Embed Size (px)
Citation preview

ARTICLE IN PRESS
Respiratory Medicine (2005) 99, 171–178
KEYWORDBullous emChronic obpulmonaryHigh-resolucomputedtomographDiffuse em
0954-6111/$ - sdoi:10.1016/j.r
�CorrespondiToronto GenerStreet, Toront4163404400; fa
E-mail addr
Bullous emphysema versus diffuse emphysema:a functional and radiologic comparison
Marco Muraa,�, Maurizio Zompatorib, Andrea Mussonia,Luca Fasanoa, Angela Maria Grazia Pacillia, Orazio Ferroc,Mario Schiavinaa, Mario Fabbria
aU.O. Fisiopatologia Respiratoria, Policlinico Sant’Orsola-Malpighi, Bologna, ItalybU.O. Radiologia, Policlinico Rasori, Parma, ItalycU.O. Statistica, Ospedale Civile, Imola, Italy
Received 10 February 2004; accepted 30 June 2004
Sphysema;structivedisease;tion
y;physema
ee front matter r 200med.2004.06.010
ng author. Thoracic Sural Hospital, Room: MBo, Ontario, Canadax: 001-4163404638.ess: [email protected]
Summary The contribution of bullous emphysema (BE) to the functionalimpairment of patients with concomitant diffuse emphysema (DE) and theconfounding effects of BE on functional measurements were investigated. Twenty-nine patients (Group I), with BE and DE were compared with a group of patientswithout BE matched, among other criteria, for radiographic extent of DE (Group II).Group I showed significantly lower PaO2; FEV1 and DLCO values and higher MRC scorethan Group II. In Group I the radiographic extent of BE and the extent of DE did notpredict the functional impairment. The FEV1/FVC ratio in the subgroup with BEextent425% of total lung volume was higher than in subgroups with BE extent420%and 15%, respectively. In the same subgroups the correlation between DE and DLCOincreased with the extent of BE. We conclude that BE contributes to the functionalimpairment of patients with concomitant DE. The confounding functional effect ofbullae depends on BE extent: relatively milder obstruction can be observed withsevere BE, whereas moderate BE causes modest deterioration of diffusing capacity,explaining the lack of functional-radiologic correlations in Group I. Therefore thecomputed tomographic scan is very useful in the work-up of BE with DE associated.r 2004 Elsevier Ltd. All rights reserved.
4 Elsevier Ltd. All rights reserv
gery Research Laboratory,RC 5R425, 200 ElizabethM5G 2C4. Tel.: 001-
ronto.ca (M. Mura).
Introduction
Lung bullae occur in a variety of disorders, mostoften in association with chronic obstructive
ed.

ARTICLE IN PRESS
Table 1 Patients characteristics.
Group I Group IIðBEþ DEÞ (DE alone)
Males/Females 25/4 25/4Age 69:5� 7:2 69:9� 7:8
(range51–82)
(range46–85)
Race Caucasian CaucasianBody mass index (kg/m2) 24:1� 3:4 24:6� 5:3Diffuse Non-BullousEmphysema extent
28:6� 14:6 28:2� 15:9
(% of total lung volume) (range5–52)
(range8–59)
Smoking history (pack-years)
44:4� 15:9 50:6� 28:9
Bullous emphysemaextent
15:4� 8:3 0
(% of total lung volume) (range5–37)
M. Mura et al.172
pulmonary disease (COPD), especially emphysema.1
However, bullae may occur in lungs that areotherwise normal.2,3 Consequently, patients withbullous lung disease can be subdivided in those withCOPD associated (bullous emphysema-BE) andthose without airways obstruction (primitive bul-lous disease–PBD).4
Pulmonary function tests (PFTs) have remark-ably practical value in distinguishing betweenlocalized bullae with otherwise normal lungand bullae in conjunction with underlyingCOPD.2 Computed tomography (CT) can locatethe bullae with considerable accuracy, evenwhen their presence was not suspected on thebasis of clinical and radiographic data. There-fore CT scan is the most useful single methodof assessing the extent and localization of bullaeand the possible association with diffuse non-bullous emphysema (DE).1,5 Furthermore, the roleof CT scan is relevant in the follow-up of BE,due to the frequently observed association withlung cancer.6
The surgical intervention of bullectomy isfunded on the reexpansion of the normal lungthat can therefore recover its elastic balance.The preoperative size of bullae is the mostimportant contributor to the improvement inventilatory capacity after bullectomy.7 How-ever, in patients with BE the intervention ofbullectomy is not so successful as in patients withPBD, even if some of the treated subjects show apostoperative improvement of the clinical condi-tions and gas exchange, especially in the case ofgiant bullae.8,9
The functional changes expected with emphyse-ma (hyperinflation, airflow limitation, impairmentof diffusing capacity for CO [DLCO]) may beconfounded by the functional changes caused byBE.10 In PBD, PFTs usually show either no functionalimpairment or a restrictive defect.2 Forcedexpired vital capacity (FVC) may be reduced,because the bulla behaves as a space occupyingmass, while the airways passage is narrow. Conse-quently, the inspired gas arrives in the bulla veryslowly.5 Lung bullae may also contribute to thedeterioration of diffusing capacity and DLCO isusually determined to distinguish between DE andlocalized bullae.4
The aim of this study was to investigatethe contribution of BE to the functional impair-ment of patients with concomitant DE bycomparing the functional and radiologic featuresof these two types of emphysema. We alsoaimed at dissecting the confounding effectsof lung bullae on the functional assess-ment.
