Embed Size (px)
Citation preview
Burn Injury… triage & assessment
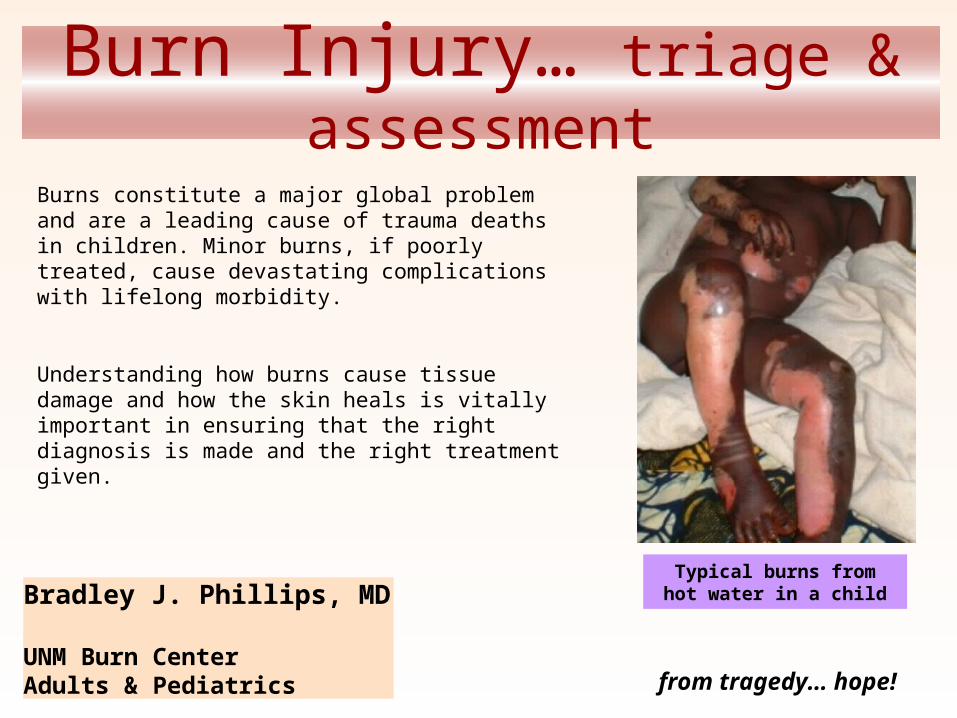
Burns constitute a major global problem and are a leading cause of trauma deaths in children. Minor burns, if poorly treated, cause devastating complications with lifelong morbidity.
Understanding how burns cause tissue damage and how the skin heals is vitally important in ensuring that the right diagnosis is made and the right treatment given.
Typical burns from hot water in a childBradley J. Phillips, MD
UNM Burn CenterAdults & Pediatrics from tragedy… hope!
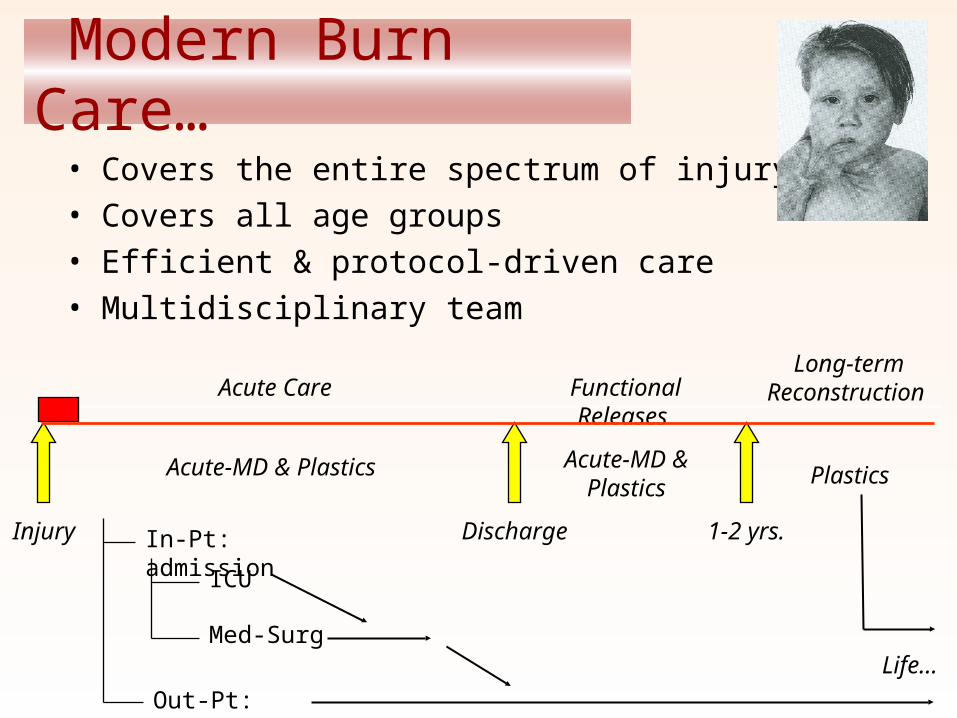
Modern Burn Care…
• Covers the entire spectrum of injury• Covers all age groups• Efficient & protocol-driven care• Multidisciplinary team
Injury
Acute Care
In-Pt: admission
Plastics
Out-Pt: clinic
ICU
Med-Surg
Functional Releases Long-term
Reconstruction
Acute-MD & Plastics
Acute-MD & Plastics
Discharge 1-2 yrs.
Life…
• As of the early 1990’s, the rate of reportable burn injuries in the U.S. had declined from about 10/10,000 to 4.2/10,000.
• 45,000 hospitalizations per year, about half to 125 specialized burn treatment centers and half to the nation’s 5,000 other hospitals.
• 700,000 annual emergency department visits @1.2 per injury. (Burn center hospitals average 200 burn admissions a year, other hospitals less than five.)
• The average size of a burn injury admitted to a burn center is about 14% of total body surface area (% TBSA). (1991-93)
• Burns of 10% TBSA or less account for 54% of burn center admissions, while burns of 60% TBSA or more account for 4% of admissions.
