Embed Size (px)
Citation preview

Ready to take a break from your board review question books? Bedtime Stories for Psychiatry Residents provides the perfect complement to board review question books and a structured reading program of up-to-date psychiatry references. This study guide contains 250 selected psychiatry topics with concise, bullet-format outlines with hundreds of high yield facts. Topics are organized in alphabetical order with key terms and phrases are in bold print to reinforce important concepts. Bedtime Stories for Psychiatry Residents: Psychiatry Board Review Topics A to Z Buy The Complete Version of This Book at Booklocker.com: http://www.booklocker.com/p/books/4958.html?s=pdf
BedtimeStories forPsychiatryResidents
Psychiatry Board Review Topics A to Z
Bascom K. Bradshaw, DO, MPH, MAS
READY TO TAKE A BREAK from your board reviewquestion books? Bedtime Stories for Psychiatry Residentsprovides the perfect complement to board review questionbooks and a structured reading program of up-to-datepsychiatry references.
• 250 selected psychiatry topics
• Concise, bullet-format outlines with hundreds of high yield facts
• Topics are organized in alphabetical order
• Key terms and phrases are in bold print to reinforce important concepts
g
g
Bedtim
e Stories for Psychiatry R
esidents: Psychiatry B
oard Review
Topics A
to ZB
ascom K
. Bradshaw
Cover image: © Cicamokus_Dreamstime.com
Copyright © 2010 Bascom K. Bradshaw
ISBN: 978-1-60910-468-9
All rights reserved, No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, recording or otherwise, without the prior written permission of the author.
Printed in the United States of America
Notice:
The author is not responsible for any injury resulting from material contained in this study guide. The information presented in this guide is not guaranteed for accuracy and should not be used for individual patient care. Every attempt has been made to present the most concise descriptions, statements and answers in this study guide as possible. Readers are encouraged to confirm the information contained in this study guide with other up-to-date sources; it is advised that readers check for updated information on the product information sheet included with drug packaging prior to administration to ensure recommended dosing and updated contraindications.
Please contact me by email at [email protected] if you note any discrepancies, so I can make immediate corrections in future editions.
The American Osteopathic Board of Neurology and Psychiatry and American Board of Psychiatry and Neurology do not endorse the material contained within this review book and are not responsible for questions answered incorrectly on board examinations.
Statements and views in this study guide are those of the author and do not reflect the policy or position of the United States Army or United States Air Force; the University of Texas Health Science Center at San Antonio (UTHSCSA); or San Antonio Uniformed Services Health Education Consortium (SAUSHEC).
Pizza Boy Publishing, Inc. 2010
3
A
Absence seizure initial treatment -Opinions vary about how to rank medications
-U.S. expert opinion, order of preference is ethosuximide, then valproic acid, and lamotrigine (Wheless et al. 2005)
-European expert opinion prefers to rank valproic acid first, followed by ethosuximide, and finally lamotrigine (Wheless et al. 2007)
-Cochrane Review reports that there is insufficient evidence to inform clinical practice (Posner et al. 2005)
-International League against Epilepsy (ILAE), noted a marked paucity of published data from adequately powered, seizure-type–specific studies (Glauser et al. 2006)
Absence vs. Partial complex seizures -abrupt ending of typical absence seizures, w/o postictal phase, is most useful clinical feature in distinguishing the 2 conditions
Partial Complex
-aura is often
-consciousness is impaired
