Embed Size (px)
Citation preview

DERENDEKE ELSEVIER Drug and Alcohol Dependence 40 (1995) 27-35
Buprenorphine treatment of opioid dependence: clinical trial of daily versus alternate-day dosing
Rolley E. Johnson *, Thomas Eissenberg, Maxine L. Stitzer, Eric C. Strain, Ira A. Liebson, George E. Bigelow
Behavioral Pharmacology Research Unit, Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, 5210 Nathan Shock Drive, Baltimore, MD 21224-6823. USA
Received 10 May 1995; accepted 7 September 1995
Abstract
Buprenorphine, a mu-opioid partial agonist, has demonstrated efficacy for the treatment of opioid dependence comparable to that of methadone. The clinical utility of buprenorphine would be enhanced if it could be dosed on a less than daily basis. The current study is a parallel-group outpatient clinical trial of daily versus alternate-day dosing with 8 mg sublingual (s.1.) buprenor- phine. Participants were randomly assigned to daily (n = 51) or alternate-day (n = 48) schedules of active medication administration for an 1 l-week double-blind trial. Patients assigned to alternate-day buprenorphine received placebo every other day. Primary out- come measures were retention in treatment and urine specimens positive for opiates. Clinic attendance, dose adequacy ratings, withdrawal symptomatology, and urine specimens positive for cocaine were secondary outcome measures. Neither endpoint analy- sis with the intent-to-treat sample nor time course analysis with treatment completers revealed any statistically significant differ- ences between the dosing schedules on any outcome measure. Examination of 95% confidence intervals suggested a non-significant trend for the daily dosing schedule to have superior clinical efficacy at the dose tested. Nevertheless, these results are generally consistent with previous studies of less than daily dosing with buprenorphine and support the conclusion that an alternateday dosing schedule can be effective in and acceptable to a substantial portion of patients.
Keywords: Buprenorphine; Drug abuse; Clinical trial; Opioid dependence; Altemateday dosing; Eff~~cy
1. Introduction
Opioid agonist maintenance therapy is a common strategy in the treatment of opioid dependence. Opioid agonists are effective, in part, because they maintain patient participation in treatment, attenuate the effects of concurrently administered opioids, and prevent opioid withdrawal. The United States Food and Drug Administration has approved two mu-opioid agonists, methadone and levo-alpha acetylmethadol (LAAM), as opioid dependence treatments (naltrexone, a third ap- proved treatment, is an opioid antagonist). Methadone requires daily dosing, while LAAM can be used on a three time per week dosing schedule (Ling et al., 1976; Judson and Goldstein, 1979; Freedman and Czertko, 1981).
Buprenorphine is a mu-opioid partial agonist under
l Corresponding author. Fax: (410) 550 0030.
development as another agonist pharmacotherapy for opioid dependence. Buprenorphine displays the advan- tages of a pure mu-opioid agonist; its subjective effects are agonist-like (e.g., Jasinski et al., 1978; Pickworth et al., 1993), it blocks the effects of concurrently ad- ministered opioids (e.g., Jasinski et al., 1978; Bickel et al., 1988; Rosen et al., 1994), and it attenuates opioid withdrawal (e.g., Kosten et al., 1993; Cheskin et al., 1994). Buprenorphine also suppresses heroin use (Mello and Mendelson, 1980; Mello et al., 1982), and is safer than pure mu-agonists like methadone and LAAM. Maximal and clinically safe buprenorphine-induced res- piratory depression is reached at 4 mg s.l., and doses as high as 32 mg s.1. have been safely administered to hu- mans (Walsh et al., 1994; Walsh et al., 1995). A 3-day induction onto buprenorphine has been used without adverse reaction in opioid treatment populations (e.g., Johnson et al., 1989; Johnson et al., 1992).
Buprenorphine has a long duration of action (Jasinski
0376-8716/95/$09.50 0 1995 Elsevier Science Ireland Ltd. All rights reserved SSDI 0376-8716(95)01189-6

28 R.E. Johnson et al, /Drug and Alcohol Dependence 40 (1995) 27-35
et al., 1978; Lewis, 1985; Johnson et al., 1989) which has led some to suggest that, as with LAAM, less than daily dosing without loss of efficacy might be feasible (Fudala et al., 1990; Resnick et al., 1993; Amass et al., 1994). If effective, less than daily dosing would reduce clinic visits, increasing both patient convenience and the num- ber of patients that could be treated at a single clinic. Also, less than daily dosing would circumvent the need for take-home medication, and thereby reduce the possibility of diversion and illicit use of buprenorphine. Finally, less than daily dosing could be offered as an in- centive in concurrent contingency management treat- ment to promote improved treatment participation and outcomes (e.g., Stitzer et al., 1992).
There are two reports of controlled evaluations of short-term, alternate-day dosing with buprenorphine (Fudala et al., 1990; Amass et al., 1994); both studies describe small groups of opioid-dependent volunteers (n = 18 and n = 13, respectively). Fudala et al. (1990) studied inpatient volunteers who were stabilized on bu- prenorphine (8 mg s.1.) for 16 days, and then assigned (double-blind) to either daily or alternate-day dosing for the pext 18 days. Daily dosing with 8 mg buprenorphine stabilized subjective effects better than did alternate-day dosing with the same dose; on 5 of 7 subjective measures patients in the alternate-day group displayed a fluc- tuating pattern of responding that co-varied with active versus placebo doses (e.g., ratings of agonist effects were higher on days when active drug was administered). The clinical significance of this fluctuating pattern is not clear because the two groups (alternate-day versus daily) did not differ on overall mean ratings on these measures.