Patients and methods
Patients
We compared the pulmonary function data and thedyspnea score of two different groups of nonasth-matic patients: Group I was affected by both BE andDE, while Group II was affected by DE only. The twopopulations were matched for gender, age, race,smoking history, body mass index (BMI) and extentof DE.
Twenty-nine patients (M/F 25/4), aged 51–82years, affected by DE and BE were included in thestudy as Group I; all of them were former smokers(Table 1). Subjects of Group I were selected amongpatients with a diagnosis of COPD11 and withradiologic evidence of BE and DE at High-resolutioncomputed tomography (HRCT) scan. Bullae weredefined as confluent areas of low density, arrangedon single layer, with diameter of at least 1 cm,visible over two or more adjacent CT cuts, with aconvex outline, thin walls and absence of lungtissue within the bulla.5,12 Bullae were distin-guished from apical blebs, defined as intrapleuralcollections of air, bronchogenic cysts, cysts ofhoneycomb lung, cystic bronchiectasis and cystsof different origin, as pneumatoceles arising duringan episode of Pneumocystis Carinii pneumonia.5,12
The population of Group II was selected amongsubjects with a diagnosis of COPD and radiologicevidence of DE at HRCT scan, while no evidence oflung bullae was found. Patients characteristics areshown in Table 1.

ARTICLE IN PRESS
Bullous versus diffuse emphysema 173
Patients with diseases other than emphysema, asinterstitial lung diseases, collagen vascular dis-eases, sarcoidosis, asthma and obstructive sleepapneae syndrome were excluded from the study.Informed consent was obtained by all patients. Asall investigations in this study are part of thenormal procedure for the diagnosis and follow-up ofemphysema of our department, the institutionalethics committee approval was not required.
Study design
The radiographic extent of BE in Group I wasquantified with a visual score (VS) from HRCT, whilethe extent of total emphysema both in Group I andII was evaluated with an automatic score (AS),obtained by helical CT and density mask program,provided with the GE light speed scanner (GeneralElectric, Milwaukee, WI, USA). The radiographicextent of DE in Group I was then calculated bysubtracting the extent of BE (VS) from the total AS.HRCT was performed in all patients together withthe helical CT scan. Scores were obtained asexplained in the CT scanning section.
The mean pressure inside the lung bullae isnegative and shows a constant parallelism with thepleural pressure. The atelectasis of the surroundingareas, observed at times, is due to the elasticretraction of normal parenchyma and not to thecompression by the bulla.3 Consequently, theradiographic extent of DE and the radiodensity oflung parenchyma affected by DE are unlikely to beaffected by the presence of bullae.
Pulmonary function data and dyspnea scores inGroup I and II were then compared. PFTs were nextcorrelated with the VS (in Group I) and the AS (inGroup I and II).
CT scanning
HRCTwas performed with the patient in the supineposition during full inspiration, without intravenousinjection of contrast material and using a filter forthe osseous tissue. One mm thick sections weretaken, with a 1 s scan time and an interval of 10mmin the apex-basis scans, including both lungs in thefield of view. Bullae observed in inspiration andexpiration do not change size to any appreciabledegree.3 The extent of emphysema was obtained inall patients from multi-slice helical CT and 3Dreconstruction of the lungs, including the voxelsbetween �910 Hounsfield Units (HU—attenuationvalue referred to the water attenuation) and�1024HU; then the AS was obtained (Volume withemphysema/Total Lung Volume). A GE light speed
scanner was used. Manual exclusion of trachea andmain bronchi was not performed, as their volumesare negligible in relation to the entire model.13
Respiratory gating was not applied, as helical CTresults are reproducible, even in its absence.14
To quantify the BE in Group I we used a visualscore, performed according to the method pre-viously described.15 Bullae were identified asdescribed in the ‘‘Patients’’ section.