-movements are usually simple, repetitive but may include complex activity
-postictal behavior; amnesia, confusion, and tendency to sleep
-frequency; 1-2 per week
-duration; 2-3 minutes
-precipitants; none identified
-EEG w/ spikes and polyspike and waves, usually over both temporal regions
Bedtime Stories for Psychiatry Residents
4
-AED tx; carbamazepine, phenytoin
Absence Seizure
-aura does NOT typically occur
-consciousness is lost at onset
-movements include blinking and facial and finger automatisms (duration dependent)
-NO postictal abnormality except amnesia for ictus
-frequency; several daily
-duration; 1-10 seconds
-precipitants; hyperventilation, photic stimulation
-EEG w/ generalize 3 Hz spike-and-wave complexes
-AED tx; ethosuxamide, valproate
Acculturation; risk for suicide, substance abuse, alcoholism -individuals who assume a new cultural identity consonant w/ that of the host culture
-individuals may be at higher risk for suicide, substance abuse, and alcoholism if he or she abandons native culture but does NOT incorporate behaviors and values of the host culture
Acute dystonia and haloperidol -occurs most commonly during the week after initiation of antipsychotics or following an abrupt and rapid dose increase (Ayd 1961; Barnes and Spence 2000; Remington and Kapur 1996)
-occurs most commonly in children and young adults, especially in males
-may appear as torticollis, trismus, tongue protrusion, pharyngeal constriction, laryngospasm, blepharospasm, oculogyric crisis, or abnormal contractions of any part of the body
-may complain of tongue thickening, throat tightening, and difficulty speaking or swallowing
Psychiatry Board Review Topics A to Z
5
-acute tx w/either anticholinergic agent or antihistamine is usually highly effective
-may need to be repeated at intervals if acute dystonia recurs before the dose of the anticholinergic is stabilized
-medications may need to be given parenterally if respiratory difficulty develops
Adoption studies, role of environment in behavioral genetics -based on knowledge that adoption separates 2 major influences, genes and rearing
-provides naturalistic setting w/ ideal separation of genetic factors from environmental influences
-4 types of adoption studies:
Adoptee study method
-study of adopted-away children of parent w/ disorder
Cross-fostering strategy
-study of children born of non-disordered parents adopted into family w/ disordered parent
Adoptees’ family method
-study of adoptive and biological relatives of disordered adoptees
Monozygotic twins reared apart
-study of monozygotic twins reared apart
-adoption studies have been carried out for schizophrenia, mood d/o, alcoholism, drug abuse, sociopathy, ADHD, other psychiatric conditions; IQ and personality variables
Aggressive behavior in preschool children; verbal inability -children behave aggressively for many reasons
-may NOT have anything to do w/ child rearing
Bedtime Stories for Psychiatry Residents
6
-young children do NOT have good language skills compared to older children
-children may act aggressively if he or she feels helpless and is unable to express feelings verbally
-children generally understand language better than they can use it; children should be spoken to in age-appropriate language about why it is important not to hit others
-role-playing may be helpful; child should be encouraged to use the language that he does have at his disposal to express his feelings to others
Akathisia, clinical features -subjective feeling of motor restlessness, compelling need to be in constant movement; may be seen as extrapyramidal adverse effect from antipsychotic use
-may be mistaken for psychotic agitation
-tx includes discontinuing medication causing akathisia; beta-adrenergic receptor antagonists (propanolol considered drug of choice), benzodiazepines, and clonidine