Burn Demographics & Incidence…
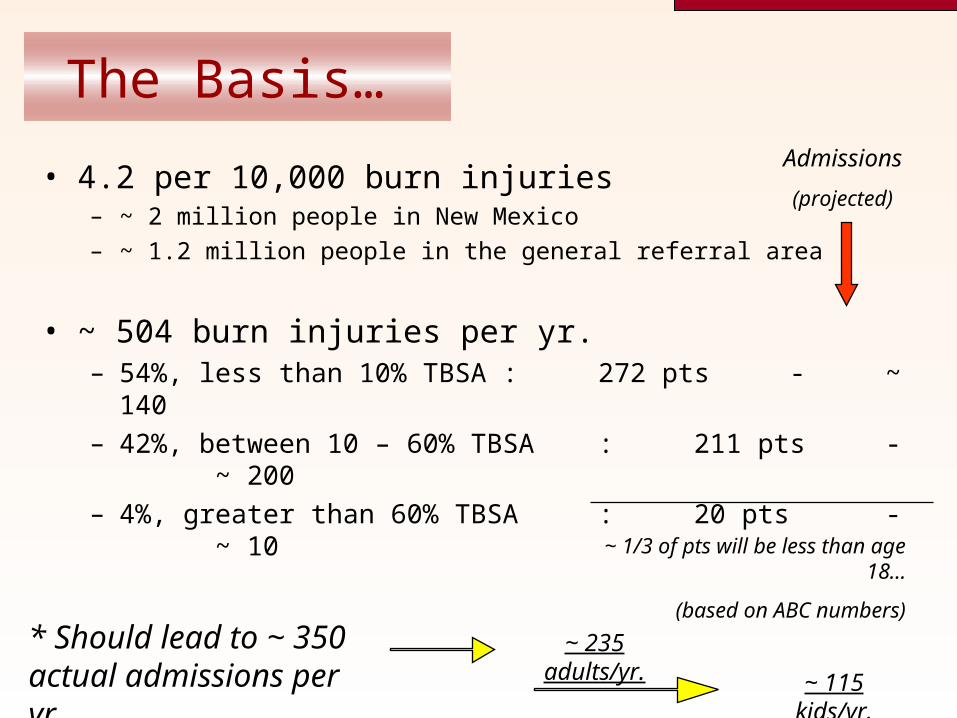
The Basis…
• 4.2 per 10,000 burn injuries– ~ 2 million people in New Mexico
– ~ 1.2 million people in the general referral area
• ~ 504 burn injuries per yr. – 54%, less than 10% TBSA : 272 pts - ~ 140– 42%, between 10 – 60% TBSA : 211 pts - ~ 200– 4%, greater than 60% TBSA : 20 pts - ~ 10
~ 1/3 of pts will be less than age 18…
(based on ABC numbers)
* Should lead to ~ 350 actual admissions per yr.
Admissions
(projected)
~ 115 kids/yr.
~ 235 adults/yr.
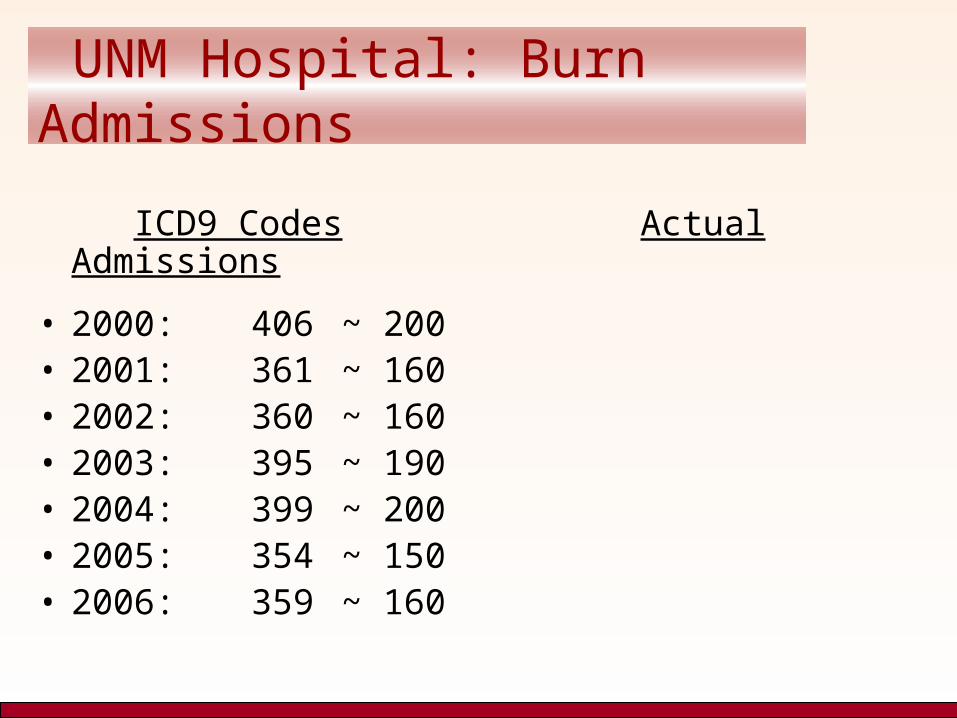
UNM Hospital: Burn Admissions
ICD9 Codes Actual Admissions
• 2000: 406 ~ 200• 2001: 361 ~ 160• 2002: 360 ~ 160• 2003: 395 ~ 190• 2004: 399 ~ 200• 2005: 354 ~ 150• 2006: 359 ~ 160
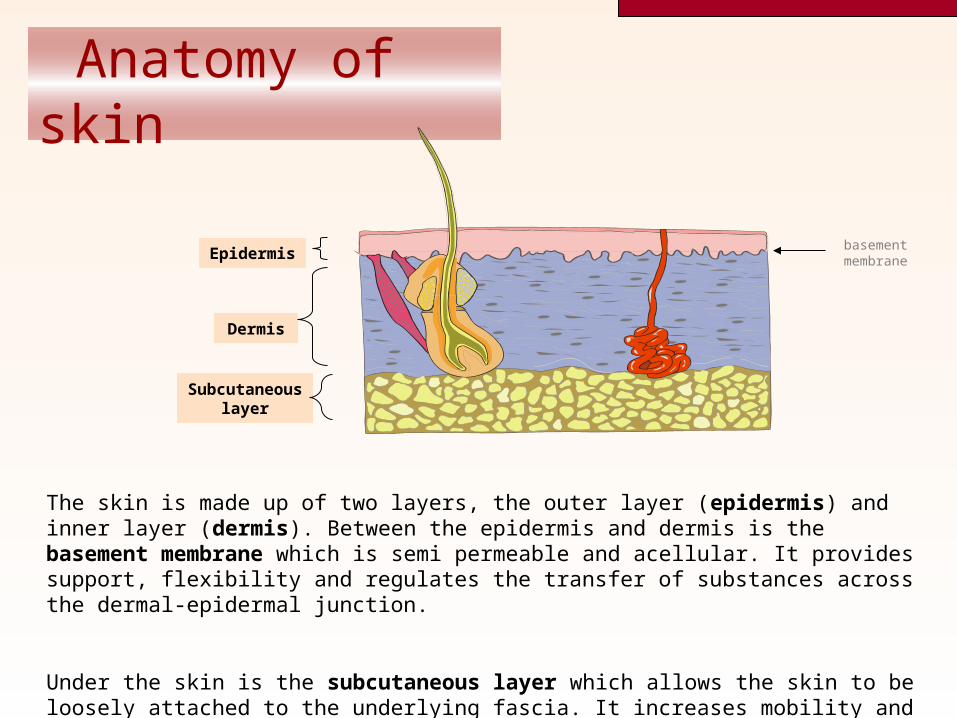
Anatomy of skin
Epidermis
Dermis
The skin is made up of two layers, the outer layer (epidermis) and inner layer (dermis). Between the epidermis and dermis is the basement membrane which is semi permeable and acellular. It provides support, flexibility and regulates the transfer of substances across the dermal-epidermal junction.