Two experienced radiologists, who were notaware of the specific aim of the study, indepen-dently examined and scored the HRCT scans;discrepancies were later solved by agreement.
Pulmonary function tests
Patients included in the study were examined inclinically stable conditions, without any sign of leftventricle dysfunction. Patients were required toabstain from receiving short-acting bronchodilatorsfor at least 24 h, not to have experienced respira-tory exacerbations in the previous month and not tobe enrolled in a rehabilitation program in theprevious two months. Patients were studied seatedupright in a comfortable chair, with a nose clip onand care was taken to keep the neck at a fixedneutral position.18 All manoeuvres were initiatedfrom resting end-expiratory lung volume (func-tional residual capacity). The following parameterswere studied in each patient:
�
Arterial O2 ðPaO2Þ and CO2 pressure ðPaCO2Þ andDðA� aÞPO2 were obtained in the seated posi-tion, at rest for at least 30min. Partial pressureswere measured with a Radiometer Abl 520gasanalyser.�
PFTs were performed according to ATS guide-lines.16 FVC and forced expired volume in 1 s(FEV1) were determined with a Morgan Transflow544 pneumotachograph, after a fast inspirationand by minimizing the end-inspiratory pause.17Each subject maintained similar duration ofmaximal expiratory effort.18
�
Lung volumes were determined with a MorganTransflow 544 body pletysmograph and expressedas percentage of the predicted value.�
DLCO was measured with the single-breathmethod, by correcting the obtained values forthe present hemoglobin values and by expressingthem as percentage of the predicted value.The predicted spirometric values, static lungvolume and DLCO values were from the EuropeanCoal and Steel Community.19

ARTICLE IN PRESS
M. Mura et al.174
Dyspnea evaluation
The severity of chronic dyspnea, defined as ‘‘un-pleasant sensation of labored or difficult breath-ing’’, was rated using the modified MedicalResearch Council (MRC) scale.20–22 Verbal descrip-tors of MRC scale start from 0 (not troubled bydyspnea) to a maximum value of 5 (dyspnea forminimal effort).
Statistical analysis
Results are expressed as mean�SD. The differencesbetween Groups I and II findings were investigatedby using the two-tailed Student’s t-test for inde-pendent variables. Correlations between PFTs andradiologic scores were examined using the two-tailed Pearson correlation. Correlations betweenMRC score, radiologic scores and PFTs wereinvestigated with the Spearman rank correlation,as the MRC score is an ordinal categorical variable.P-values o0:05 were regarded as significant. TheSSPS software package was used (SPSS Inc.,Chicago, IL, USA).
Results
Pulmonary function data of Groups I and II areshown in Table 2. Group I, affected by BE with
Table 2 Comparison of pulmonary function findings bindependent variables).
Group IBE+DE
MRC score 3.771.1PaO2 (mmHg) 64.279.0DðA� aÞPO2 (mmHg) 49.5748.8PaCO2 (mmHg) 46.677.5FVC (% pred) 74.6720.5FEV1 (% pred) 35.7715.6FEV1/FVC 47.2712.6DLCO (% pred) 40.7714.8IC (% pred) 70.2720.0RVHE (% pred) 92.4748.0RVPL (% pred) 218.7753.8DRV (1) 3.371.2TLCHE (% pred) 84.2715.9TLCPL (% pred) 130.6723.4D TLC (1) 2.971.3
MRC score: MRC scale of dyspnea; PaO2: arterial O2 pressure; Dcapacity; FEV1: forced expiratory volume in 1 s; DLCO: diffusincapacity; RVHE: residual volume calculated with helium dilution;difference between RVPL and RVHE; TLCHE total lung capacitycalculated with pletysmograph; DTLC: difference between TLCPL
concomitant DE, and Group II, affected by DE only,were compared: PaO2; FEV1 and DLCO weresignificantly lower in Group I. The most significantdifference between the two groups concernedDLCO. No significant difference was observedconsidering DðA� aÞPO2; FVC, FEV1/FVC and IC.The MRC score was significantly higher in Group I.
Group I showed also total lung capacity calcu-lated by helium dilution ðTLCHEÞ values significantlylower than Group II, while the residual volumemeasured with pletysmograph ðRVPLÞ was signifi-cantly higher. No significant difference was ob-served between the two groups regarding RVHE andTLCPL: The differences between RVPL and RVHE; andbetween TLCPL and TLCHE were significantly higherin Group I (Table 2).