-trial of anticholinergics (cyproheptadine, benztropine) for tx neuroleptic-induced acute akathisia is reasonable
Alcohol intoxication and suicide risk assessment -patients under the influence of alcohol or other substances are at an increased risk of causing harm to themselves or others, often accidentally or impulsively
-should generally NOT be discharged from psychiatric emergency service into less restrictive setting unless he or she has attained clinical sobriety
-clinical sobriety is NOT to be equated w/ a particular blood concentration of intoxicant
-patient should be retained for additional observation; should focus on erratic behaviors
-duration of observation will be a function of pharmacokinetics of circulating drug
Psychiatry Board Review Topics A to Z
7
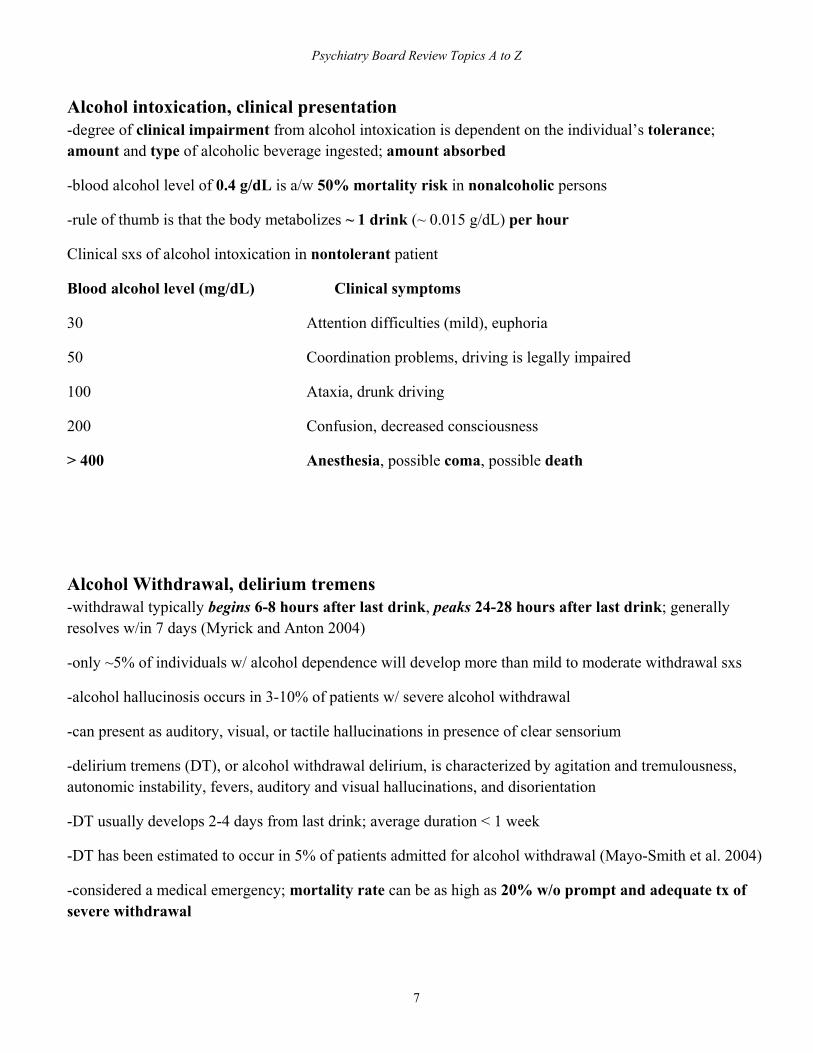
Alcohol intoxication, clinical presentation -degree of clinical impairment from alcohol intoxication is dependent on the individual’s tolerance; amount and type of alcoholic beverage ingested; amount absorbed
-blood alcohol level of 0.4 g/dL is a/w 50% mortality risk in nonalcoholic persons
-rule of thumb is that the body metabolizes ~ 1 drink (~ 0.015 g/dL) per hour
Clinical sxs of alcohol intoxication in nontolerant patient
Blood alcohol level (mg/dL) Clinical symptoms
30 Attention difficulties (mild), euphoria
50 Coordination problems, driving is legally impaired
100 Ataxia, drunk driving
200 Confusion, decreased consciousness
> 400 Anesthesia, possible coma, possible death
Alcohol Withdrawal, delirium tremens -withdrawal typically begins 6-8 hours after last drink, peaks 24-28 hours after last drink; generally resolves w/in 7 days (Myrick and Anton 2004)
-only ~5% of individuals w/ alcohol dependence will develop more than mild to moderate withdrawal sxs
-alcohol hallucinosis occurs in 3-10% of patients w/ severe alcohol withdrawal
-can present as auditory, visual, or tactile hallucinations in presence of clear sensorium
-delirium tremens (DT), or alcohol withdrawal delirium, is characterized by agitation and tremulousness, autonomic instability, fevers, auditory and visual hallucinations, and disorientation
-DT usually develops 2-4 days from last drink; average duration < 1 week
-DT has been estimated to occur in 5% of patients admitted for alcohol withdrawal (Mayo-Smith et al. 2004)
-considered a medical emergency; mortality rate can be as high as 20% w/o prompt and adequate tx of severe withdrawal
Bedtime Stories for Psychiatry Residents
8
-seizures are estimated to occur in 5-15% of patients; usually occur in first 24 hours from last drink, but can occur any time in first 5 days
-alcohol withdrawal seizures are usually grand mal in type
-past hx of alcohol withdrawal seizures are at increased risk for seizures in subsequent episodes of alcohol withdrawal
Alcohol-induced “blackout” -anterograde amnesia for events of any part of drinking episode w/o loss of consciousness; unable to make new long term memories, but still able to retrieve the memories established before alcohol consumption
-characterized by memory impairment during intoxication in relative absence of other skill deficits
-NOT to be confused w/ “passing out”
-may be complete (en-bloc) or partial (fragmentary, or grayout)
-en bloc blackout is complete amnesia for significant events otherwise memorable under usual circumstances; defining characteristic is permanent memory loss for period and cannot be recalled under any circumstances
-fragmentary blackouts occur more frequently; recall is usually possible and can be aided by cueing
-no longer considered as a signal of irreversible alcoholism
Alcohol-Induced Amnestic Disorder, Korsakoff’s syndrome -essential feature of alcohol-induced persisting amnestic d/o is disturbance in short-term memory caused by prolonged heavy use of alcohol
-rare in persons younger than age 35
-also described as Wernicke-Korsakoff Syndrome (a set of acute sxs) and Korsakoff’s syndrome (chronic condition)