Under the skin is the subcutaneous layer which allows the skin to be loosely attached to the underlying fascia. It increases mobility and is especially important over joints.
basement membrane
Subcutaneous layer
Local effects of burn injury
Local effects:– Cell death/disturbed function– Release of inflammatory mediators– Increased capillary permeability– Microvascular thrombosis
Due to differences in skin thickness with age, at 55C, severe damage occurs after 10 seconds in a child and 30 seconds in an adult.
Skin thickness is also reduced in older people and in certain conditions (e.g. steroid therapy).
Local effects (cont.)
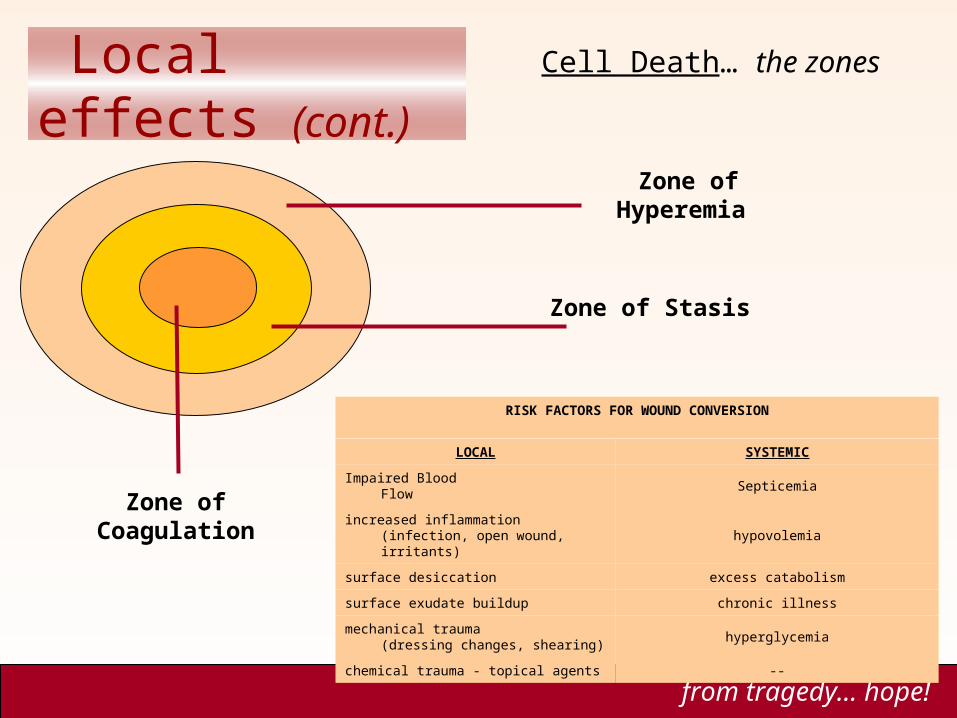
Cell Death… the zones
from tragedy… hope!
Zone of Coagulation
Zone of Stasis
Zone of Hyperemia
RISK FACTORS FOR WOUND CONVERSION
LOCAL SYSTEMIC
Impaired Blood Flow Septicemia
increased inflammation(infection, open wound, irritants)
hypovolemia
surface desiccation excess catabolism
surface exudate buildup chronic illness
mechanical trauma(dressing changes, shearing)
hyperglycemia
chemical trauma - topical agents --
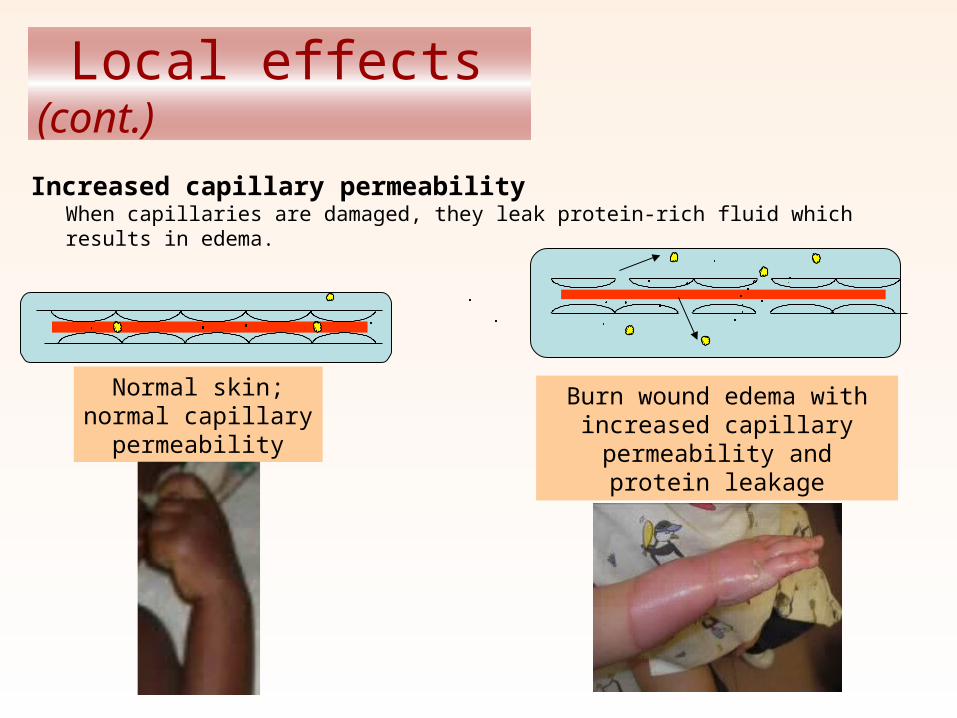
Increased capillary permeabilityWhen capillaries are damaged, they leak protein-rich fluid which results in edema.
Normal skin; normal capillary permeability
Burn wound edema with increased capillary permeability
and protein leakage
Local effects (cont.)
