Embed Size (px)
Citation preview

BUREAU OF BUSINESS AND ECONOMIC RESEARCHU N I V E R S I T Y O F M O N TA N A
THE ECONOMIC IMPACT OF MEDICAID EXPANSION IN MONTANA: UPDATED FINDINGS
BRYCE WARD & BRANDON BRIDGEJANUARY 2019
The Montana Healthcare Foundation and Headwaters Foundation


Acknowledgements
ThisreportwasauthoredbyBryceWardoftheUniversityofMontanaandABMJConsulting
andBrandonBridgeoftheUniversityofMontana’sBureauofBusinessandEconomic
Research.Allstatementsandconclusionsincludedinthisreportbelongtotheauthorsand
donotrepresentthepositionoftheUniversityofMontana.
Wewouldliketothankthefollowingpartnersforsupportingthisresearch:
Formoreinformation,contact:BryceWard
[email protected]@mso.umt.edu
ABMJConsulting
(406)219-0694
www.abmjconsulting.com
BrandonBridge
BureauofBusinessandEconomicResearch
GallagherBusinessBuilding,Suite231
Missoula,MT59812
(406)543-5113
www.bber.umt.edu

TableofContents
Abstract.....................................................................................................................................................0
I.Summary................................................................................................................................................1
II.Background..........................................................................................................................................4
III.REMIModel........................................................................................................................................7A.Directimpacts...............................................................................................................................................................7
B.Statewideresults.......................................................................................................................................................11
C.ByRegion......................................................................................................................................................................12
IV.Empiricalestimates.........................................................................................................................13
V.OtherEconomicEffectsofMedicaidExpansion..........................................................................17A.Healthcareaccessandhealthoutcomes........................................................................................................17
B.Financialsecurity.......................................................................................................................................................19
C.Crime..............................................................................................................................................................................19
D.Employment................................................................................................................................................................19
F.Healthcaresector.....................................................................................................................................................21
VI.FiscalEffects......................................................................................................................................24
VII.Conclusion........................................................................................................................................26
Appendix.................................................................................................................................................28A.Selectingcomparisonstates.................................................................................................................................28
B.DirecteffectsforREMImodel..............................................................................................................................29
C.Resultsfromalternativespecifications............................................................................................................39
D.Differences-in-DifferencesModel......................................................................................................................39
E.ImpactofMedicaidExpansion/HELP-LinkonLaborForceParticipation.............................................42
F.ImpactofMedicaidexpansiononhealthcaresector.................................................................................44
G.ANoteonWoodworkEffects...............................................................................................................................47

Abstract
MedicaidexpansionhasasubstantialeffectonMontana’seconomy.Eachyear,
expansionbringsover$600millionintoMontanathatwouldnototherwisebehere.This
moneyripplesthroughMontana’seconomy,generatingbetween5,900and7,500,jobsand
between$350-$385millioninpersonalincomeeachyearbetween2018and2020.These
resultsareconsistentwiththeobservedchangeineconomicactivityinotherexpansion
statesthatexperiencedchangesinMedicaidcoverageanduninsurancesimilartoMontana.
Inadditiontogeneratingeconomicactivity,Medicaidexpansionappearstoimprovea
varietyofotheroutcomes—reducingcrime,improvinghealth,loweringdebt,andcreating
amorerobusthealthcaresector.Whilethestatepaysanominalamountforthesebenefits,
thecoststothestatebudgetaremorethanoffsetbythesavingscreatedbyMedicaid
expansionandbytherevenuesassociatedwithincreasedeconomicactivity.

TheEconomicImpactofMedicaidExpansioninMontana
1
I.Summary
Inthisreport,weupdateandreplaceourApril2018reportontheeconomicimpactsof
MedicaidexpansiononMontana’seconomy.ThisreportusesmorerecentdataonMedicaid
expansionenrollmentandspending,insurancecoverage,andemployment.Whilewe
employnewdataandanalysis,wereachthesameconclusion:MedicaidexpansionhasasubstantialimpactonMontana’seconomy.1
Aneconomicimpactstudydescribeshowmanyjobsandhowmuchincomestemsfrom
Medicaidexpansion.Ouranalysiscoverstheperiodfrom2016to2020.Assuch,italso
implicitlyanswersthequestion:“HowwouldfailingtorenewMedicaidexpansionin2019
impactMontana’seconomy?”
MedicaidexpansioninMontana—createdbytheHELPACTof2015—infusesa
significantamountofmoneyintothestate’seconomy.Duringitsfirsttwoandahalfyears,
Medicaidexpansionprovidedbeneficiarieswithnearly$1.4billionofhealthcare.The
federalgovernmentpaidformostofthis,andmostofthesefederaldollarswouldnothave
beenspentinMontanawithoutMedicaidexpansion.Approximately85percentofMedicaid
spendingrepresentsnewmoneyinMontana.Thismeansthattheannualinfusionofnew
moneyintoMontana’seconomyisslightlybiggerthantheeconomiesinDawsonandBig
HornCountiesandslightlysmallerthantheeconomiesinStillwaterandLakeCounties.2
MedicaidexpansionspendingentersMontana’seconomyintwoways.First,itsupports
newhealthcarespending.NearlyoneintenMontananswasenrolledinMedicaid
expansionasofOctober2018.Mostexpansionenrolleeswouldhavebeenuninsuredinthe
absenceoftheexpansion.Assuch,Medicaidexpansionprovidestensofthousandsof
uninsured,underinsured,andlow-incomeMontananswithhealthcaretheywouldnot
otherwisereceive.Second,Medicaidexpansionspendingreplacesexistingspending.Even
withoutMedicaidexpansion,beneficiarieswouldhavereceivedsomehealthcare.Medicaid
expansionchangeswhopaysforthishealthcare.Withoutexpansion,thestate,thefederal
government,employers,providers,andthebeneficiariesthemselvesallpaidforsomeof
thecarethatisnowpaidviaMedicaid.Withexpansion,thefederalgovernmentpaysfor
nearlyallexpansionbeneficiaries’healthcare.
1WeincludeasummaryofthedifferencesbetweenthisreportandourpriorreportinAppendixH.2TheBureauofEconomicAnalysisrecentlyreleasedGDPestimatesforcounties.AccordingtotheseestimatestheGDPsofDawson,BigHorn,Stillwater,andLakeCountieswere$523million,$546million,$661million,and$685millionrespectivelyin2015(in$2018).WeestimatethatMedicaidexpansionwillinfuseover$600millioninnewmoneyintoMontana’seconomyeachyearbetween2018and2020.

TheEconomicImpactofMedicaidExpansioninMontana
2
Asaresult,Medicaidexpansionstimulateseconomicactivity.Weestimatethatitwill
generatebetween5,900and7,500jobsandbetween$350-$385millioninpersonalincome
annuallybetween2018and2020(seeTable1).Thisrepresentsapproximatelyonepercent
ofMontana’stotalemploymentandincome.Duringitsfirstfiveyears,Medicaidexpansion
isexpectedtogenerateapproximately$1.6billioninpersonalincomeand$2.1billionin
grossdomesticproduct.
Table1:SummaryofEconomicImpactsofMedicaidExpansioninMontana/YearandCumulative(incomeandsalesinmillionsof2018dollars) 2016 2017 2018 2019 2020 Cumulative
Jobs 3,456 6,537 7,442 6,874 5,906 PersonalIncome $168 $325 $385 $377 $348 $1,603GDP $229 $440 $509 $478 $420 $2,076Population 1,066 2,768 4,334 5,376 5,990
Notes:DetailsforthisanalysisinSectionIIIandAppendixB.
Theseresultsareconsistentwiththeresultsfromanewdifferences-in-differences
analysisoftheeffectsofMedicaidexpansiononstates’economies.Adifferences-in-
differencesanalysiscomparesthechangeinoutcomesinexpansionstatestothechangein
outcomesinnon-expansionstates.Weuseasubsetofexpansionstatesinthisanalysis.
Specifically,weincludestateswhereMedicaidexpansionledtolargechangesinMedicaid
coverageanduninsurance,similartoMontana.Wefindthat,onaverage,Medicaid
expansionincreasesthesizeofastate’shealthcaresectorbyapproximatelythree
percentagepointsthreetofouryearsafterexpansion.Furthermore,consistentwiththe
resultsinTable1,wefindthatMedicaidexpansionisassociatedwithaonepercentage
pointincreaseintotalemployment.
TheeconomicimpactsofMedicaidexpansionarenotlimitedtothejobsandincomeit
supports.MedicaidexpansionalsorepresentsasignificantinvestmentinMontanans’
healthandwell-being,andtheseinvestmentspayoff.Asubstantialbodyofresearchfrom
aroundtheU.S.hasevaluatedtheeffectsofMedicaidexpansionandfoundthatit:
• Improveshealth.OnestudyfoundthatMedicaidexpansionwasassociatedwitha5.1percentagepointincreaseintheshareoflow-incomeadultsin

TheEconomicImpactofMedicaidExpansioninMontana
3
excellenthealth.3Thisisconsistentwithalargerbodyofliteraturethatfinds
thatinsuranceexpansionsimprovementalhealthandreducemortality.4
• Improvesfinancialhealth.Forinstance,onerecentstudyfoundthatMedicaidexpansionreducedmedicaldebtby$900pertreatedperson,prevented50,000
bankruptcies,andledtobettercredittermsforborrowers.5
• Reducescrime.Medicaidexpansionreducedcrimebymorethanthreepercent,generatingsocialbenefitsworthmorethan$10-$13billionannually.6
• Makesthehealthcaresectormorerobust,particularlyinruralareas.Medicaidexpansionledtodramaticreductionsinuncompensatedcareand
improvementinprovideroperatingmargins,particularlyamonghospitalsin
ruralareas.
Furthermore,Medicaidexpansion,alongwiththeassociatedHELP-Linkworkforce
developmentprogram,mayhaveimprovedlabormarketoutcomesforlow-income
Montanans.Followingexpansion,laborforceparticipationamonglow-income
Montanans—ages18-64—increasedbyfourtosixpercentagepointsrelativetothechange
amongthesamepopulationinotherstatesorrelativetothechangeamonghigher-income
Montanans.ThissuggeststhatMedicaidexpansionandHELP-Linkimprovedlabormarket
outcomesforlow-incomeMontanans.
WhileMontanapayspartofthecostofMedicaidexpansion,thesecostsaremorethan
offsetbycostsavingsandincreasedrevenues.Medicaidexpansionhasallowedsome
peopletoswitchfromtraditionalMedicaidtotheexpansion.BecauseMontanapays35
percentofthecostfortraditionalMedicaidbutlessthantenpercentintheexpansion,this
hassavedthestatemorethan$50millionduringthefirsttwoandahalfyears.Medicaid
expansionalsosavedapproximately$3millionperyearbyreducingthecostofinmate
3Sommers,B.D.,Maylone,B.,Blendon,R.J.,Orav,E.J.,andEpstein,A.M.,“Three-YearImpactsoftheAffordableCareAct:ImprovedMedicalCareandHealthAmongLow-IncomeAdults,”HealthAffairs36,no.6(June1,2017):1119-1128.4Sommers,B.D.,Gawande,A.A.,andBaicker,K.,“HealthInsuranceCoverageandHealth—WhattheRecentEvidenceTellsUs,”NewEnglandJournalofMedicine377,no.6(August10,2017).5Brevoort,K.,Grodzicki,D.,andHackmann,M.B.,MedicaidandFinancialHealth(No.w24002),NationalBureauofEconomicResearch(2017);Hu,L.,Kaestner,R.,Mazumder,B.,Miller,S.,andWong,A.TheEffectofthePatientProtectionandAffordableCareActMedicaidExpansionsonFinancialWellbeing(No.w22170),NationalBureauofEconomicResearch(2016).6Vogler,J.,“AccesstoHealthCareandCriminalBehavior:Short-RunEvidenceFromtheACAMedicaidExpansions,”(November14,2017);He,Q.,“TheEffectofHealthInsuranceonCrime:EvidenceFromtheAffordableCareActMedicaidExpansion,”(2017).Foranexpansiverecentbibliographysee:Antonisse,L.,Garfield,R.,Rudowitz,R.,andArtiga,S.,“TheEffectsofMedicaidExpansionUndertheACA:UpdatedFindingsfromaLiteratureReview,”(2017).

TheEconomicImpactofMedicaidExpansioninMontana
4
care7,andanadditional$3millionperyearinreducedspendingonmentalhealthand
substanceabusetreatment.Italsobenefitsstatecoffersbyincreasingeconomicactivity
andstaterevenues.AsshowninTable2,costsavingsandincreasedrevenuemorethan
offsetexpansioncosts.Thiswillremaintrueevenafterthestate'sshareofMedicaid
expansioncostsrisestotenpercentin2020.
Table2:FiscalEffectsofMedicaidExpansioninMontana/Year(inmillionsof2018dollars) 2016 2017 2018 2019 2020NetcostofexpansiontoMT(cost–savings–premiums)
-$10.2 -$5.3 $3.3 $10.7 $20.4
EstimatedtaxrevenuesbasedestimatesinTable1
$13.7 $26.4 $30.5 $28.7 $25.2
Neteffectonstatebudget $23.9 $31.7 $27.2 $18.0 $4.8Notes:DetailsforthisanalysisinSectionVI.
II.Background
In2015,MontanapassedtheHELPAct,whichexpandedMedicaidundertheAffordable
CareAct(“ACA”).Startingin2016,Montananswithincomesbelow138percentofthe
FederalPovertyLevel(“FPL”)couldenrollinMedicaid,andthefederalgovernmentwould
payformostofthecosts.Specifically,thefederalgovernmentpaid100percentofcostsfor
eligibleenrolleesin2016and95percentin2017.Itwillpay94percentin2018,93percent
in2019,and90percentin2020andbeyond.8
TheHELPActaddedsomeprovisionstothetypicalMedicaidexpansion.Forinstance,it
requiredenrolleestopaypremiumsandmakeco-paymentsforsomeservices,and
enrolleesmaybedisenrollediftheyfailtopaytheirpremiums.Italsoincluded12-month
continuouseligibility,whichallowsenrolleestomaintainMedicaidcoverageforuptoone
year,regardlessofchangestoincomeorfamilystatus.Additionally,theHELPAct
authorizedaworkforcedevelopmentprogram(HELP-Link)toimproveemployment
outcomesforMedicaidexpansionbeneficiaries.
7Pre-MedicaidexpansionannualoutsidemedicalcostsfortheDepartmentofCorrectionstotaled$8.3million.Afterexpansion,theytotaled$5.5million.Thus,spendingforoutsidemedicalcarefellby$2.8million.8 ThesharepaidbythefederalgovernmentinMontanadiffersslightlyfromtheseamounts.InexchangeforallowingMontanatooffer12-monthcontinuouseligibility,thefederalgovernmentloweredtheshareitpaysbylessthanonepercentagepoint.However,someofthisisoffsetbythefactthatthefederalgovernmentpaysfor100percentofcertaincosts(e.g.,IndianHealthServices).AccordingtoprojectionsbytheLegislativeFiscalDivisionthestatewillpay8.9percentofthetotalcostsofMedicaidexpansioninFY2021.https://leg.mt.gov/content/Publications/fiscal/BA-2021/2021BienniumVolume1_Final.pdf[accessedDecember22,2018]

TheEconomicImpactofMedicaidExpansioninMontana
5
Morethan40,000MontananshadenrolledinMedicaidthroughtheexpansionby
January2016,andenrollmentplateauedatapproximately96,000inMay2018.Medicaid
expansionspendingonbenefitsandclaimsinMontanawas$130millionduringFY2016
(whichcoveredJanuary-June2016),$558millioninFY2017,and$693millionduringFY
2018.Thus,duringitsfirsttwoandahalfyears,Medicaidexpansionspendingonbenefits
andclaimstotalednearly$1.4billion.
ThisreportcomputestheeconomicimpactsgeneratedbyMedicaidexpansion.An
economicimpactanalysisisappropriatetostudyMedicaidexpansionbecause,from
Montana’sperspective,thedecisiontoexpandMedicaidbringsfederaldollarsintothestate
thatarenotoffsetbyincreasedpaymentstothefederalgovernment.9Thatis,when
MontanaagreedtoexpandMedicaid,thefederalgovernmentdidnotimposeaspecialtax
onMontananstopayforthecostsoftheexpansioninMontana.Statesthatdonotexpand
Medicaiddonotreceiveaspecialtaxbreakorgrantequaltotheamountoffederal
Medicaiddollarsforegone.Thus,atthemargin,thedecisiontoexpandMedicaidis,inpart,
adecisiontobringasubstantialamountofmoney(andtheassociatedeconomicactivity)
intoMontana’seconomy.
Therearetwowaystothinkaboutthemarginalcosttothefederalgovernmentthatis
associatedwithMontana’sdecisiontoexpandMedicaid.First,aswritten,theACAwaspaid
for;itraisedsufficientrevenuetopaytheexpectedcostsofexpandingMedicaidinall50
states.Assuch,onecouldarguethatthemarginalcostsassociatedwithMontanaexpanding
Medicaidarezero.Thefederalgovernmentdoesnotneedtoraiseanyadditionalfunds
fromMontanansorotherstopayforthecostofMontana’sexpansion.Alternatively,ifone
viewsMontana’sMedicaidexpansionasamarginalfederalexpenditurethatmustbeoffset
atsomepointwithhigherfederalrevenues,theincreasedrevenuerequiredtopayfor
Montana’sexpansionwillbepassedontoallAmericans.GiventhatMontanansprovideless
thanonepercentoffederalrevenues,morethan99percentofthefederalmarginalcosts
associatedwithMontana’sMedicaidexpansionarepassedontotaxpayersinotherstates.
Thus,thetotalmarginalcosttoMontanansassociatedwiththedecisiontoexpandMedicaid
islimitedtothesharepaiddirectlybythestateplus,atmost,Montana’sshareofallfederal
revenues.
9AlargeamountofliteratureestablishesthatMedicaidexpansionspendinggeneratesamarginalincreaseineconomicactivitythatcanbeevaluatedusinganeconomicimpactanalysis.See,forinstance,Ayanian,J.Z.,Ehrlich,G.M.,Grimes,D.R.,andLevy,H.,“EconomicEffectsofMedicaidExpansioninMichigan,”NewEnglandJournalofMedicine376,no.5(2017):407-410;DeloitteDevelopmentLLC.MedicaidExpansionReport:2014.CommonwealthofKentucky(2015);Chernow,M.,“TheEconomicsofMedicaidExpansion,”(2016)https://www.healthaffairs.org/do/10.1377/hblog20160321.054035/full/;Brown,etal.,“AssessingtheEconomicandBudgetaryImpactofMedicaidExpansioninColorado,”(2016).