Amass et al. (1994) evaluated daily versus altemate- day buprenorphine administration in an outpatient treatment population. In this crossover study out- patients were maintained for 13 consecutive days of treatment using an individually titrated buprenorphine dose (doses were either 2 (n = 2), 4 (n = 6), or 8 (n = 5) mg/70 kg s.l.), and then entered a 2-part crossover phase (42 days total) where they were given either their main- tenance dose daily, or twice their maintenance dose on alternate days. The two dosing regimens were equally effective for suppressing withdrawal and promoting retention and compliance.
The present study extends observations of Fudala et al. (1990) and Amass et al. (1994) by assessing treatment outcomes during alternate-day versus daily dosing with a single uniform 8-mg s.1. buprenorphine dose. This study, a large sample, parallel-group clinical trial, was designed to determine the clinical efficacy of an 8-mg alternate-day dosing schedule.
2. Materials and method
2. I. Patients Male and female volunteers admitted to a short-term
opioid treatment research clinic were enrolled in two consecutive studies, spanning a 20-week period. Criteria for patient admission for both studies, and results from study 1 are reported elsewhere (Johnson et al., 1995, this issue). Briefly, in study 1, 150 patients (who met DSM- III-R diagnosis of opiate dependence, according to the structured clinical interview for DSM-III-R; Spitzer and Williams, 1987) were randomly assigned to 1 of 3 groups: placebo, 2 mg or 8 mg s.1. buprenorphine. An initial exclusion criterion required that at least 1 of 2 urine specimens collected test negative for cocaine; be- cause many patients seeking treatment at our clinic could not meet this criterion, it was removed after the first 30 admissions. Study 1 lasted 14 days. Forty pa- tients dropped out of treatment during study 1. Follow- ing study 1 (during days 15-21) the remaining 110 patients were stabilized on 8 mg buprenorphine s.1. Eleven patients dropped out of treatment during this stabilization week. The second study (results of which are reported here) lasted 11 weeks (weeks 4-14), and is based on the 99 patients who remained in treatment past study day 21.
The study was approved by the local institutional re- view board, and each patient gave written, informed consent prior to participation. During the consent pro- cedure, patients were informed that they would be ran- domly assigned to treatment conditions that might involve placebo dosing on some days. At the end of the third week of treatment, patients were randomly assign- ed to either daily (n = 51) or alternate-day (n = 48) dos- ing groups, stratified by race and gender. Table 1 summarizes demographic information by group. The groups were well-balanced on virtually all demographic variables. However, there were small but statistically significant differences in the heroin use in the 30 days prior to admission and previous treatment episodes (both less in the alternate-day group). The difference in mean heroin use resulted from the presence of 4 patients in the alternate-day group who reported atypically low recent rates of heroin use (6-20 days of the past 30 days, versus an average of 29 days for all other patients). Removing these four patients from all subsequent analy- ses does not change the pattern of results. The daily and alternate-day groups did not differ significantly on any other demographic characteristic.
2.2. Procedure This 1 l-week study used a.randomized, double-blind,
parallel-group design. During treatment week 4, follow- ing completion of study 1 (weeks l-2) and 1 week of stabilization on 8 mg buprenorphine (week 3) patients assigned to the alternate-day dosing group underwent a dose step-down procedure on alternate days (i.e., se- quential daily doses of 8 mg, 6 mg, 8 mg, 4. mg, 8 mg, 2 mg, 8 mg, 0 mg) to acclimate them gradually to the alternate-day schedule. During this period patients

R. E. Johnson et al. /Drug and Alcohol Dependence 40 (1995) 27-35 29
Table I Demographic characteristics by treatment group
Demographic characteristics
Buprenorphine dose schedule
Daily Alternate-day (n = 51) (n = 48)
Female (“‘u) Non-white (%) Marital status (%)
Single Married Separated
Employed (“/u) Legal problems (%) Education
Mean S.D.
Age Mean SD.
Past 30 day drug use (days)
Heroin* Mean SD.
Cocaine Mean SD.
Lifetime drug use Wars)
Heroin Mean SD.
Cocaine Mean S.D.
Previous treatment episodes*
Mean S.D.
21 31 53 46
45 38 22 21 33 35 39 33 33 38
II.5 11.27 1.6 1.5
34 33.57 6.57 6.68
29.92 28.38 0.34 4.57
6.61 6.21 10.29 9.3
8.70 8.25 7.04 7.24
2.10 1.37 3.43 2.41
I.90 1.21 1.63 1.38
*P < 0.05, group differences were significant for Past 30 day heroin use and Previous treatment episodes.
assigned to daily dosing continued to receive their 8-mg maintenance dose. During weeks 5-14 patients were maintained on 8 mg s.1. of buprenorphine daily or on alternate days, with the alternate-day group receiving placebo medication on the intervening days. Buprenor- phine was prepared in a 30% ethanol solution. Placebo consisted of the 30% ethanol vehicle. All dosing was double-blind.