Wernicke’s encephalopathy
Psychiatry Board Review Topics A to Z
9
-completely reversible w/ tx; only ~ 20% of patients w/Korsakoff’s syndrome recover
-pathophysiological connection b/w 2 syndromes is thiamine deficiency, caused either by poor nutritional habits or by malabsorption problems
-thiamine is a cofactor for several important enzymes; may be involved in conduction of axon potential along axon and in synaptic transmission
-neuropathological lesions are symmetrical and paraventricular, involving mammillary bodies, thalamus, hypothalamus, midbrain, pons, medulla, fornix, and cerebellum
-tx in early stages of Wernicke’s encephalopathy responds rapidly to large doses of parenteral thiamine; believed to be effective in preventing progression into Korsakoff’s syndrome; dosage of thiamine is usually initiated at 100 mg by mouth 2-3 times daily and is continued for 1 to 2 weeks
-in patients w/ alcohol-related disorders who are receiving IV glucose solution, it is good practice to include 100 mg of thiamine in each liter of the glucose solution
Korsakoff’s syndrome
-chronic amnestic syndrome that can follow Wernicke’s encephalopathy
-cardinal features are impaired mental syndrome (especially recent memory) and anterograde amnesia in an alert and responsive patient; may or may not have confabulation
-tx of Korsakoff’s syndrome is also thiamine given 100 mg by mouth 2-3 times daily; should continue for 3-12 months; few patients ever fully recover, although many have some improvement in cognitive abilities w/ thiamine and nutritional support
-Korsakoff’s syndrome can occur in other malnourished conditions, such as marasmus, gastric carcinoma, and HIV
Alexia w/ agraphia; embolic stroke, left angular gyrus -alexia w/ agraphia is also known as angular gyrus syndrome and central alexia
-considered acquired illiteracy; patients lose previously acquired reading and writing skills
-most lose spelling and ability to understand words spelled to them
-many patients have fluent, paraphasic speech, unlike preserved speech of pure alexia w/o agraphia
-auditory comprehension is much superior to reading comprehension
Bedtime Stories for Psychiatry Residents
10
-lesion usually involves angular gyrus area in LEFT inferior parietal lobule
-syndrome was described by Dejerine
-closely related to pure alexia w/ agraphia syndrome, Gerstmann syndrome; Gerstmann brought together 4 deficits of agraphia, acalculia, right-left confusion, and finger agnosia and associated them w/ lesions of dominant parietal lobe; alexia was not originally a cardinal feature of Gerstmann syndrome but is often associated
-modern authors (Benton) have questioned validity of Gerstmann syndrome
-some patients may have one or more deficits w/o the others; stimulation studies in epileptic patients have reproduced combinations of these deficits w/ stimulation in angular gyrus area, confirming association of key elements of Gerstmann syndrome
Alzheimer Disease, early onset -some forms of familial early-onset Alzheimer dz can appear as early as third decade; represents a subgroup of < 10% of all familial cases of Alzheimer dz
-familial forms of Alzheimer dz account for < 7% of all cases of Alzheimer dz; most cases are sporadic (not inherited)
-mutations in genes coding for 3 proteins unequivocally cause Alzheimer dz:
amyloid precursor protein (APP, on chromosome 21)
presenilin I (on chromosome 14)
presenilin II (on chromosome 1)
-all lead to a relative excess in production of stickier 42-amino acid form of beta-amyloid peptide over less sticky 40-amino acid form
Alzheimer’s Disease, dementia -most common cause of dementia in patients over age 65
-definite dx requires histologic examination of brain tissue
Psychiatry Board Review Topics A to Z
11
-probable, or clinical, dx includes: insidious onset of a progressively worsening dementia; clinical and laboratory evaluations that exclude alternative neurologic and systemic illness
