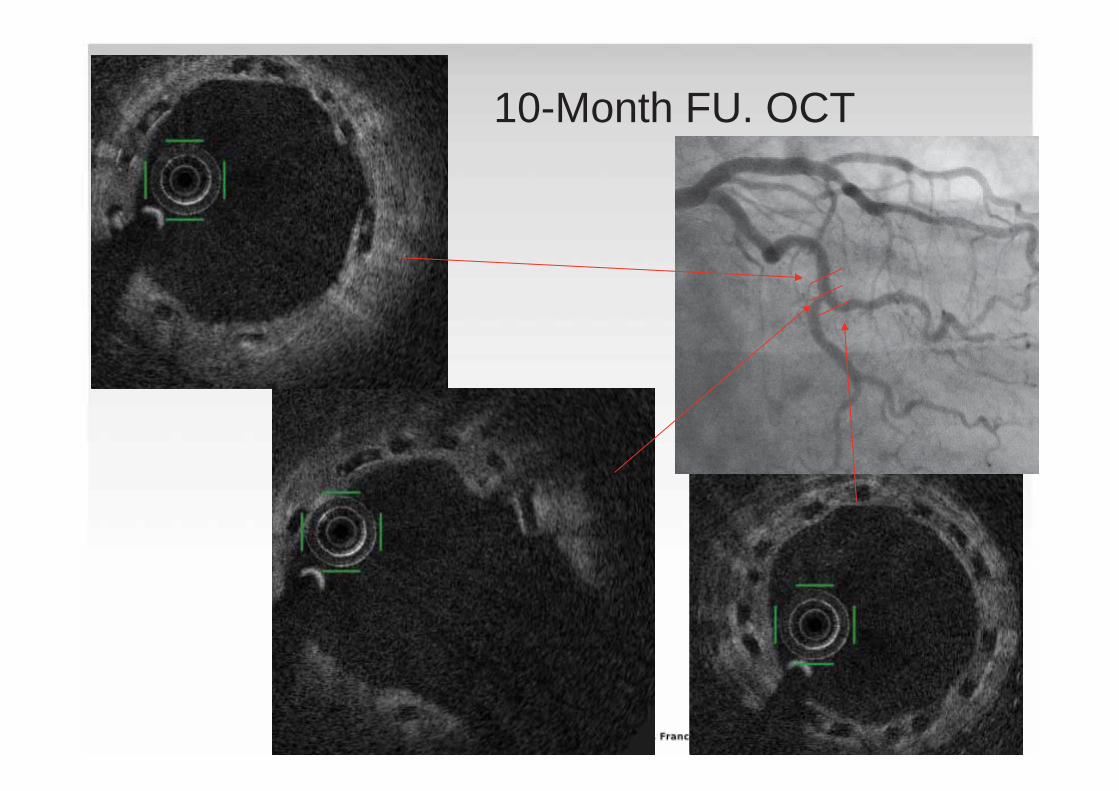
10-Month FU. OCT
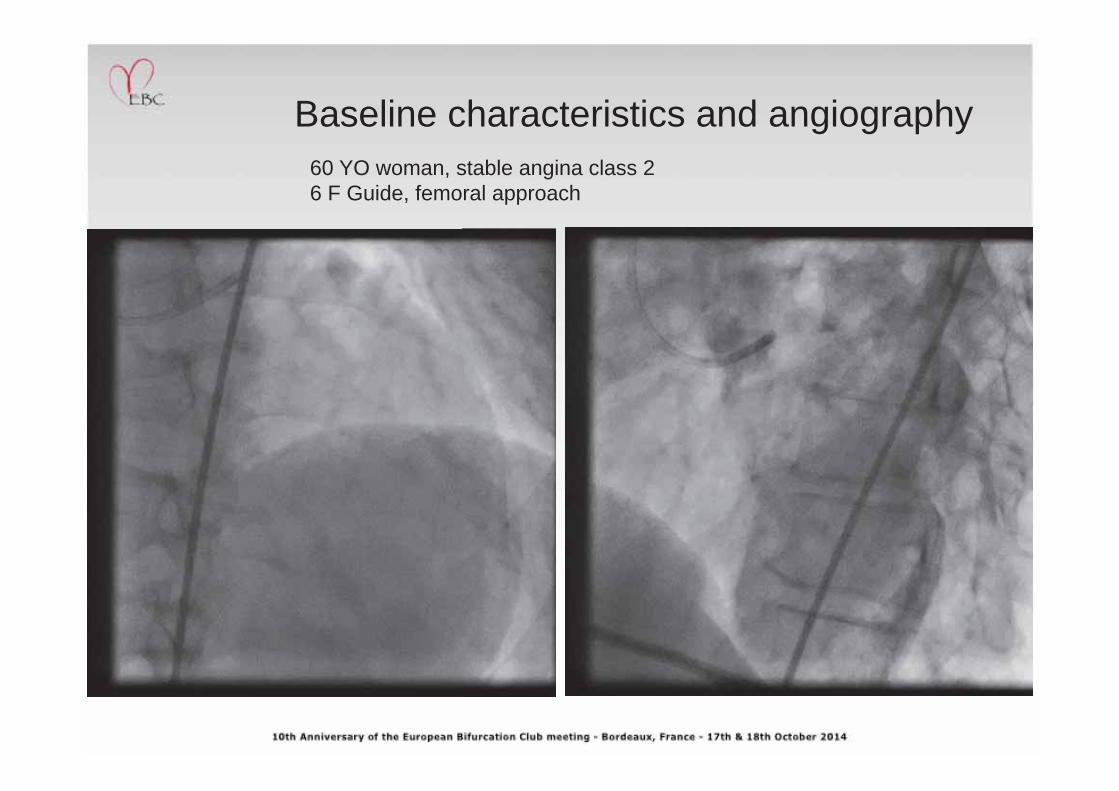
Baseline characteristics and angiography 60 YO woman, stable angina class 2 6 F Guide, femoral approach
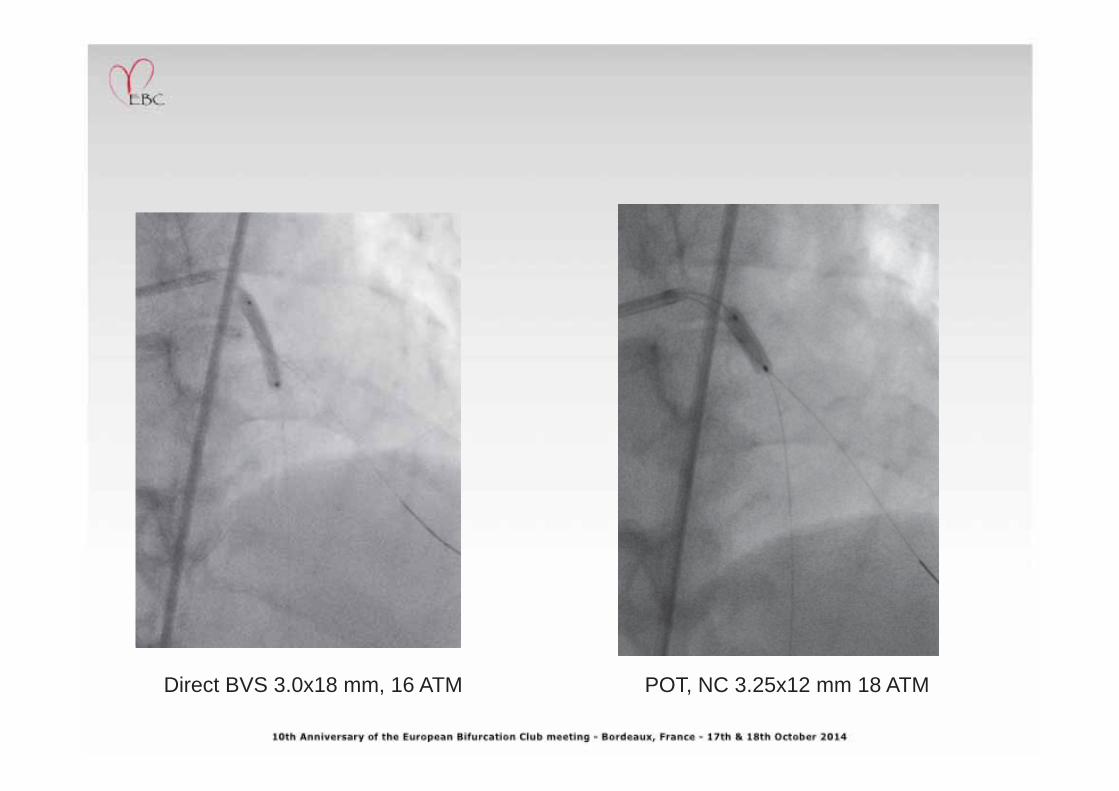
Direct BVS 3.0x18 mm, 16 ATM POT, NC 3.25x12 mm 18 ATM