Patients were required to come to the clinic daily to receive their medication. Medication administration was supervised and patients held their medication under the tongue for 5 min (Johnson et al., 1995). Participants who missed 5 consecutive days of clinic attendance were dropped from the study. Intermittent attendance was tolerated. However, no adjustments were made to the dosing schedule for alternate-day patients on occasions when a patient failed to attend the clinic and missed
medication. Thus, if a patient assigned to alternate-day dosing missed an active dose, that patient went without active medication for three consecutive days. No take- home medication was provided. Routine individual and group counseling were provided. In brief, a counselor (assigned to each patient) worked with the patient to set treatment goals and develop an individualized treatment plan. The two groups did not differ in the amount of counseling received; patients in both groups had an average of 6 individual counseling sessions of average 29-30-min duration. Group therapy focused primarily on relapse prevention. Routine medical services were also provided. At the end of the 11 weeks of the second study (week 14), all patients who remained in treatment began a dose reduction period that ended with placebo dosing for the last 10 days of treatment (weeks 19 and 20). Patients seeking longer-term treatment were assis- ted with transfer to other local programs.
2.3. Primary outcome measures Retention in treatment is defined as the number of
weeks patients (n = 99) remained in the study (weeks 4- 14) before reaching the end of the protocol or missing 5 consecutive days.
Percent of opiate-positive urine specimens is defined as the percent of all urine specimens provided by an in- dividual during the study that tested opiate-positive by enzyme-multiplied immunoassay (greater than or equal to 300 @ml; EMIT, Syva Cot-p, Palo Alto, CA). Super- vised urines were collected on Mondays, Wednesdays and Fridays; therefore an individual could provide a maximum of three urines each week and a maximum of 33 for the entire evaluation period.
2.4. Secondary outcome measures Percent of urine specimens positive for cocaine is
defined as the percent of urine specimens provided by an individual during treatment that tested cocaine-positive by EMIT (greater than or equal to 300 @ml).
Clinic attendance is defined as percent of available treatment days on which a patient received his or her assigned dose (either placebo or 8 mg buprenorphine). This measure is intended as an index of treatment com- pliance.
Dose adequacy is defined as a response on a visual analog scale (VAS) on which patients were instructed to make a vertical mark on a 100~mm line in response to three questions: (a) “How well has this dose of medicine been holding you for the past week (seven days)?” (HOLD); (b) “For the past week (seven days) how much have you felt hooked by the medicine?” (HOOK); and (c) “For the past week (seven days) how much have you liked the medicine?” (LIKE). The HOLD VAS was an- chored by ‘too low’ on the left and ‘too high’ on the right; HOOK and LIKE were anchored by ‘not at all’ on the left and ‘a lot’ on the right. Each VAS measure was

30 R.E. Johnson et al. /Drug and Alcohol Dependence 40 (1995) 27-35
scored as distance (in mm) from the left end of the line to the vertical mark of the patient. Patients completed the VAS weekly during the study period.
Opiate withdrawal symptom checklist is defined as the total score from a weekly withdrawal symptom ques- tionnaire containing a list of 20 typical withdrawal symptoms. The 20-item list was headed by the question “Have you had any of these symptoms or feelings in the past 24 h?“. Each item in the list consisted of 10 discrete open circles, anchored by ‘not at all’ on the left and ‘se- vere’ on the right. Patients were instructed to darken the single circle that best described the intensity of the symptom. Each item was scored on a 0-Ppoint scale. Thus the total (summed) score for this measure could range from 0- 180. The items were muscle cramps, de- pressed or sad, painful joints, yawning, hot or cold flashes, trouble getting to sleep, sick to stomach, ir- ritable, runny nose, poor appetite, weak knees, sneezing, tense and jittery, watery eyes, abdominal cramps, fitful sleep, chills and goose-flesh, backache, bothered by noises, and skin clammy and damp. Patients completed the withdrawal symptom scale once weekly. It should be noted that patients assigned to alternate-day dosing sometimes responded to the opiate symptoms question- naire the day after active dosing, and other times responded the day after placebo dosing.
2.5. Data analysis Retention data were evaluated in a survival analysis
using the Lee-Desu statistic (Lee and Desu, 1992). Urine, clinic attendance, and questionnaire data were analyzed two ways: (a) endpoint analysis using the intent-to-treat sample (n = 99) and (b) time course anal- ysis using a sample of treatment completers (completers were defined as those patients who completed study 1 and for whom data were collected through all 11 weeks of study 2; n = 56). All proportional data (e.g., urine re- sults) were analyzed both as raw data and following an arcsine transformation in order to clarify potentially meaningful differences at the extremes of the distribu- tion (Snedcor and Cochran, 1989). As these analyses yielded equivalent results, the raw data are presented for clarity.
. .
2.5.1. Endpoint analysis. An endpoint was defined as the average of the data points collected in the last two weeks of the participation of each patient in the study. Thus if a patient remained in treatment through week 7, data collected in weeks 6 and 7 were averaged to form a single score for each variable. If a patient completed only one week (e.g., week 4), data from that week were used for this endpoint analysis. Using this definition, endpoints were calculated for all patients. In order to better understand why patients failed to complete the 1 l-week treatment evaluation period, endpoints were submitted to a two-factor analysis of variance (ANOVA), with dosing schedule (daily and altemate-
day) and completion status as between subjects factors. For retention data, the total days in treatment (possible range of l-77) for each patient were submitted to a single factor (dosing schedule) ANOVA.