TheEconomicImpactofMedicaidExpansioninMontana
6
SomehavearguedthatMedicaidexpansioncannotgenerateeconomicimpactsand
boosteconomicgrowth.10Thisargumentisrootedinthenotionthathealthcareispartof
thelocal(ornon-traded)sector.Demandforlocalsectorindustriescomesfromlocal
residents.Therefore,growthinthelocalsectorreflectsgrowthinthebroadereconomy.It
isnotacauseofit.Whilethislogicmayapplytopartsofhealthcare,itdoesnotapplyto
Medicaidexpansion.ThebulkofthemoneythatpaysforMedicaidexpansioncomesfrom
outsideofMontana.Assuch,theimpactofMedicaidexpansiononMontana’seconomyis
similartoanewfactoryoranewgovernmentcontract.Medicaidexpansionbringsmoney
intoMontana’seconomythatwouldnototherwisebehere,andthismoneyripplesthrough
thestate’seconomycreatingjobsandincome.
ToestimatetheeconomicimpactofMedicaidexpansion,weneedtocomparewhathas
happened(andwhatisforecasttohappen)withexpansiontowhatlikelywouldhave
happenedinitsabsence.Ofcourse,wedonotobservewhatwouldhavehappenedhad
MontananotexpandedMedicaid.Thisworldmustbeconstructedusingstatisticalanalyses
andassumptions.
WeusetwomethodstoidentifytheimpactofMedicaidexpansiononMontana’s
economy.First,weusetheREMImodel,aneconomicmodelcalibratedtorepresentthe
interactionsinMontana'seconomy,leasedfromRegionalEconomicModels,Inc.Usingthe
modelwecomputeabaselinemodelofMontana’seconomywithoutMedicaidexpansion.
Then,wecomputethesamemodeladdingMedicaidexpansion.Theeconomicimpactof
Medicaidexpansionisthedifferencebetweenthesetwoscenarios.
Second,weuseastatisticalapproachtoestimatetheeffectofMedicaidexpansionon
thehealthcaresector(wherethebulkoftheeconomicimpactsaregenerated)andthe
wholeeconomy.Thestatisticalapproachweemploy(calledadifferences-in-differences
analysis)comparesthechangeinoutcome(e.g.,healthcareemployment)instatesthat
expandedMedicaidtothechangeinoutcomeinstatesthatdidnot.Ifthechangein
outcomeislarger(orsmaller)inexpansionstatesrelativetonon-expansionstates,this
differenceplausiblyreflectstheeffectsofMedicaidexpansion.
10Seeforinstance,commentsprovidedbytheMontanaPolicyInstitutetotheChildrenandFamilyInterimCommitteeinMay2018.

TheEconomicImpactofMedicaidExpansioninMontana
7
III.REMIModel
First,wecalculatetheimpactofMedicaidexpansionusingtheREMImodel.TheREMI
modelisaneconomicmodelcalibratedtorepresenttheinteractionsintheMontana
economy.TheREMImodelisoneofthebestknownandmostrespectedanalyticaltoolsin
thepolicyanalysisarena,andhasbeenusedinmorethan100previousstudiesaswellas
dozensofpeer-reviewedarticlesinscholarlyjournals.Itisastate-of-the-arteconometric
forecastingmodelthatincorporatesdynamicfeedbacksbetweeneconomicand
demographicvariables.TheREMImodelforecastsemployment,income,expenditures,and
populationsforcountiesandregionsbasedonamodelcontainingmorethan100
stochasticanddynamicrelationshipsaswellasanumberofidentities.11
A.Directimpacts
TocompletetheREMImodel,wefirstestimatethedirectimpactsoftheMedicaid
expansion.Thatis,wedeterminehowmuchmoneygetsaddedorsubtractedfromvarious
partsoftheeconomyasadirectresultofexpansion.
Inthissection,webrieflyoutlinetheassumptionsusedtoquantifythedirectimpactsof
Medicaidexpansion.Amorecompletedescriptionofourassumptionsandtheir
justificationsareincludedinAppendixA-C.
Thedirectimpactsofexpansionstemfromthethreemajorchangesitcauses:
(1) MedicaidexpansionincreasesMedicaidcoverageandreducesuninsuranceandotherformsofcoverage;
(2) Medicaidexpansionincreaseslow-incomeMontanans’healthcarespending;and(3) Medicaidexpansionshiftswhopaysforthebulkoflow-incomeMontanans’health
carefromavarietyoflargelyMontana-basedsourcestothefederalgovernment.
Morespecifically,Medicaidexpansion:
(a) IncreasestotalspendingonhealthcareinMontanabyincreasinghealthcareconsumptionandreducinguncompensatedcare;
11Afullexplanationofthedesignandoperationofthemodelcanbefoundin:Treyz,G.I.,Rickman,D.S.,&Shao,G.(1991).TheREMIeconomic-demographicforecastingandsimulationmodel.InternationalRegionalScienceReview,14(3),221-253.

TheEconomicImpactofMedicaidExpansioninMontana
8
(b) IncreasesfederalgovernmentspendinginMontanabyanamountequaltothefederalshareofexpansionspendingminusthechangeinfederalspendingonother
programsliketraditionalMedicaidorexchangesubsidies;
(c) Increasesstategovernmentspendingbyanamountequaltothestateshareofexpansioncosts(includingadministrationcosts)minusthechangeinspendingon
otherprogramsliketraditionalMedicaid,correctionshealthcare,andother
programsthatprovidehealthcareforlow-incomepopulations;
(d) Reducesindividuals’(orhouseholds’)healthcarespendingbyanamountequaltotheirspendingonMedicaidexpansionpremiumsandout-of-pocketcostsminus
whattheywouldhavespentonpremiumsandout-of-pocketscostswithout
expansion(individual/householdspendingonothergoodsandservicesthen
increasesbyaproportionalamount);12,13and
(e) Reducesemployers’healthcarespendingbyantheamounttheyspendonhealthinsurancepremiumswithexpansionminuswhattheywouldhavespentinthe
absenceofexpansion(ownerand/orworkerincomeincreasesbyanequal
amount).14,15,
TheneteffectofthesechangesisalargeinfusionofnewmoneyintoMontana’seconomy.
ThesearethedirecteffectsofMedicaidexpansion.
Thereareavarietyofdirecteffectsofexpansionthatwedonotincludeinthemodel.
Forinstance,anewreportfromtheMontanaDepartmentofRevenueandtheMontana
DepartmentofLaborandIndustriessuggeststhatMedicaidexpansionallowedMontana
businesstoavoid$11.1-16.7milliondollarsofpenaltiesrelatedtotheACA’semployer
mandate.16Wedonotincludetheseeffectsintheanalysis.Similarly,wedonotincludethe
effectthatindividualswithbettercredit/lessdebtcouldhaveonMontana’seconomyor
individualmandatepenalties(whiletheyapplied).Theseomissionsmayleadustoslightly
understateexpansion’simpacts.
12TheimpactofMedicaidexpansiononthestateandfederalgovernmentisfurtheroffsetbytheamountofconsumptiontaxespaidonthisspending.13Thenetchangeinindividual/householdspendingmaybefurtherreducedifthefederalorstategovernmentlevytaxesonMontananstopayforincreasedspendingduetoexpansion;however,individual/householdspendingmayincreaseasaresultoflowerdebtandimprovedcredit.14Sinceemployerpaymentsforhealthinsurancepremiumsareuntaxed,theimpactofMedicaidexpansiononthestateandfederalgovernmentisfurtheroffsetbytheamountofincometaxespaidonthisincome.15Thenetchangeinemployer/workerspendingmaybefurtherreducedifthefederalorstategovernmentlevytaxesonMontananstopayforincreasedspendingduetoexpansion.16http://lmi.mt.gov/Portals/193/Publications/LMI-Pubs/Special%20Reports%20and%20Studies/MT-Medicaid_Report.pdf[accessedJanuary8,2019]

TheEconomicImpactofMedicaidExpansioninMontana
9
InAppendixB,wedetailourassumptionsforeachoftheseeffects.Inbrief,
approximately85percentofMedicaidexpansionspendingwouldnotbespentin
Montana’seconomywithoutexpansion.
Between48-60percentofMedicaidspendingpaysfornewhealthcareservices.This
spendingincludesdoctor’svisitsandtreatmentsthatwouldnotoccurintheabsenceof
Medicaidexpansion.Italsoincludesreductionsinuncompensatedcare.17
TheremainingspendingistransferredtothosethatwouldhavepaidMedicaid
expansionbeneficiaries’carewithoutexpansion.Withoutexpansion,someexpansion
beneficiarieswouldhaveenrolledintraditionalMedicaid.Thestateandfederal
governmentswouldhavepaidforthiscare.Somewouldhaveenrolledinanindividual
insuranceplan(e.g.,anexchangeplan).Thefederalgovernment(viaexchangesubsidies,
forthosewhoqualify18)andtheindividuals(viapremiumsandout-of-pocketpayments)
wouldhavepaidforthiscare.Somewouldhaveobtainedinsuranceviatheiremployer.The
employer(viatheemployer’sshareofpremiumcosts)andtheemployee(viathe
employee’sshareofpremiumsandout-of-pocketpayments)wouldhavepaidforthiscare.
Forinstance,anuninsuredindividualwhomayhavespent$1,700out-of-pocketon
healthcareintheabsenceofexpansioncanstillconsumethiscarewithexpansion.
However,thefederalgovernmentpaysformostofthiscare.The$1,700stayswiththe
individualandcanbespentonotheritems.Similarly,foranindividualwhowouldhavehad
employercoveragewithemployerpremiumsof$5,600,employeecontributionsof$1,100,
andout-of-pocketspendingof$800,Medicaidexpansionallowstheemployertoredirect
$5,600tootherthings(includingproprietorincomeorworkerincome)andallowsthe
individualtoredirectmostofthe$1,900dollarstowardothergoodsandservices.19
Table3summarizesonescenarioforhowMedicaidexpansiondirectlyimpacts
Montana’seconomyin2020.20Weestimatethatexpansionincreasesnetfederalspending
inMontanabyapproximately$617million.Netstatespendingwillincreaseby
approximately$20million.Individualspendingonhealthcarewillfall(andspendingon
17Weincludeuncompensatedcareas“new”spendingbecauseuncompensatedcareabsorbedbyprovidersisnotcountedinhealthcareexpendituredata.Assuch,fromtheperspectiveoftheREMImodel,thisisnewspending.18Individualswithincomesbetween100percentand138percentoftheFPLareeligibleforexchangesubsidiesandcost-sharingreduction(“CSRs”)instatesthathavenotexpandedMedicaid.19InMontana,expansionbeneficiariesmaystillpaysomeamounttowardpremiumsandout-of-pocketcosts.20AsdiscussedintheAppendixC,givenuncertaintyaboutdifferentassumptions,weexplorearangeofoutcomes.Thisexamplecorrespondstooneillustrativescenario.Otherscenariosdifferslightly.

TheEconomicImpactofMedicaidExpansioninMontana
10
othergoodsandserviceswillincrease)byroughly$185million.Employerspendingon
healthcarewillfall(andproprietorand/oremployeeincomewillincrease)by$93million.
Table3:IllustrativeestimatesformaincomponentsofthedirecteffectsofMedicaidexpansion($millions) Spending
2020Totalfederalspendingonexpansion $682
Reductionsinfederalspendingduetoexpansion(e.g.,traditionalMedicaid,exchangesubsidies)
-$60
FederalshareofHELPpremiums -$5Netchangefederalspending $617Totalstatespendingonexpansion $58
Reductionsinstatespendingduetoexpansion -$43StateshareofHELPpremiums -$0.4
Netchangestatespending $20Individualspendingtopayforexpansion(e.g.,premiums) $5.5
Reductionsinindividualspending(e.g.,insurancepremiumsandout-of-pocketspending)
-$191
Netchangeinindividualspending -$185Employerspendingtopayforexpansion -
Reductionsinspendingemployerspending(e.g.,premiums) -93Netchangeinemployerspending -93
TocomputetheeconomicimpactsofMedicaidexpansion,weinputsimilarvaluesinto
theREMImodeltoestimatehowMontana’seconomywoulddifferwithoutthesechanges.
Weallocatethesedirectimpactsacrossproviders,government,business,andindividuals
asdescribedabove.Newspendingonhealthcareisallocatedacrosshealthcaresectorsin
proportiontoreportedMedicaidexpansionspending.21Wefurtherallocatespending
acrossMontanaregionsinproportiontoMedicaidenrollment.22
Weestimateimpactsusingthefollowingprocess.First,abaselineprojectionofthe
economyisproducedusingtheREMImodel,utilizinginputsandassumptionsthat
extrapolategrowthandconditionsofrecenthistoryintheabsenceofMedicaidexpansion.
Themodelisthenusedasecondtimewithidenticalinputs,exceptthatMedicaidexpansion
isadded.Thus,Medicaidexpansionproducesadifferenteconomy,reflectingnotonlythe
expansion,butalsohowtherestoftheeconomyreactstoit.Thedifferencebetweenthe
21http://dphhs.mt.gov/Portals/85/Documents/healthcare/MedicaidExpansionHealthCareServicesProfile.pdf22WeallocateMedicaidenrollmentbycountyintothefiveregionsavailableintheREMImodel.http://dphhs.mt.gov/Portals/85/Documents/healthcare/MedicaidExpansionMemberProfile.pdf

TheEconomicImpactofMedicaidExpansioninMontana
11
baselineandalternativescenariosoftheeconomyrepresentstheeconomicimpactof
Medicaidexpansion.
B.Statewideresults
Table4presentsthestatewideeffectsofMedicaidexpansion.23Undertheconditions
andassumptionsoutlined,weestimatethatMedicaidexpansionadded3,456jobs,$168
millioninpersonalincome,and$229millioninGDPtoMontana’seconomyin2016.We
projectthattheseeffectspeakedalongwithexpansionspendingin2018andwilldecline
somethrough2020.In2020,Medicaidexpansionisexpectedtosupport5,906jobs,$348
millioninpersonalincome,and$420millioninGDP.
Bytheendofitsfirstfiveyears,Medicaidexpansionisexpectedtocreateatotalof
about$1.6billioninpersonalincomeand$2.1billioninGDP.Weexcludejobsand
populationfromthecumulativetotalbecausetheyarenotadditiveacrossyears.They
representthedifferenceinemployment(orpopulation)relativetonoexpansionineach
year.24
Table4:SummaryofEconomicImpactsofMedicaidExpansioninMontana/YearandCumulative(incomeandsalesinmillionsof2018dollars) 2016 2017 2018 2019 2020 Cumulative
Totalexpansionspending $332 $693 $798 $759 $745
Jobs 3,456 6,537 7,442 6,874 5,906 PersonalIncome $168 $325 $385 $377 $348 $1,603GDP $229 $440 $509 $478 $420 $2,076Population 1,066 2,768 4,334 5,376 5,990
Notes:TotalexpansionspendingestimatesobtainedfromLFDbudgetestimates.WetranslateFYtoCYbased
onenrollmentatthetime.https://leg.mt.gov/content/Publications/fiscal/BA-
2021/2021BienniumVolume1_Final.pdf.
Table5showsthebreakdownofemploymentbyindustry.Asonemightexpect,the
largestimpactsareinhealthcare.OuranalysissuggeststhatMedicaidexpansionwill
createapproximately2,500additionalhealthcarejobs.However,therearealsosignificant
effectsonretailtrade(morethan1,000jobs)andconstruction(morethan600jobs).
23Theseresultsreflectone(fairlyconservative)setofplausibleassumptions.WepresentarangeofalternativesinAppendixC.24Ouranalysisdoesnotsaythattheexpansioncreates6,000jobsinoneyearandthenadifferentadditional6,000newjobsthenextyear.Manyofthejobsarecreatedinoneyearandthenpersist.Forinstance,anursingpositioncreatedasaresultofexpansionin2017thatpersiststhrough2020wouldbepartofthe(approximately)6,000in2020.

