Embed Size (px)
Citation preview

bluecrosswisconsin.com
Available through…
Direct and Online Sales
QUOTE: OCTOBER 1
EFFECTIVE: NOVEMBER 1

bluecrosswisconsin.com
Product Objectives:
•To meet the needs of the those uninsured or underinsured
• To offer an economical product
• To serve the small group business market.

bluecrosswisconsin.com
BENEFITS
WAITING PERIODS A condition which manifests itself in the 6 months before the member’s effective date. No benefits are payable for a pre-existing condition until one of the following: 12 consecutive months after the effective date during which no care was received or during which the member was insured under this contract. Portability applies.
DEPENDENT ELIGIBILITY
Dependents to 19, end of year Full-time students to age 23, end of year
bluecrosswisconsin.com
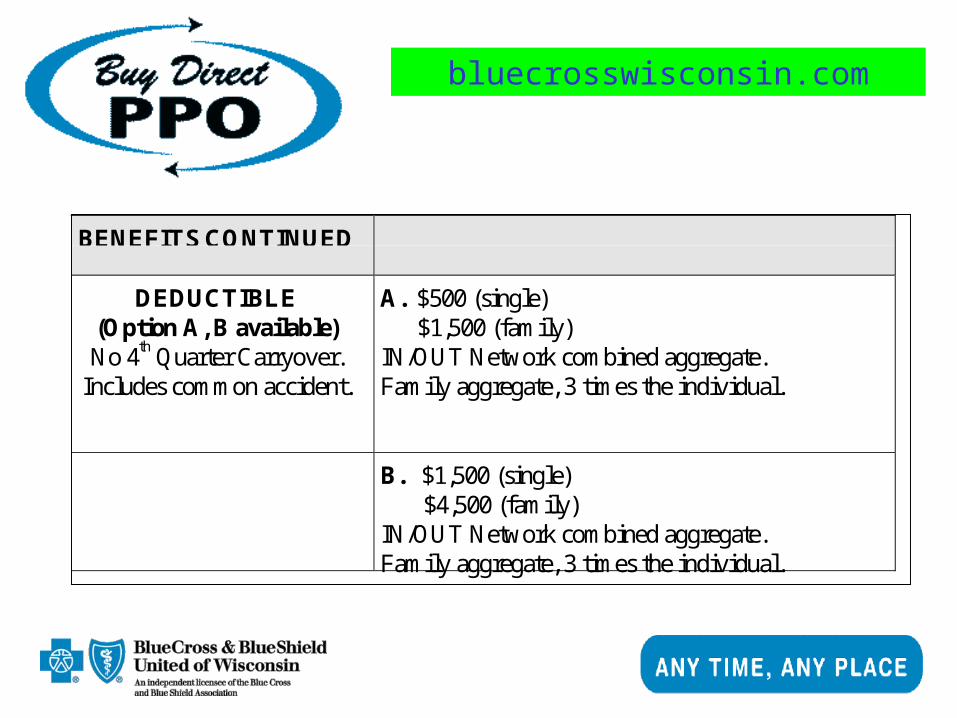
BENEFITS CONTINUED
DEDUCTIBLE(Option A, B available)No 4th Quarter Carryover.
Includes common accident.
A. $500 (single) $1,500 (family)IN/OUT Network combined aggregate.Family aggregate, 3 times the individual.
B. $1,500 (single) $4,500 (family)IN/OUT Network combined aggregate.Family aggregate, 3 times the individual.
bluecrosswisconsin.com
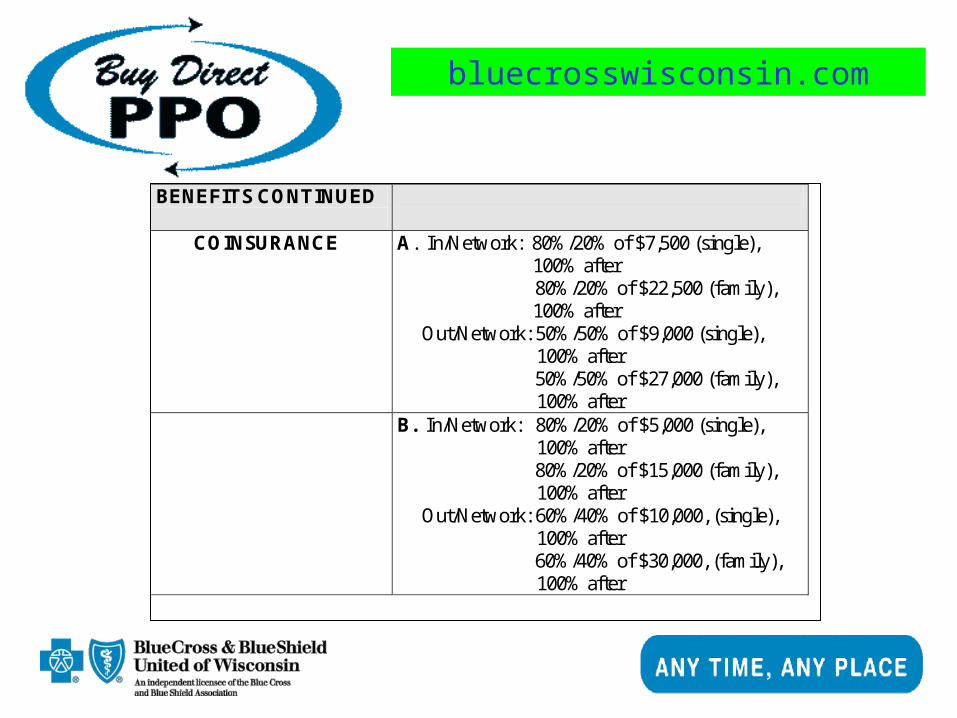
BENEFITS CONTINUED
COINSURANCE
A. In/Network: 80%/20% of $7,500 (single), 100% after
80%/20% of $22,500 (family), 100% after
Out/Network: 50%/50% of $9,000 (single), 100% after
50%/50% of $27,000 (family), 100% after
B. In/Network: 80%/20% of $5,000 (single), 100% after
80%/20% of $15,000 (family), 100% after
Out/Network: 60%/40% of $10,000, (single), 100% after
60%/40% of $30,000, (family), 100% after