Ninety-five percent confidence intervals were calculated for differences between the means (daily minus alternate-day group) obtained in endpoint analy- sis. Taking variability around sample mean differences into account, confidence intervals give the range of out- comes likely to occur with repetitions of the experiment. If a 95% confidence interval (C.I.) contains the null value (0 in the case of mean differences) then there is some probability that the true difference between means is zero or in the direction contrary to the hypothesis. The CL can provide an estimate of the clinical benefits of an intervention as well as providing information about statistical significance. A C.I. allows clinicians to decide if an intervention is worth delivering, given that the effect to be expected will generally be within the bounds of the interval (Borenstein, 1994).
2.5.2. Time course analysis. A two-factor analysis of variance (ANOVA) was performed with dosing schedule (daily or alternate-day) as a between subjects variable, and study week (4-14) as a within subjects variable. Subjects included in these analyses are those who com- pleted 14 weeks of treatment and provided data for each of the 11 treatment evaluation weeks of the present study. Urine data sample sizes were n = 32 for daily dos- ing and n = 20 for alternate-day dosing. Clinic atten- dance and subjective report data sample sizes were 34 for daily dosing and 22 for alternate-day dosing.
3.Results
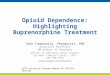
3.1. Primary outcome measures: endpoint analysis 3.Z.1. Retention in treatment. Fig. 1 shows the percent
of patients (n = 99) who remained in the study (weeks 4- 14) by dosing schedule and study week. Retention did not differ significantly between daily and alternate-day dosing schedules (P > 0.05) (Lee and Desu, 1992), though the two schedules appear to diverge over weeks with a trend toward greater retention for patients assign- ed to the daily dosing schedule.
The single-factor (dosing schedule) ANOVA on the total days of patients in treatment revealed no difference between daily and alternate-day dosing (F < 1). Table 2 displays the group means, and the 95% confidence in- terval for the difference between the means. As can be seen from Table 2, patients assigned to the daily dosing schedule remained in treatment, on average, 1.9 days longer than did patients assigned to the alternate-day dosing schedule (95% C.I. of -8.7 to 12.5 days, ns).
3.1.2. Mean percent of urine specimens positive for opiates. Endpoint analysis (n = 98, one patient failed to submit at least one urine) on this primary outcome mea- sure revealed a significant main effect of treatment com-

R. E. Johnson et al. /Drug and Alcohol Dependence 40 (1995) 27-35 31
Retention
-t- Daily
WEEK
Fig. 1. Retention by group for the 99 patients who began either daily (8 mg) or alternate-day (8 mg, placebo) treatment with buprenorphine.
pletion status (F(1,94) = 9.1, P c .Ol), but no significant interaction with or main effect of dose schedule (Fs < 1). As can be seen in Table 2, patients assigned to the daily dosing schedule submitted, on average, 11.9% fewer opiate-positive urines in the last 2 weeks of treat- ment than did patients assigned to the alternate-day dos- ing schedule (95% CL of -28.1% fewer to 4.3% more opiate-positive urines submitted; ns). Table 3 shows that patients who completed the study submitted, on aver- age, 26.1% fewer opiate-positive urines in their final 2 weeks of treatment than did patients who failed to com-
Table 2 Endpoint analysis of daily versus alternate-day groups
plete the 1 l-week study, independent of dosing schedule (95% C.I. of -41.4% to -lO.ti%, P c 0.01).
3.2. Secondary outcome measures: endpoint analysis 3.2.1. Percent of urine specimens positive for cocaine.
Endpoint analysis (n = 98, one daily patient failed to submit at least 1 urine) revealed a significant main effect of completion status (F(1,94) = 11.2, P < O.Ol), but no significant interaction or main effect of dose schedule (Fs < 1). As can be seen in Table 2, patients assigned to the daily dosing schedule submitted, on average, 2.4% more cocaine-positive urine specimens in the last 2 weeks of treatment than did patients assigned to the alternate-day dosing schedule (95% C.I. of -20.3% to 15.5, ns). Table 3 shows that patients who completed the study submitted, on average, 27.7% fewer cocaine- positive urine specimens in their final 2 weeks of treat- ment than did those who failed to complete the 1 l-week study, independent of dosing schedule (95% C.I. of -45.0% to -10.4%, P < 0.01).
3.2.2. Percent clinic &ys attended Endpoint analysis data (n = 99) revealed a significant main effect of com- pletion status (F(1,95) = 28.4, P c O.OOl), but no signif- icant interaction or main effect of dose schedule (Fs < 1). As can be seen in Table 2, patients assigned to the daily dosing schedule attended the clinic 7.9% more days in their last 2 weeks of treatment than did those assigned to the alternate-day dosing schedule (95% C.I. of -1.5% to 17.5% days, ns). As can be seen in Table 3, patients who completed the study attended the clinic 23.8% more days in their final 2 weeks of treatment than did those who failed to complete the study, independent of dosing schedule (95% C.I. of 15.3% to 32.3%, P < 0.001).
Failure to attend the clinic could have affected pa-
Outcome measure Daily Alternate-day Group difference (daily minus alternate-day)
Mean S.E.M. n Mean S.E.M. n Mean 95% C.I.