TheEconomicImpactofMedicaidExpansioninMontana
12
Table5:IndustryBreakdownofEmploymentImpacts 2016 2017 2018 2019 2020HealthCareandSocialAssistance
1,261 2,574 2,874 2,631 2,441
RetailTrade 596 1,193 1,354 1,257 1,140Construction 341 702 878 837 667AccommodationandFood 203 399 465 448 416OtherServices,ExceptPublicAdministration
201 386 424 380 332
Professional,Scientific,andTechnicalServices
105 207 243 232 206
RealEstateandRental 90 178 208 198 179AdministrativeandWasteManagementService
94 180 202 184 160
Other 565 718 794 707 365
C.ByRegion
Table6summarizestheeconomicimpactsofMedicaidexpansionacrossfiveMontana
regions:Northwest,Southwest,Central,NorthCentral,andEast.25Medicaidenrollment
doesnotdeviatethatmuchfrompopulation.Assuch,economicimpactsacrossregionsare
somewhatproportionaltopopulation.
25TheNorthwestregionincludesFlathead,Granite,Lake,Lincoln,Mineral,Missoula,Powell,Ravalli,andSanderscounties.TheSouthwestregionincludesBeaverhead,Broadwater,DeerLodge,Gallatin,Jefferson,Madison,Meagher,Park,andSilverBowcounties.TheNorthCentralregionincludesBlaine,Cascade,Chouteau,Glacier,Hill,LewisandClark,Liberty,Pondera,Teton,andToolecounties.TheCentralregionincludesBigHorn,Carbon,Fergus,GoldenValley,JudithBasin,Musselshell,Petroleum,Stillwater,SweetGrass,Treasure,Wheatland,andYellowstonecounties.TheEastregionincludesCarter,Custer,Daniels,Dawson,Fallon,Garfield,McCone,Phillips,PowderRiver,Prairie,Richland,Rosebud,Sheridan,Valley,andWibauxcounties.

TheEconomicImpactofMedicaidExpansioninMontana
13
Table6:EconomicImpactsbyRegion,2019andCumulative2016-2020(incomeandsalesinmillionsof$2018) NW SW Central
2019 Cumul. 2019 Cumul. 2019 Cumul.Jobs 2,557 1,458 1,505 PersonalIncome $128 $549 $84 $356 $89 $378GDP $170 $735 $103 $447 $113 $488Population 1,859 1,207 1,208
N.Central East
2019 Cumul. 2019 Cumul.Jobs 1,033 321 PersonalIncome $56 $241 $19 $80GDP $72 $315 $21 $93Population 817 230
IV.Empiricalestimates
Inthissection,weestimatetheeconomicimpactofMedicaidexpansionusinga
differentapproach:adifferences-in-differencesanalysis.Thedifferences-in-differences
approachusesnon-expansionstatesasacontrolgroup,andprovidesananswertothe
question:“Howmuchdidthetrajectoryofeconomicactivitychangeinexpansionstates
relativetonon-expansionstatesafterexpansion?”
Thisstatisticalapproachprovidesawaytocheckthereasonablenessoftheresults
generatedbytheREMImodelandtheassumptionsthatunderlieit.Italsoprovidesan
independentestimateoftheeffectsofMedicaidexpansionthatrestsonfewerassumptions.
Specifically,ifoneassumesthatexpansionstatesandnon-expansionstateswouldhave
followedparalleltrendsintheabsenceofexpansion,thenthisapproachcalculatesthe
effectsofMedicaidexpansion.InAppendixD,weprovideevidencethatsuggeststhis
assumptionisreasonablefortheanalysesusedinthisreport.
TheimpactofMedicaidexpansionvarieswidelyacrossexpansionstates,evenonthe
outcomesmostdirectlyaffectedbyexpansion–e.g.,theshareofpeoplecoveredby
Medicaidortheshareuninsured.Insomeexpansionstates,theshareofpeoplewith
Medicaidbarelychangedfollowingexpansion.Inotherexpansionstates,itchanged
substantially.AvarietyoffactorsexplainthedifferencesinMedicaidexpansion’seffectson
healthinsurancecoverage(e.g.,somestateshadalreadyexpandedMedicaidcoverageto
childlessadultswithincomesatorabovethepovertyline).

TheEconomicImpactofMedicaidExpansioninMontana
14
Inthisreport,wefocusontheeconomicimpactofMedicaidexpansioninMontana,a
statewhereMedicaidexpansionhadalargeeffectonMedicaidenrollment.Assuch,we
limittheanalysistoincludestateswhoseMedicaidexpansionexperienceresembles
Montana’s.Specifically,wefocusonMedicaidexpansionstatesthatexperiencedlarge
changesintheshareoftheexpansioneligiblewithhealthinsuranceandlargechangesin
theshareoftheexpansioneligiblewithMedicaidafterACAimplementationin2014.The
expansionstatesincludedinouranalysisare:Alaska,Arkansas,California,Illinois,Indiana,
Kentucky,Louisiana,Michigan,Montana,Nevada,NewMexico,Oregon,RhodeIsland,
Washington,andWestVirginia.26Theaveragechangeininsurancecoverageinthesestates
betweenthepre-expansionperiod(2010-2013)and2017isroughlyequaltothechangein
Montana.WeprovideadditionaldetailsontheselectedstatesinAppendixA.
First,weexaminetheeffectofMedicaidexpansiononthehealthcaresector.We
presentresultsforthreedifferenthealthcaresectoroutcomes:healthcareemployment,
healthcarecompensation,andhealthcareGDP.Ourregressionsincludecontrolsforstate,
year,totalpopulation,populationoverage65,populationwithadisability,populationover
age25withatleastaBachelor’sdegree,andtotalemploymentinthetradedsector.27A
morecompletediscussionoftheseregressionsisavailableinAppendixC.
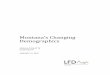
Figure1presentsthecoreresultsfromtheseanalyses.Theseresultsshowthat
Medicaidexpansionisassociatedwithsubstantialincreasesinthesizeofthehealthcare
sectorinthestatesexamined.Theresultsalsoshowthatexpansion’simpactsgrowover
thefirstfewyearsofexpansion.Forinstance,fouryearsafterexpansion,employment
growthinthehealthcaresectorwas3.2percentagepointslargerintheincludedexpansion
statesthaninthenon-expansionstates.Similarly,bythefourthyearofexpansion,the
growthintotalcompensationinthehealthcaresectorwas2.9percentagepointslarger
thaninnon-expansionstatesandgrowthinhealthcareGDPwas2.6percentagepoints
larger.
26Ourresultsdonotchangesubstantiallywhenusingmoreorlessrestrictivecriteriaforinclusion.27Thetradedsectoristhesetofindustriesthatprimarilyselltocustomersoutsidetheirlocalregion.Stateswithlargershockstotheirtradedsectorwillexperiencelargerchangesineconomicactivityandlargerchangesinhealthcareactivity.WedefinethetradedsectorusingtheresultsdescribedinJensen(2012).Specifically,wemultiplytotalemploymentineach2-digitNAICSindustryobtainedfromBEAregionaleconomicaccountsdatabythesharesreportedinJenson’sTable2.3andsumtoobtainanestimatefortotalemploymentinthetradedsector.

TheEconomicImpactofMedicaidExpansioninMontana
15
Figure1:AverageeffectofMedicaidexpansiononhealthcaresectorgrowthinincludedexpansionstatesbyyearssinceexpansion
Notes:Datapresentedarecoefficientsfromdifferences-in-differencesregressions;allregressionsinclude
stateandyearfixedeffectsandcontrolsforln(population),ln(populationwithadisability),ln(population
overage65),ln(populationoverage25withBachelor’sdegree),ln(totalemploymentintradedsector);all
regressionshave272observations.Allcoefficientsarestatisticallysignificantwithp<0.05,exceptunderlined
values.Theunderlinedcoefficientsaresignificantatp<0.06.
TheseresultsalignwiththeresultsfromtheREMImodelpresentedinSectionIII.
ApplyingtheseresultstoMontanasuggestsweshouldexpectMedicaidexpansiontocreate
anadditional2,500healthcarejobs.TheresultsfromtheREMImodelindicatethat
Medicaidexpansionwillincreasehealthcareemploymentby2,441jobsin2020.Similarly,
theseresultssuggestMedicaidexpansionwillincreasehealthcareearningsby
approximately$130million.TheREMImodelcalculatesthatMedicaidexpansionwill
increasehealthcareearningsby$160millionin2020.
Next,weexaminetheimpactofMedicaidexpansionontotalemployment.Table7
presentsresultsfromregressionswiththesamespecificationasabove.Theseresultsshow
thatMedicaidexpansionisassociatedwithsignificantincreasesintotalemployment.For
instance,thecoefficientof0.013inyear4indicatesthatgrowthintotalemploymentinthe
includedexpansionstateswas1.3percentagepointshigherthaninthenon-expansion
statesfouryearsafterexpansion.
1.9%
2.1%
2.8%
3.2%
1.1%
2.0%
3.0%2.9%
1.2%
1.9%
2.8%
2.6%
Year1 Year2 Year3 Year4
Employment
Compensation
GDP

TheEconomicImpactofMedicaidExpansioninMontana
16
Table7:Differences-in-differencesestimatesoftheeffectsofMedicaidexpansionontotalemploymentinincludedstates Ln(totalemp.) Ln(tradedsector
emp.)Ln(localsectoremp.)
Year1 0.004
(0.002)
-0.011
(0.007)
0.006
(0.004)
Year2 0.006+
(0.003)
-0.011
(0.009)
0.009+
(0.004)
Year3 0.009*
(0.004)
-0.002
(0.012)
0.014*
(0.006)
Year4 0.013**
(0.005)
-0.005
(0.012)
0.020*
(0.007)
Notes:Cluster-robuststandarderrorsclusteredonstateinparentheses,+p<0.10,*p<0.05,**p<0.01;all
regressionsincludestateandyearfixedeffectsandcontrolsforln(population),ln(populationwitha
disability),ln(populationoverage65),ln(populationoverage25withBachelor’sdegree),thefirstandthird
columnsincludethecontrolln(totalemploymentintradedsector);allregressionshave272observations.
Table7alsopresentsresultsthatexaminethetradedandnon-traded(local)sectors
separately.28Asdescribedabove,Medicaidexpansionincreasesdemandforhealthcareand
allowsindividualstoshiftmoneyfromhealthcaretootherconsumption.Assuch,any
increaseintotalemploymentattributabletoMedicaidexpansionshouldbedrivenby
increasesinthenon-traded(orlocal)sector.Medicaidexpansionshouldnotsubstantially
increaseactivityinlocalfactories,farms,etc.thatprimarilyselltonon-Montanans.
Consistentwiththishypothesis,therelationshipbetweenMedicaidexpansionandtraded
28Incontrasttothetradedsector,thenon-traded(orlocal)sectorconsistsprimarilyoffirmsandindustriesthatsellgoodsandservicestolocalconsumers.Bothtradedandlocalsectorentitiiesarevitaltoeconomichealth,buttheircontributiondiffers.Thetradedsectorisimportantprimarilybecauseitbringsmoneyintotheeconomyfromoutside.Thisoutsidespendingcirculatesthroughtheeconomysupportingadditionaljobsandincome.Thelocalsectorisimportantbecauseitprovidesthegoodsandservicesthatarenecessarytomakeaplaceadesirableplacetoliveandwork.Withoutagoodlocalsector,firmsandworkerswillnotwanttolocateinaregion.ForadditionaldiscussionofthedifferencesbetweenthetradedandlocalsectorsseeWard,B.etal(2012)TheTradedSectorinPortland’RegionalEconomy[https://studylib.net/doc/8135122/traded-sector-final]andWard,B.(2016)TheContributionofHealthCaretoFlatheadCounty’sEconomy[https://kalispellchamber.com/wp-content/uploads/2017/03/the-contribution-of-health-care-to-flathead-countys-economy-nov-2016.pdf]

TheEconomicImpactofMedicaidExpansioninMontana
17
sectoremploymentissmallandnotstatisticallysignificant,buttherelationshipbetween
expansionandlocalsectoremploymentispositiveandstatisticallysignificant.29
TheseresultssuggesttheMedicaidexpansionisassociatedwithslightlylargereffects
thanprojectedbytheREMImodelpresentedinSectionIII.A1.3percentagepointincrease
intotalemploymentinMontanaisover8,000jobs.TheREMImodelprojectedatotal
increaseof6,874jobsinthefourthyearofexpansion(equaltoapproximatelyonepercent
oftotalemployment).ThissuggeststhattheREMIresultspresentedinTable1maybe
conservative.30
V.OtherEconomicEffectsofMedicaidExpansion
Theresultsabovefocusoneconomicimpactsanddonotaccountformanyother
expansionbenefits.Inthissection,wehighlightafewadditionalfindingsfromthe
literatureandourownanalyses.TheKaiserFamilyFoundationhasregularlycompileda
summaryoftheeffectsofMedicaidexpansion.Themostrecentsummaryisavailableat:
https://www.kff.org/medicaid/issue-brief/the-effects-of-medicaid-expansion-under-the-
aca-updated-findings-from-a-literature-review-march-2018/
A.Healthcareaccessandhealthoutcomes
Medicaidexpansionimprovesaccesstohealthcareandmayimprovehealth.31For
instance,afterMedicaidexpansion,theshareoflow-incomeMontananswhoskippedcare
duetocostfellby21percent.Similarly,thesharewhohadnothadacheck-upwithinthe
pasttwoyearsfellby17percent(seeFigure2).Thesedatacoveronlythefirsttwoyearsof
MedicaidexpansioninMontana.AsimilaranalysisofstatesthatexpandedMedicaidin
2014showsthattheseeffectsgrowovertime.
29Healthcareispartofthelocalsector,butexcludinghealthcareemploymentfromtheregressiondoesnotsubstantiallychangetheresults.Forinstance,inyear4,excludinghealthcarefromlocalemploymentonlycausesthecoefficienttofallto0.018(p<0.03).30AnalternativeREMIspecificationthatassumesahigher(55percentinsteadof48percent)shareofMedicaidexpansionspendingisnew,generateshigheremploymentestimates(7,256inyear4),buttheseestimatesstillfallbelowtheempiricalestimates.31Sommers,B.D.,Maylone,B.,Blendon,R.J.,Orav,E.J.,andEpstein,A.M.,“Three-YearImpactsoftheAffordableCareAct:ImprovedMedicalCareandHealthAmongLow-IncomeAdults,”HealthAffairs36,no.6(2017):1119-1128;Mahendraratnam,N.,Dustbin,S.B.,andFarley,J.F.,“PrescriptionDrugUtilizationandReimbursementIncreasedFollowingStateMedicaidExpansionin2014,”JournalofManagedCare&SpecialtyPharmacy23,no.3(2017):355-363;Antonisse,L.,Garfield,R.,Rudowitz,R.,andArtiga,S.,“TheEffectsofMedicaidExpansionUndertheACA:UpdatedFindingsFromaLiteratureReview,”HealthAffairs35,no.10(2016):1810-1815.