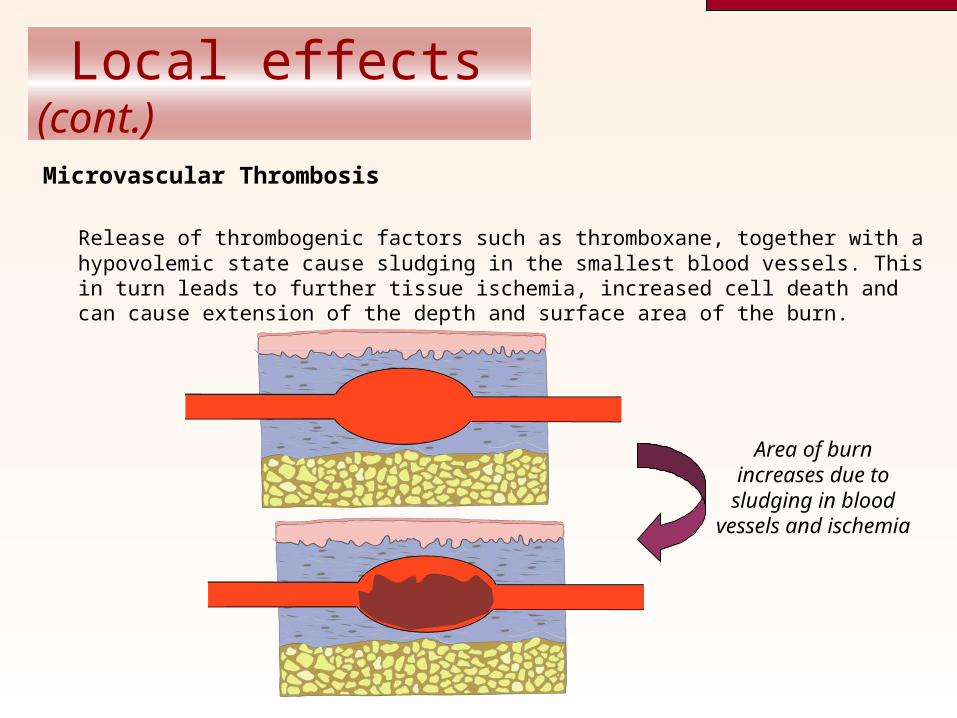
Microvascular Thrombosis
Release of thrombogenic factors such as thromboxane, together with a hypovolemic state cause sludging in the smallest blood vessels. This in turn leads to further tissue ischemia, increased cell death and can cause extension of the depth and surface area of the burn.
Area of burn increases due to sludging in blood
vessels and ischemia
Local effects (cont.)
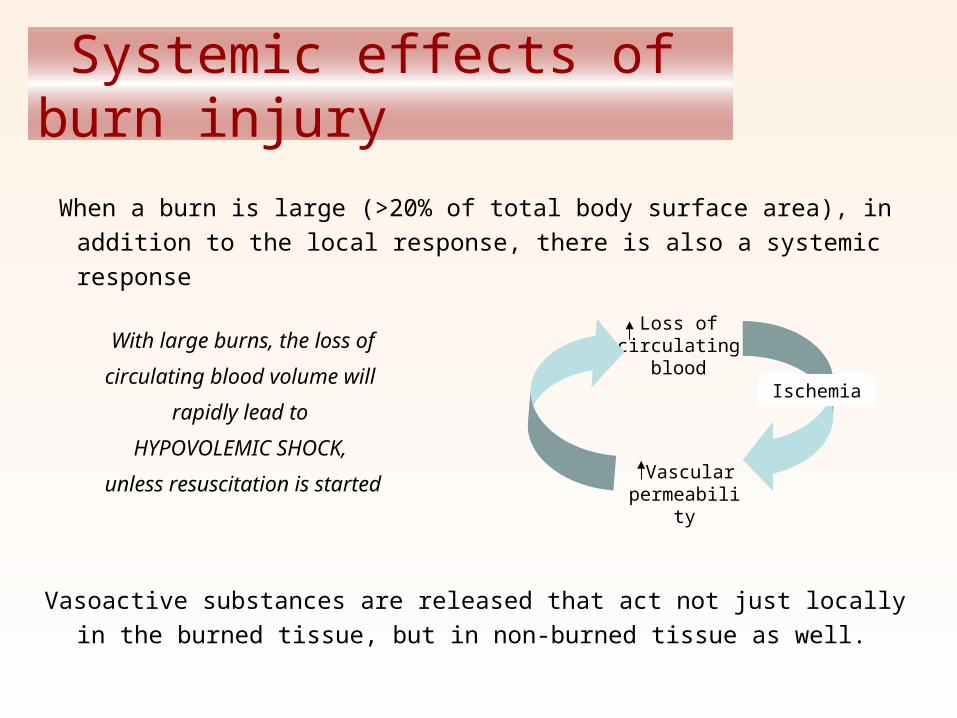
Systemic effects of burn injury
When a burn is large (>20% of total body surface area), in addition to
the local response, there is also a systemic response
Vasoactive substances are released that act not just locally in the burned
tissue, but in non-burned tissue as well.
With large burns, the loss of
circulating blood volume will
rapidly lead to
HYPOVOLEMIC SHOCK,
unless resuscitation is started
Loss of circulating
blood
Vascular permeability
Ischemia
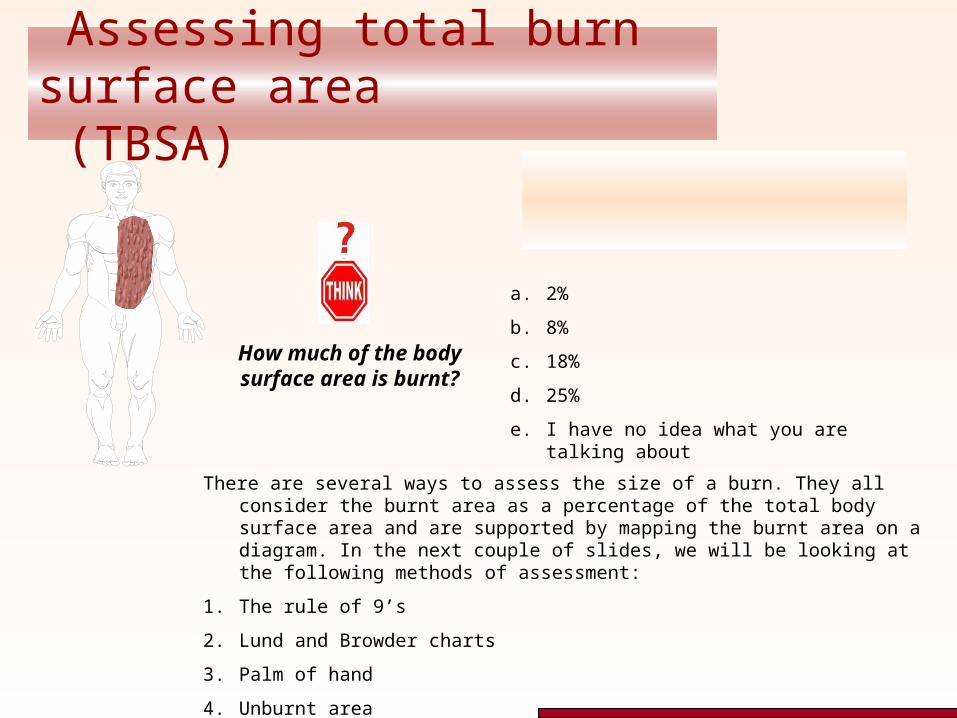
Assessing total burn surface area (TBSA)
The area of this burn is about 8% of total body surface area.
How much of the body surface area is burnt?