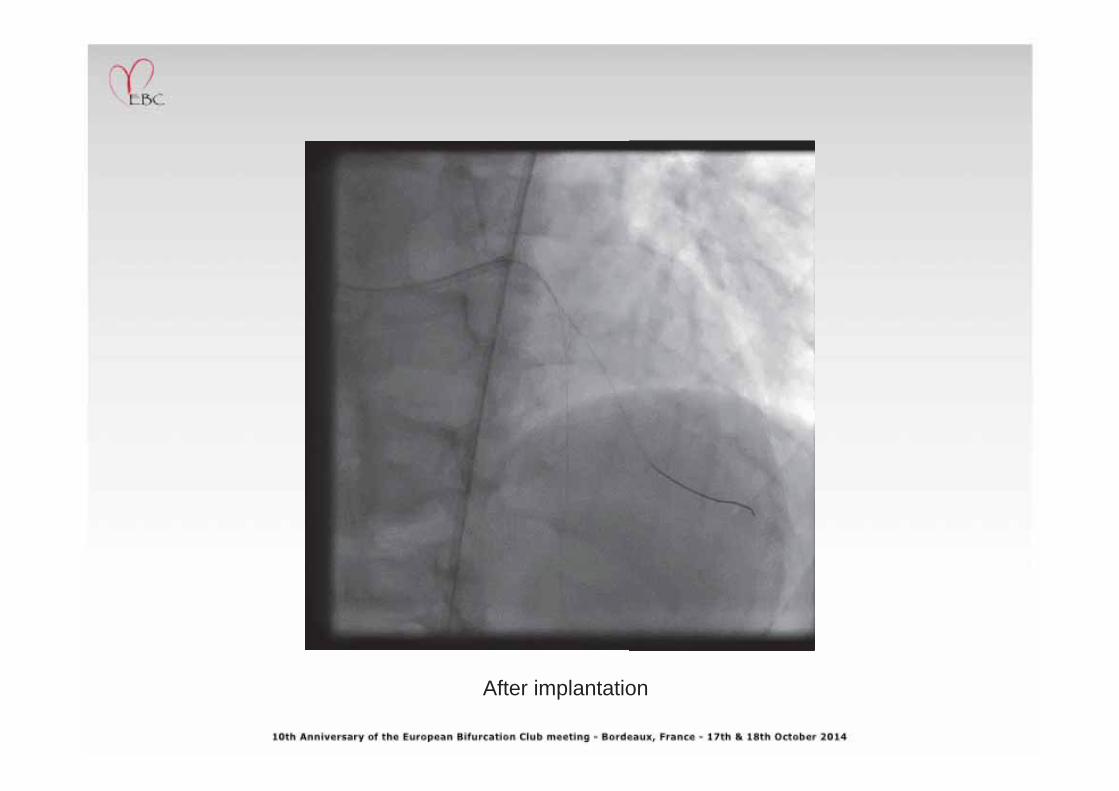
After implantation
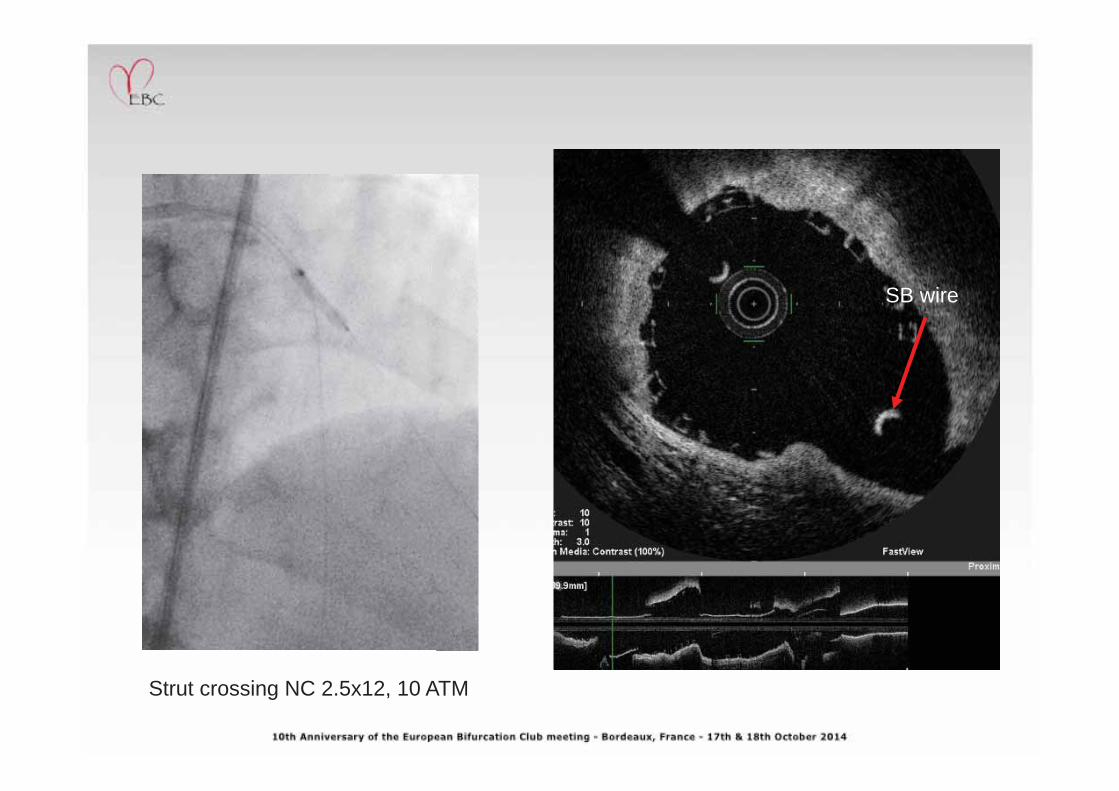
Strut crossing NC 2.5x12, 10 ATM
SB wire
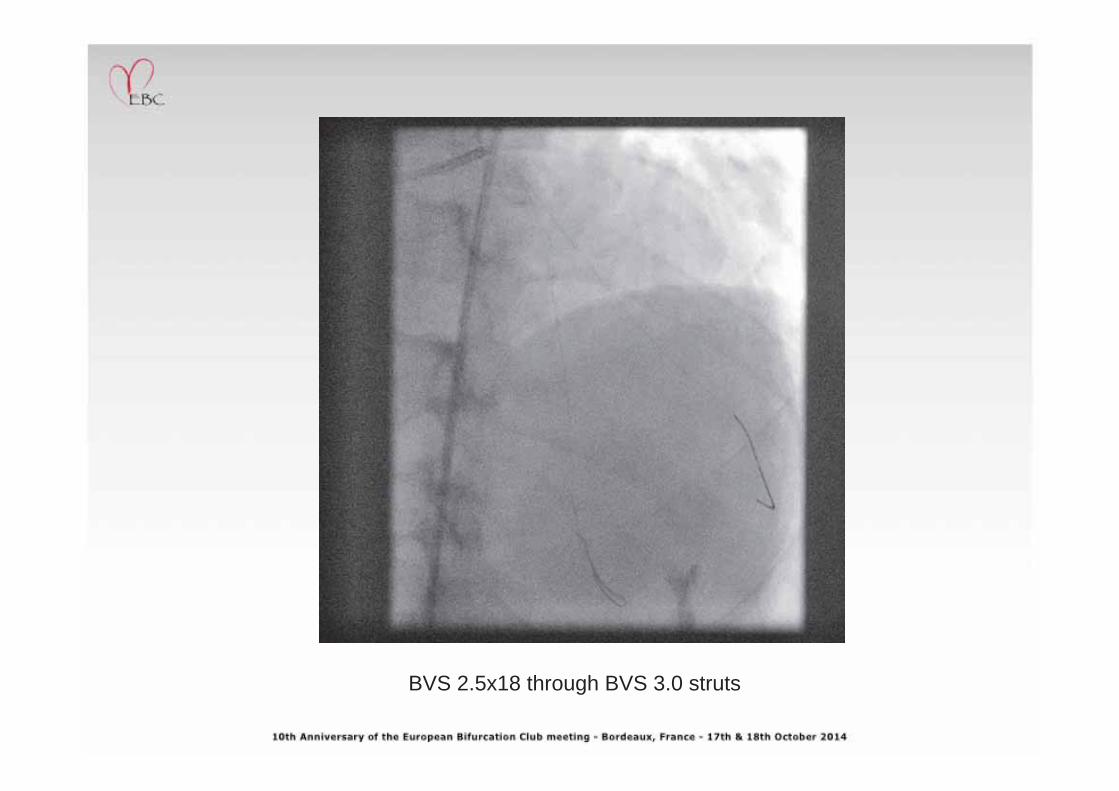
BVS 2.5x18 through BVS 3.0 struts
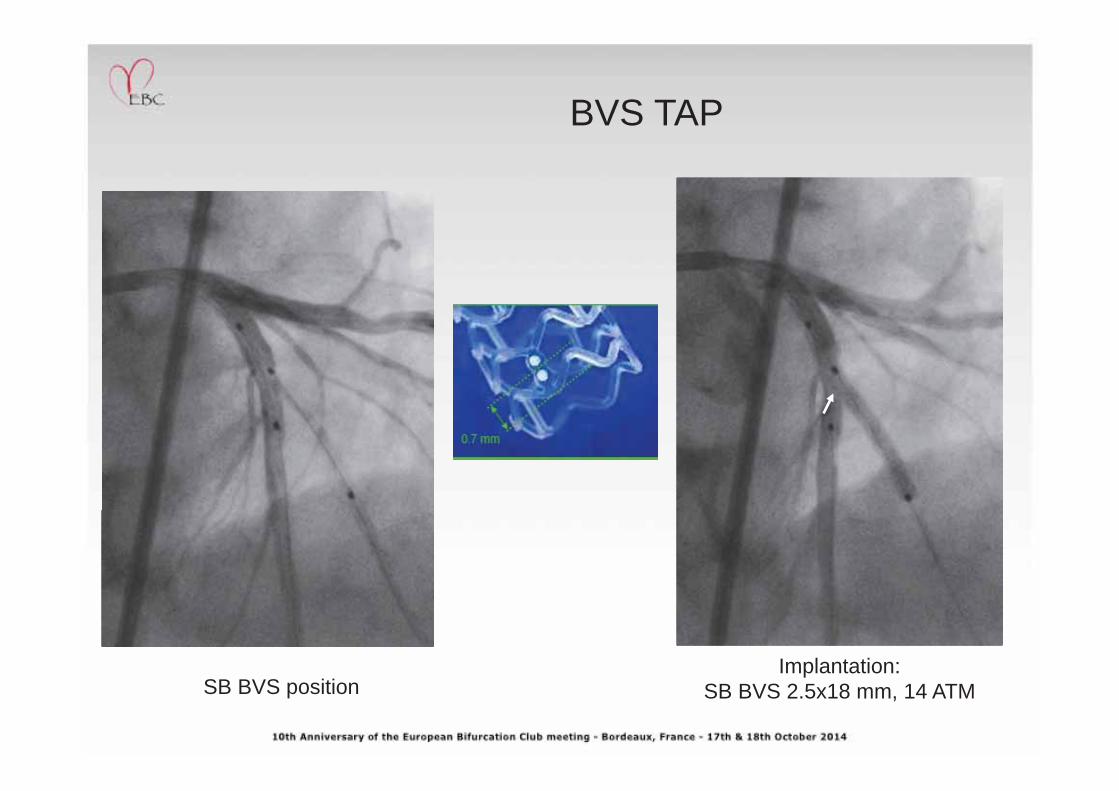
BVS TAP
SB BVS position Implantation:
SB BVS 2.5x18 mm, 14 ATM
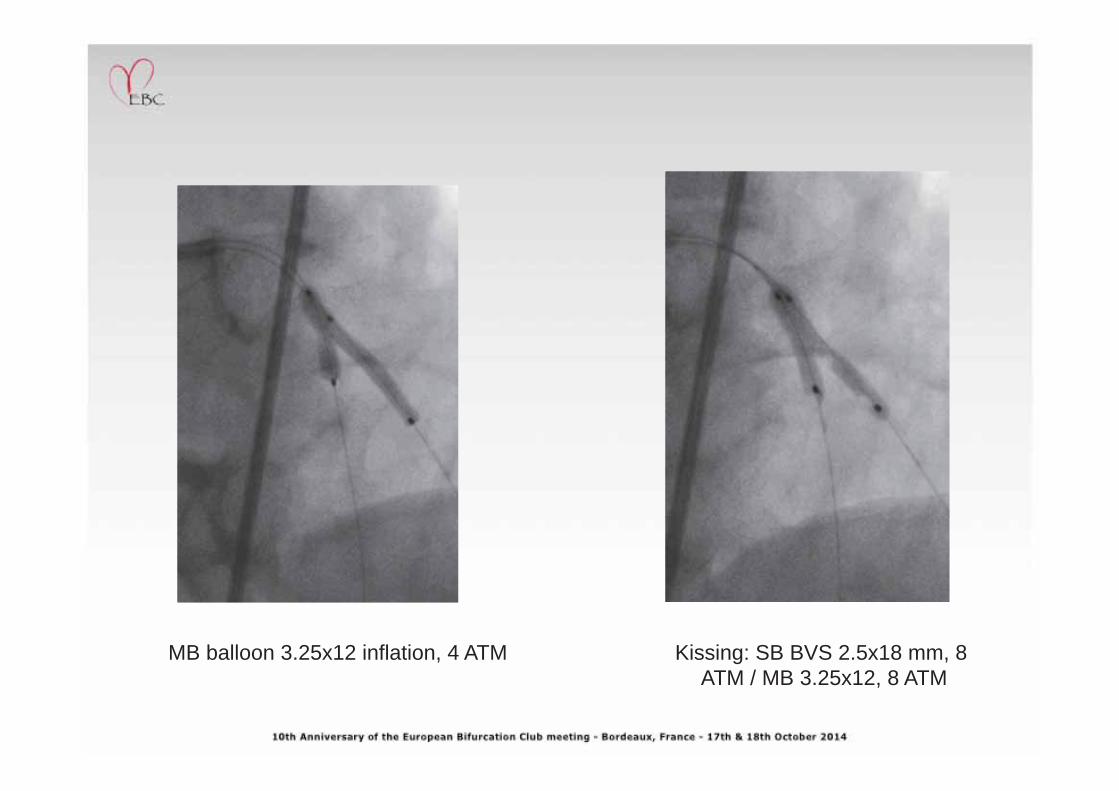
MB balloon 3.25x12 inflation, 4 ATM Kissing: SB BVS 2.5x18 mm, 8 ATM / MB 3.25x12, 8 ATM
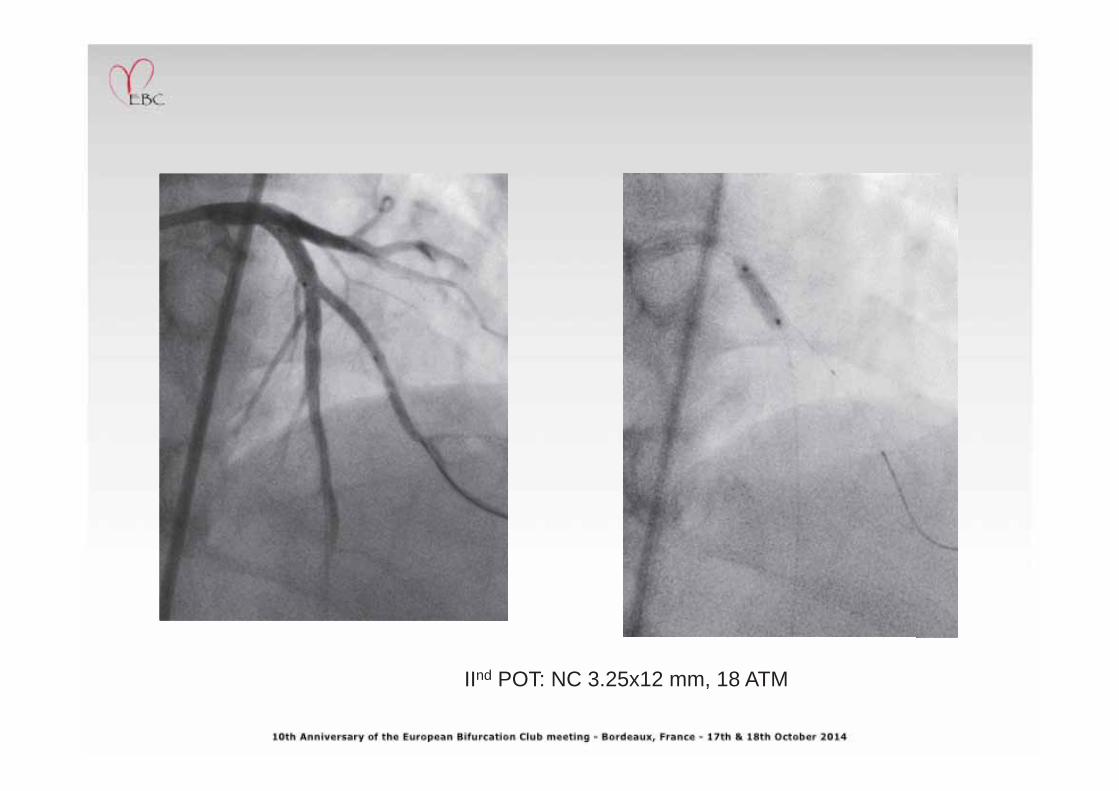
IInd POT: NC 3.25x12 mm, 18 ATM
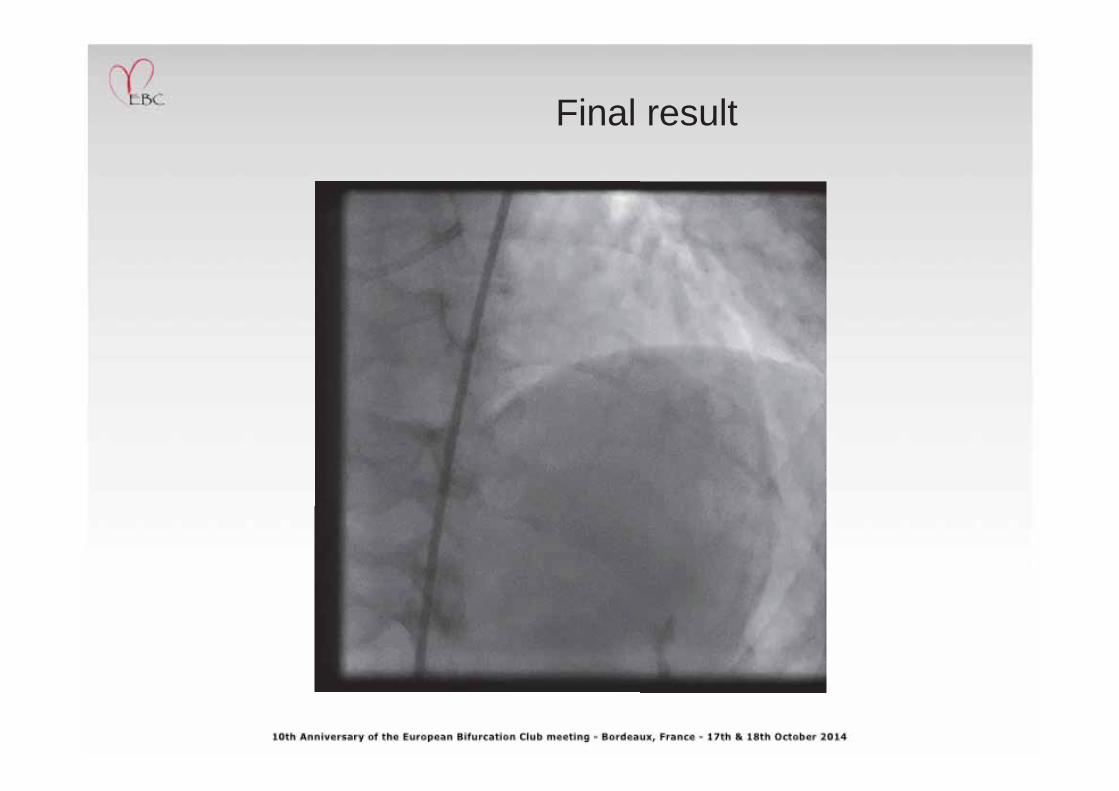
Final result