TheEconomicImpactofMedicaidExpansioninMontana
18
Improvedhealthcareaccessmayimprovehealthoutcomes.Whilenoteverystudyhas
foundthatMedicaidexpansionimproveshealthoutcomesinitsfirstfewyears,manyhave.
Forinstance,onestudyfoundthatMedicaidexpansionwasassociatedwitha5.1
percentagepoint(or23percent)increaseintheshareoflow-incomeadultsinexcellent
health.32AdifferentstudyfoundthatMedicaidexpansionwasassociatedwithareduction
inthenumberofpoorhealthdaysanddepressiondiagnosisamongadultswithchronic
conditions.33Analysesofotherinsuranceexpansionshavefoundthatprovidinghealth
insuranceimprovesdepressionoutcomesandreducesmortality.34
Figure2:ChangeinHealthCareAccessAmongLow-IncomeMontanansBeforeandAfterMedicaidExpansion
Source:Authors’analysisof2015-2017BehavioralRiskFactorSurveillanceSystemdata.
32Sommers,B.D.,Maylone,B.,Blendon,R.J.,Orav,E.J.,andEpstein,A.M.,“Three-YearImpactsoftheAffordableCareAct:ImprovedMedicalCareandHealthAmongLow-IncomeAdults,”HealthAffairs36,no.6(2017):1119-1128.33Winkelman,T.N.,&Chang,V.W.(2018).Medicaidexpansion,mentalhealth,andaccesstocareamongchildlessadultswithandwithoutchronicconditions.Journalofgeneralinternalmedicine,33(3),376-383.34Sommers,B.D.,Gawande,A.A.,andBaicker,K.,“HealthInsuranceCoverageandHealth—WhattheRecentEvidenceTellsUs,”(2017).
29%
36%
25%
29%
23%
30%
Skippedcareduetocost Nocheck-upinlast2years
2015
2016
2017

TheEconomicImpactofMedicaidExpansioninMontana
19
B.Financialsecurity
Medicaidexpansionalsogeneratesmajorimprovementsinfinancialsecurity.Itreduces
debtcollections,reducesbankruptcies,andimprovescreditscores.35Forinstance,one
recentstudyfoundthatMedicaidexpansionreducedmedicaldebtby$900pertreated
person,prevented50,000bankruptcies,andledtobettercredittermsforborrowers.36The
interestsavingsfromtheseimprovementswereworth$280pertreatedpersonor$520
millionoverall.Thesefinancialbenefitsareonthesamemagnitudeasthereductionin
uninsuredindividuals’out-of-pocketcosts.
C.Crime
MultiplerecentstudiesfindthatMedicaidexpansionreducedbothviolentcrimeand
propertycrime.37Onestudyarguesthesebenefitsmaystemfromincreasedmentalhealth
andsubstanceabusetreatment.Nationally,thebenefitsofexpansion-inducedcrime
reductionmayexceed$10billionannually.
D.Employment
SomeworrythatexpandingMedicaidwillreduceworkincentives.However,several
studiesfindnoevidencethatMedicaidexpansiondepressesemployment.38Onestudyeven
foundthatMedicaidexpansionincreasedemploymentamongpeoplewithdisabilities.39A
differentstudyofpre-ACAexpansionsinMedicaideligibilityfoundthatmoregenerous
35Brevoort,K.,Grodzicki,D.,andHackmann,M.B.,MedicaidandFinancialHealth(No.w24002).NationalBureauofEconomicResearch(2017);Hu,L.,Kaestner,R.,Mazumder,B.,Miller,S.,andWong,A.,TheEffectofthePatientProtectionandAffordableCareActMedicaidExpansionsonFinancialWellbeing(No.w22170),NationalBureauofEconomicResearch(2016).36Brevoort,etal.,(2017).37Vogler,J.,“AccesstoHealthCareandCriminalBehavior:Short-RunEvidenceFromtheACAMedicaidExpansions(2017);He,Q.,“TheEffectofHealthInsuranceonCrimeEvidenceFromtheAffordableCareActMedicaidExpansion(2017).Thesestudiesareconsistentwithresearchthatexaminedtheeffectsofpriorinsuranceexpansionsoncrime,erg,.Wen,H.,Hockenberry,J.M.,andCummings,J.R.,“TheEffectofMedicaidExpansiononCrimeReduction:EvidenceFromHIFA-WaiverExpansions,”JournalofPublicEconomics154(2017):67-94.38Leung,P.,andMas,A.EmploymentEffectsoftheACAMedicaidExpansions(No.w22540).NationalBureauofEconomicResearch(2016);Kaestner,R.,Garrett,B.,Chen,J.,Gangopadhyaya,A.,andFleming,C.,“EffectsofACAMedicaidExpansionsonHealthInsuranceCoverageandLaborSupply,”JournalofPolicyAnalysisandManagement36,no.3(2017):608-642;Duggan,M.,Goda,G.S.,andJackson,E.,TheEffectsoftheAffordableCareActonHealthInsuranceCoverageandLaborMarketOutcomes(No.w23607),NationalBureauofEconomicResearch(2017);Frisvold,D.E.,andJung,Y.,“TheImpactofExpandingMedicaidonHealthInsuranceCoverageandLaborMarketOutcomes,”InternationalJournalofHealthEconomicsandManagement(2016):1-23.39Hall,J.P.,Shartzer,A.,Kurth,N.K.,andThomas,K.C.,“EffectofMedicaidExpansiononWorkforceParticipationforPeopleWithDisabilities,”AmericanJournalofPublicHealth107,no.2(2017):262-264.

TheEconomicImpactofMedicaidExpansioninMontana
20
publichealthinsuranceincreasedtheprobabilityofsomeonepursuingriskier,buthigher
payingjobs.40
AccordingtoarecentsurveyofOhio’sMedicaidexpansionpopulation,Medicaid
expansionmakesiteasierforpeopletowork.41Amongemployed,continuouslyenrolled
beneficiaries,83percentreportedthatexpansionmadeiteasierforthemtowork,and60
percentofunemployed,continuouslyenrolledbeneficiariesreportedthatMedicaid
expansionmadeiteasierforthemtolookforwork.
DatafromMontanashownoadverseeffectofMedicaidexpansionontheemployment
oflow-incomeMontanans.Infact,Montanasawanincreaseinlow-incomelaborforce
participationfollowingMedicaidexpansion.Table8showsthechangeinlaborforce
participationobservedintwodatasets:theCurrentPopulationSurveyAnnualSocialand
EconomicSupplement(“CPSASEC”)andtheAmericanCommunitySurvey(“ACS”).As
showninthetable,laborforceparticipationroseinthefirst-twoyearsafterexpansion
amongnon-disabledMontanans,ages18-64,withincomesbelow139percentFPL.Similar
increasesinlaborforceparticipationwerenotobservedamonghigher-incomeMontanans
orlow-incomeresidentsinotherstates.Infact,laborforceparticipationfellintheseother
groups.Ifweassumethatlow-incomelaborforceparticipationinMontanawasexpectedto
followthetrendsinotherstatesoramonghigh-incomeMontanans,thentheincreasein
laborforceparticipationamonglow-incomeMontanansisevenlarger(6.2percentage
pointsintheCPSdataand3.9percentagepointsintheACSdata).
WhiletheseresultsdonotprovethatMedicaidexpansionincreasedemployment,they
suggestitmighthave.Thispatternofresultsisconsistentwiththehypothesisthat
MedicaidexpansionandMontana’sHELP-Linkprogramimprovedemploymentoutcomes
forMontana’sMedicaidexpansionbeneficiaries.Theseeffectscouldreflecttheimpactof
obtaininghealthinsuranceandanyassociatedimprovementsinhealth,theimpactof
HELP-Link,acombinationofthetwo,orsomeothernotyetunderstoodfactor.Wenote,
consistentwiththeinterpretationthatHELP-linkaffectedemployment,arecentanalysisof
aprograminNevada,similartoHELP-Link,thatprovidedeligibilityreviewandjob
counselingservicestorandomlyselectedunemploymentinsurancerecipientsledto
persistentincreasesinlong-termemploymentandearnings.42
40Farooq,A.,&Kugler,A.(2016).Beyondjoblock:impactsofpublichealthinsuranceonoccupationalandindustrialmobility(No.w22118).NationalBureauofEconomicResearch. 41OhioDepartmentofMedicaid(2018).2018OhioMedicaidGroupVIIIAssessment:Afollow-uptothe2016OhioMedicaidGroupVIIAssessment.https://medicaid.ohio.gov/Portals/0/Resources/Reports/Annual/Group-VIII-Final-Report.pdf42Manoli,D.S.,Michaelides,M.,andPatel,A.,Long-TermEffectsofJob-SearchAssistance:ExperimentalEvidenceUsingAdministrativeTaxData(No.w24422),NationalBureauofEconomicResearch(2018).

TheEconomicImpactofMedicaidExpansioninMontana
21
Table8:LaborForceParticipationAmongNon-DisabledPeopleAges18-64,BeforeandAfterExpansioninMontanaCurrentPopulationSurveyASEC
Before(2012-2015)
After(2016-2018)
Difference(afterminusbefore)
DifferenceinDifference
(MTdifferenceminusrestdifference)
0-138%FPL Montana 57.9% 60.7% 2.7%
RestofU.S. 57.6% 54.2% -3.5%*** 6.2%***>138%FPL
Montana 85.8% 84.0% -1.7%* RestofU.S. 83.4% 83.6% 0.2% -2.0%***
AmericanCommunitySurvey
Before(2012-2015)
After(2016-2017)
Difference(afterminusbefore)
DifferenceinDifference
(MTdifferenceminusrestdifference)
0-138%FPL Montana 63.0% 64.2% 1.3%
RestofU.S. 59.3% 56.7 -2.7%*** 3.9%***>138%FPL
Montana 86.0% 86.6% -1.7% RestofU.S. 85.6% 85.9% 0.1% 0.3%***
Source:Authors’analysisofCurrentPopulationSurveyASECandAmericanCommunitySurveymicrodata
obtainedfromIPUMS-CPSandIPUMS-USA.Analysesconductedattheindividuallevelwithprovidedperson
weights.Samplelimitedtoincludepeopleages18-64withincome<139percentFPLandnodisability,
***=p<0.01,*=p<0.05.Difference-in-differenceresultsobtainedfromregressionwithstateandyearfixed
effects.Standarderrorsclusteredatstatelevel.SeeAppendixEforadditionaldetails.
F.Healthcaresector
Finally,asdiscussedabove,Medicaidexpansionrepresentsasignificantinvestmentin
Montana’shealthcaresystem,particularlyitscriticalaccesshospitalsandruralproviders.
Italsosignificantlyimprovesthefinancialhealthofsafety-nethospitals.43Amorerobust
healthcaresectorbenefitsallresidents.Forinstance,ifaruralhospitalcloses,allresidents
suffer.Thus,totheextentexpansionpreservesorexpandstherangeofservicesavailablein
anarea,allresidentsbenefit.
43Dobson,A.,DaVanzo,J.E.,Haught,R.,andPhap-Hoa,L.,“ComparingtheAffordableCareAct'sFinancialImpactonSafety-NetHospitalsinStatesThatExpandedMedicaidandThoseThatDidNot,”IssueBrief(CommonwealthFund),(2017):1-10.

TheEconomicImpactofMedicaidExpansioninMontana
22
AhandfulofstudieshaveexaminedtheeffectofMedicaidexpansiononthefinancial
performanceofthehealthcaresector.Thesestudiesgenerateaconsistentpictureof
Medicaidexpansion’seffects–Medicaidexpansionimproveshospitals’financialhealthand
reducestheoddsthathospitalsclose.TheeffectsofMedicaidexpansionareparticularly
stronginruralareasandinareaswithsubstantialnumbersofuninsuredadultspriorto
expansion.
OnesetofarticlesexaminedtheimpactofMedicaidexpansiononhospitalfinances
through2015.44Thesestudiesfindthat,relativetonon-expansionstates,hospitalsin
Medicaidexpansionstates:
• ReduceduncompensatedcarerelativetoaFY11-FY13baselineby34percentandreduceduncompensatedcareasapercentageofexpensesby1.7percentagepoints;
• IncreasedMedicaidrevenueby18.2percent;
• Improvedoperatingmarginsby2.5percentagepoints(67.3percent);and
• Improvedexcessmarginsby1.7percentagepoints(41.4percent).
Thesestudiesalsofindthattheimpactsonnon-metrohospitalswerelarger,
particularlyontheirprofitmargins.Hospitalsoutsidemetro-areasinexpansionstatessaw
operatingmarginsincreaseby4.0percentagepointsandexcessmarginsincreasedby2.3
percentagepointsrelativetonon-metrohospitalsinnon-expansionstates.
Wequasi-replicatedtheseanalysesusingdatathatextendinto2017andfoundsimilar
results(seeAppendixEfordetails).Thepassageoftimehastendedtoincreasethe
estimatesoftheeffectsofMedicaidexpansion.Forinstance,weestimatethattheimpactof
Medicaidexpansiononuncompensatedcaregrewfrom1.5percentto2.6percentoftotal
expensesbetweenthefirstandthirdyearsfollowingexpansion.
Wealsoestimatethateffectsaremuchlargerforprovidersinstates(likeMontana)
withabove-averageMedicaidexpansionenrollment.Providersinhighenrollmentstates
sawmuchlargerincreasesinnetMedicaidrevenue,muchlargerdecreasesin
uncompensatedcare,andmorerobustimprovementinoperatingmargins.
AdifferentstudyexaminedtheimpactofMedicaidexpansiononhospitalclosuresusing
datafrom2008-2016.45Thisstudyfoundthat:
44Blavin,F.(2017).HowHastheACAChangedFinancesforDifferentTypesofHospitals?UpdatedInsightsfrom2015CostReportData;Blavin,F.(2016).Associationbetweenthe2014MedicaidexpansionandUShospitalfinances.Jama,316(14),1475-1483.

TheEconomicImpactofMedicaidExpansioninMontana
23
“theACA’sMedicaidexpansionwasassociatedwithimprovedhospitalfinancial
performanceandsubstantiallylowerlikelihoodsofclosure,especiallyinrural
marketsandcountieswithlargenumbersofuninsuredadultsbeforeMedicaid
expansion.”
Inparticular,thisstudyshowsthathospitalsinexpansionstatesweresixtimeslesslikely
toclosethanhospitalsinnon-expansionstates.ItalsofindsthattheimpactofMedicaid
expansionisstrongerincountiesthathadmoreuninsuredpriortoexpansion.Incounties
whereover30percentofadultswereuninsuredpriortoexpansion,Medicaidexpansionis
associatedwitha90percentreductionintheoddsofhospitalclosure.Similartothe
analysisdescribedabove,thisstudyalsofindsthatMedicaidexpansionimprovesprofit
marginsinruralareasbyalargeramount.
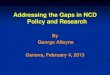
Figure3:TotalhealthcareemploymentoutsideMontana’smetro-areaandmicro-areas,2013-2017
Notes:Author’sanalysisofQuarterlyCensusofEmploymentandWages(QCEW)data.Figurerepresentstotal
statewideemploymentminusemploymentinYellowstone,Missoula,Cascade,Gallatin,Flathead,Lewisand
Clark,andSilverBowcounties.
Figure3helpsillustratetheimpactofMedicaidexpansiononthehealthcaresectorin
ruralareasinMontana.Consistentwithimprovementsinruralproviders’financials,health
45Lindrooth,R.C.,Perraillon,M.C.,Hardy,R.Y.,&Tung,G.J.(2018).UnderstandingTheRelationshipBetweenMedicaidExpansionsAndHospitalClosures.HealthAffairs,37(1),111-120.
15400
15600
15800
16000
16200
16400
16600
2013 2014 2015 2016 2017

TheEconomicImpactofMedicaidExpansioninMontana
24
careemploymentinMontana’sruralareasbegangrowingonceMontanaexpanded
Medicaid.Inthetwoyearspriortoexpansion,totalhealthcareemploymentinrural
Montanagrewbarelyatall,lessthanonepercent,only100totalnewjobs.However,once
Medicaidexpanded,ruralhealthcaregrew,addingnearly600jobsintwoyears.
VI.FiscalEffects
Medicaidexpansionalsoaffectsthestate’sbudget.Whileitreducessomestatecosts,it
imposesothers.Asnotedpreviously,thestate’sshareofexpansioncostswillrisetoten
percentin2020andbeyond.Technically,thecosttothestateismorecomplicatedthan
this.BecauseMontanaoffers12-monthcontinuouseligibility,itmustpayaslightlyhigher
shareofcosts.However,thefederalgovernmentpaysfor100percentofcertainexpansion
costs(e.g.,costsofservicesprovidedbytheIndianHealthService).Accordingtothe
LegislativeFiscalDivision’s2021BienniumBudgetAnalysis,theGeneralFundcostof
Medicaidexpansionrisesto8.9percentofthetotalMedicaidcostinFY2021.46
Asubstantialproportionofthecosttothestateisoffsetbyvarioussavings.As
discussedabove,MedicaidexpansionreducesthecostoftraditionalMedicaid,healthcare
spendingbytheDepartmentofCorrections,andspendingonsubstanceusedisordersand
mentalhealth.47PremiumspaidbyHELPbeneficiariesalsohelpoffsetcosttothestate
generalfund.48Intotal,weestimatethesesavingsoffset71percentoftheexpectedgeneral
fundcostsinFY2020and64percentoftheexpectedgeneralfundcostsinFY2021.Assuch,
theexpectedcosttothestategeneralfundnetofthesesavingsisapproximately$17
millioninFY2020and$23.7millioninFY2021.
However,asdescribedinSectionsIIIandIV,Medicaidexpansionalsoincreases
economicactivity.Increasedactivitywillincreasestaterevenues.Theincreaseinstate
revenuesattributabletoMedicaidexpansionwilllikelyexceedtheremainingcostof
46https://leg.mt.gov/content/Publications/fiscal/BA-2021/2021BienniumVolume1_Final.pdf[accessedDecember22,2018]47WeuseestimatesfrmMedicaidExpansion:HowitaffectsMontana’sstatebudget,economy,andresidents.https://mthcf.org/wp-content/uploads/2018/06/Manatt-MedEx_FINAL_6.1.18.pdfforsomeofthesesavings;however,forDepartmentofCorrectionssavingsweuseadifferentestimatebasedonthechangeinoutsidemedicalspendingbeforeandafterexpansion.Pre-MedicaidexpansionannualoutsidemedicalcostsfortheDepartmentofCorrectionstotaled$8.3million.Afterexpansion,theytotaled$5.5million.Thus,spendingforoutsidemedicalcarefellby$2.8million.Inaddition,weassume$2.6millionperyearinfacilityreimbursementsavings.WealsousetheprojectedtraditionalMedicaidsavingsfromtheLFDreportforFY20andFY21.48Asweunderstandit,premiumpaymentstothefederalgovernmentareincludedaspartofthetotalcosttothestate,sowesubtractthefullpremiumestimatefromthestatetotal.Basedoncorrespondencewithstateofficials,weassumepremiumswillbe$4.6millionperyearinFY20andFY21.