In Group I the radiographic extent of BE was apoor predictor of the functional impairment. Nosignificant correlation was found between MRCscore, PFTs and the extent of BE. Likewise, in thesame group the radiographic extent of DE did notcorrelate significantly with PFTs and MRC score. It isnoteworthy that the radiographic extent of overallemphysema, including both BE and DE, did notcorrelate with any PFT (Table 3).
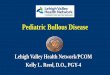
In contrast, in Group II DLCO was a good predictorof the disease extent (Fig. 1A). Table 3 shows thecorrelations between PFTs, MRC score and DEradiographic extent in Group II. DðA� aÞPO2
showed the best correlation with the MRC score(Fig. 1B). The correlations between MRC score and
etween Group I and Group II (Student’s t-test for
Group II Statistical significance(DE alone) (P-value)
2.771.1 0.00171.9710.2 0.00341.0727.7 n.s.43.875.8 n.s.81.7723.6 n.s.5.6724.0 0.007
58.9714.8 0.00262.7725.0) 0.000180.3726.1 n.s.99.8738.3 n.s.
171.4760.5 0.0091.971.5 0.001
100.9722.1 0.002122.7718.6 n.s.
1.771.4 0.001
ðA� aÞPO2: alveolar-arterial O2 gradient; FVC: forced vitalg capacity of the lung for carbon monoxide; IC: inspiratoryRVPL: residual volume calculated with pletysmograph; DRV:
calculated with helium dilution; TLCPL: total lung capacityand TLCHE.

ARTICLE IN PRESS
Table 3 Pearson correlations between the radio-graphic extent of DE, MRC score and PFTs in GroupII; r-values are indicated.
Group II ðn ¼ 29Þ DE extent MRC scoreðþÞ
(% of TLC)
MRC scoreðþÞ 0.12 ‘‘
PaO2 (mmHg) �0.08 �0.56
ðP ¼ 0:001ÞDðA� aÞPO2 (mmHg) 0.10 0:67
ðP ¼ 0:0001ÞFVC (% pred) �0.04 �0.20FEV1 (% pred) �0.24 �0.47
ðP ¼ 0:001ÞFEV1/FVC �0.39 �0.50
ðP ¼ 0:039Þ ðP ¼ 0:007ÞDLCO (% pred) �0.64 �0.45
ðPo0:001Þ ðP ¼ 0:03ÞIC (% pred) 0.17 �0.37
MRC score: MRC scale of dyspnea; PaO2: arterial O2
pressure; DðA� aÞPO2: alveolar-arterial O2 gradient; FVC:forced vital capacity; FEV1: forced expiratory volume in1 s; DLCO: diffusing capacity of the lung for carbonmonoxide; IC: inspiratory capacity. Significant correla-tions are indicated with a : Correlations between MRCscale and the others parameters were calculated bySpearman rank correlation ðþÞ:
Figure 1 (A) Relationships between: radiographic extentof DE and DLCO in Group II ðn ¼ 29Þ (Pearson correlation);(B) DðA� aÞPO2 and MRC score in the same Group(Spearman Rank correlation).
Bullous versus diffuse emphysema 175
PaO2; FEV1 and DLCO, respectively, were significantas well (Table 3).
In order to investigate the confounding effects ofBE on the functional evaluation of COPD, wedivided Group I in subgroups by using threedifferent cut-offs: 15%, 20% and 25% of BE radio-graphic extent. Over 15%, the correlation betweenDE and DLCO increased with the extent of BE. Theabsence of significance in the latter subgroup wasprobably due to the small number of cases (Table4A). In contrast, in the subgroups with less than15%, 20% and 25% of BE radiographic extent,respectively, no correlation between DLCO andthe radiographic extent of DE was observed.
In order to study the possible restrictive func-tional impairment due to BE, the FEV1/FVC ratio inthe same subgroups mentioned above was consid-ered. The FEV1/FVC ratio in the group with BEradiographic extent 425% showed a higher valuethan subgroups with BE radiographic extent 415%and 420%; respectively (Table 4B). Furthermore,when the difference in the FEV1/FVC ratio betweeneach couple of subgroups (½o15%� � ½415%�;½o20%� � ½420%�; ½o25%� � ½425%�) was consid-ered, we observed that it became smaller as theextent of BE increased (Table 4B). Therefore, theobstructive impairment, mainly due to underlyingDE and COPD, became relatively less evident withthe increase of BE radiographic extent.