There are several ways to assess the size of a burn. They all consider the burnt area as a percentage of the total body surface area and are supported by mapping the burnt area on a diagram. In the next couple of slides, we will be looking at the following methods of assessment:
1. The rule of 9’s
2. Lund and Browder charts
3. Palm of hand
4. Unburnt area
a. 2%
b. 8%
c. 18%
d. 25%
e. I have no idea what you are talking about
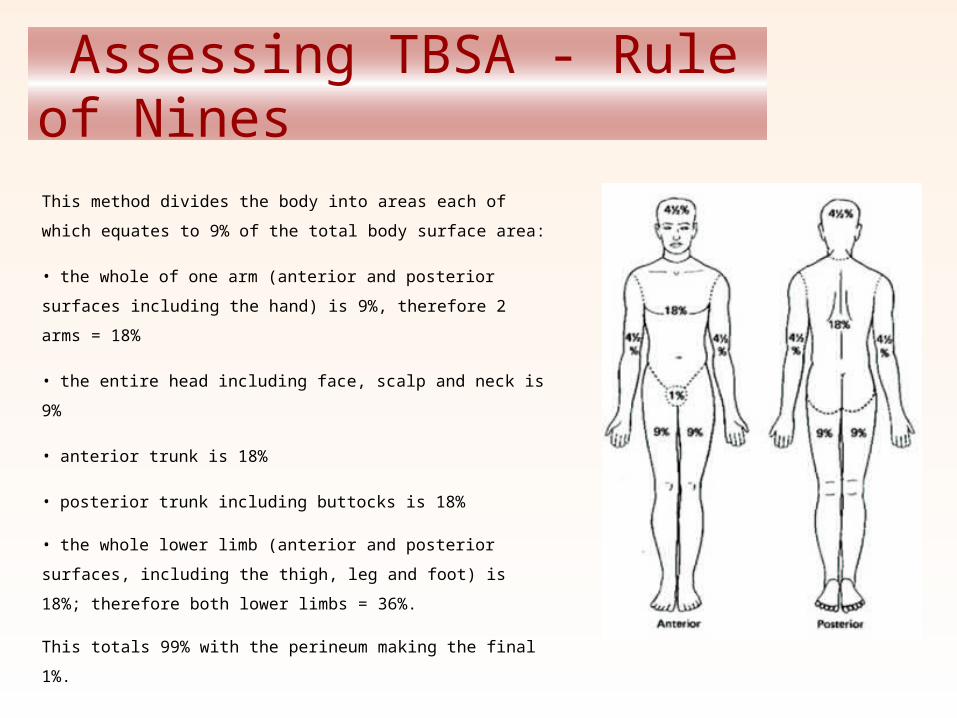
Assessing TBSA - Rule of Nines
This method divides the body into areas each of which
equates to 9% of the total body surface area:
• the whole of one arm (anterior and posterior surfaces
including the hand) is 9%, therefore 2 arms = 18%
• the entire head including face, scalp and neck is 9%
• anterior trunk is 18%
• posterior trunk including buttocks is 18%
• the whole lower limb (anterior and posterior surfaces,
including the thigh, leg and foot) is 18%; therefore both lower
limbs = 36%.
This totals 99% with the perineum making the final 1%.
Assessing TBSA in children
Why might the “rule of 9’s” be unreliable in children?
Body proportions change with age. In a child, the head represents a much greater proportion of the
total body surface area.
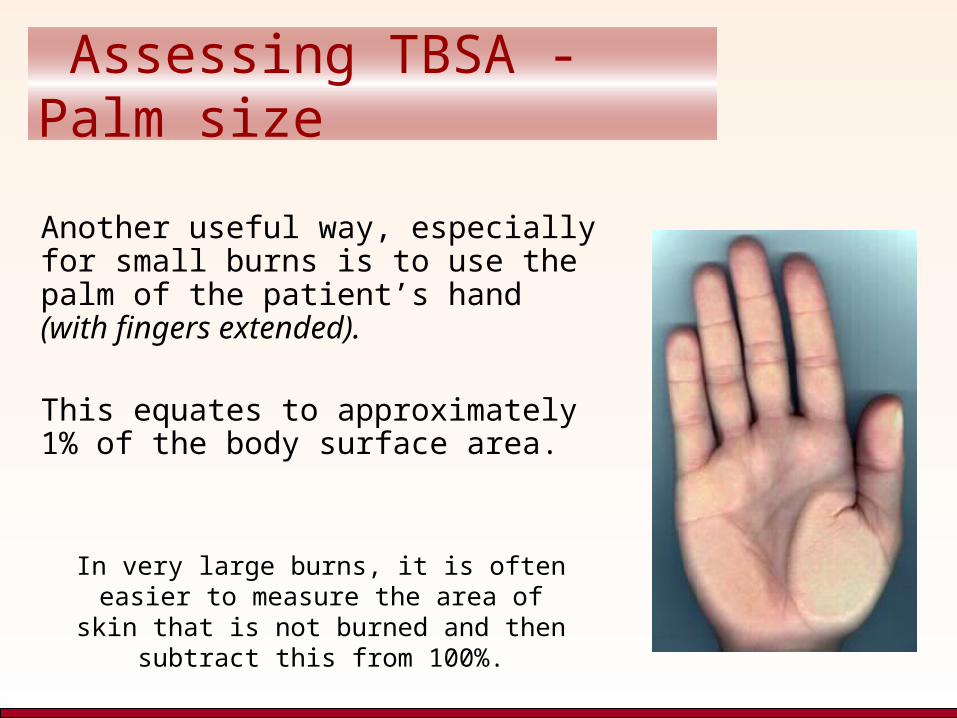
Assessing TBSA - Palm size
Another useful way, especially for small burns is to use the palm of the patient’s hand (with fingers extended).
This equates to approximately 1% of the body surface area.
In very large burns, it is often easier to measure the area of skin that is not
burned and then subtract this from 100%.
Depth of burn
The depth of a burn determines its treatment and how long it takes to heal.
For this reason, it is important to be able to assess the depth as:
Superficial…………………………………………. “1st Degree”
Partial thickness………………………………….. “2nd Degree”
• Superficial partial thickness
• Deep partial thickness
Full thickness……………………………………... “3rd Degree”
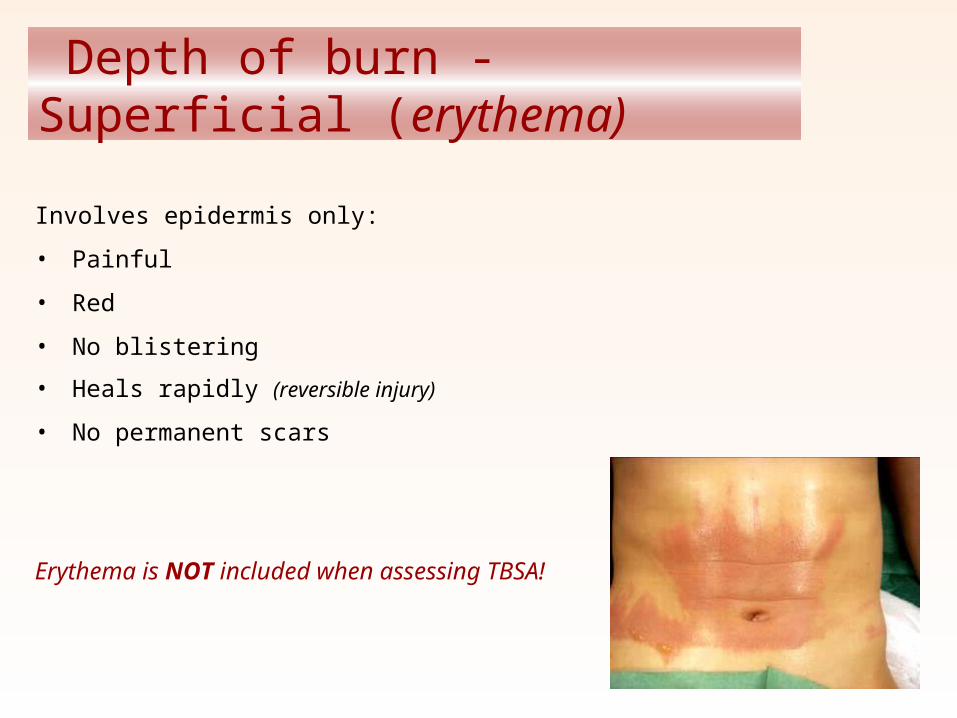
Depth of burn - Superficial (erythema)
Involves epidermis only:
• Painful
• Red
• No blistering
• Heals rapidly (reversible injury)
• No permanent scars
Erythema is NOT included when assessing TBSA!