-above clinical criteria yields an antemortem diagnostic accuracy of almost 90%; would be more reliable by excluding those w/ EPS and frontal lobe dysfunction
Amantadine, treatment of antipsychotic side effects, Parkinsonism -FDA-approved for tx of neuroleptic-induced Parkinsonism (NIP) and Parkinson’s dz, as well as tx and prophylaxis of influenza A respiratory illness; NOT effective in tx of akathisia
-dosages of 100-300 mg/day are used for tx of NIP, and plasma concentrations may have some correlation w/ improvement
-water-soluble tricyclic amine; binds to M2 protein, membrane protein that functions as an ion channel on influenza A virus
-activity in reducing EPS is not known; shown to be active at glutamate receptors
-slowly and well absorbed from GI tract, w/ unchanged oral bioavailability over dose range of 50-300mg
-reaches steady state in 4-7 days; plasma concentrations (0.12-1.12 g/mL) may have some correlation w/ improvement in EPS
-relatively constant blood levels and long duration of action; excreted unchanged by kidneys
-half-life for elimination is ~16 hrs; prolonged in elderly patients and in impaired renal function
-has no anticholinergic activity in animal tests, only 1/209,000th as potent as atropine
-appears to cause release of dopamine and other catecholamines from intraneuronal storage sites in amphetamine-like mechanism; also shown to have activity at glutamate receptors, which may contribute to its antiparkinsonian effect
-no reported interactions b/w amantadine and other drugs

Bedtime Stories for Psychiatry Residents
12
Anosognosia -failure to recognize a deficit or dz
-most common example is ignoring a left hemiparesis because of a right cerebral infarction
-another example is denial of blindness from occipital lobe infarction (Anton’s syndrome)
Antipsychotic use in elderly -increasingly used in geriatric patients, particularly dementia given difference in prevalence rates; prevalence of schizophrenia remains < 1%, prevalence of dementia is ~2-5% for people > 60 yrs, increases to 15-40% for > 85 yrs
-not FDA-approved for tx of psychosis or behavioral dyscontrol in dementia
-drug interactions need to be considered in elderly patients
-age-related decreases in gut motility and anticholinergic effects of antipsychotics may decrease absorption rates
-antipsychotic drugs undergo biotransformation primarily in the liver, w/ GI tract, lungs, and kidneys being secondary sites; antipsychotics have slightly longer half-lives in elderly; drugs take longer to reach therapeutic blood levels and longer to leave the system
-dopamine neurons degenerate w/ aging, particularly after 70 yrs, decrease in number of available dopaminergic receptors reduces tolerance of elderly patients to antipsychotics, thereby increasing likelihood of neurological side effects, including EPS and TD
-more sensitive to side effects, sedation, cardiac effects (e.g., tachycardia, orthostatic hypotension), anticholinergic side effects (e.g., dry mouth, blurred vision, constipation, urinary retention), NMS w/ hyperpyrexia, autonomic instability and tachycardia, pigmentary retinopathy, weight gain and associated metabolic changes, allergic reactions, and seizures
-chlorpromazine and thioridazine and atypical antipsychotics clozapine, risperidone, olanzapine, and quetiapine antipsychotics most likely to cause orthostatic hypotension
-a/w increased risk of sudden cardiac death; thioridazine appears to carry highest risk of sudden unexplained death; risperidone prolongs QTc interval but has no effect on QT dispersion

Psychiatry Board Review Topics A to Z
13
Antiretroviral drugs, hepatotoxicity -antiretroviral related liver injury (ARLI) is a common cause of morbidity, mortality and tx discontinuation in HIV-infected patients