Days in treatment 59.9 3.9 51 Percent of urines positive for 56.7 6.1 50
opiates Percent of urines positive for 49.3 6.3 50
cocaine Percent of clinic days 77.8 3.1 51
attended
Dose adequacy VAS HOLD HOOK LIKE
Withdrawal symptom checklist
24.6 3.2 46 20.1 2.5 46 4.5 -3.6 to 12.6 28.7 3.5 46 24.8 3.4 46 3.9 -6.0 to 13.8 29.2 3.4 46 21.5 3.4 46 1.7 -7.9 to 11.3 41.1 6.1 51 48.1 6.3 48 -7.0 -24.5 to 10.5
58.1 3.6 48 1.9 -8.1 to 12.5 68.6 5.4 48 -11.9 -28.1 to 4.3
46.9 6.4 48 2.4 -20.3 to 15.5
69.9 3.6 48 7.9 -1.5 to 17.5
Data are independent of study completion status.

32 R. E. Johnson et al. /Drug and Alcohol Dependence 40 (1995) 27-35
tients assigned to the two dosing schedules differently. That is, a single missed dose for a patient assigned to the daily dosing schedule meant one day without active dos- ing, whereas a single missed dose for a patient assigned to the alternate-day dosing schedule could mean three days without active dosing (if the patient missed a scheduled active dose). The percent of scheduled active doses administered to each patient during their period of treatment retention was compared for the two dosing schedules. Patients assigned to daily dosing missed, on average, 19.9% of scheduled active doses, compared to 28.1% of scheduled active doses missed by patients assigned to the alternate-day group. The difference be- tween groups was not significant (F(1,91) = 3.4, P > 0.06).
3.2.3. Dose adequacy. Endpoint analysis (n = 92; 5 daily and 2 alternate-day patients failed to complete at least 1 dose adequacy questionnaire) revealed a signifi- cant main effect of study completion status for HOOK (F(1,88) = 5.9, P < 0.05) and for LIKE (F(1,88) = 5.0, P < 0.05). No significant interactions or main effects of dose schedule (Fs < 1) were revealed. Table 2 shows that there was a trend toward patients assigned to the daily dosing schedule to report that buprenorphine was HOLDing them better (difference between the means of 4.5 mm, with a 95% C.I. of -3.6 to 12.6 mm, ns), they felt more HOOKed (difference between the means of 3.9 mm, with a 95% C.I. of -6.0 to 13.8 mm, ns), and that they LIKEd their buprenorphine better (difference be- tween the means of 1.7 mm with a 95% C.I. of -7.9 to 11.3 mm, ns), as compared to patients assigned to the alternate-day dosing schedule. As can be seen in Table 3, patients who completed the study reported that the buprenorphine was HOLDing them better (difference
Table 3 Endpoint analysis of treatment completers versus non-completers
between the means of 7.7 mm, with a 95% C.I. of 0.0 to 15.4 mm, ns), made them feel more HOOKed (difference between the means of 12.7 mm, with a 95% C.I. of 3.5 to 21.9 mm, P < 0.05), and that they LIKEd their medi- cation more (difference between the means of 10.8 mm, with a 95% C.1. of 2.0 to 19.6 mm, P < 0.05), than did patients who failed to complete the study.
3.2.4. Opiate withdrawal symptom checklist. Endpoint analysis (n = 99) revealed no significant interaction or main effects (F’s < 1). Table 2 shows that patients assigned to the daily dosing schedule scored, on average, 7.0 points lower on the withdrawal symptom scale than did patients assigned to the alternate-day dosing sched- ule (95% C.I. of -24.5 to 10.5, ns). Similarly, Table 3 shows that patients who completed the study scored, on average, 15.6 points lower on the withdrawal symptom scale than did patients who failed to complete the study, independent of dosing schedule (95% C.I. of -32.9 to 1.7, ns).
3.3. Primary and secondary outcome measures: time course analysis
No significant main effects or interactions were observed for the treatment completer sample on percent of opiate-positive urines, percent of cocaine-positive urines, percent of available clinic days attended, opiate withdrawal symptoms or dose adequacy VAS scores (all Fs < 1). The main effect of treatment week was signifi- cant (F(10,540) = 2.61, P c 0.05) for HOOK, indicating a significant increase in feeling HOOKecl across weeks, independent of dose schedule while the main effect of week for the LIKE VAS approached conventional levels of significance (fl10,540) = 1.81, P < 0.09).
Outcome measure Completers Non-completers Group difference (completers minus non-completers)
Mean S.E.M. n Mean S.E.M. n Mean 95% C.I.
Percent of urines positive for 51.3.’ 5.5 56 11.4 5.3 42 -26.1 -41.4 to -10.6 opiates
Percent of urines positive for 36.2*' 5.5 56 63.9 6.7 42 -27.7 -45.0 to -10.4 cocaine
Percent of clinic days i34.3*** 2.1 56 60.5 3.3 43 23.8 15.3 to 32.3 attended
Dose adequacy VAS HOLD HOOK LIKE
Withdrawal symptom checklist
25.4 2.8 56 17.6 2.7 36 1.1 0.0 to 15.4 31.7* 3.4 56 19.0 3.1 36 12.1 3.5 to 21.9 32.6* 3.3 56 21.8 2.9 36 10.8 2.0 to 19.6 31.8 5.9 56 53.3 6.4 43 -15.6 -32.9 to 1.7
*P < 0.05, significant difference from non-completers; **P < 0.01, significant difference from non-completers; **P < 0.001, significant difference from non-completers. All outcome measures except retention are included. Data are independent of study completion status.