bluecrosswisconsin.com
BENEFITS CONTINUED
COINSURANCE OUT-OF-POCKET
MAXIMUM (per calendar year, does not
include deductible) level 1 and level 2 accumulate
separately under the out-of-pocket maximum
A. In/Network: $1,500 out of pocket maximum (single)
$4,500 out of pocket maximum (family)
Out/Network: $4,500 out of pocket maximum (single)
$13,500 out of pocket maximum (family)
B. In/Network: $1,000 out of pocket maximum (single)
$3,000 out of pocket maximum (family)
Out/Network: $4,000 out of pocket maximum (single)
$12,000 out of pocket maximum (family)
LIFETIME MAXIMUM $1,000,000

bluecrosswisconsin.com
INPATIENT HOSPITALSERVICES
INPATIENT HOSPITALDAY MAXIMUM
Unlimited inpatient days, per member, perconfinement - including accommodations andancillary services.Discharge and re-admission equals newconfinement.Subject to deductibles and coinsurance.
ACCOMMODATIONS Average Semi-Private room

bluecrosswisconsin.com
OUTPATIENTHOSPITAL SERVICES
EMERGENCY ACCIDENTCARE/
EMERGENCY MEDICALCARE/
ILLNESS
In/Network: $100 / Out/Network: $150 copay forEmergency outpatient hospital charge (per visit) -Waived if admitted or related to a surgicalprocedure.Additional services related to the emergency/clinicsroom/clinics stay are subject to any applicabledeductibles and coinsurance.
DIAGNOSTIC, XRAY &LAB
(Includes mammograms)
Subject to deductibles and coinsurance.(2 mammograms between 45-49 years of age, oneper year 50+)

bluecrosswisconsin.com
SURGICALPROFESSIONAL
SERVICES
SURGERY Subject to deductibles and coinsurance.STERILIZATIONS Subject to deductibles and coinsurance.
ELECTIVE/ THERAPEUTICABORTIONS
Subject to deductibles and coinsurance.
ASSISTANT SURGEON Subject to deductibles and coinsurance.ORGAN TRANSPLANTS
(365 day waiting period for alltransplants other than kidneywill apply)
Kidney, cornea, heart, lung, heart/lung, liver,pancreas, and non-experimental/investigationalbone marrow.Subject to deductibles and coinsurance.