TheEconomicImpactofMedicaidExpansioninMontana
25
Medicaidexpansion.Table9presentsasimpleanalysisofthenetfiscaleffectsofMedicaid
expansionbasedonlyontaxrevenues.Onaverage,between2012and2016,totalstatetax
revenesequaledsixpercentofstategrossdomesticproduct.Assuch,weassumethatthe
staterecovers6percentoftheincreaseinGDPattributabletoMedicaidexpansion.49We
applythisvaluetotheincreaseinGDPpresentedinTable1andtotheestimatespresented
inAppendixC,TableA6forAlternative3.ThisanalysissuggeststhatMedicaidexpansion
hasapositiveneteffectonMontana’sstatebudget.
Forinstance,assumingthathalfofthenetcostestimatesineachofFY2020andFY2021
willbeincurredinCY2020thenetcostofMedicaidexpansioninCY2020willbe$20.4
million.TheREMImodelestimatespresentedinTable1suggestthatMedicaidexpansion
willadd$420milliontogrossdomesticproductin2020.Applyingthe6percentaverage
taxsharetothechangeinGDPsuggeststhatMedicaidexpansionwillgenerate$25.2
millioninstatetaxrevenueinCY2020.Thisexceedstheremainingcostestimateby$4.8
million.TheempiricalestimatesinSectionIVandalternativeREMIspecificationssuggest
thepositiveneteffectofMedicaidexpansiononthestatebudgetmaybeevenlarger.
Table9:NetfiscaleffectofMedicaidexpansion($millions)forcalendaryears2016-2020 2016 2017 2018 2019 2020NetcostofexpansiontoMT -$10.2 -$5.3 $3.3 $10.7 $20.4
EstimatedtaxrevenuesbasedestimatesinTable1
$13.7 $26.4 $30.5 $28.7 $25.2
Neteffectonstatebudget $23.9 $31.7 $27.2 $18.0 $4.8
EstimatedtaxrevenuesbasedonestimatesTableA6Alt.3
$14.5 $28.0 $32.4 $30.5 $26.9
Neteffectonstatebudget $24.7 $33.3 $29.1 $19.8 $6.5Notes:Taxrevenuesequal6percentofestimatedimpactonGDP.
TheresultsinTable9focusexclusivelyontheeffectofMedicaidexpansionontax
revenue.However,theincreaseineconomicactivityattributabletoMedicaidexpansion
willlikelyaffectotherpartsofMontana’sbudget.Itwillincreaseotherformsofrevenue,
anditmaychangeexpenditures.ThemarginaleffectofMedicaidexpansionontheseother
aspectsofthebudgetisuncertain.Table10presentstheresultsbasedonabroader
approach.TheseresultsusetheFiscalImpactAssessmentTool(“FIAT”),amodulethat
estimatesstaterevenueandexpenditureimpactsbasedontheoutputfromtheREMI
49StatetaxrevenuedataobtainedfromtheU.S.CensusBureau’sAnnualSurveyofStateGovernmentFinances.GrossstateproductobtainedfromtheBureauofEconomicAnalysis.

TheEconomicImpactofMedicaidExpansioninMontana
26
model.UsingtheFIAT,wefindthatby2020bothtotalrevenuesandexpendituresrise,but
theneteffectisa$42.1millionincreaseinstatefiscalresources.Thisissubstantiallymore
thantheestimated$20.4millionnetcostin2020.
Table10:NetfiscalimpactsofREMIresultsinTable1usingtheFIAT(millionsof$2018) 2016 2017 2018 2019 2020TotalRevenues 26.1 53.0 65.3 66.5 63.9TotalExpenditures -12.4 -15.7 -5.7 8.9 21.8NetFiscalImpact 38.5 68.7 71.0 57.6 42.1CumulativeFiscalImpact 38.5 107.2 178.2 235.8 277.9Note:TheFIATmodeloutputisin$2012.Weinflateto2018usingthechainedPCEindexobtainedfrom
https://fred.stlouisfed.org/series/PCEPI.
TheFIATmodeluseshistoricalaveragerelationshipsbetweeneconomicactivity
(particularlypopulation,personalincome,andemployment)andstaterevenuesand
expenditurestoprojecthowrevenuesandexpenditureschangeinresponsetochanging
population,personalincome,andemployment.Assuch,theseresultscomewithan
importantcaveat.Theyarebasedonthehistoricalaveragerelationshipsbetweeneconomic
activityandstaterevenuesandspending.However,thefuturemarginalfiscalimpactof
Medicaidexpansionmaydifferfromthehistoricalaveragerelationshipbetweeneconomic
activityandthestatebudget.Somerevenuesandexpenditureswilllikelybeunaffectedby
Medicaidexpansion.Otheraspectsofthestatebudgetmaymovebymorethanaverage.
Ultimately,itisdifficulttoisolatetheeffectsofMedicaidexpansionthroughoutthewhole
budget(bothrevenuesandexpenses).Statebudgetsareveryflexibleandrespondto
shockslikeMedicaidexpansionincomplicatedways.50However,inMontanaandinmost
otherstates,staterevenuesandexpenditurestendtoremainatarelativelyconstantshare
ofeconomicactivityoverlongperiodsoftime.Assuch,theapproachinTable9andthe
FIATapproachlikelyprovideareasonableestimateofMedicaidexpansion’sfiscaleffects.
VII.Conclusion
MedicaidexpansionhasasubstantialpositiveimpactonMontana’seconomy.While
impactsvaryfromyear-to-year,itbringsover$600millionofnewspendingintoMontana’s
economyeachyear.ThisspendingripplesthroughMontana’seconomy,generating
thousandsofjobsandhundredsofmillionsinpersonalincomeeachyear.Forinstance,in
50AlongerdiscussionofthechallengesofestimatingbudgetimpactsofMedicaidexpansioncanbefoundin
Dorn,S.,“TheEffectsoftheMedicaidExpansiononStateBudgets:AnEarlyLookinSelectStates,”(2015).

TheEconomicImpactofMedicaidExpansioninMontana
27
2020,weestimatethatitwillsupportnearly6,000jobsand$350millioninpersonal
income.Inadditiontogeneratingeconomicactivity,Medicaidexpansionappearsto
improveoutcomes—reducingcrime,improvinghealth,andshrinkingdebt.Whilethestate
paysforthesebenefits,thecoststothestatebudgetaremorethanoffsetbythesavings
createdbyMedicaidexpansionandbytherevenuesassociatedwithincreasedeconomic
activity.
Likeanystudy,thisstudyhaslimitations.Theassumptionsusedtoestimatethedirect
impactsofMedicaidexpansionmaybeunderminedbyreal-worldevents.Similarlythe
assumptionsthatunderlietheREMImodelmayalsofailtoaccuratelycapturetheeconomic
relationshipsatissue.Inordertoaccountfortheseweaknesses,weconductedseveral
sensitivityanalyses.Thatis,weestimatedseveraladditionalmodelsusingalternative
assumptions.Ingeneral,theseadditionalanalysesyieldresultssimilartothosedescribed
here.
Acrossavarietyofspecifications,Medicaidexpansiongeneratesseveralthousand
additionaljobsandseveralhundredmilliondollarsinadditionalincome.Thecumulative
effecttendstobeanapproximateonepercentincreaseinemploymentandincome.These
resultsalignempiricalestimatesfortheimpactofMedicaidexpansionontotalemployment
inasetofstateswheretheimpactofMedicaidexpansiononinsurancecoverages
resemblesthechangeinMontana.
Atthislevelofactivity,Medicaidexpansionalsopaysforitself.Thesavingsand
additionalrevenuesattributabletoMedicaidexpansionexceedthecoststothestate.While
theremaybeconditionsunderwhichMedicaidexpansionimposesnetcostsonthestate,
weexpectsuchinstancestooccurrarely,assumingMedicaidexpansionretainsitscurrent
structure.

TheEconomicImpactofMedicaidExpansioninMontana
28
Appendix
A.Selectingcomparisonstates
Inthedifferences-in-differencesanalysisinSectionIVandseveralsimilaranalyses
describedinthisappendix,welimitthesetofexpansionstatesincludedintheanalysis.We
limitthesetofexpansionstatesexaminedbecausestates’experienceswithMedicaid
expansionvarywildly,andMontana’sexperienceisaboveaverage.
FigureA1helpstoillustratethevariationacrossstates.Itplotstheshareofexpansion
eligible(peopleages18-64withincomelessthan139percentofFPL)withMedicaid
(horizontalaxis)againstthesharewithanyinsurance(verticalaxis).
FigureA1:ChangeinsharewithanyinsuranceandsharewithMedicaidamongpeopleages18-64withincome<139FPLinexpansionstates
Notes:Author’sanalysisofAmericanCommunitySurveymicrodataobtainedfromIPUMS-USA.Change=
Level2017–AvgLevel2010-2013.
Weincludethestateslistedinredinouranalyses.Inthesestates,theaveragechange
alongbothdimensionsisroughlyequaltothechangeinMontana.Theincludedstatesare
alsowellmatchedtothecontrol(non-expansion)states.Thatis,theincludedstateswere
similartonon-expansionstatespriortoexpansion.

TheEconomicImpactofMedicaidExpansioninMontana
29
FigureA2showstheaverageshareofpeoplewithanyhealthinsuranceintheincluded
expansionstatesandnon-expansionstatesduring2010-2013.Thedifferencesaresmall
andstatisticallyinsignificant.
FigureA2:Averageshareof18-64yearoldpopulationwithanyhealthinsurance2010-2013byincomelevel
Notes:Authors’analysisofAmericanCommunitySurveymicrodataobtainedfromIPUMS-USA.
Werecognizethatonecouldarguefortheinclusionorexclusionofvariousstates
aroundthemargins.Inlightofthis,weconductedsensitivityanalysesthatmodifiedtheset
ofincludedstates.Modifyingthesetofincludedstatesslightlychangesthecoefficientsand
levelsofstatisticalsignificanceslightly,buttheoverallpatternofresultsisunaffected.
B.DirecteffectsforREMImodel
ToestimatetheeconomicimpactsofMedicaidexpansion,weneedtounderstandthe
directeffectofMedicaidexpansiononMontana’seconomy.Thatis,weneedtoanswerthe
question:“WithoutMedicaidexpansion,whichpartsoftheeconomywouldhavemore/less
moneyandhowmuchmore/lesswouldtheyhave?”
AsdescribedinSectionIII,Medicaidexpansionintroducesthreekeychanges:
(1) Medicaidexpansionchangeslow-incomeMontanans’insurancecoverage(bothwhethertheyarecoveredandthetypeofinsurancethosewithcoveragehave);
(2) Medicaidexpansionchangeshowmuchhealthcarelow-incomeMontanansconsume;and
0.55
0.75
0.56
0.77
<139 All
Includedexpansion
Non-expansion

TheEconomicImpactofMedicaidExpansioninMontana
30
(3) Medicaidexpansionchangeswhopaysforlow-incomeMontanans’healthcare. Incombination,thesethreechangesproducethedirecteffectsofMedicaidexpansion.
1.HowdoesMedicaidexpansionchangeinsurancecoverage?
Medicaidexpansionreducesthenumberofuninsuredpeopleandchangesthe
proportionofpeoplewithdifferenttypesofinsurance(e.g.,traditionalMedicaid,employer
sponsored,directpurchase).
AportionofMedicaidexpansionbeneficiarieswouldhavebeenenrolledintraditional
Medicaidwithoutexpansion.Thistransfersavesthestatemoney.Weusesavingsestimates
fromthestatetoestimatethesizeofthispopulationusingthefollowingequation:
!"#"$ !"#$ !ℎ!"# !"#$%&!! = !"#"$ !ℎ!"#!"#$ ∗ !"#$%&$'!"#$%,!
Forpurposesofthiscalculation,weassumethatshiftingthispopulationfromtraditional
Medicaidtotheexpansiondoesnotchangetheirtotalspending.Giventheserelationships,
totalspendingamongthispopulationequals:
!"#$%&$'!"#$%,! =!"#"$ !"#$ !ℎ!"# !"#$%&!!
!"#"$ !ℎ!"#!"#$
Giventhisrelationship,weestimatethetotalhealthcarespendingamongtheMedicaid
transferpopulationisapproximately12percentoftotalexpansionspending.Ifweassume
thattheaveragespendingperpersoninthetransferpopulationequalstheaverage
spendingperpersoninthenon-transferpopulation,thissuggeststhat12percentof
expansionbeneficiarieswouldhaveenrolledintraditionalMedicaidwithoutexpansion.
ThevastmajorityoftheremainingMedicaidexpansionbeneficiarieswouldhavebeen
uninsuredwithoutexpansion.Toestimatethisshareandtheshareofpeoplewhoswitch
fromotherformsofinsurance,weuseadifferences-in-differenceanalysissimilartothe
onepresentedinSectionIV.However,inthisanalysis,theoutcomesaretheshareofpeople
withMedicaid,anyinsurance,orprivateinsurance.51
51ForthisanalysisweuseAmericanCommunitySurveypublic-usemicrodatafortheyears2010-2017obtainedfromIPUMS-USA.WenotethattheACSinsurancequestionshaveknownlimitations.E.g.,onestudyfoundthatitsystematicallyundercountsMedicaidenrollmentby23percent.Bourdreaux,M.,K.ThiedeCall,JTurner,B.Fried,andB.O’Hara(2013)AccuracyofMedicaidReportingintheACS:PreliminaryResultsfromLinkedData.SHADACandUSBureauofCensus.

TheEconomicImpactofMedicaidExpansioninMontana
31
WeusetheresultsfromthisanalysistoestimatewhattypesofinsuranceMedicaid
expansionbeneficiarieswouldlikelyhavewithoutexpansion.Specifically,wedividethe
differences-in-differencescoefficientforthechangeintheshareofpeoplewithaparticular
typeofinsurancebythechangeinthesharewithMedicaid.TableA1presentstheresults
fromthisanalysis.
TableA1:CompositionofchangeinMedicaidenrollmentforselectedpopulations. ComparisonStates,all18-64 Montanaonly,all18-64 Any Private Any PrivateYear1 0.75 0.27 0.88 0.11Year2 0.73 0.28 0.81 0.16Year3 0.77 0.23 Year4 0.74 0.26
Average 0.75 0.26 0.84 0.13
ComparisonStates,18-64<139FPL
Montanaonly,18-64<139FPL
Any Private Any PrivateYear1 0.83 0.18 0.62 0.29Year2 0.79 0.21 0.80 0.22Year3 0.81 0.20 Year4 0.75 0.27
Average 0.80 0.21 0.71 0.25
Averageasshareoftotalenrollment,assuming12percentwithinMedicaidtransfer Private Private Private PrivateAll 0.66 0.23 0.74 0.12<139 0.70 0.19 0.63 0.22Notes:Authors’analysisofAmericanCommunitySurvey2010-2017microdataobtainedfromIPUMS-USA.
Regressioncoefficientsthatformbasisforlistedsharesobtainedfromregressingsharewitheachtypeof
insuranceoninteractionsequaltooneifanincludedexpansionstateNyearsafterexpansioninthatstate
alongwithstateandyearfixedeffects.Thepopulationintheseregressionsislimitedasdescribedintable
withanadditionalrestrictionthattheindividualhaveonlyonetypeofinsurance.
Wereportresultsforfourdifferentpopulations.Thetopportionofthetableexamines
coverageamongtheentire18-64year-oldpopulation,andthebottomportionexamines
coverageamong18-64yearoldswithincomesbelow139percentofthepovertyline.The
leftportionofthetablepresentsresultsthatcomparetheselectedMedicaidexpansion
statestonon-expansionstates,andtherightportionpresentsresultsthatcompare
Montanatonon-expansionstates.Theresultsvarysome,butthegeneralpatternisthe
same–thevastmajorityofthegrowthinMedicaidcoveragecamefromtheuninsured
population.Forinstance,intheselectedexpansionstates(i.e.,stateswhereuninsurance
declinedbyasimilaramounttoMontana),approximately75percentofthenetchangein
Medicaidenrollmentcamefromtheuninsured.TheremaininggrowthinMedicaid

