Embed Size (px)
Citation preview

Bundling…..Will we survive?Bundling…..Will we survive?
Thomas E. Amitrano BSN, MPA, RN

Bundling…..Will we survive?Bundling…..Will we survive?

Bundling Bundling HowHow Will We Will We Survive ?Survive ?

A bit of HistoryA bit of History In 1972 Congress enacted legislation to In 1972 Congress enacted legislation to
create a way to finance End Stage Renal create a way to finance End Stage Renal Disease (ESRD)Disease (ESRD)
In 2008 Congress passed the Medical In 2008 Congress passed the Medical Modernization Act (MMA) as well as the Modernization Act (MMA) as well as the Medicare Improvements for Patients and Medicare Improvements for Patients and Providers Act (MIPPA) these acts required the Providers Act (MIPPA) these acts required the Centers for Medicare and Medicaid Services Centers for Medicare and Medicaid Services (CMS) to look at the elimination of payments (CMS) to look at the elimination of payments that were separately paid for dialysis services that were separately paid for dialysis services and drugs.and drugs.
Bundling is the solution CMS has proposedBundling is the solution CMS has proposed

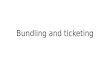
Estimated point prevalent ESRD patients Estimated point prevalent ESRD patients
Figure 11.3 (Volume 2)Figure 11.3 (Volume 2)
December 31 point prevalent ESRD patients; non-Medicare status determined from payor sequence.
USRDS 2009 ADR

Total Medicare dollars spent Total Medicare dollars spent
on ESRD, by type of service on ESRD, by type of service Figure 11.5 (Volume 2) Figure 11.5 (Volume 2)
ESRD spending obtained from Medicare ESRD claims, & includes all Medicare as primary payor claims as well as amounts paid by Medicare as secondary payor.
USDRS 2009 ADR

Total Medicare ESRD Total Medicare ESRD expenditures, by modality expenditures, by modality
Figure 11.6 (Volume 2) Figure 11.6 (Volume 2)
Period prevalent ESRD patients. Modalities determined using Model 1 methodology. Includes Medicare paid claims for ESRD patients, starting at first ESRD service date & continuing until death or the end of the study period. Patients with Medicare as secondary payor are included.
USRDS 2009 ADR

Total Medicare spending Total Medicare spending on injectables on injectables Figure 11.13 (Volume 2) Figure 11.13 (Volume 2)
Period prevalent dialysis patients.. ESAs: erythropoiesis stimulating agents.
USRDS 2009 ADR

Why change?Why change?
In a separately billable system In a separately billable system certain services are billed for as certain services are billed for as “composite” and others are billed for “composite” and others are billed for as “separately billable”. This system as “separately billable”. This system left some question as to the profit left some question as to the profit margin some dialysis units reported. margin some dialysis units reported. If all services were equal why did If all services were equal why did some units make more money than some units make more money than others?others?

Proposed* ChangesProposed* Changes
Payment will be on a per treatment basisPayment will be on a per treatment basis All drugs and labs will be includedAll drugs and labs will be included
– All renal service oral drugs including All renal service oral drugs including Phosphorus bindersPhosphorus binders
– All labs ordered by Nephrologists or othersAll labs ordered by Nephrologists or others Reimbursement would “trim 2% of the Reimbursement would “trim 2% of the
estimated payments that would have been estimated payments that would have been made in 2011 under the previous payment made in 2011 under the previous payment system”system”
No adjustment for Race/EthnicityNo adjustment for Race/Ethnicity Wage Index Adjustments are likelyWage Index Adjustments are likely

Proposed* Changes Proposed* Changes (con’t)(con’t)
Units will have the option of easing in over Units will have the option of easing in over 4 years or going 100% at one time4 years or going 100% at one time
The Math……The Math……– 2007 claims data proposed the 2011 rate 2007 claims data proposed the 2011 rate
would be $261.58would be $261.58– CMS is proposing a 21.73% reduction = CMS is proposing a 21.73% reduction =
$204.74$204.74– Proposed Outlier Adjustment 1% reduction = Proposed Outlier Adjustment 1% reduction =
$202.69$202.69– MIPPA required a 98% reduction = $198.64MIPPA required a 98% reduction = $198.64