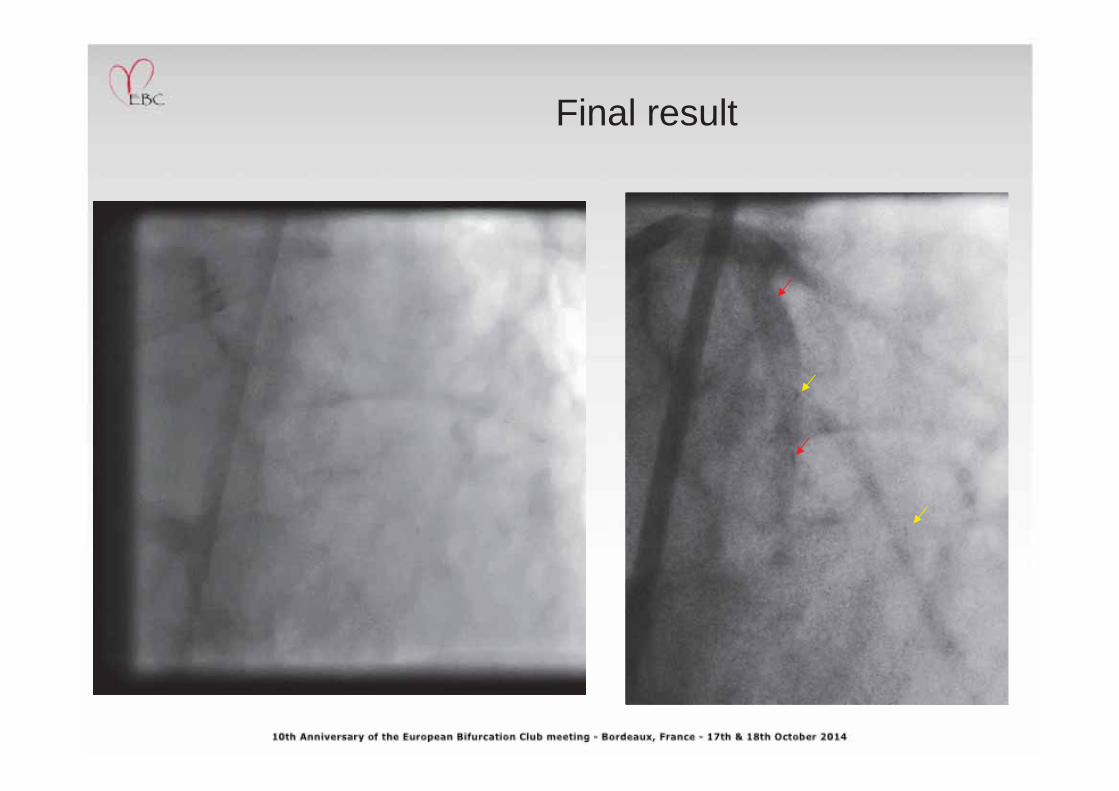
Final result
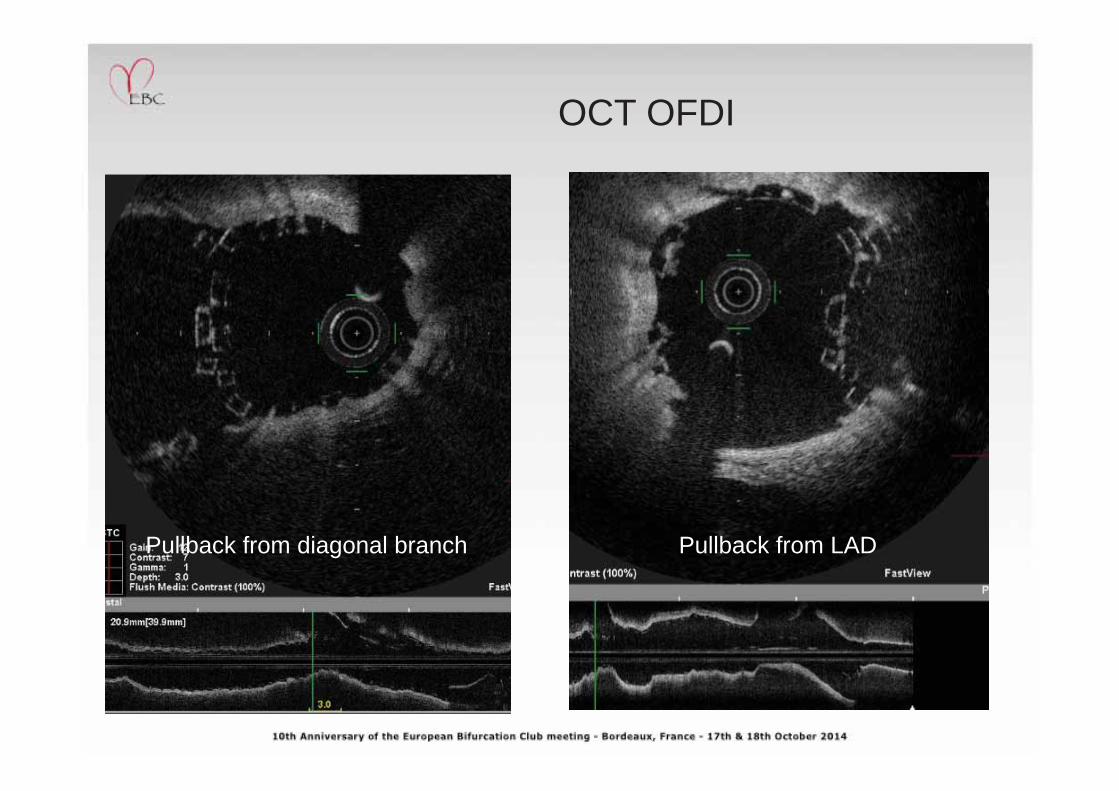
OCT OFDI
Pullback from diagonal branch Pullback from LAD
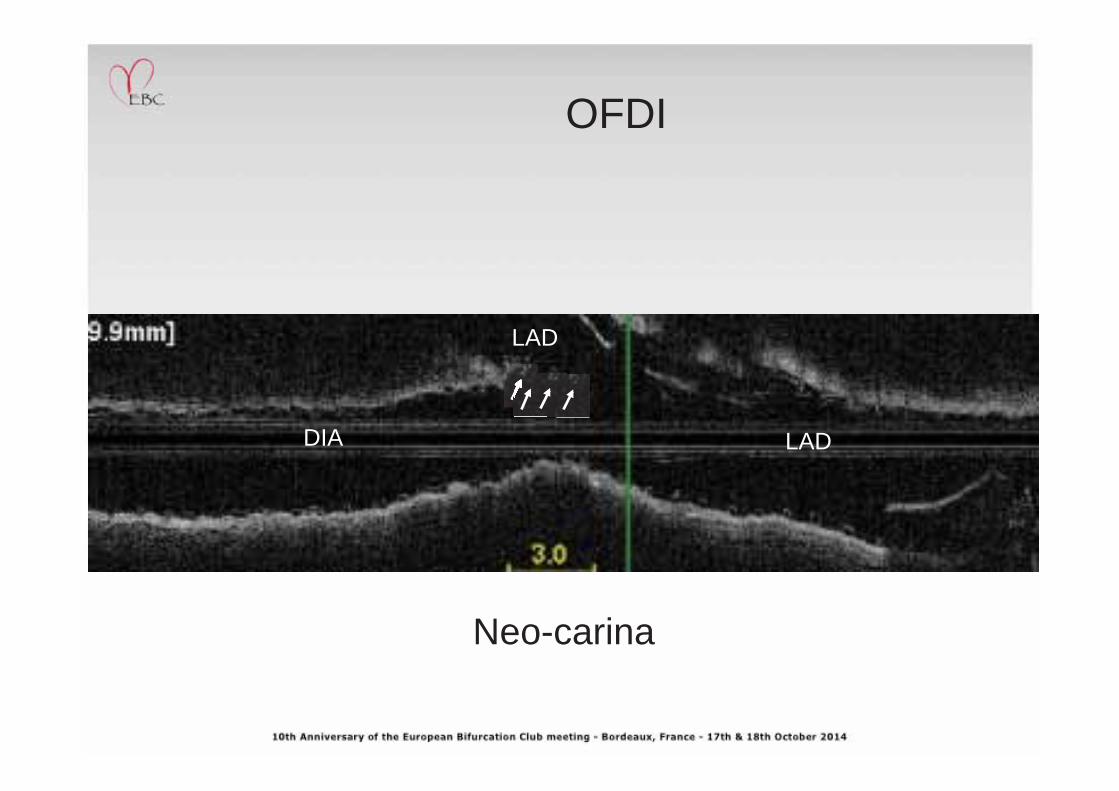
OFDI
Pullback from diagonal branch Pullback from LAD
DIA LAD
Neo-carina
LAD
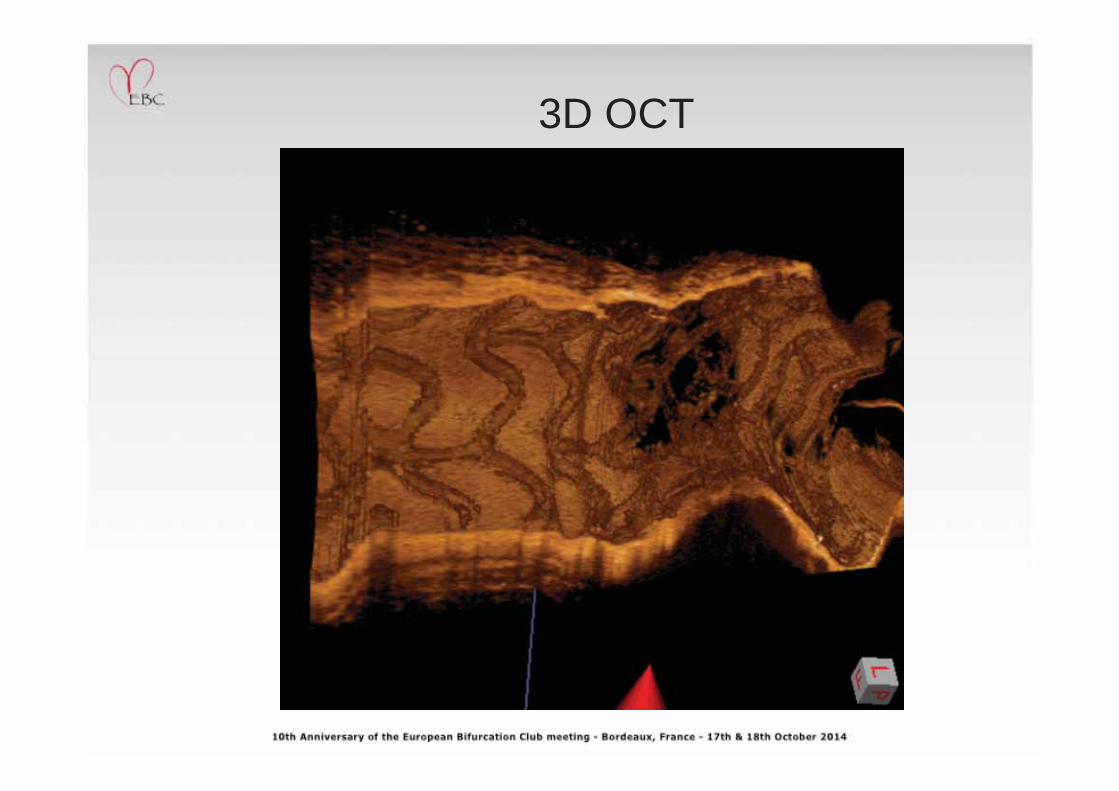