-every licensed antiretroviral medication has been a/w liver enzyme elevations; some may cause liver injury more frequently than others
-several major mechanisms of ARLI include metabolic host mediated injury, hypersensitivity reactions, mitochondrial toxicity and immune phenomena
Antisocial Personality Disorder, alcohol abuse and dependence -epidemiologic studies, association b/w ASPD and alcohol abuse and dependence
-Epidemiologic Catchment Area Survey, individuals meeting DSM criteria for ASPD were 21 times more likely to develop alcohol abuse and dependence at some point during their lives
-study found that people w/ ASPD before developing drinking problems consumed significantly more drinks per day; experienced significantly more alcohol-related problems compared w/ people who did not meet criteria for ASPD
Anxiety Disorder, differential diagnosis -organic causes must be considered first w/ any acute change in mental status or sudden-onset change in behavior in a previously well individual
-especially when signs and sxs overlap w/ life-threatening condition and when psychiatric syndrome being considered occurs outside of usual age window of presentation
-initial presentation w/ dyspnea, tachycardia, diaphoresis, chest pain, and light-headedness should receive thorough medical evaluation before being assigned dx of panic d/o
-should r/o unstable angina and MI, hypoglycemia, anemia, pulmonary embolism, asthma, obstructive pulmonary dz, GERD, irritable bowel dz, hyperparathyroidism, hyperthyroidism, pheochromocytoma, Huntington’s dz, Parkinson’s dz, seizure d/o, and autoimmune disorders, such as systemic lupus erythematosus
Bedtime Stories for Psychiatry Residents
14
-use of benzodiazepine may be helpful to make patient more comfortable, but care should be taken not to mask sxs of more serious underlying condition
Aphasia -disorder of verbal or written language rather than simply speech production
-almost always results results from discrete lesions in the dominant cerebral hemisphere’s perisylvian language arc
-aspects of aphasia may occasionally result from Alzheimer’s dz and degenerative conditions
Apraxia -loss of the ability to execute or carry out learned purposeful movements, despite having the physical ability and motivation to perform the movements
-it is a disorder of motor planning which may be acquired or developmental
-NOT caused by incoordination, sensory loss, or failure to comprehend simple commands
-types include: ideomotor, ideational, verbal, constructional, oculomotor, limb kinetic
Asperger Disorder, clinical description -in distinction from autistic d/o, “clinically significant general delay in language” and “cognitive delay” are exclusionary criteria
-significant impairments in social interaction and restricted and repetitive interests and behaviors are hallmarks
-unusual communication is common; often characterized by pedantic speech, intense preoccupations, and poor or nonexistent nonverbal communication
-it is commonly held that individuals w/ Asperger’s d/o are clumsy
Psychiatry Board Review Topics A to Z
15
Aspirin and Vascular dementia -observational data suggest low-dose aspirin may be a/w reduced risk of cognitive decline and dementia
-mechanism w/ Alzheimer’s dz is uncertain
-low-dose aspirin reduces risk of stroke and this probably reduces risk of cognitive decline secondarily
-prospective randomized trials are needed to confirm whether aspirin can prevent cognitive decline
Astasia abasia -inability to stand or walk in a normal manner
-normal leg movements can be performed in a sitting or lying down position
Astereognosis -a variety of cortical sensory loss
-inability to identify objects by touch
-seen w/ lesions of the contralateral parietal lobe
Athetosis -involuntary movement disorder
-usually results from basal ganglia damage from perinatal jaundice, anoxia, or prematurity
-characterized by slow writhing, sinuous movement of the arms or legs