TheEconomicImpactofMedicaidExpansioninMontana
32
enrollmentprimarilyreflectsareductionintheshareofpeoplewithsomeformofprivate
insurance.
TheseestimatesfocusonthenetchangeintotalMedicaidenrollment.Assuch,theydo
notaccountforwithin-Medicaidtransfers.Forpurposesofouranalysis,weassumethat12
percentoftotalexpansionenrollmentareMedicaidtransfers.Assuch,weassumethat
roughly60-70percentofexpansionenrolleescomefromtheuninsuredpopulation.
Weassumetheremaining18-28percentofMontanaMedicaidexpansionenrollees
switchfromsomeformofprivateinsurance.Theallocationoftheseenrolleesbetween
employer-sponsoredanddirectpurchaseinsuranceismoredifficulttodetermine.Analyses
ofMedicaidexpansionseffectsontheshareofpeoplewithdifferenttypesofprivate
insurancedonotyieldconsistentresults.Someanalysessuggestthat70percentoftheshift
fromprivateinsurancetoMedicaidwasamongpeoplewithemployer-sponsored
insurance,otherssuggestthat70percentofthisshiftwasfrompeoplewithdirectpurchase
insurance.
Forthepurposesofthisanalysis,wealsoneedtoidentifythosewhowouldhave
receivedsubsidiesfromthefederalgovernmenttoobtaininsurancethroughtheexchange.
WhentheseindividualsswitchtoMedicaid,thefederalgovernmenteffectivelytransfers
whatitwouldhavespentonsubsidiestoMedicaidexpansion.Assuch,aportionof
Medicaidexpansionspendingfortheseindividualsdoesnotrepresentnewmoneyin
Montana’seconomyandshouldnotbeincludedasdirectimpacts.
Unfortunately,thedatatoestimatemovementfromtheexchangetoMedicaid
expansionislimited.Thesurveyusedintheanalysesabovedoesnotseparateexchange
coveragefromotherformsofdirectpurchaseinsurance.Giventhatsubsidiesareonly
availabletoindividualswithincomeabove100percentofthefederalpovertyline,theset
ofbeneficiarieswithincomeabovethisthresholdprovideanupperboundestimateforthis
value.AccordingtoDPHHS,11percentofexpansionbeneficiarieshaveincomesabove100
percentFPL.52Ofcourse,itisunlikelythatall(orevenmostofthispopulation)was
enrolledontheexchange.AccordingtodatafromtheMedicalExpenditurePanelSurvey
(“MEPS”),only6percentofAmericansages18-64withincomebetween100-150percent
oftheFPLwereenrolledonanexchangein2016.53Whilethesedataarenotreportedby
52https://dphhs.mt.gov/Portals/85/Documents/healthcare/MedicaidExpansionMemberProfile.pdf[accessedDecember22,2018]53MEPSdataobtainedfromIPUMS-MEPSincludedatafrom2010-2016.LynnA.Blewett,JuliaA.RiveraDrew,RisaGriffin,KariC.W.Williams,andDanielBackman.IPUMSHealthSurveys:MedicalExpenditurePanelSurvey,Version1.0[dataset].Minneapolis:UniversityofMinnesota,2018.http://doi.org/10.18128/D071.V1.0

TheEconomicImpactofMedicaidExpansioninMontana
33
thestate,thisvaluevariesonlyslightlyacrossregions.IntheSouth,wherefewstateshad
expandedMedicaidin2016,6.2percentofthispopulationwasenrolledinanexchange.In
theNortheast,wherenearlyallstateshadexpanded,thesharewas5.7percent.Adifferent
analysisofMEPSdatasuggeststhatonly3.5percentofthosewhogainedMedicaid
coverageinthispopulationwereenrolledintheexchangeatanypointduringtheyear
priortoMedicaidenrollment.
Thesedatasuggestthatonlyasmallproportionofthosewhoenrolledintheexpansion
otherwisewouldhaveenrolledintheexchangeandreceivedsubsidies.Weusethehigher
number(6percent)inordertoobtainamoreconservativeestimateofMedicaid
expansion’seconomicimpacts.Giventhat11percentofMontanaMedicaidexpansion
beneficiarieswereeligibleforsubsidiesthroughtheexchange,lessthanonepercentof
Medicaidbeneficiarieslikelywouldhaveobtainedsubsidieswithoutexpansion.
TableA2summarizesourassumptionsforthetypeofinsurancecoverageexpansion
beneficiarieswouldhavewithoutexpansion.Toillustratearangeofplausiblevalues,we
presenttwodifferentscenarios.
TableA2:IllustrativeallocationsofMedicaidexpansionbeneficiariestoalternativeformsofcoveragewithoutexpansionTypeofinsurance Uninsured 60% 70%TraditionalMedicaid 12% 12%EmployerSponsored 17% 11%Exchange 1% 1%Otherprivate 10% 6%
2.HowdoesMedicaidexpansionchangetotalhealthcarespending?
Individualhealthspendingchangeswithinsurancecoverage.Forthisstudy,themost
importantrelationshipisbetweenanycoverageandspending.Accordingtodatafromthe
MEPS,low-income(<150percentoftheFederalPovertyLine)individualsaged18-64
withoutinsurancespentapproximately$1,700onhealthcarein2016.54Thisis25percent
ofthespendingforsimilarindividualswhowereinsured($6,700).
Amongthosewithinsurance,spendingvariesbytype.TableA3presentsaverage
annualspendingforlow-incomeAmericansbetweentheagesof18and64withdifferent
54ThispopulationhasanagedistributionthatisverysimilartoMontana’sMedicaidexpansion.Weincludepeopleupto150percentoftheFederalPovertyLinebecausesurveymeasuresofMedicaidexpansioneligibilitytypicallyfailtoaccuratelyidentifythefullsetofMedicaidexpansionindividuals.Thismay,inpart,reflectthingslike12montheligibility.MEPSdataobtainedfromIPUMS-MEPS.

TheEconomicImpactofMedicaidExpansioninMontana
34
typesofinsurance.TheMEPSdoesnotseparatepeoplewithtraditionalMedicaidfrom
thoseintheexpansion.Assuch,theMedicaidvalueblendsbothpopulations;however,
reportedMedicaidspendingalignswithreportedperbeneficiaryspendinginthe
expansionpopulation.Accordingthemostrecentestimates,expansionspendingper
beneficiarywas$6,365inFY2015and$5,965inFY2016.55
TableA3:Averagehealthcarespendingforlow-incomeindividualsages18-64bytypeofhealthinsurance,2016 <150 Difference
withMedicaid
Uninsured $1,681 $4,886Privateinsurance $5,613 $948Group(e.g.,employer) $6,210 $345
Exchange $4,240 $2,341Medicaid $6,411 $0Notes:Authors’analysisofMedicalExpenditurePanelSurveydata.Foreachcategory,welimitthesampleto
individualsenrolledinthistypeofcoverageforthefullyear.TheMedicaidcategoryincludesbothtraditional
MedicaidandMedicaidexpansion.
WeobtainanestimatefornewhealthcarespendinginducedbyMedicaidexpansionby
combiningtheestimatesinTableA2withtheestimatesinTableA3.Multiplyingthe
differencewithMedicaidcolumnfromTableA3bythesharesinTableA2,summingthese
valuesanddividingbyaverageMedicaidspendingsuggeststhat48-55percentofMedicaid
expansionspendingisnewspending.
Asarobustnesscheck,wealsousetheMEPSdatafor2013-2016toestimatehow
individualhealthexpenditureschangewhensomeonegainsorlosesMedicaidcoverage.
Werestrictthesampletopeopleages18-64,andweregressthenaturallogofindividual
healthexpendituresonthenumberofmonthsofMedicaidcoverageoranindicatorequalto
oneiftheindividualwascoveredbyMedicaidinall12monthsalongwithindividualand
yearfixedeffects.TableA4presentstheresults.
Theseresultsareconsistentwiththeresultsabove.Theyindicatethat,onaverage,each
monthofMedicaidcoverageisassociatedwitha$267increaseintotalhealthcare
552017ActuarialReportontheOutlookforMedicaid.https://www.cms.gov/Research-Statistics-Data-and-Systems/Research/ActuarialStudies/Downloads/MedicaidReport2017.pdf[accessedDecember30,2018].

TheEconomicImpactofMedicaidExpansioninMontana
35
spending.TheseestimatessuggestthatobtainingMedicaidmorethandoubleshealthcare
spending.Assuch,50-60percentofMedicaidspendingisnewspending.56
TableA4:EffectofMedicaidcoverageonaveragehealthcarespending Totalhealth
expendituresTotalhealthexpenditures
Totalhealthexpenditures
Totalhealthexpenditures
Medicaidmonths
267***(29)
266***(43)
12monthsofMedicaid
3,560***(440)
3,637***(637)
Population All18-64 All18-64 Low-income18-64
Low-income18-64
N 85,007 78,010 47,228 21,837Notes:Authors’analysisofMEPSdataforyears2013-2016obtainedfromIPUMS-MEPS.Resultsfrom
regressionofln(totalhealthexpenditure+1)onMedicaidcoveragewithindividualandyearfixedeffectsfor
populationages18-64.Robuststandarderrorsinparentheses.***indicatesstatisticallysignificantat0.001
level.Fortheregressionthatfocusesonafull-yearofMedicaidcoverage,weexcludepeoplewithapartial
yearofMedicaidcoverage.TheMedicaidvariableincludesbothtraditionalMedicaidandMedicaidexpansion.
Asanadditionalrobustnesscheck,weusedataontotalhealthcarespendingbystate
between2010and2014toconductanadditionaldifferences-in-differencesregression.57
Again,welimitthesetofexpansionstatestothehighimpactstatesdescribedaboveand
comparethechangeinhealthcarespendinginthatsetofstatestothechangeinnon-
expansionstates.Specifically,weregressthenaturallogoftotalhealthspendingonan
indicatorforincludedexpansionstatesafterexpansionalongwithcontrolsforthenatural
logoftotalpopulation,thenaturallogofpersonalincome,thenaturallogofthepopulation
overage65,thenaturallogthepopulationwithadisability,andstateandyearfixedeffects.
ThisregressionsuggeststhatMedicaidexpansionincreasedtotalhealthcarespendingin
expansionstatesduringthefirstyearofexpansionby1.6percent(p<0.01).Applyingthis
estimatetoexpectedtotalhealthexpendituresinMontanain2016,suggestsMedicaid
expansionincreasedtotalhealthspendingbyapproximately$150million,or
approximately48percentof2016Medicaidexpansionspending.58
56E.g.,averageMedicaidspendinginthefull18-64year-oldpopulationaveragedapproximately$6,200.$267*12/$6,200=0.52.57Atpresent,2014isthemostrecentdatawithstatelevelhealthcareexpendituredataavailablefromtheNationalHealthExpendituresprogram.58ThemostrecentdataonhealthexpendituresinMontanaarefor2014.Toobtainanestimatefor2016,weapplythenationalrategrowthrateofpersonalhealthcarespendingin2015(6.1percent)and2016(4.9percent)tothe2014Montanaestimate($8.409billion).Wethenmultiplythisnumberby1.6percentanddividebytotal2016Medicaidexpansionspendingonbenefitsandclaims($315million).

TheEconomicImpactofMedicaidExpansioninMontana
36
Collectively,theseanalysessuggestthattotalhealthcarespendinginMontana
increasesbyanamountequaltobetween48-60percentoftotalMedicaidexpansion
spending.Inthemodelpresentedinthemainreport,weconservativelyassumethat48
percentofexpansionspendingisnewspending.
3.HowdoesMedicaidexpansionchangewhopaysforhealthcare?
ThefinalpartofdeterminingthedirecteffectsofMedicaidexpansionisdescribinghow
thesourceofhealthcarepaymentchanges.WithMedicaidexpansion,whopaysforcareis
relativelystraightforward.Thefederalgovernmentpaysformost(roughly90percentin
2020),thestatepaysalittle(roughly10percentin2020),and,becauseMontanahas
premiumsandcostsharing,thebeneficiariespayalittleaswell(lessthanonepercent).
WithoutMedicaidexpansion,whopaysforcareismorecomplicated.TableA2outlines
arangeofallocationsforthetypesofinsuranceexpansionbeneficiarieswouldhavehad
withoutexpansion.Theseestimatesprovideacrudeestimateforwhopaysforcare,but
therearecomplications.First,amongtheuninsured,mostspendingislikelyout-of-pocket;
however,someoftheirspendingmaybeoffsetbystateorfederalgovernmentprogramsor
bycharitabledonations.Second,amongthosewithemployersponsoredinsurance,
individualspayforpartofthecostintheformofpremiumsandout-of-pocketpayments.
Furthermore,economistsdebatewhopaystheemployershareofpremiums–the
employerortheemployee.
a.Federal
Thechangeinfederalspendingisgovernedby:
!"#"$%&! − !"#"$%&! = !! !" + !" + !" − ! − (!!!" + !")
where!! istheFMAPforexpansion,!"isexpansionspendingbypeoplewhootherwisewouldhavereceievedsubsidiestopurchasecoveragethroughtheexchange,!"isexpansionspendingbypeoplewhowouldhavebeencoveredbytraditionalMedicaid,!"isexpansionspendingbyeveryoneelse,!ispremiumspaidbyexpansionbeneficiaries,!! istheFMAPfortraditionalMedicaid,and!istheaverageexchagesubsidyforthosewhowouldhavereceivedthem.Overthelongruntheremaybeadditionalreductionsinfederal
spendingattributabletoMedicaidexpansion(e.g.,federalpaymentsforuncompensated
careweresupposedtobereducedbutthesereductionshavebeendelayed);however,we
havenotincludedthesepotentialreductionsinouranalysis.

TheEconomicImpactofMedicaidExpansioninMontana
37
Weassume!(averagespendingperexpansionbeneficiary)isthesameforallgroups.WeusethestatedFMAPforeachyear.Weassume!equals0.6percentoftotalspending(basedonstatebudgetreportsandforecasts).Wecompute!usingtheKaiserFamilyFoundation’sHealthInsuranceMarketplaceCalculatortoobtainsubsidyestimatesfor
someonewithanincomeequalto125percentFPLatfive-yearageintervalsfor2015and
140percentFPLfor2016-2019.Weaveragetheseamountsweightingbytheshareof
Medicaidexpansionbeneficiariesineachagegroup.59Tothisamount,weadd$1,500,the
averageapproximateannualCSRinMontanain2016.60Forfutureyears,weincreasethis
amountby5percent.
Wedonotincludeanychangeinfederalrevenuesinourcalculation.Forinstance,given
thatpaymentsforemployer-sponsoredhealthinsurance(“ESI”)arenottaxedasincome,
reducedspendingonESIwill(inpart)becomeincreasedincomeforworkers,proprietors,
orowners.Thisincomewillbetaxedatsomelevel.Suchrevenueincreasesoffsetthecost
ofexpansiontothefederalgovernment.However,wehavenotincludedsuchpaymentsas
partofourcalculationofthedirectimpactsofexpansion.
b.State
Thechangeinstatespendingisgovernedby:
!"#"$! − !"#"$! = !! !" + !" + !" − ! + !"#! + !"#! − !!!" + !"#! + !"#!
= !!(!" + !" − !) + !! − !! !" + !"#! − !"#! + (!"#! − !"#!)
whereallvariablesaredefinedthesameasinthefederalequationsand!! and!! arethestatesharesforexpansionandtraditionalMedicaid, !"#! − !"#! issavingstostate
facilitiesthatcannowbillMedicaidfor24hourinpatienthospitalizationandsimilar
savingstotheDepartmentofCorrections,and(!"#! − !"#!)issavingstothestatefromreducedspendingonmentalhealthandsubstanceabuse.Dataforthesavingfor24-hour
59http://dphhs.mt.gov/Portals/85/Documents/healthcare/MedicaidExpansionMemberProfile.pdf.60TheTrumpadministrationcanceledfederalCSRpaymentsfor2018.However,insuranceprovidersarestillobligatedtoprovidethem.Assuch,theyhaveraisedpremiums.Giventhestructureoffederalsubsidies,whichlimitpremiumstoapercentageofincomeforpeoplewithincomeslessthan400percentFPL,thefederalgovernmentstilleffectivelyfundsmostoftheCSRpaymentsbecausethegovernmentabsorbsmostoftheincreaseinpremiums.However,someoftheburdenforthehigherCSRpaymentswillfallonindividualswithincomesgreaterthan400percentFPLwhodonotqualifyforsubsidies.GiventhatMedicaidexpansionreducestheneedforCSRs,expansionmaylowerpremiumsforhigher-incomeMontanans.Wedonotincludethesesavingsinourmodel.