3D OCT
ANGIO FU after 6 months
Medina 0,0,1
61 YO woman, stable angina class 2, Hypertension, IDDM 6 F Guide, femoral approach
06 DEC 2013
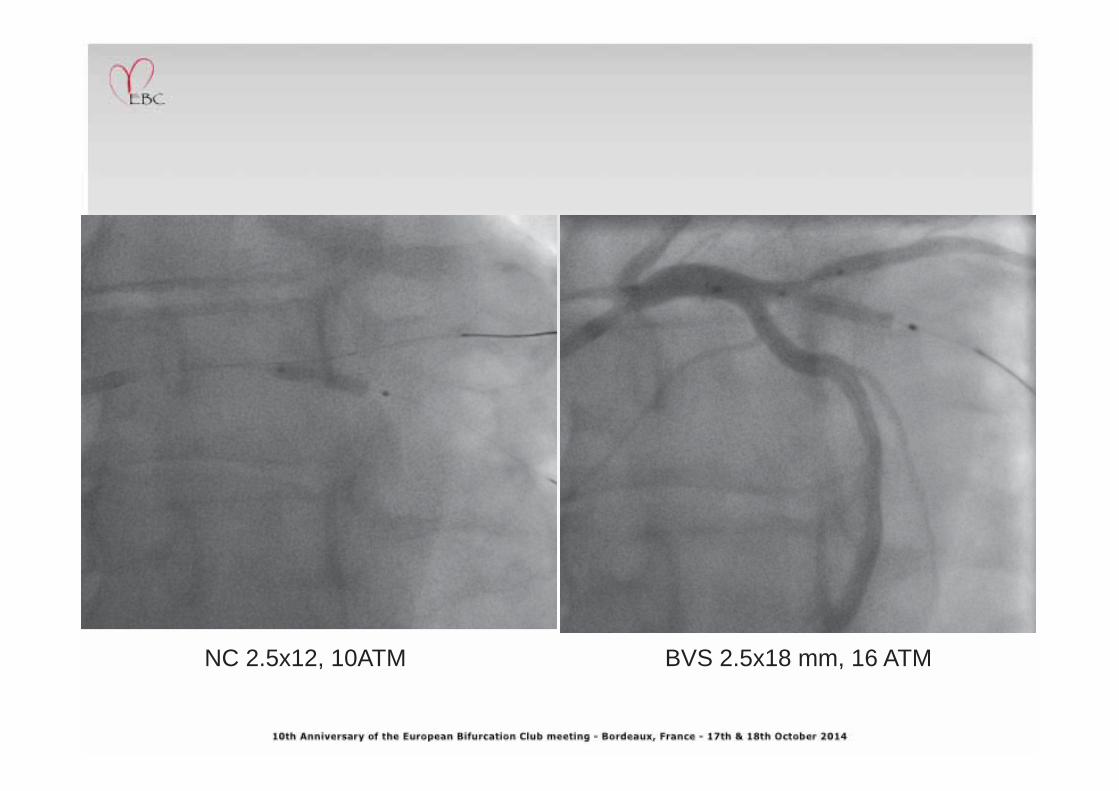
BVS 2.5x18 mm, 16 ATM NC 2.5x12, 10ATM
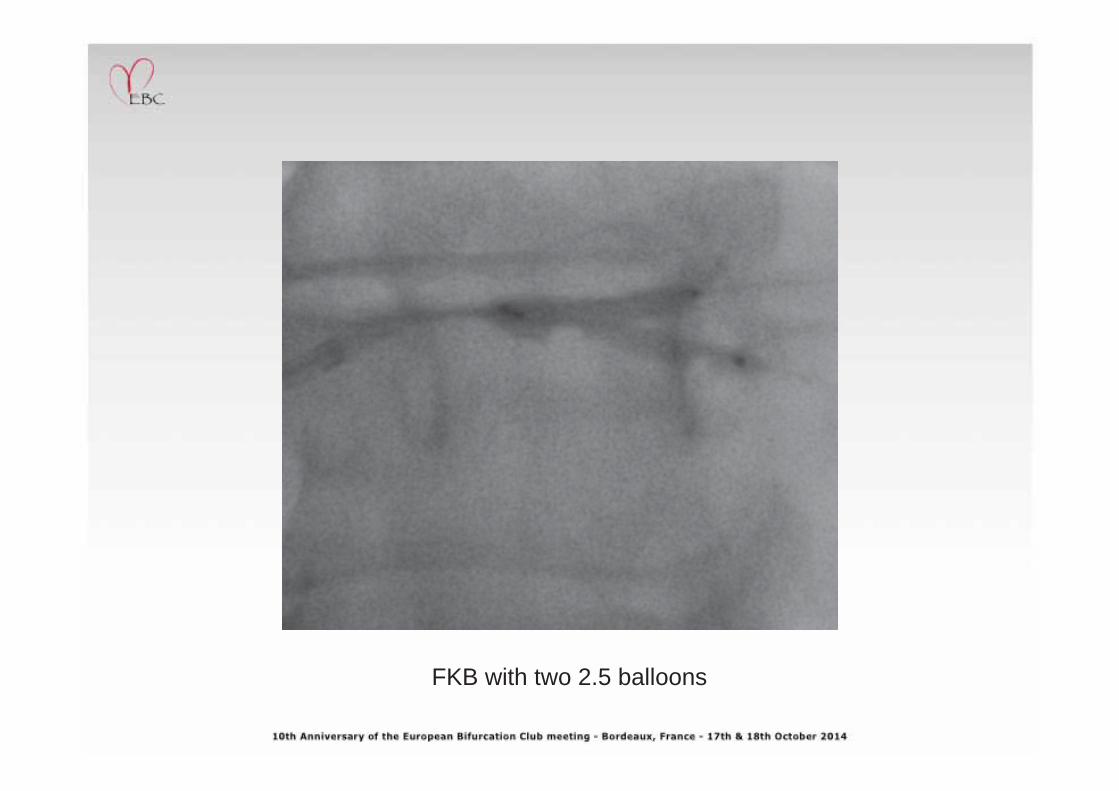
FKB with two 2.5 balloons