-more pronounced in the distal part of the limbs
Bedtime Stories for Psychiatry Residents
16
Atomoxetine, adolescents with ADHD and substance use disorder -adolescents presenting for substance use disorder (SUD) tx have increased rates of ADHD, ranging from 30-50%
-co-occurring ADHD is a/w more severe substance use and worse substance use d/o outcomes
-atomoxetine is typically used to tx ADHD in adolescents w/ substance use d/o because of its limited abuse potential
Attention-Deficit Hyperactivity Disorder, comorbidity -individuals w/ADHD have poorer academic performance and higher rates of Learning Disorders than other children
-inattentive subtype may have more anxiety and somatic complaints than those w/combined or hyperactive–impulsive type; they have higher rates of Learning Disorders as well
Attention-Deficit Hyperactivity Disorder, comorbid depression -comorbid conditions should be considered simultaneously; better understand sxs and optimal tx
-depressed patients demonstrate diminished concentration; w/ bipolar d/o often manifest psychomotor agitation and distractibility; may be difficult to differentiate sxs from cardinal sxs of ADHD
-long-term follow-up studies have demonstrated that individuals w/ ADHD and comorbid disorders have poorer prognoses and greater hospitalization rates than ADHD alone; ADHD and/or comorbid condition often persists for several years
-overlap b/w depression and ADHD is well recognized; children and adults referred for ADHD demonstrate higher than chance incidence of depression, individuals referred for depression show elevated rates of ADHD
-depressed children tend to present w/ irritability, negativism, social withdrawal, school dysfunction, and somatic d/o
-family studies suggest some genetic link b/w depression and ADHD, rates of ADHD among relatives of children w/ ADHD w/ or w/o depression were significantly higher than among relatives of controls

Psychiatry Board Review Topics A to Z
17
-stimulants do NOT significantly improve depression; tx for mood d/o are generally not helpful for ADHD
-in presence of a comorbid mood d/o, stimulants are less effective for ADHD; nonstimulant tx that is noradrenergic but not serotonergic are effective for ADHD; serotonergic antidepressants are effective for juvenile depression but not for ADHD
-buproprion (both noradrenergic and dopaminergic) shown to be efficacious for adolescents w/ comorbid ADHD and depression
Attention-Deficit Hyperactivity Disorder, course and prognosis -course is variable; ~50% of cases have sxs persist into adolescence or adulthood
-hyperactivity may disappear in some cases but decreased attention span and impulse-control problems persist
-overactivity is usually first symptom to remit; distractibility is last
-ADHD does NOT usually remit during middle childhood
-persistence is predicted by family hx of ADHD, negative life events, and comorbidity w/conduct sxs, depression, and anxiety d/o
-remission is unlikely before 12 yrs; usually occurs b/w ages 12-20 yrs
-most patients w/ ADHD have partial remission and are vulnerable to antisocial behavior, substance use d/o, and mood d/o
-learning problems often continue throughout life; ~40-50% of cases have sxs persist into adulthood
-adults w/ ADHD may show diminished hyperactivity, but remain impulsive and accident-prone
-educational attainments as a group are lower than those w/o ADHD; early employment hx do not differ from those w/similar education
-children w/ sxs persisting into adolescence are at risk for developing conduct d/o
-children w/ both ADHD and conduct d/o are also at risk for developing a substance-related d/o; appears to be related to presence of conduct d/o rather than ADHD alone
-Most children w/ ADHD have some social difficulties; significantly higher rates of comorbid psychiatric disorders and experience more problems w/ behavior in school as well as w/ peers and family