R.E. Johnson et al. /Drug and Alcohol Dependence 40 (199s) 27-35 33
4. Discussion
This study showed that both daily and alternate-day dosing with 8 mg s.1. buprenorphine produced similar treatment outcomes in opioid-dependent drug abusers on two primary (retention in treatment and urines posi- tive for opiates) and four secondary (clinic attendance, dose adequacy, withdrawal symptoms, and urines posi- tive for cocaine) outcome measures. There were no statistically significant differences between the two dos- ing schedules using survival analysis, endpoint analysis, or time course analysis. In contrast, significant differ- ences were observed for the primary measures (percent of urines positive for opiates) and for three secondary measures (clinic attendance, dose adequacy, and percent of urines positive for cocaine) when study completers were compared to non-completers, independent of group assignment. Specifically, patients who completed the present study submitted fewer opiate- and cocaine- positive urine specimens, attended the clinic more often, and reported greater dose adequacy then those patients who failed to complete the study. These effects of com- pletion status suggest that the majority of outcome mea- sures in this study were sensitive to variables that led some patients to drop out and others to remain in treat- ment. This demonstrated measurement sensitivity makes the observed lack of differences between the daily and alternate-day dosing schedules more convincing.
Despite consistent demonstrations of no statistically significant differences between daily and alternate-day dosing schedules in this and previous studies (Fudala et al., 1990; Resnick et al., 1993; Amass et al., 1994), 95% confidence intervals on endpoint data suggest that the daily dosing schedule may have marginal clinical superiority over the alternate-day schedule at the dose tested. Confidence intervals give an estimate of the size of an effect, bounded by the lower and upper limits that make up the interval. Thus an interval might suggest clinical importance if most of the values within that interval fall on the side of clinical utility. For example, opiate-positive urines suggest a marginal clinical superiority of daily dosing over alternate-day dosing because the 95% confidence interval ranges from a decrease of 28.1% positive urine specimens to an increase of 4.3% positive urine specimens. Thus the interval suggests that daily dosing with 8 mg buprenor- phine, when compared to alternate-day dosing, is more likely to lead to clinically useful outcomes, with the best outcome consistent with the current data being a 28.1% decrease in opiate-positive urine samples. Similarly, the confidence interval for the withdrawal symptom scale suggests a clinical advantage for the patients assigned to the daily dosing schedule. The interval for this measure ranges from 24.5 fewer points on the withdrawal symp- tom scale to 10.5 more points. Thus the 95% confidence intervals suggest a modest clinical benefit for the daily
dosing schedule - patients maintained on a daily dos- ing schedule will tend to use opiates less, and to report withdrawal symptoms of lesser magnitude than patients maintained on an alternate-day schedule. The conti- dence interval for mean days in treatment fails to sup- port any superiority of daily over alternate-day dosing, as patients assigned to a daily dosing schedule can be expected to remain in treatment anywhere from 8.7 days more to 12.5 days less than patients assigned to an alternate-day dosing schedule.
Overall, the results of this study are consistent with previous reports of alternate-day dosing effects. The observed lack of statistical difference between daily and alternate-day dosing schedules is in agreement with a previously reported inpatient study comparing daily ver- sus alternate-day buprenorphine (Fudala et al., 1990). In that study, no significant effects of dosing schedule were observed overall on scales measuring drug effects and opioid withdrawal symptoms. However, within-group analyses revealed systematic but non-significant differ- ences between drug and non-drug days in the altemate- day dosing condition, Specifically, patients assigned to the alternate-day dosing schedule reported a greater urge for an opiate on days when they received placebo, and ratings of agonist effects were higher on days when they received active drug. The fluctuating response pat- tern in the alternate-day group may reflect either sensi- tivity to the agonist effects of buprenorphine or the onset of an opioid withdrawal syndrome. The present study is unable to address intragroup differences across dosing days, as subjective measures were collected week- ly, not daily. Also, subjects in the present study may have administered illicit opiates, a factor Fudala et al. (1990) avoided in their inpatient study.
Fudala et al. (1990) recommended daily dosing in preference to alternate-day dosing with 8 mg s.1. buprenorphine because of the observed intragroup dif- ferences. This trend toward more stable subjective effects in the daily dosing group is consistent with the trends for somewhat better clinical outcomes seen in the present study for daily dosing. Unlike Fudala et al. (1990), Amass et al. (1994) and Resnick et al. (1993) did not recommend a specific dosage schedule, however their results are consistent with the present study in that neither of these investigators detected differences be- tween daily and alternate-day dosing. When Fudala et al. (1990) and the present study are compared with Amass et al. (1994) and Resnick et al. (1993) an impor- tant difference is apparent; in the latter two studies patients were assigned to individualized daily doses and these doses were doubled during the alternate-day dos- ing regimen. Future research will help to determine if dosing with double the stabilization dose enhances an alternate-day dosing schedule.
The present daily and alternate-day dosing schedules differ in both their timing of drug administration and in

34 R. E. Johnson et al. I Drug and Alcohol Dependence 40 (1995) 27-35
their average mg/day of buprenorphine delivered (i.e., the 8-mg alternate-day condition averages only 4 mg/day). These differences must certainly influence both the mean level and the temporal pattern of buprenor- phine blood concentrations. Thus, any trends for out- come differences might result from differences in the average mg/day dose, or blood concentration, or from differences in pharmacokinetic time course (Rowland and Tozen, 1989). In the case of methadone treatment, dose is clearly related to clinical outcome, with higher doses producing better outcomes (e.g., Strain et al., 1993). Even when dose is constant, there may be marked variations in plasma concentration across individuals maintained on either methadone (Holmstrand et al., 1978; Nilsson et al., 1983; Tennant et al., 1983) or bu- prenorphine (Ed Cone, Ph.D., personal communica- tion) and lower plasma levels of methadone have been associated with greater frequency of opiate-positive urines and poorer treatment outcome (Holmstrand et al., 1978; Nilsson et al., 1983; Tennant et al., 1983).