ProblemsProblems
Old data may have been used – cost Old data may have been used – cost reports etc. in some cases are datedreports etc. in some cases are dated
No consideration of inflationNo consideration of inflation Certain areas of the country will get Certain areas of the country will get
less reimbursement for the same less reimbursement for the same servicesservices
Potential for decreased care based Potential for decreased care based on decreased reimbursement existson decreased reimbursement exists

New Quality Indicators on or New Quality Indicators on or after July 1,2010after July 1,2010
Kt/V must be reported for both HD Kt/V must be reported for both HD and PDand PD
Access type must be reported for HD Access type must be reported for HD – Modifier V5: Vascular CatheterModifier V5: Vascular Catheter– Modifier V6: Arteriovenous GraftModifier V6: Arteriovenous Graft– Modifier V7: Arteriovenous FistulaModifier V7: Arteriovenous Fistula– Modifier V8: Infection presentModifier V8: Infection present– Modifier V9: No Infection presentModifier V9: No Infection present

Worries/ ConcernsWorries/ Concerns
Will Practice be a result of PaymentWill Practice be a result of Payment Will Quality and Performance Will Quality and Performance
Improvement ChangeImprovement Change Will Hospitalizations be decreased or Will Hospitalizations be decreased or
shortened for the wrong reasonsshortened for the wrong reasons Will units close and leave gaps in Will units close and leave gaps in
serviceservice Will we have to do more with lessWill we have to do more with less

Our Role in BundlingOur Role in Bundling
Maintain high standards of careMaintain high standards of care Encourage each patient to maintain Encourage each patient to maintain
their optimal level of healththeir optimal level of health Educate patients to be proactive and Educate patients to be proactive and
preventative not reactive regarding preventative not reactive regarding their healththeir health
Work diligently to prevent patient Work diligently to prevent patient illnessillness

Our Role in Bundling Our Role in Bundling (con’t)(con’t)
Accurately document all information Accurately document all information on all forms….. co morbid conditions on all forms….. co morbid conditions are important are important
Look for ways to improve efficiencyLook for ways to improve efficiency Make patient safety and well being a Make patient safety and well being a
major priority and goalmajor priority and goal– Decrease hospitalizationsDecrease hospitalizations– Decrease infectionsDecrease infections– Manage medications Manage medications

Our Role in Bundling Our Role in Bundling (con’t)(con’t)
Remain in close communication with Remain in close communication with the Hospital Dialysis Units maintain the Hospital Dialysis Units maintain continuity thru the continuum of continuity thru the continuum of health/illnesshealth/illness
Develop Policies and Practices that Develop Policies and Practices that are evidence based to ensure high are evidence based to ensure high standardsstandards
““No missed Treatment” philosophy No missed Treatment” philosophy offer alternate times/daysoffer alternate times/days

Planning for ChangePlanning for Change Assess current practices and Assess current practices and
critically analyze the ability of the critically analyze the ability of the practice to survivepractice to survive
Develop strategies that promote Develop strategies that promote patient well being across the patient well being across the continuum of healthcontinuum of health
Incorporate Evidence Based Practice Incorporate Evidence Based Practice into Policies and Practicesinto Policies and Practices

Planning for Change Planning for Change (con’t)(con’t)
Analyze QAPI data for trends and Analyze QAPI data for trends and patternspatterns– Deming cycleDeming cycle

Planning for Change Planning for Change (con’t)(con’t)
Read, Read, ReadRead, Read, Read Actively engage your colleagues in a Actively engage your colleagues in a
Spirit of ChangeSpirit of Change– Buy in on all levels will be criticalBuy in on all levels will be critical– Team work is essential to successTeam work is essential to success– Embrace the opportunity to help your Embrace the opportunity to help your
unit succeedunit succeed

SummarySummary
Bundling is going to happen in some Bundling is going to happen in some formform
We will need to be ready in some wayWe will need to be ready in some way We will all be effected some howWe will all be effected some how We can all do something to prepare for We can all do something to prepare for
the changethe change– Review practiceReview practice– Educate patientsEducate patients– Set high StandardsSet high Standards

ResourcesResources
http://www.annanurse.orghttp://www.annanurse.org http://www.cmms.hhs.govhttp://www.cmms.hhs.gov http://www.usrds.orghttp://www.usrds.org [email protected]@sjhmc.org