Bedtime Stories for Psychiatry Residents
18
Attunement -Daniel Stern (1985) looked at developmental research and issues from a psychoanalytic perspective
-affect attunement is the ability to know what the other person is experiencing subjectively; not only emphatic understanding but also the basis for early meaningful communication and, most importantly, provides a way for mutual appreciation of the other’s mental state
-highly attuned mothers foster infant progression from being skilled dyadic partners to being skilled triadic partners, who communicate readily about shared experiences in the world
-from an early age, Stern suggests that the child has the capacity to integrate different sensory information about an object in the world, and play an active role in their relationships w/ others
-children are gradually organizing and ordering them
-relationships to others are vital both for a sense of self and a sense of other as a separate other person in his or her own right
-affect attunement means a sharing or alignment of internal states in the domain of intersubjective relatedness
-attunement relates to the a) intensity b) timing and c) shape of a behavior; an example would be a mother responding w/ a sound and/or movement to her 9 month old child that corresponds equally to duration and amplitude of the child’s cooing
Autism spectrum disorder, pharmacological treatment Atypical antipsychotics
-risperidone; only atypical antipsychotic studied using randomized, double-blind methods and large number of patients, Research Units on Pediatric Psychopharmacology (RUPP) Autism Network
-tx w/ risperidone (dosage range, 0.5-3.5 mg/day) resulted in 56.9% reduction in irritability scores, compared to 14.1% decrease in placebo group
-improvements noted in stereotypic behavior and hyperactivity
-2/3 of children w/ positive response to risperidone at 8 weeks, benefit was maintained at 6 mos
-social isolation and interest in communicating w/ others did not differ significantly b/w tx and placebo

Psychiatry Board Review Topics A to Z
19
-similar results in children w/ subaverage intelligence and no autism; sxs of conduct problems, irritability, and hyperactivity responded to risperidone
Selective Serotonin Reuptake Inhibitors
-demonstrated effectiveness in reducing aggression, irritability, stereotypies, and other disruptive behaviors, no SSRI has been shown to be superior to another
-no SSRI has been shown to improve specific social communication sxs
Aversive conditioning, or punishment -procedure in which punishment or aversive stimulus is used to reduce frequency of a target behavior
Avoidant Personality Disorder, differential diagnosis -schizoid PD also involves social isolation, but schizoid person does NOT desire relationships
-avoidant person desires relationships but avoids them because of anxiety and fears of humiliation and rejection
-avoidant PD is characterized by avoidance of situations and relationships involving possible rejection, disappointment, ridicule, or shame
-Axis I social phobia usually consists of specific fears related to social performance (e.g., fear of saying something inappropriate or of being unable to answer questions in front of other people)
Ready to take a break from your board review question books? Bedtime Stories for Psychiatry Residents provides the perfect complement to board review question books and a structured reading program of up-to-date psychiatry references. This study guide contains 250 selected psychiatry topics with concise, bullet-format outlines with hundreds of high yield facts. Topics are organized in alphabetical order with key terms and phrases are in bold print to reinforce important concepts. Bedtime Stories for Psychiatry Residents: Psychiatry Board Review Topics A to Z Buy The Complete Version of This Book at Booklocker.com: http://www.booklocker.com/p/books/4958.html?s=pdf