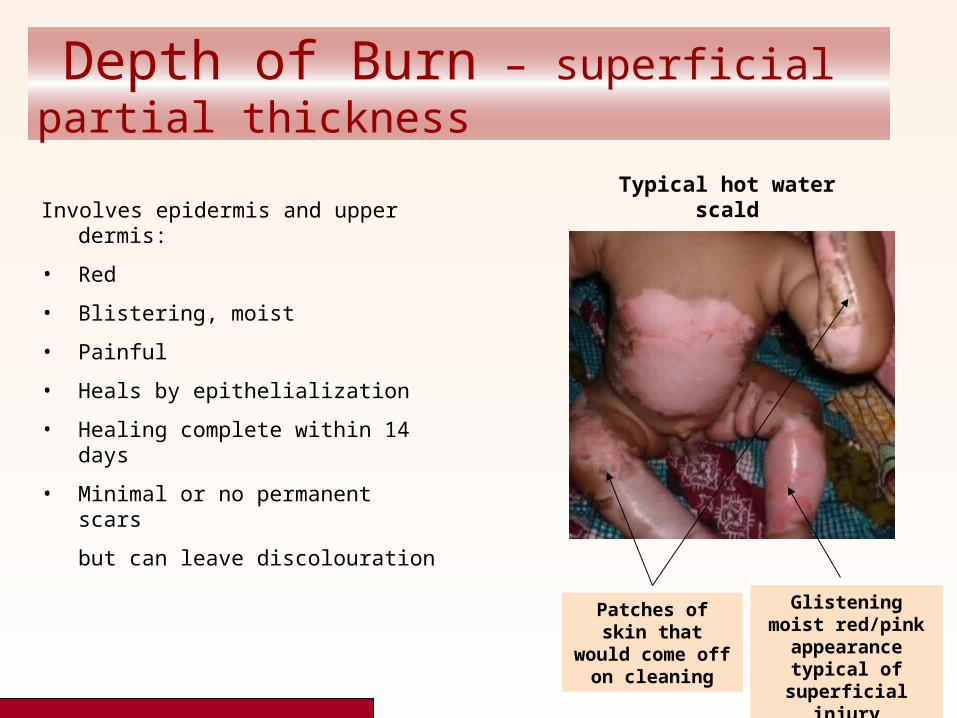
Depth of Burn – superficial partial thickness
Patches of skin that would come off on cleaning
Glistening moist red/pink
appearance typical of superficial injury
Typical hot water scaldInvolves epidermis and upper dermis:
• Red
• Blistering, moist
• Painful
• Heals by epithelialization
• Healing complete within 14 days
• Minimal or no permanent scars
but can leave discolouration
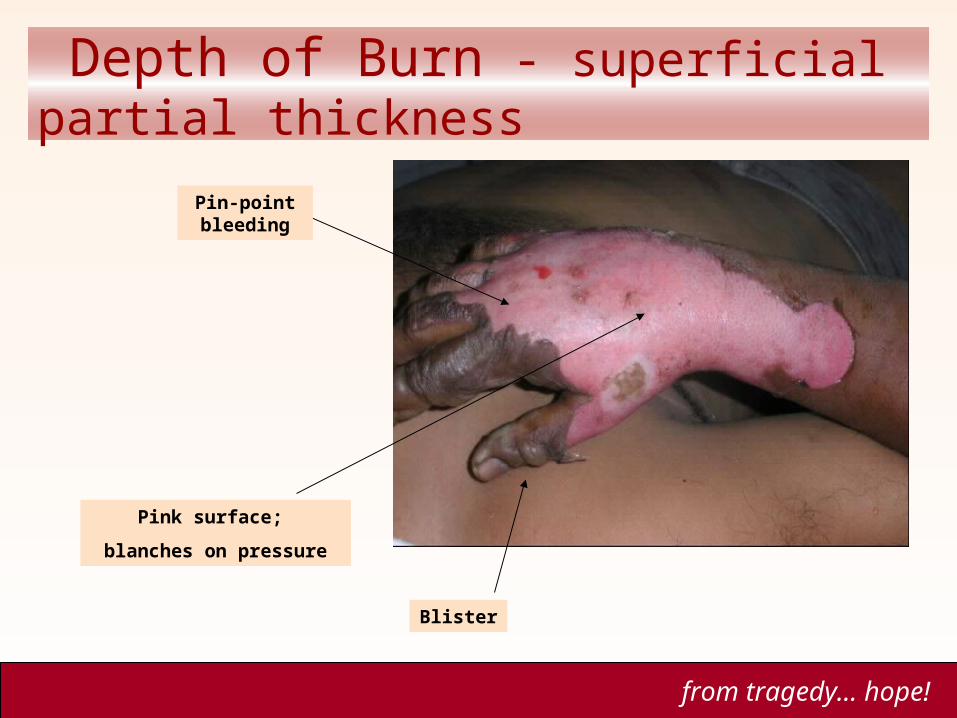
Depth of Burn - superficial partial thickness
Blister
Pin-point bleeding
Pink surface;
blanches on pressure
from tragedy… hope!