Plasma levels of buprenorphine may also be related to treatment outcome. If so, doubling a daily stabilization dose during alternate-day dosing, as has been done in previous studies (Resnick et al., 1993; Amass et al., 1994), may be a better strategy for maintaining effective plasma levels during a 48-h period than omitting alter- nate daily doses, as was done in the present study. Had individualized dosing been used, the present study may have included patients for whom either 4 or 8 mglday would be adequate to suppress withdrawal and block opiate use. Patients for whom a daily dose of 4 mg is adequate should do well when dosed with 8 mg bu- prenorphine every other day (as did 6 patients reported by Amass et al., 1994). However, patients for whom a daily dose of 8 mg is adequate may not do as well when dosed with 8 mg buprenorphine every other day - for these patients the plasma concentration of buprenor- phine might fall below the effective level during the 48 h following their last dose. These patients may do better when dosed with 16 mg buprenorphine every other day (i.e., twice their daily stabilization dose). Two recent studies of acute buprenorphine administration (Walsh et al., 1994; Walsh et al., 1995) suggest that the agonist ef- fects of buprenorphine reach a ceiling at the 8-16-mg dose range. Importantly, blood levels of buprenorphine remain elevated longer when higher doses are ad- ministered (for example, doubling the buprenorphine dose from 8 mg to 16 mg leads to approximately doubl- ed buprenorphine blood levels at 24 h post-drug; Walsh et al., 1994) suggesting that higher doses may increase the efficacy of alternate-day dosing for some patients.
Results of this trial may have been biased by the placebo controlled study in which all patients had par- ticipated during their first 2 weeks of treatment (Johnson et al., 1995, this issue). One hundred and fifty patients were initially enrolled, but only 99 participated in the present study, 51 patients having left treatment
during the first study and the stabilization week between the two studies. It is possible that those patients who left treatment may have been the least tolerant of low or placebo dosing, while those who remained in treatment and who participated in the present study may have been relatively more tolerant of low or placebo dosing. Patients who participated in this study, therefore, may have been in part self-selected on the basis of their abili- ty to tolerate low or placebo dosing. This self-selection may have differentially improved outcomes in the alternate-day group to the extent that the group contain- ed patients tolerant of placebo dosing on alternate days. Thus results of this study must be interpreted with this potential source of bias in mind.
Taken together, the present and previous reports sug- gest that better outcomes might be achieved with alternate-day dosing if higher doses are given. It is also possible that flexible dosing could be successfully used as in the Amass et al. (1994) study to individualize daily doses and then double these doses for alternate-day regimens. Future studies of less than daily dosing schedules may also benefit from correlating plasma level of buprenorphine with treatment outcome. Finally, re- sults from this and previous studies are consistent with a flexible approach to buprenorphine treatment delivery wherein patients could be allowed latitude in selecting the frequency and size of their doses. Thus, some patients might elect to attend clinic on alternate days while others would choose to attend daily.
Despite the potential self-selection bias in this study, these results demonstrate that daily and alternate-day dosing of buprenorphine 8 mg s.l. can produce compar- able treatment outcomes and support the conclusion that alternate-day dosing should be feasible to imple- ment clinically and should be effective in and acceptable to a substantial portion of patients. However, when trends and confidence intervals were taken into account, the results favored daily versus alternate-day dosing with buprenorphine at the dose tested. It is possible that even better outcomes with alternate-day dosing might be achieved if doses higher than 8 mg were routinely util- ized or if doses were individualized based on effective daily dose, patient illicit drug use, and withdrawal symptoms.
Acknowledgments
This research was supported by USPHS grants R18 DA 06165, T32 DA 07209, and KO5 DA 00050. We thank Ms. Iona Johnson, Ms. Connie Lowery, Mr. Tim Mudric, Ms. Ginger Rafferty, the Counseling, and Intake staffs for their excellent technical support.
References
Amass, L., Bickel, W.K., Higgins ST. and Badger G.J. ( 1994) Alternate-day dosing during buprenorphine treatment of opioid dependence. Life Sci. 54, 1215-1228.

R.E. Johnson et al. /Drug and Alcohol Dependence 40 (1995) 27-35 35
Bickel, W.K., Stitzer, M.L., Bigelow, G.E., Liebson, I.A., Jasinski, D.R. and Johnson, R.E. (1988) Buprenorphine: dose-related blockade of opioid challenge effects in opioid dependent humans. J. Pharmacol. Exp. Ther. 247, 47-53.
Borenstein, M. (1994) The case for confidence intervals in controlled clinical trials. Controlled Clin. Trials 15, 41 l-428.
Cheskin, L.J., Fudala, P.J. and Johnson, R.E. (1994) A controlled comparison of buprenorphine and clonidine for acute detoxilica- tion of opioids. Drug Alcohol Depend. 36, 115-121.
Freedman, R.R. and Czertko, G. (1981) A comparison of thrice week- ly LAAM and daily methadone in employed heroin addicts. Drug Alcohol Depend. 8, 215-222.