TheEconomicImpactofMedicaidExpansioninMontana
38
inpatientadmissionscomesfromthestateofficials.61Dataforthesizeofthesavingson
mentalhealthandsubstanceabusetreatmentcomesfromareportpreparedbyManatt.62
Wedonotincludeanychangeinstaterevenuesinourcalculation.Asdiscussedabove,
shiftingpeopleintotheexpansionlikelyleadstodirectchangesintaxrevenuethatmay
offsetpartofthecostofexpansiontothestate.However,wedonotincludetheserevenues
whencomputingthedirectimpactofexpansion.
c.Individualsandemployers
Thechangeinindividualspendingisgovernedby:
!"#! − !"#! = ! − !!! ∗ (!! + !!)! + (!! + !!)! + (!! + !!)!
where!equalstheindividual’sMedicaidexpansionpremium,Oequalsout-of-pocketspendingand!equalstheindividual’spremiumcontributionforeachtypeofcoverage(uninsured(U),unsubsidizeddirectpurchase(I),subsidizedexchangepurchase(X),
employer-sponsored(E))withoutexpansion.
WeuseMEPSspendingdatatocapturespendingamongtheuninsured.Weusethe
priceofanexchangepolicy(computedusingthesamemethodaswasusedtocomputethe
sizeoftheexchangesubsidy)tocomputethepremiumforindividualswithdirectpurchase
insurance.WeusedatafromtheMEPSInsurance/EmployerComponent63tocomputethe
individualcontributionforanindividualemployer-sponsoredplaninMontana.Wegrowall
valuesat5percentperyear.
Thechangeinemployerspendingequalstheemployercontributiontimesthenumber
ofpeoplewhoswitchfromanemployerpolicy.WealsouseMEPS-IEtoobtainaverage
employercontributionforanindividualpolicyinMontana.
CombinedtheseassumptionsguidehowweallocateMedicaidexpansionspendingin
theREMImodel.TableA5presentsareasonablerangeofallocationsgiventheabove
assumptions.Forinstance,onesetofassumptionsassumesthat48percentofMedicaid
expansionspendingsupportsnewhealthcarespending,9percentrepresentssavingsto
61Incorrespondence,stateofficialsdocumenta$2.8millionreductioninoutsidespendingonhealthcareintheDepartmentofCorrections.Theyalsonoteanadditional$2.6millionsavingstostatefacilitiesthatcannowbillMedicaidfor24hourinpatienthospitalization.62MedicaidExpansion:HowitaffectsMontana’sstatebudget,economy,andresidents.https://mthcf.org/wp-content/uploads/2018/06/Manatt-MedEx_FINAL_6.1.18.pdf63https://meps.ahrq.gov/data_stats/quick_tables_search.jsp?component=2&subcomponent=2

TheEconomicImpactofMedicaidExpansioninMontana
39
otherfederalprograms,5percentissavingstootherstateprograms,24percentrepresents
savingstoindividuals,and13percentrepresentssavingstoemployers.
TableA5:RangeofallocationsofMedicaidexpansionspendingacrossgroups Lowrange HighrangeNew 48% 55%Federal 9% 9%State 5% 5%Individuals 25% 25%Employers 13% 7%
C.Resultsfromalternativespecifications
TableA6presentsresultsfromseveralalternativeREMIspecifications.Ineach
specification,wekeepactualandprojectedMedicaidexpansionspendingfixed,butwevary
theshareofspendingthatsupportsnewhealthcarespending,thesharethatoffsetsother
federalorstatespending,andthesharethatoffsetsindividualoremployerspending.For
eachspecification,wepresentonlytheresultsfortheyear2020.
WhiletheassumptionsabouttheallocationofMedicaidexpansionspendingvary,the
basicorderofmagnitudeoftheresultsdoesnot.Givenprojectedspending,theREMImodel
calculatesthatMedicaidexpansiongeneratesroughly6,000jobs,roughly$350millionin
personalincome,androughly$430millioningrossdomesticproduct.Inthemaintext,we
presentthemostconservativeassumption.
TableA6:Alternativeeconomicimpactestimatesfor2020(millionsof$2018) Table1 Alternative1 Alternative2 Alternative3Jobs 5,906 5,977 6,080 6,272PersonalIncome
$348 $367 $351 $356
GDP $420 $428 $435 $449
Assumedallocationsbeneficiariesofexpansionspending
New:48%Federal:9%State:4%
Individual:27%Employer:12%
New:52%Federal:20%
State:9%Individual:12%Employer:8%
New:52%Federal:15%
State:7%Individual:14%Employer:14%
New:55%Federal:9%State:4%
Individual:24%Employer:9%
D.Differences-in-DifferencesModel
Thedifferences-in-differencesanalysespresentedinSectionIVresultfromestimating
equationswiththeform:

TheEconomicImpactofMedicaidExpansioninMontana
40
!!" = !!!"#!! + !!!"#!! + !!!"#!!+!!!"#!! + !!"!! + !! + !! + !!"
Wherethevariablesareasfollows:
• !!"istheoutcomeofinterest:ln(healthcareemployment),ln(healthcarecompensation,ln(healthcareGDP),ln(totalemployment).ThedataforeachoftheseoutcomeswasobtainedfromtheBureauofEconomicAnalysis’RegionalEconomicAccounts;
• !"#!" isavariableequalto1ifstateiisanexpansionstatejyearssinceexpansion(j=0isthefirstyearofexpansion),andzerootherwise;
• !!"isavectorofcontrolvariablesthatincludesln(totalpopulation),ln(tradedsectoremployment),ln(populationoverage65),ln(populationwithadisability),andln(populationoverage25withatleastaBachelor’sdegree)foreachstateandyear.Thedatafortotalpopulation,overage65,withadisability,andwithaBachelor’sdegreewereobtainedfromtheCensus.Totaltradedsectoremploymentwasobtainedbyapplyingestimatesforthepercentofemploymentineach2-digitNAICSindustryinthetradedsectorobtainedfromJensen(2012)tostate-year2-digittotalemploymentestimatesfromtheBureauofEconomicAnalysisRegionalEconomicAccounts;64
• !! arestatefixedeffects;and• !!areyearfixedeffects.
Weestimatethisequationusingdataforthe34includedstatesduringtheperiod2010-
2017.
Thecoreassumptionofadifferences-in-differencesanalysisistheparalleltrend
assumption.Thatis,thisanalysisrestsontheassumptionthat,intheabsenceofMedicaid
expansion,thechangeinoutcomesforexpansionstateswouldhavefollowedthesame
trajectoryasnon-expansionstates.
Onewaytotestthereasonablenessofthisassumptionistoexaminethechangein
outcomepriortoexpansion.Ifexpansionandnon-expansionstatesfollowedsimilar
trajectoriespriortoexpansion,itisplausiblethattheywouldhavefollowedsimilar
trajectoriesafterexpansion.Assuch,onecanperformadifferences-in-differencesanalysis
intheperiodspriortoexpansion.Ifoneobservesstatisticallysignificantresultsinthepre-
period,thentheexpansionstatesmayhavebeenfollowingadifferenttrajectorypriorto
expansionandthenon-expansionstatesmaynotprovideareasonablecontrolgroup.
64Jensen,J.B.(2011).Globaltradeinservices:fear,facts,andoffshoring.Washington,DC:PetersonInstituteforInternationalEconomics,Table2.3.

TheEconomicImpactofMedicaidExpansioninMontana
41
Totestthisassumptionweestimatethefollowingregression:
!!" = !!!!"#!!! + !!!!"#!!! +!!!!"#!!! + !!!"#!! + !!!"#!! + !!!"#!!+!!!"#!! +!!"!! + !! + !! + !!"
Thisdifferences-in-differencesanalysiscomparesthechangeinoutcomebetween
expansionandnon-expansionstateintheperiodspriortoexpansion.Wepresentselected
resultsinTableA7.Wedonotobserveaconsistentpatternofstatisticallysignificant
differences.Thereisabitofevidence(thoughnotstatisticallysignificant)thatexpansion
states’healthcaresectorsbegangrowingpriortoexpansion.Thismaybedrivenbythe
handfulofstatesthatbeganexpandingMedicaidin2013;itmayreflectprovidersbuilding
capacityinanticipationofexpansion;oritmayreflectsomeothereffect.65Totheextent
thesechangesaretheresultofexpansion,ourmainestimatesunderestimatetheeffectsof
Medicaidexpansion.
TableA7:Selectedcoefficientsfromtestsofparalleltrendassumption Ln(health
careemployment)
Ln(healthcareGDP)
Ln(totalemployment)
Ln(localsector
employment)4yearspre-expansion
-0.014(0.009)
-0.003(0.006)
-0.002(0.002)
-0.003(0.003)
3yearspre-expansion
-0.013(0.009)
0.000(0.005)
-0.001(0.002)
-0.002(0.003)
1yearpre-expansion
0.008(0.006)
0.010(0.007)
0.001(0.002)
0.002(0.003)
Notes:Cluster-robuststandarderrorsclusteredonstateinparentheses,+p<0.10,*p<0.05,**p<0.01;all
regressionsspecifiedasaboveandincludesamecontrolsasmainspecification.
Theinterpretationofourdifferences-in-differencesresultsisfurthercomplicatedby
thefactsthatnoteverystateexpandedatthesametimeandexpansiontimingvarieswith
respecttotheimplementationofotherpartsoftheACA.Assuch,wepresentanadditional
robustnesscheckwhereweseparatetheincludedexpansionstatesintothosethat
expandedin2014andthosedidnot.Theresultsfromtheseanalysesshowsimilareffects,
inspiteofthefactthatexpansioninthesegroupsoccurredatdifferentpointsrelativeto
otherchangesinducedbytheACA.
65Consistentwithanticipatoryeffects,healthcareemploymentinMontanabegantogrowatafasterrateinthequarterfollowingtheHELPact’spassage(whichwastwoquarterspriortoimplementation).

TheEconomicImpactofMedicaidExpansioninMontana
42
TableA8:Differences-in-differencesresultsfor2014expansionstatesandpost-2014expansionstates Ln(health
careemployment)
Ln(healthcare
employment)
Ln(totalemployment)
Ln(totalemployment)
Year1 0.020+(0.012)
0.009(0.006)
0.005(0.003)
0.000(0.002)
Year2 0.020(0.013)
0.016**(0.006)
0.006(0.004)
0.004+(0.002)
Year3 0.026+(0.014)
0.021*(0.010)
0.009*(0.004)
0.010**(0.003)
Year4 0.031+(0.016)
0.013*(0.005)
Expansionstates
Initial Late Initial Late
Notes:Cluster-robuststandarderrorsclusteredonstateinparentheses,+p<0.10,*p<0.05,**p<0.01;all
regressionsspecifiedasaboveandincludesamecontrolsasmainspecification.
Finally,wenotethestandarderrorsforourcoefficientsfrequentlyhoverrightaboveor
belowthestandard(thougharbitrary)0.05level.Thisisnotterriblysurprisinggiventhe
smallsamplesandrelativelysmalleffect.Wenotethatthecoefficients,though,remain
consistent.Changingthesetofstatesexamined,thesetofcontrolvariablesincluded,etc.
doesnotchangetheoveralltenoroftheresults.
E.ImpactofMedicaidExpansion/HELP-LinkonLaborForce
Participation
AsdiscussedinSectionV,laborforceparticipationamonglow-incomeMontanans
increasedafterMontanaexpandedMedicaid.Thesefindingsarebasedonananalysisof
microdatafromtheCurrentPopulationSurveyAnnualSocialandEconomicSupplement
andtheAmericanCommunitySurveyobtainedfromIPUMS.66
Inthemaintext,wefocusonindividualsages18-64withincomesbelow139percent
FPLwhodonotreportadisability.67Wereportthepercentageofpeopleinthisgroup
66Flood,S.King,M.,Ruggles,S.,andWarren,J.R,“IntegratedPublicUseMicrodataSeries,CurrentPopulationSurvey:Version5.0,”[dataset]Minneapolis:UniversityofMinnesota(2017).https://doi.org/10.18128/D030.V5.0;StevenRuggles,SarahFlood,RonaldGoeken,JosiahGrover,ErinMeyer,JosePacas,andMatthewSobek.IPUMSUSA:Version8.0[dataset].Minneapolis,MN:IPUMS,2018.https://doi.org/10.18128/D010.V8.067WecomputeincomeasapercentofpovertyusingIPUMS-CPSvariablesofftotvalandoffcutoff.

TheEconomicImpactofMedicaidExpansioninMontana
43
participatinginthelaborforcebeforeMontanaexpandedMedicaid(2012-2015)andafter
MontanaexpandedMedicaid(2016-2018).
TableA9:Differences-in-DifferencesRegressionAnalysisofImpactofMedicaidExpansiononLaborForceParticipationCurrentPopulationSurveyASEC Low-income
(0-138%FPL)HigherIncome(>138%FPL)
Low-income(0-138%FPL)
HigherIncome(>138%FPL)
Montana 0.056**(0.003)
0.043**(0.009)
0.062*(0.002)
0.049**(0.009)
After -0.053**(0.008)
0.007*(0.002)
-0.043**(0.006)
0.009**(0.002)
Montana*After
0.057**(0.006)
-0.022**(0.002)
0.037**(0.005)
-0.02**(0.002)
Controls Age,age2,sex,whitenon-Hispanic,child<18,stateand
yearFE
Age,age2,sex,whitenon-Hispanic,child<18,disabled
status,stateandyearFE
Population Non-disabled Non-disabled All AllN 129,925 617,458 154,341 658,173 AmericanCommunitySurvey Low-income
(0-138%FPL)HigherIncome(>138%FPL)
Low-income(0-138%FPL)
HigherIncome(>138%FPL)
Montana 0.074**(0.002)
0.032**(0.009)
0.079**(0.001)
0.043**(0.000)
After -0.036**(0.003)
0.006**(0.002)
-0.031**(0.003)
0.007**(0.001)
Montana*After
0.032**(0.001)
0.004**(0.001)
0.029**(0.001)
0.005**(0.001)
Controls Age,age2,sex,whitenon-Hispanic,child<18,stateand
yearFE
Age,age2,sex,whitenon-Hispanic,child<18,disabled
status,stateandyearFE
Population Non-disabled Non-disabled All AllN 2,040,660 8,091,695 2,604,575 8,848,404Note:Robuststandarderrorsclusteredatstatelevelinparentheses,**p<0.01,*p<0.05.
IntableA9,wereportresultsfromasimilardifferences-in-differencesanalysisthat
usesregressionanalysistoaddcontrolsforage,age2,sex,race(whitenon-Hispanic),
whethertheindividualhaschildrenlessthanage18,andstateandyearfixedeffects.The
effectsobtainedfromthisspecificationaresimilartothosereportedinthemaintext.

TheEconomicImpactofMedicaidExpansioninMontana
44
Relativetolow-incomepeopleinotherstates,laborforceparticipation(“LFP”)increased
by3-6percentagepointsmoreinMontanathaninotherareas.Thiseffectisnotobserved
amonghigher-incomeMontanans,suggestingthatthechangeinLFPisnotaMontana
effect,itonlyappliestolow-incomeMontanans.MedicaidexpansionandHELP-Link
provideaplausibleexplanationfortheseobservedeffects.
F.ImpactofMedicaidexpansiononhealthcaresector
TableA10presentsresultsthatareaquasi-replicationofthedifferences-in-differences
resultsinBlevin(2016,2017).Theyareaquasi-replicationbecauseouranalysisdiffersina
fewways.First,wepresentseparateresultsforproviderswhosefiscalyearextendsinto
somepartof2017(the2017group)andthosewhosefiscalyeardoesnot(the2016group).
Second,BlevinusesprovidercharacteristicsobtainedfromtheAmericanHospital
Associationinhisanalysis.Wedonothavethesedata,sowelimitthesampleanduse
controlvariablesobtainedfromCMS’sPOSfile.Third,weincludelateexpanders.Thatis,
weincludedatafromstates(NH,MI,PA,IA,MT,AK,LA)thatexpandedaftertheinitial
expansionintheanalysis.Third,weexcludealargersetofstatesas“pre-expansion”states.
InadditiontoexcludingstatesthatoptedintotheACAexpansionearly,wealsoexclude
statesthathadexpandedMedicaidtoalargersetofpeoplepriorto2014.68Fourth,wealso
tryandeliminatetheinfluenceofoutlierdatabyeliminatingthetopandbottomone
percentofnationaloutcomes;however,wearenotcertainweeliminatedoutliersinexactly
thesamemannerasBlevin.
Tocompletetheseanalyses,weusedataobtainedtheCenterforMedicareandMedicaid
Services’(“CMS”)HealthcareCostReportingInformationSystem(“HCRIS”)augmented
withdatafromCMS’sProviderofServices(“POS”)file.69AllMedicare-certifiedinstitutional
providersarerequiredtoreportinformationonfacilitycharacteristics,utilization,and
coststothesedatabases.Werestrictouranalysistoincludenon-federal,short-termand
criticalaccesshospitals.Wealsorestrictouranalysistoincludeproviderswhousea
consistent12-monthreportingperiodthroughouttheperiodexamined(2012-2017).70
Whilethesedatahavesomeknownlimitations(e.g.,implausiblevaluesforsome
variables),severalresearchershaveemployedthemtoinvestigatehospitalfinancial
68Specifically,weexcludeCalifornia,Colorado,Connecticut,Delaware,DC,Hawaii,Iowa,Massachusetts,Minnesota,NewJersey,NewYork,Vermont,andWashington.69HCRISdataobtainedfromhttp://www.nber.org/data/hcris.html70Someproviderschangedtheirreportingcycleatsomepoint.Asaresult,theseprovidersreportonlyapartialyearinoneoftheirreports.Thesesevenprovidersareexcludedfromtheanalysisbecausetheydonotfitconsistentlyintoeitherofthetwogroupsanalyzed.

TheEconomicImpactofMedicaidExpansioninMontana
45
performance.71Theyprovideconvenientaccesstoaconsistentsetofvariablesforalarge
numberofproviders.
HospitalsreportdatatoHCRISusingtheirownfiscalyear.Thiscreatesasignificant
challengeforthisanalysis.Noteveryobservationisclearlypre-orpost-expansion.For
someproviders,Medicaidexpansionbeganinthemiddleoftheirfiscalyear.Fortunately,
formostoftheseproviders,FY2017isavailable,sowehaveatleastonefullyearofpost
expansiondata,onethatincludesinformationfrom6to18-monthsafterthestartof
expansion.Otherprovidersfollowthecalendaryear.Theseprovidershaveacleanerpre-,
post-expansiondivide;however,weonlyhavedataforCY2016fortheseproviders
(CY2017dataisnotyetavailable).
TheresultsinTableA10aresimilartothosedescribedinBlevin(2016,2017).Relative
toprovidersinnon-expansionstates,providersinexpansionstatesexperiencerisingnet
Medicaidrevenues.Theaverageproviderinexpansionstatesenjoyedseveralmillion
dollarsofadditionalMedicaidrevenue.Theseeffectsgrowovertime.Similarly,relativeto
providersinnon-expansionstates,theaverageproviderenjoyedaseveralmilliondollar
reductioninuncompensatedcare.Theseeffectsalsogrowovertime.Theaverageprovided
sawuncompensatedcarefallby2.5percentoftotalexpensesmorethantheaverage
providerinnon-expansionstates.
Theaverageoperatingmarginalsoimprovedinexpansionstatesrelativetonon-
expansionstatesforthenearlytwo-thirdsofprovidersinthe2016group.Bythreeyears
afterexpansion,theaverageoperatingmarginhadimprovedby2.5percentagepoints.
However,operatingmarginsforprovidersinthe2017groupdonotshowsimilar
improvements.Theaveragechangeinoperatingmarginforthisgroupissmalland
statisticallyinsignificant.
TableA11replicatesTableA10butrestrictsthesetofMedicaidexpansionstatesto
includestateswithaboveaverageMedicaidgrowthafter2014.Thepotentialimpactof
Medicaidexpansionislikelylargerinthesestates.TableA2confirmsthis.Thebasicpattern
ofresultsissimilartothosepresentedabove;however,thesizeofthecoefficientsislarger
inalmosteverycase.
71SeeBlevin(2016,2017);Lindroothetal(2018);Bazzoli,G.J.,Fareed,N.,&Waters,T.M.(2014).Hospitalfinancialperformanceintherecentrecessionandimplicationsforinstitutionsthatremainfinanciallyweak.HealthAffairs,33(5),739-745.