Final result
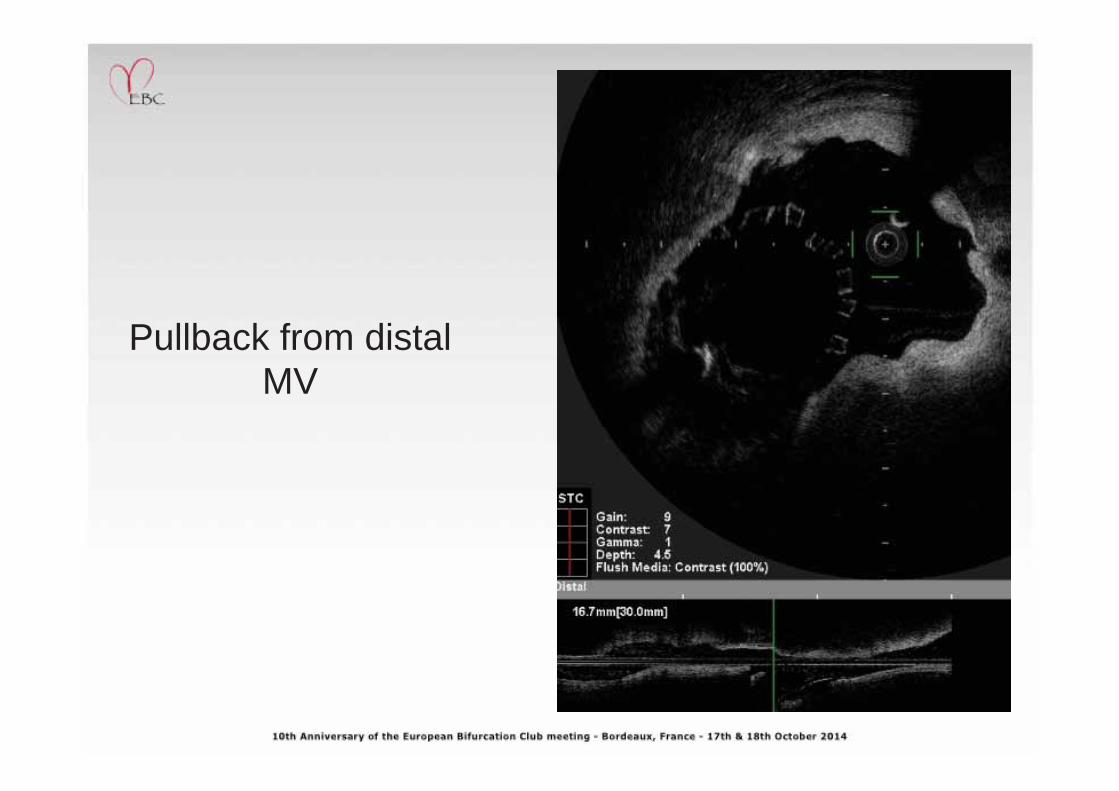
Pullback from distal MV
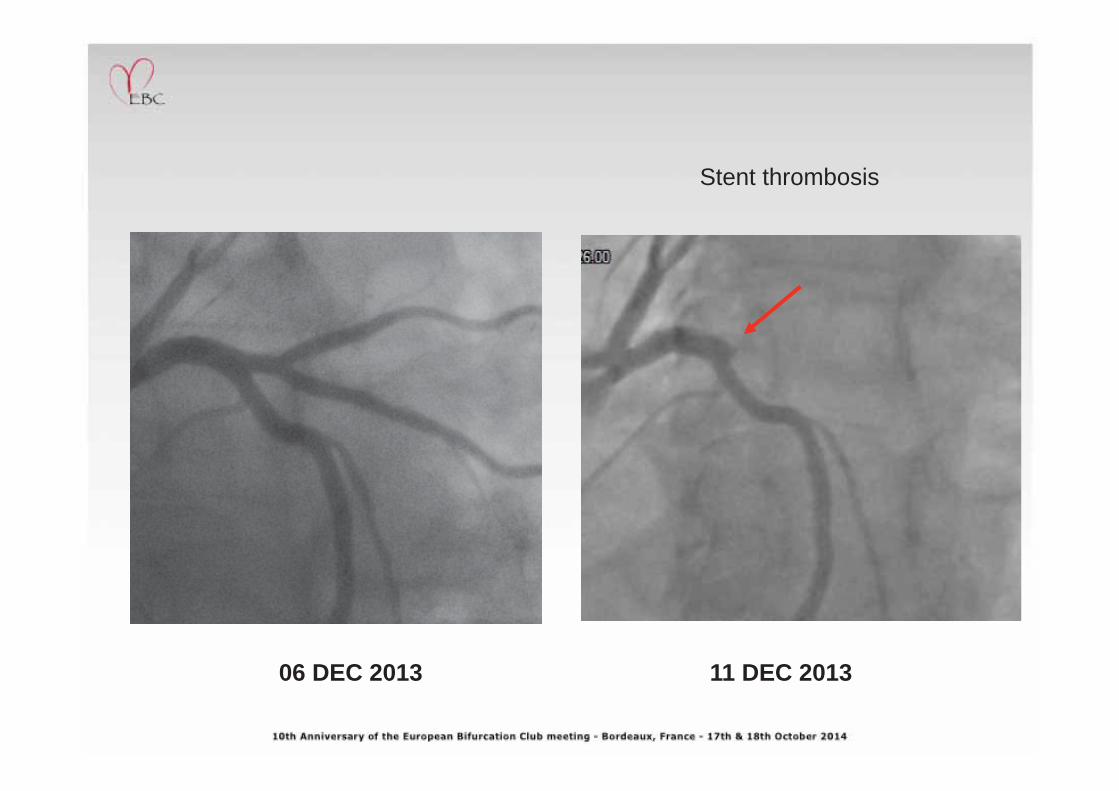
06 DEC 2013 11 DEC 2013
Stent thrombosis
BVS for bifurcations Conclusion
• Bifurcation stenting with BVS is feasible in most of the anatomical variants
• In-hospital results are satisfactory with very few complications
• Subacute stent thrombosis may be an issue. Platelet function testing or routine use of modern P2Y12 inhibitors (at least in the early months) is strongly recommended
Poznan





























![bS`TOQS - Berklee College of Music...87BB3@ 8WbbS` VOa [O\g QOcaSa Pcb bVS STTSQb Wa b] dO`g bVS bW[SPOaS ]` `SUcZO`Wbg ]T bVS QZ]QY ^cZaSa ^`]dWRSR b] bVS agabS[ BVS STTSQb ]T XWbbS`](https://img.pdfslide.us/doc/110x75/5e95cea8cf6e12611e2f56f7/bstoqs-berklee-college-of-music-87bb3-8wbbs-voa-og-qocasa-pcb-bvs-sttsqb.jpg)