bluecrosswisconsin.com
MEDICALPROFESSIONAL
SERVICES
INPATIENT GENERALMEDICAL CARE &CONSULTATIONS
Subject to deductibles and coinsurance.
HOME, OFFICE,OUTPATIENT VISITS& CONSULTATIONS
Subject to deductible and coinsurance.
CHIROPRACTOR Subject to deductible and coinsurance.ACCIDENT
CARE/URGENT CARESubject to deductibles and coinsurance.

bluecrosswisconsin.com
MEDICALPROFESSIONAL
SERVICESCONTINUEDCHILDHOOD
IMMUNIZATION(As of 11/01/00)
The in-network benefit is notsubject to the plan'sdeductible, coinsurance,copayment or $500 routinemaximum. For OON, thenormal plan cost-sharingrequirements apply.
Benefits are available to dependents under 6 yearsof age for appropriate and necessaryimmunizations. “Appropriate and necessaryimmunizations” means the administration ofvaccine that meets the standards approved by theU.S. public health services for such biologicalproducts against at least all of the following:diphtheria, pertussis, tetanus, polio, measles,mumps, rubella, hemophilus influenza B, hepatitisB, varicella.
bluecrosswisconsin.com
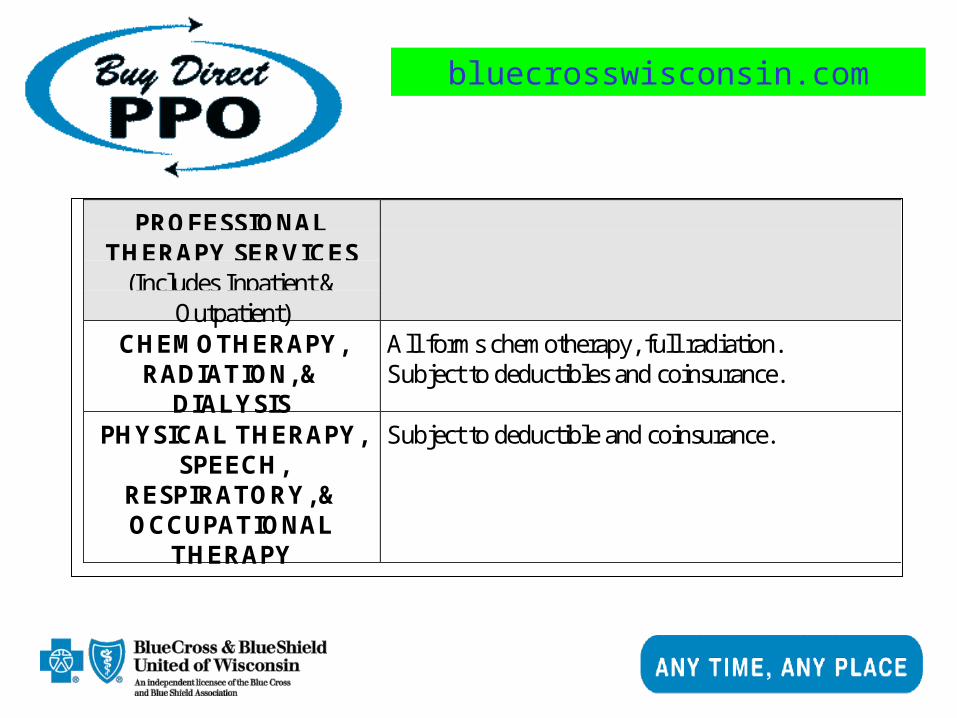
PROFESSIONALTHERAPY SERVICES
(Includes Inpatient &Outpatient)
CHEMOTHERAPY,RADIATION, &
DIALYSIS
All forms chemotherapy, full radiation.Subject to deductibles and coinsurance.
PHYSICAL THERAPY,SPEECH,
RESPIRATORY, &OCCUPATIONAL
THERAPY
Subject to deductible and coinsurance.
bluecrosswisconsin.com
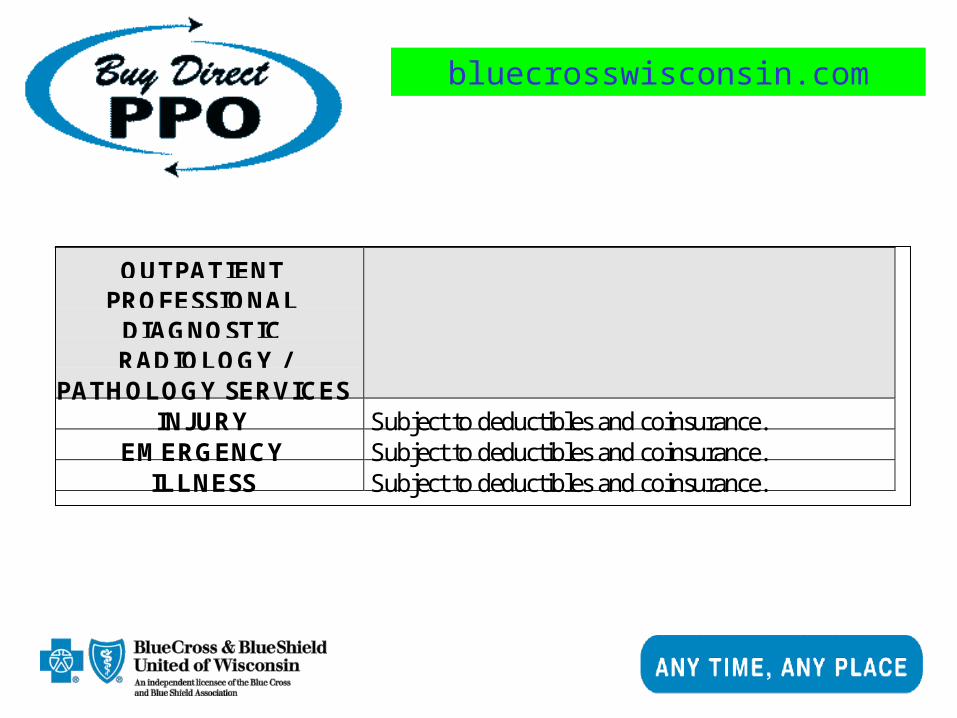
OUTPATIENTPROFESSIONAL
DIAGNOSTICRADIOLOGY /
PATHOLOGY SERVICESINJURY Subject to deductibles and coinsurance.
EMERGENCY Subject to deductibles and coinsurance.ILLNESS Subject to deductibles and coinsurance.
bluecrosswisconsin.com
OTHER PROFESSIONALSERVICES
PRIVATE DUTYNURSING
Paid only under Home Care
ANESTHESIA Includes CRNA, excludes attending PhysicianSubject to deductibles and coinsurance.