TheEconomicImpactofMedicaidExpansioninMontana
46
TableA10:Differences-in-differencesanalysisofeffectofMedicaidexpansiononhospitalperformance
NetMedicaidRevenue UncompensatedCareUncomp.Careas%ofTotalExpenses
OperatingMargin
Yr 2017Group
2016Group
2017Group
2016Group
2017Group
2016Group
2017Group
2016Group
1 950568(740911)
1515697+(831667)
-617273(383278)
-2309174**(518020)
-0.006*(0.002)
-0.015**(0.003)
-0.003(0.007)
0.011*(0.005)
2 4936912**(1175690)
3086237*(1216801)
-2554580**(921546)
-3174756**(651988)
-0.018**(0.005)
-0.021**(0.003)
0.009(0.007)
0.014+(0.008)
3 6736014**(1485363)
4231590**(1214123)
-3062830**(877254)
-4446721**(518354)
-0.021**(0.006)
-0.026**(0.002)
0.004(0.008)
0.024*(0.010)
4 6979139**(2176856)
-3807065**(910543)
-0.023**(0.006)
0.002(0.009)
N 6481 10711 6334 10378 6332 10377 6347 10447
Notes:Authors’analysisofHCRISandPOSdataforshort-termandcriticalaccesshospitals.Allanalyses
includeproviderandyearfixedeffectsandcontrolsforruralstatus,bedcount,ownership,andservices
provided(openheartsurgery,alcoholanddrugservices,burncare,cardiaccatheterization,chemotherapy,
ob/gyn,andneurosurgicalservices).Providersinearlyexpansionstatesareexcluded.Topandbottomone
percentofoutcomemeasuresexcluded.AlldollarvaluesadjustedforinflationbasedonCPIformedical
expenses.Standarderrorsclusteredatstatelevel.+p<0.10,*p<0.05,**p<0.01.
TableA11:Differences-in-differencesanalysisofeffectofMedicaidexpansiononhospitalperformanceinaboveaverageexpansionstates
NetMedicaidRevenue UncompensatedCareUncomp.Careas%ofTotalExpenses
OperatingMargin
Yr 2017Group 2016Group
2017Group
2016Group
2017Group
2016Group
2017Group
2016Group
1 1775868+(1003950)
3750419**(872646)
-1125669**(264112)
-2547446**(403758)
-0.009**(0.003)
-0.017**(0.002)
-0.005(0.007)
0.012+(0.007)
29857050**(2786093)
8346136**(2555012)
-4579100**(790229)
-3702039**(498594)
-0.026**(0.005)
-0.026**(0.003)
0.018*(0.007)
0.014+(0.008)
311318310**(2111943)
7535823**(2084808)
-5097892**(634990)
-4253825**(488114)
-0.033**(0.005)
-0.025**(0.003)
0.015(0.010)
0.015+(0.008)
412657633**(3264866)
-5220159**(480428)
-0.030**(0.005)
-0.004(0.013)
N 5372 10163 5248 9737 5247 9736 5270 9742
Notes:Authors’analysisofHCRISandPOSdataforshort-termandcriticalaccesshospitals.Allanalyses
includeproviderandyearfixedeffectsandcontrolsforruralstatus,bedcount,control,andservicesprovided
(openheartsurgery,alcoholanddrugservices,burncare,cardiaccatheterization,chemotherapy,ob/gyn,and
neurosurgicalservices).Onlyaboveaverageexpansionstatesandnon-expansionstatesincluded.Topand
bottomonepercentofoutcomemeasuresexcluded.AlldollarvaluesadjustedforinflationbasedonCPIfor
medicalexpenses.Standarderrorsclusteredatstatelevel.+p<0.10,*p<0.05,**p<0.01.

TheEconomicImpactofMedicaidExpansioninMontana
47
G.ANoteonWoodworkEffects
SomearguethatthecostsofMedicaidexpansionshouldinclude“woodwork”effects,
whichmeansthattheavailabilityofMedicaidexpansionincreasesenrollmentintraditional
Medicaid.Ifso,thecostofMedicaidexpansioncouldincludethecostsassociatedwiththese
enrollees.
Wedonotincludewoodworkeffectsinthisanalysis,primarilybecausetheliterature
findsthattheACAincreasedenrollmentintraditionalMedicaid,buttheseincreaseswere
notrelatedtoMedicaidexpansion.Forinstance,onerecentstudyfound“similarly-sized
woodworkeffectsinallgroupsofstates,regardlessofMedicaidexpansionstatus.”72
Similarly,ourownanalysisofwoodworkeffectsinlate-expansionstatesdoesnotfind
evidencethatMedicaidexpansionincreasestraditionalMedicaidenrollment.
Ifoneweretoincludewoodworkeffects,itwouldbeimportanttoincludebothbenefits
andcosts,suchastheeffectsofincreasedactivityassociatedwiththisspending.
Furthermore,evenifoneassumesthatthereissomelevelofwoodworkeffectsassociated
withtheimplementationofMedicaidexpansion,oneshouldnotassumethatending
Medicaidexpansionwilleliminatethesecosts.Itisnotclearwhetherthoseeligiblefor
traditionalMedicaidwillreturntobeinguninsuredifMedicaidexpansionweretocease.It
seemslikelythatmanywouldremain.
H.Summaryofchangestopreviousreport
ThisreportupdatesandreplacesourApril2018report,TheeconomicimpactofMedicaidexpansioninMontana.Thecoremessageofbothreportsisthesame:
MedicaidexpansionbringsasubstantialamountofmoneyintoMontana’seconomy.
ThismoneycirculatesthroughMontana’seconomyincreasingtotalemployment
andincomebyapproximately1percentagepoint.Inadditiontothethousandsof
jobsandhundredsofmillionsinincome,Medicaidexpansiongeneratesother
benefits,e.g.,improvedaccesstohealthcare,betterhealth,betterfinancialhealth,
andlowercrime.InMontana,implementationofMedicaidexpansionandthe
associatedHELP-Linkprogramwasalsoassociatedwithimprovementsinlabor
forceparticipationamonglow-incomeMontanans.Similarimprovementswerenot
observedamonglow-incomeresidentsinotherstatesoramonghigherincome
Montanans.WhilethestatemustpaypartofthecostofMedicaidexpansion,the
72Frean,M.,Gruber,J.,andSommers,B.D.,“PremiumSubsidies,theMandate,andMedicaidExpansion:CoverageEffectsoftheAffordableCareAct.”JournalofHealthEconomics53(2017):72-86.

TheEconomicImpactofMedicaidExpansioninMontana
48
combinationofbudgetsavingsattributabletoMedicaidexpansionplusthetax
revenuefromincreasedeconomicactivitymorethanoffsettheexpectedcosttothe
statebudget.
However,therearedifferencesbetweenthetworeports.Wesummarizethemain
differencesbelow.
(1) ActualandprojectedMedicaidexpansionspendingishigherinthenewreport.Thisgenerateslargereconomicimpacts.
Inourfirstreport,weprojectedMedicaidexpansionspendingusingacombinationof
datathatincludedexpansionspendingreportedbyDPHHSthroughlate201773,an
enrollmentforecast,andapermemberspendingforecast.74
Inthisreport,weusetheactualandprojectedspendingreportedbythestateonpage
13oftheLegislativeFiscalDivision’sLegislativeBudgetAnalysis:2021Biennium,Volume1:StatewidePerspectives.75
AsshowninFigure1,spendingintheLFDreportishigherthanweassumedinour
priorreport.Thedifferencelikelyreflectsavarietyoffactors:lagsinprocessingclaims,
higherenrollmentin2018-2020thanweassumed,andhigherspendingperbeneficiary
thanweweassumed.
Higherspendinggenerateslargereconomicimpacts.Inourlastreport,wereported
impactsofroughly5,000jobsand$280millioninpersonalincome.Inthisreport,we
reportimpactsofroughly6,000jobsand$350millioninpersonalincome.Thevast
majorityofthisdifferenceinimpactisattributabletothedifferenceintotalexpansion
spending.
(2) Theallocationofdirectimpactschangedbasedonupdateddataandadditionalanalyses.
Medicaidexpansionaddsmoneytothepocketsoffivegroups:providers(whoenjoy
increaseddemandandreduceduncompensatedcare),thefederalgovernment(Medicaid
73Specifically,wereportedspendingonhealthcareservicesintheMedicaidExpansionMemberProfilereportsregularlygeneratedbyDPHHS.https://dphhs.mt.gov/Portals/85/Documents/healthcare/MedicaidExpansionMemberProfile.pdf74OurspendingforecastwaslargelybasedontheperMedicaidexpansionbeneficiaryspendingforecastincludedinCentersforMedicareandMedicaidServices.2016ActuarialReportontheFinancialOutlookforMedicaid,(2016). 75https://leg.mt.gov/content/Publications/fiscal/BA-2021/2021BienniumVolume1_Final.pdf

TheEconomicImpactofMedicaidExpansioninMontana
49
expansionreducesspendingonsomefederalprograms),stategovernment(Medicaid
expansionreducesspendingonsomestateprograms),individuals,andemployers.How
muchexpansionspendingeachgroupcapturesaffectstheREMIresults.
TableA12comparestheallocationsweusedtocomputethemainresultsinboth
reports.First,inthisreport,wereducedshareofexpansionspendingthatrepresentednew
healthcarespendingfrom52percentto48percent.Thischangewasbasedonseveralnew
analysesconductedforthisreport.TheseanalysessuggesttheMedicaidexpansion
increasedtotalhealthcarespendingbybetween48-60percent.Whilethevalueassumedin
ourpreviousreportfallssquarelywithinthisrange,weoptedtochoosethebottomendof
therangeinordertoobtainamoreconservativeestimate.
TableA12:Allocationofexpansionspendingbetweenreports April2018 January2019New 52% 48%
Federal 19% 9%
State 8% 4%
Individual 12% 27%
Employer 9% 12%
Second,wereducedtheassumptionfortheshareofMedicaidexpansionspendingthat
wastransferredwithinthefederalgovernmentfrom19percenttoninepercent.Inpart,
thisreflectsadownwardrevisioninourestimatefortheshareofpeoplewhowouldhave
enrolledintraditionalMedicaidwithoutexpansion.Inpart,itreflectsadownwardrevision
intheshareofbeneficiarieswhowouldhavereceivedexchangesubsidieswithout
expansion.ThedeclineintheshareofspendingintraditionalMedicaidmostlystemsfrom
thefactthattheprojectedMedicaidsavingsremainedconstantbutestimatesforspending
increased.Thedeclineinexchangesubsidesreflectsadditionalanalysis.Inourfirstreport,
welookedatthechangeintheshareofexpansioneligiblepeoplewithdirectpurchase.To
ensureamoreconservativeestimate,assumedalargeshareofsuchpeoplereceived
subsidies.Inthisreport,weconductednewanalysesusinglongitudinaldatafromtheMEPS
thatindicatethattheshareofpeoplewhotransitionbetweenMedicaidandtheexchanges
isverysmall.Assuch,wereducedourassumptionfortheshareofexpansionbeneficiaries
whowouldhavereceivedexchangesubsidies.
Third,wereducedourassumptionfortheshareofexpansionspendingthatreduced
statespending.ThedownwardrevisionintheassumedshareofwithinMedicaidtransfers
describedinthepreviousparagraphdrivesthisresult.

TheEconomicImpactofMedicaidExpansioninMontana
50
Fourth,weincreasedourassumptionsforhowmuchMedicaidexpansionspending
reducedhealthcarespendingamongindividualsandemployers.Thisisthenatural
byproductofreducingtheassumedamountsintheothercategories.Theincreaseineach
oftheseareasreflectsbothanincreaseinthenumberofpeopleweassumewouldfallinto
thesecategorieswithoutexpansionandanincreaseinwhatweassumeeachpersonin
thesecategorieswouldpayinpremiumsandout-of-pocketcosts.
Thesechangesmakeonlyasmallimpactonourresults.TableA6Alternative1presents
resultsthatapplytheoldallocationtothenewspendinglevels.Thedifferencesinthe
resultsareveryminor(e.g.,lessthan100jobsin2020).
(3) WepresentanewanalysisthatestimatestheexpectedimpactofMedicaidexpansioninMontanabasedontheobservedchangesinotherexpansionstates.
TheresultsfromtheREMImodelrestonalargenumberofassumptions.First,theREMI
modelitselfisacomplicatedsetofassumptionsabouthowvariouspiecesoftheeconomy
interact.Second,weinputavarietyofassumptionsabouthowMedicaidexpansiondirectly
changesMontana’seconomy.WhiletheREMImodel’sassumptionshavebeenrigorously
investigatedandwhileweendeavoredtoselectreasonableestimatesforthedirecteffects
ofexpansion,itispossiblethatsomeofourassumptionsmissthemark.
GiventhatotherstatesexpandedMedicaidandmostexpandedbeforeMontanadid,we
canlookatwhathappenedintheseotherstatestoobtainanalternativeestimatefor
Medicaidexpansion’seffectsinMontana.Specifically,wedevelopadifferences-in-
differencesestimatethatcomparesthechangeinoutcomesinexpansionstatestothe
changeinoutcomesinnon-expansionstates.Theseresultsdonotrequireassumptions
abouttotalexpansionspending,theshareofthisspendingthatisnew,etc.Theysimply
provideananswertothequestion:“Howmuchdidthetrajectoryofeconomicactivityin
expansionstateschangerelativetonon-expansionstatesafterexpansion?”
ToobtainanestimatefortheeffectofexpansioninMontana(asopposedtotheaverage
effectofexpansionoverall),welimitthesetofstatesincludedtothosewhereexpansion’s
effectsoninsurancecoverageweresimilartoMontana.Conveniently,theuninsuredrate
amongtheeligiblepopulationinthissetofstatesmorecloselyresembledthatinnon-
expansionstatespriortoexpansion.
TheresultsfromthismodelareconsistentwithourREMIresults.Weestimatethat,
afterthreetofouryears,Medicaidexpansionincreasesthesizeofthehealthcaresectorby
roughlythreepercentagepointsandtotalemploymentbyroughlyonepercentagepoint.

TheEconomicImpactofMedicaidExpansioninMontana
51
Theconsistencybetweenthesetwoapproachesprovidesconfidencethatourestimates
fortheeconomicimpactsofexpansioninMontanaareroughlycorrect.
(4) WeupdateouranalysisoftheimpactofexpansionandHELP-Linkonlaborforceparticipationamonglow-incomeMontanans.
Weupdatetheanalysispresentedinourfirstreportonthechangeinlaborforce
participationamonglow-incomeMontanansbyaddinganadditionalyearofdatafromboth
theCurrentPopulationSurveyandtheAmericanCommunitySurvey.Specifically,weadd
datafromthe2018CurrentPopulationSurveyAnnualSocialandEconomicSupplement
andthe2017AmericanCommunitySurvey.Addingthisadditionaldatareducedthesizeof
theobservedchangesfromsixtoninepercenttofourtosixpercent.However,theseresults
remaineconomicallymeaningfulandstatisticallysignificant.
(5) Weupdatedourreviewofotherexpansioneffects.
Wereviewedadditionalliteratureandhighlightedsomeadditionalfindingsofthe
broadereffectsofMedicaidexpansion.Inparticular,weaddedextensivediscussionofthe
impactofexpansiononthefinancialhealthofproviders,particularlyinruralareas.Several
studiesshowtheMedicaidexpansionprovidesaparticularlylargeboontoruralproviders.
Consistentwiththis,weshowthathealthcareemploymentinruralMontanagrewquickly
followingexpansionafterseveralyearsofstagnation.
(6) Weupdatedouranalysisofexpansion’sfiscaleffects,butthechangesaretrivial.Wecontinuetoestimatethatsavingsandrevenueattributedtoexpansionexceedexpectedcosttothestate.
Inthenewreport,ourestimatesforstatebudgetsavingsattributedtoexpansion,the
expectedcosttothestate,andtheexpectedrevenuesfromincreasedactivityallchange.
However,theneteffectofthesechangesissmall.WecontinuetoestimatethatMedicaid
expansionhasapositiveimpactonthestatebudget.