Fudala, P.J., Jaffe, J.H., Dax, E.M. and Johnson, R.E. (1990) Use of buprenorphine in the treatment of opioid addiction. II. Physiologic and behavioral effects of daily and alternate-day administration and abrupt withdrawal. Clin. Pharmacol. Ther. 47, 525-534.
Holmstrand, J., Anggard, E. and Gunne, L.-M. (1978) Methadone maintenance: plasma levels and therapeutic outcome. Clin. Phar- macol. Ther. 23, 175-180.
Jasinski, D.R., Pevnick, J.S. and Griffith, J.D. (1978) Human pharma- cology and abuse potential of the analgesic buprenorphine. Arch. Gen. Psychiatry 35, 501-516.
Johnson, R.E., Cone, E.J., Henningfield, J.E. and Fudala, P.J. (1989) Use of buprenorphine in the treatment of opiate addiction. I. Physiologic and behavioral effects during a rapid dose induction. Clin. Pharmacol. Ther. 46, 335-343.
Johnson, R.E., Eissenberg, T., Stitzer, M.L., Strain, E.C., Liebson, LA. and Bigelow, G.E. (1995) A placebo controlled clinical trial of buprenorphine as a treatment for opioid dependence. Drug and Alcohol Depend. 40, 17-25.
Johnson, R.E., Fudala, P.J. and Jaffe, J.H. (1992) A controlled trial of buprenorphine for opioid dependence. J. Am. Med. Assoc. 267, 2750-2755.
Judson, B.A. and Goldstein, A. (1979) Levo-alpha-acetylmethadol (LAAM) in the treatment of heroin addicts. I. Dosage schedule for induction and stabilization. Drug Alcohol Depend. 4, 461-466.
Kosten, T.R., Schottenfeld, R., Ziedonis, D. and Falcioni, J. (1993) Buprenorphine versus methadone maintenance for opioid depen- dence. J. Nerv. Ment. Dis. 181, 358-364.
Lee, E. and Desu, M. (1972) A computer program for comparing k samples with right-censored data. Comput. Programs Biomed. 2, 315-321.
Lewis, J.W. (1985) Buprenorphine. Drug Alcohol Depend. 14, 363-372.
Ling, W., Charuvastra, C., Kaim, SC. and Klett, C.J. (1976)
Methadyl acetate and methadone as maintenance treatments for heroin addicts. Arch. Gen. Psychiatry 33, 709-720.
Mello, N.K. and Mendelson, J.H. (1980) Buprenorphine suppresses heroin use by heroin addicts. Science 207, 657-659.
Mello, N.K., Mendelson, J.H. and Kuehnle, J.C. (1982) Buprenor- phine effects on human heroin self-administration: an operant analysis. J. Pharmacol. Exp. Ther. 223, 30-39.
Nilsson, M.-I., Gronbladh, L., Widerlov, E. and Anggard, E. (1983) Pharmacokinetics of methadone in methadone maintenance treat- ment: characterization of therapeutic failures. Eur. J. Clin. Phar- macol. 25, 497-501.
Pickworth, W.B., Johnson, R.E., Holicky, B.A. and Cone, E.J. (1993) Subjective and physiologic effects of intravenous buprenorphine in humans. Clin. Pharmacol. Ther. 53, 570-576.
Resnick, R.B., Pycha, C. and Galanter, M. (1993) Buprenorphine maintenance: reduced dosing frequency. NIDA Res. Monogr. I41 (2). 454.
Rosen, M.I., Wallace, E.A., McMahon, T.J., Pearsall, H.R., Woods, S.W., Price, L.H. and Kosten, T.R. (1994) Buprenorphine: dura- tion of blockade of effects of intramuscular hydromorphone. Drug Alcohol Depend. 35, 141-149.
Rowland, M. and Tozer, T.N. (1989) Clinical Pharmacokinetics: Con- cepts and Applications, 2nd. Edition, Lea and Febiger, Philadelphia.
Snedcor, G.W. and Cochran, W.G. (1989) Statistical Methods, Iowa State University Press, Ames.
Spitzer, R.L. and Williams, J.B.W. (1987) Structured Interview for DSM-III-R (SCID), New York State Psychiatric Institute, Biometrics Research, New York.
Stitzer, M.L., Iguchi, M.Y. and Felch, L.J. (1992) Contingent take- home incentive: effects on drug use of methadone maintenance pa- tients. J. Consult. Clin. Psychol. 60, 927-934.
Strain, E.C., Stitzer, M.L., Liebson, I.A. and Bigelow, G.E. (1993) Methadone dose and treatment outcome. Drug Alcohol Depend. 33, 105-117.
Tennant, F.S., Rawson, R.A., Cohen, A., Tarver, A. and Clabough, D. (1983) Methadone plasma levels and persistent drug abuse in high dose maintenance patients. Substance Alcohol Actions/Mis- use 4, 369-374.
Walsh, S.L., Preston, K.L., Bigelow, G.E. and Stitzer, M.L. (1995) Acute administration of buprenorphine in humans: partial agonist and blockade effects. J. Pharmacol. Exp. Ther. 274, 361-372.
Walsh, S.L., Preston, K.L., Stitzer, M.L., Cone, E.J. and Bigelow, G.E. (1994) Clinical pharmacology of buprenorphine: ceiling ef- fects at high doses. Clin. Pharmacol. Ther. 55, 569-580.