bluecrosswisconsin.com
OTHER SERVICES
MATERNITY(Includes prenatal/postnatal
care and delivery)
Subject to deductibles and coinsurance.Benefits for a hospital stay following the birth of achild will not be less than 48 hours for a vaginaldelivery and 96 hours for a cesarean section.
HOME CARE 40 visits per calendar year, additional 40 ifterminally ill.Subject to deductibles and coinsurance.
SKILLED NURSINGFACILITY
30 days per admissionSubject to deductibles and coinsurance.
PRE-CERTIFICATIONPROGRAM
Advantage Program in effect$500 penalty for non-compliance with pre-certification requirements. Does not apply towardsdeductibles, coinsurance, or any applicablecopayment.

bluecrosswisconsin.com
OTHER SERVICES CONTINUEDMENTAL
HEALTH/ALCOHOLISMOR OTHER DRUG
ABUSE – INPATIENT
$7,000, lesser of 30 days or $7,000 minus 10%.Not subject to deductibles and coinsurance.
Once the maximum is met, one additional Inpatientday of care, is available for mental health at 100%.This benefit does not include services rendered forthe treatment of alcoholism or other drug abuseproblems.
MENTAL HEALTH –TRANSITIONAL
DRUG ANDALCOHOLISM
Subject to $3,000 maximum minus 10%coinsurance.Not subject to deductible and coinsurance.
Once the maximum is met, one additionalTransitional treatment, is available for mentalhealth at 100%. This benefit does not includeservices rendered for the treatment of alcoholism orother drug abuse problems.
bluecrosswisconsin.com
MENTAL HEALTH –OUTPATIENT OFFICE
VISIT DRUG ANDALCOHOLISM
Subject to $2,000 maximum minus 10%coinsurance.Not subject to deductible and coinsurance.
Once the maximum is met, one additionalOutpatient visit, is available for mental health at100%. This benefit does not include servicesrendered for the treatment of alcoholism or otherdrug abuse problems.
ROUTINE CARE(Physical exams, well baby,and immunizations over age
6. Includes related DXL.Includes physical exams forsports, school, employment,occupation, & insurance.)
Paid at 100% with $500 annual maximum perperson.(Only in network.)

bluecrosswisconsin.com
MENTAL HEALTH –OUTPATIENT OFFICE
VISIT DRUG ANDALCOHOLISM
Subject to $2,000 maximum minus 10%coinsurance.Not subject to deductible and coinsurance.
Once the maximum is met, one additionalOutpatient visit, is available for mental health at100%. This benefit does not include servicesrendered for the treatment of alcoholism or otherdrug abuse problems.
ROUTINE CARE(Physical exams, well baby,and immunizations over age
6. Includes related DXL.Includes physical exams forsports, school, employment,occupation, & insurance.)
Paid at 100% with $500 annual maximum perperson.(Only in network.)

bluecrosswisconsin.com
AMBULANCE Services limited to $200 per trip.Not subject to deductible and coinsurance.
OTHER SERVICES CONTINUEDBLOOD Covered from 1st pint.
Subject to deductible and coinsurance.LEAD SCREENING Subject to deductibles and coinsurance, (up to age
6).PROSTHETICS ANDDURABLE MEDICAL
EQUIPMENT
Subject to deductibles and coinsurance.
MEDICAL SUPPLIES Subject to deductibles and coinsurance.HOLD HARMLESS None

bluecrosswisconsin.com
EXCLUSIONS PPO does not provide coverage for the following: Routine oradministrative physical exams out-of-network, exceptmammographies. Hearing aids. Dentistry, including treatmentfor temporomandibular joint (TMJ) disorders, except asspecifically described in the policy. Cosmetic surgery, unlessneeded as a result of an accident, to correct a birth defect, orfor breast reconstruction following a mastectomy. Weight-lossprograms, except as covered under the wellness program.Orthodontics, orthognathic surgery and osteotomies. Illness orinjury eligible for workers compensation. Services for whichan individual is eligible under Medicare, whether or not theindividual is enrolled in Medicare. (continued)

bluecrosswisconsin.com
EXCLUSIONSCONTINUED
Services considered not medically necessary orexperimental/investigational. Services performed by animmediate family member or someone who lives with thepatient. For organ or bone marrow transplants other than:kidney, cornea, non-experimental/investigational bone marrow,including hematopoietic stem cell support, heart, lung,heart/lung, liver and pancreas. Inpatient hospitalizationprimarily for physical, x-ray and radiation therapies. Anyinfertility treatment. Reversal of sterilization. Any portion of acharge for a specific service that is greater than the usual andcustomary allowance in that area.
UWG LIFEBENEFIT
Life Insurance Benefits to be underwritten by United WisconsinGroup. $10,000, Life, $200 STD.
8/23/00

bluecrosswisconsin.com
Buy Direct PPO
Plan A
Plan B
1 MM Lifetime Max
PPO ER-Copay/$100
Non-PPO ER-Copay/$150
Full-time students to age 23
Family Aggregate-3X Individual
Routine Care w/out office visit Copay
2 to 99
Option 1
Option 2
2 MM Lifetime Max
PPO ER-Copay/$50
Non-PPO ER-Copay/$75
Full-time students to age 26
Family Aggregate-2X Individual
Routine Care w/office visit Copay
Product Variations





