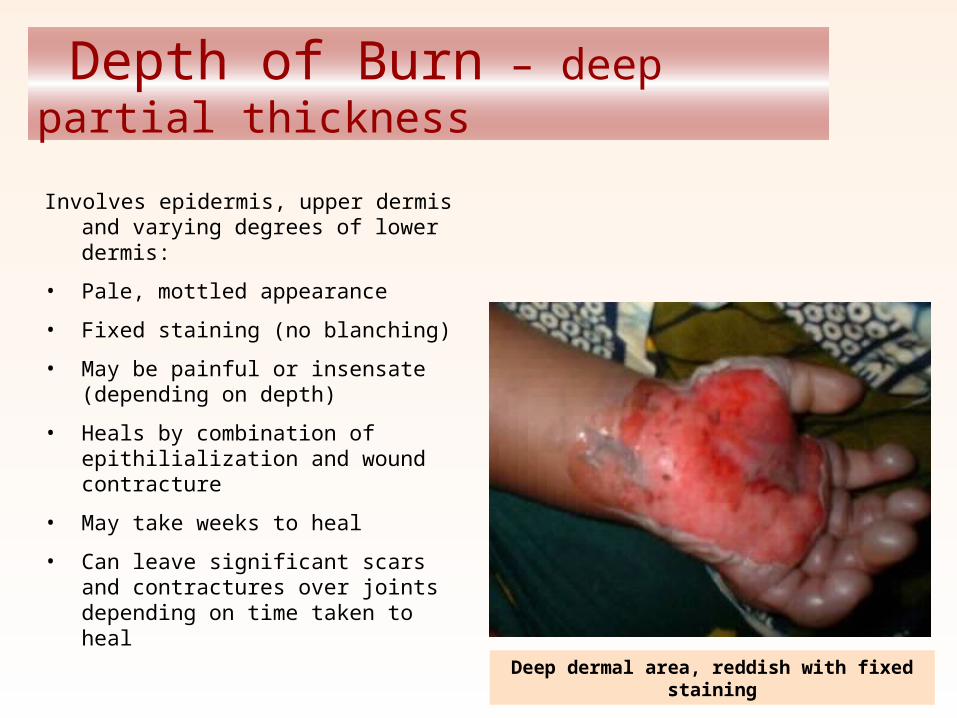
Depth of Burn – deep partial thickness
Involves epidermis, upper dermis and varying degrees of lower dermis:
• Pale, mottled appearance
• Fixed staining (no blanching)
• May be painful or insensate (depending on depth)
• Heals by combination of epithilialization and wound contracture
• May take weeks to heal
• Can leave significant scars and contractures over joints depending on time taken to heal
Deep dermal area, reddish with fixed staining
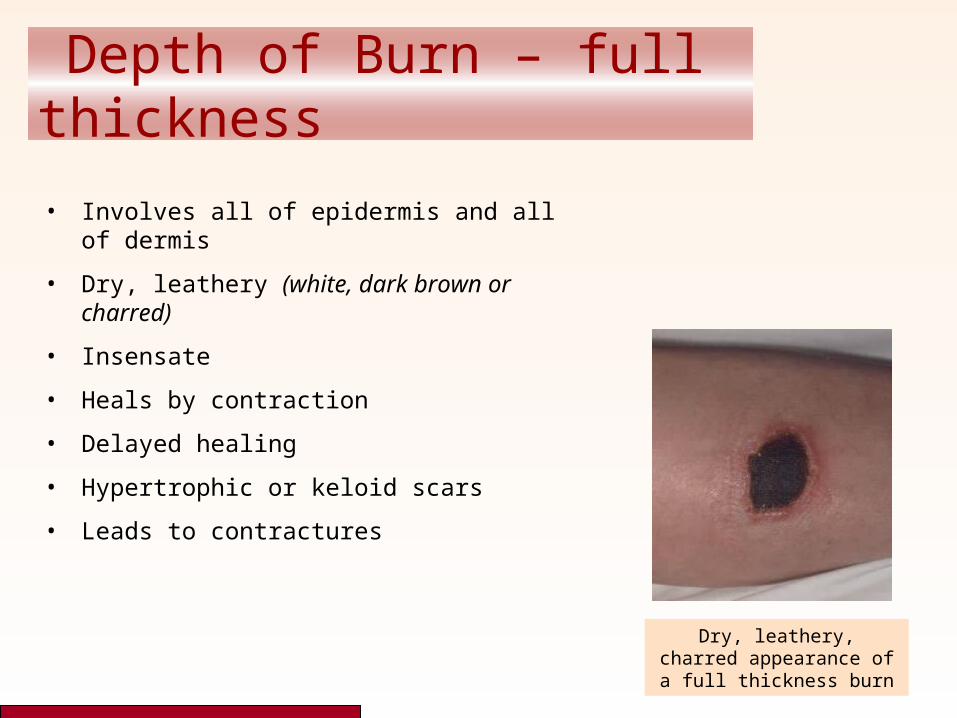
Depth of Burn – full thickness
• Involves all of epidermis and all of dermis
• Dry, leathery (white, dark brown or charred)
• Insensate
• Heals by contraction
• Delayed healing
• Hypertrophic or keloid scars
• Leads to contractures
Dry, leathery, charred appearance of a full
thickness burn
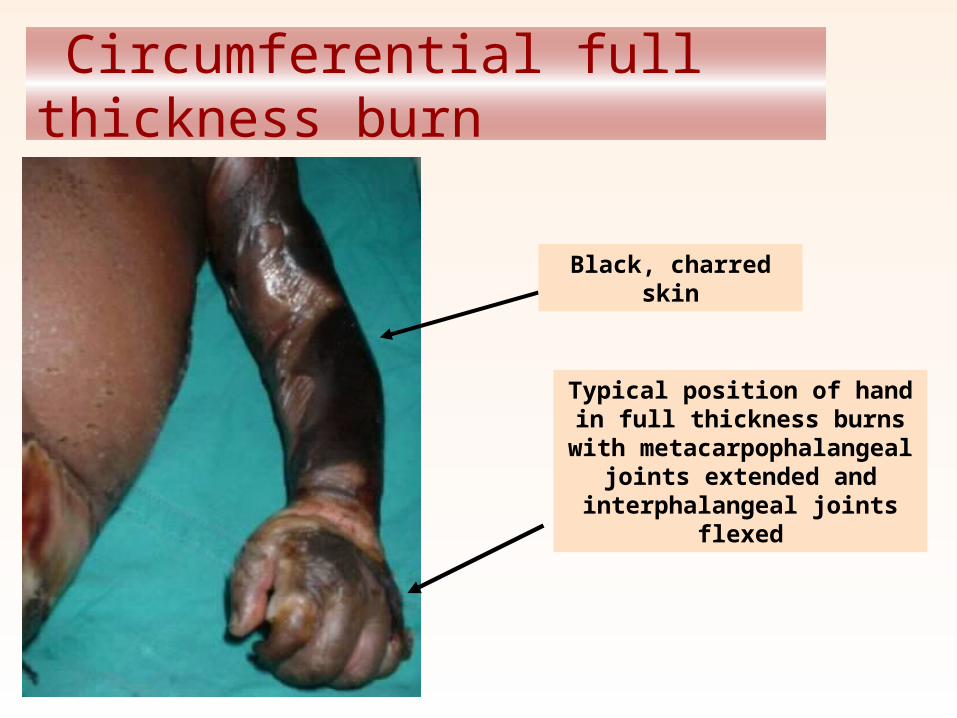
Circumferential full thickness burn
Typical position of hand in full thickness burns with
metacarpophalangeal joints extended and interphalangeal
joints flexed
Black, charred skin

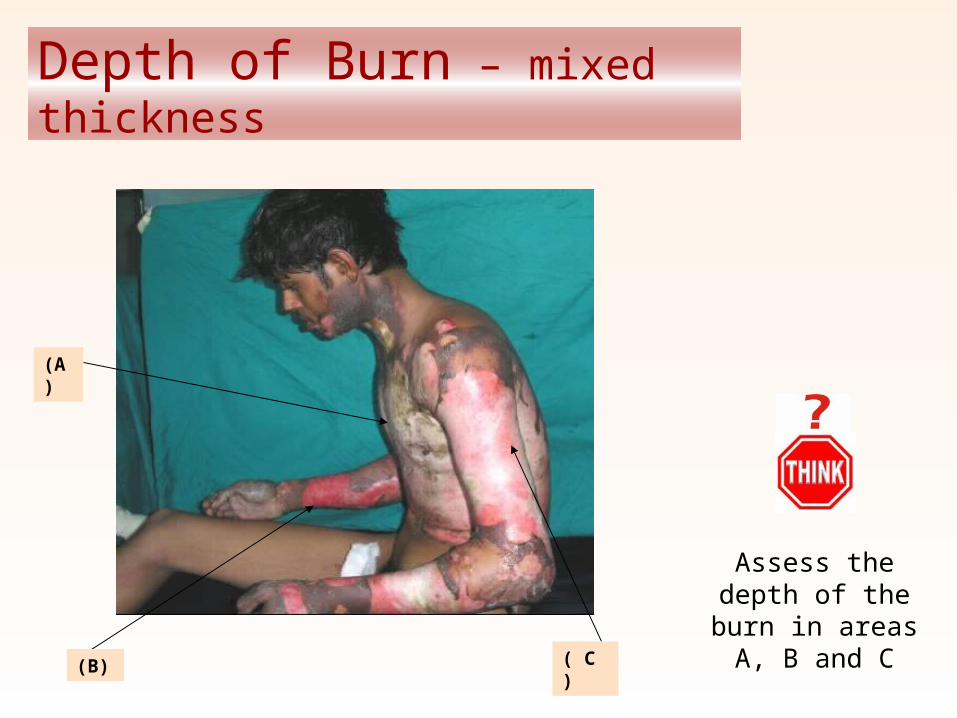
Depth of Burn – mixed thickness
Assess the depth of the burn in
areas A, B and C( C )(B)
(A)
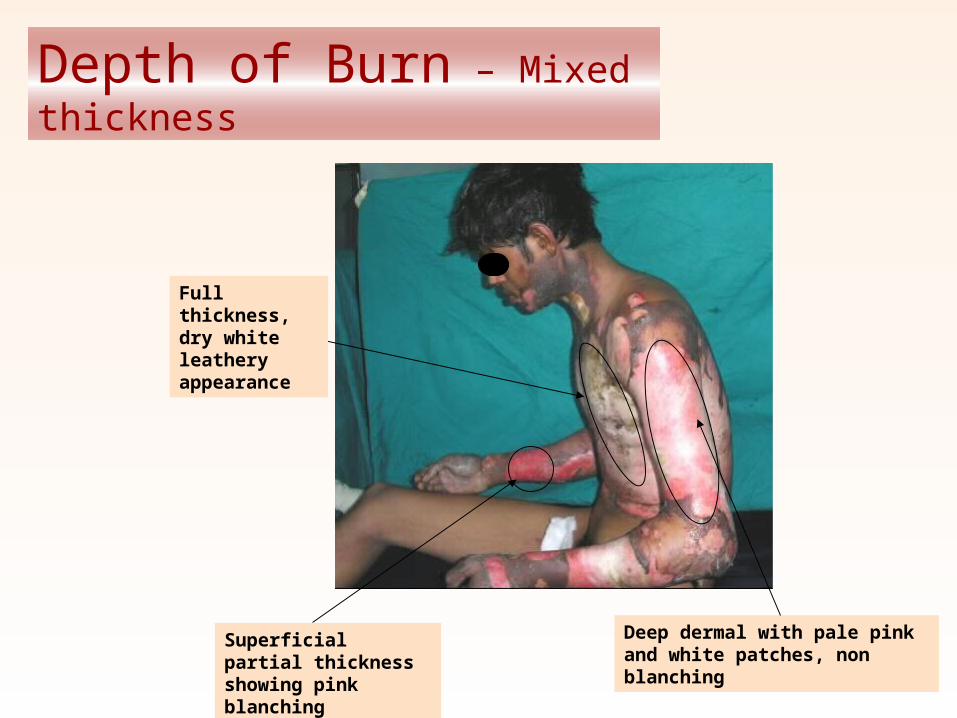
Depth of Burn – Mixed thickness
Deep dermal with pale pink and white patches, non blanching
Superficial partial thickness showing pink blanching
Full thickness, dry white leathery appearance
Classifying the patient…
* First you should assess the severity of the burn injury according to– TBSA– depth– position– presence of infection– time since the burn– presence or absence of inhalation injury
* Combine this information with patient factors:– age – associated injuries– other medical problems– nutritional status
* Finally consider social and family factors to classify the patient according to how and where to provide treatment.
Remember…
• All Burn Patients are “Trauma Patients”, first!
• Airway… Breathing… Circulation
• FLUIDS – FLUIDS – FLUIDS– Up to a point!........................How much fluid should be given?
– Pain Control!!
– Dressings: keep the wounds clean & dry!
– Transfer to the UNM Burn Center (criteria) Remember the Tetanus Shot!
Fluids… a guide
• Classic Parkland Formula
4cc per % TBSA BURNED per Kg
½ given over the first 8 hrs
Remaining ½ given over the next 16 hrs
Type of Fluid: LR
Inhalation Injury: INCREASE Rate to 6cc per % per kg!
ABA Transfer Criteria• 1. Partial thickness burns greater than 10 % total body surface area (TBSA)
• 2. Burns that involve the face, hands, feet, genitalia, perineum, or major joints
• 3. Third-degree burns of any size and any age group
• 4. Electrical burns, including lightning injury
• 5. Chemical burns
• 6. Inhalation injury
• 7. Burn injury in patients with preexisting medical disorders that could complicate management, prolong recovery, or affect mortality
• 8. Any patient with burns and concomitant trauma (such as fractures) in which the burn injury poses the greatest risk of morbidity or mortality. In such cases, if the trauma poses the greater immediate risk, the patient may be initially stabilized in a trauma center before being transferred to a burn unit. Physician judgment will be necessary in such situations and should be in concert with the regional medical control plan and triage protocols
• 9. Burned children in hospitals without qualified personnel or equipment for the care of children
• 10. Burn injury in patients who will require special social, emotional and/or long-term rehabilitative interventions.
Questions…
one child burned, is one child too many!
Bradley J. Phillips, MD
UNM Burn CenterAdults & Pediatrics
from tragedy… hope!
The New Mexico Burn Corps
Call 1-888-UNM-PALS to join our TEAM!
We need active VOLUNTEERS from all ages to help us meet the needs of New Mexico!
Bradley J. Phillips, MD