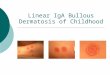
In the density histogram of CT we observed abimodal distribution of lung density in the rangebetween �910 and �1024HU; corresponding to thedensity of emphysema (Fig. 2). In our study this signwas present only in two patients: both of thempresented a BE radiographic extent 430% of thetotal lung volume and a giant bulla occupying halfof a lung. The more negative density peak, on theleft, probably corresponds to the large bulla(Fig. 2).
Discussion
In order to select those COPD patients who aremore likely to benefit from lung volume reductionsurgery (LVRS), the preoperative assessment isessential. The presence of DE reduces the func-tional improvement after bullectomy when com-pared to a resection of large bullae in the absenceof DE.23 The present study was designed toinvestigate the functional impact of BE in patientswith concomitant COPD and DE and the confound-ing effect of bullae on the pulmonary functionmeasurements.

ARTICLE IN PRESS
Table 4 (B) FEV1/FVC ratio in the same sixsubgroups and differences ðDÞ between each coupleof subgroups.
SubgroupsFEV1/FVC ratio
o15% 48:9� 14:7! Dðo15%Þð415%Þ ¼ 4:3
415% 44:9� 9:4
o20% 48:1� 14:0! Dðo20%Þð420%Þ ¼ 4:1
420% 44:0� 6:6
o25% 47:3� 13:6! Dðo25%Þð425%Þ ¼ 1:3
425% 46:0� 6:7
n ¼ number of cases; r ¼ Pearson correlation; P ¼
two-tailed significance:
Figure 2 Inspiratory CT with 3D reconstruction. Emphy-sema amounts to 51.4% of the whole total lung volume. Abimodal distribution of lung density is observed. Themore negative density peak, on the left, corresponds to alarge bulla.
Table 4 Double confounding functional effect ofBE with concomitant DE. (A) Correlations betweenDLCO and DE in three different subgroups selectedby using three cut-offs in Group I: 15, 20 and 25% ofBE radiographic extent (% of total lung volume). Nosignificant correlations were found in the subgroupso15%, 20% and 25% of BE extent, respectively.
Subgroups n r P
415% 13 �0.67 �0.017420% 7 �0.82 0.045425% 5 �0.93 0.060
M. Mura et al.176
Our findings suggest that the extent of BE is tosome extent responsible of the functional impair-ment, being the hypoxemia, the airflow obstructionand the diffusing capacity significantly worse inCOPD patients affected by BE than in matchedpatients without bullae, after excluding othercauses of functional deterioration. Patients withBE showed also a significantly higher dyspnea score.
Bullae develop after retraction and collapse ofsurrounding lung away from a region of weakness.3
Our findings can be explained by the contribution oflung bullae to the airways obstruction, due to theircomplete loss of elastic recoil.24 The static elasticrecoil pressure of the emphysematous lung istherefore further decreased. Even if the bullaeremain in free communication with the airway,they do not significantly participate in the ventila-tion.3 Furthermore, the chest wall mechanics isaltered because of the loss of linkage with the non-bullous lung tissue, leading to increased chest wall
work and worsening of hyperinflation and sensationof dyspnea.
A recent report demonstrated that in patientswith both end-stage DE and BE, bullectomy iscomparable to LVRS.25 By repositioning the dia-phragm and the chest wall, the intervention ofbullectomy reduces the lung volumes and can beconsidered a special case of LVRS.25,26 These resultsfurther underline the important contribution of BEto the functional impairment in patients withconcomitant DE.
The absence of significant correlations betweenthe radiologic scores and the pulmonary functiondata in Group I suggested that the presence of BEhas confounding effects on the functional assess-ment. Furthermore, no good predictors of exer-tional dyspnea were found among PFTs andradiologic scores. Our findings, shown in Table 4,imply that the confounding functional effects oflung bullae in COPD patients follow two differentdirections: more extended BE (425% of total lungvolume) shows a less evident obstructive ventila-tory incapacity, while in less extended BE (o25% oftotal lung volume) no significant correlation be-tween diffusing capacity and extent of DE isobserved. Larger bullae occupy more space andare therefore responsible of a more evidentrestrictive impairment. Larger bullae are alsotenser, due to the minor compliance of surroundinglung, that makes the pressure required to inflate it

ARTICLE IN PRESS
Bullous versus diffuse emphysema 177
exceed the pressure necessary to inflate thebulla.24 Moreover, their larger volume furtherdecreases their participation in ventilation; thuslarger bullae may not participate to any importantextent in gas exchange. On the other hand, smallerbullae, even if barely participate in ventilation,may still participate to some extent in gasexchange because of the presence of residualvascular internal surface. Consequently, in BE withDE associated we can expect either a milderobstructive incapacity, despite the presence ofwider bullae, or absence of correlation between DEand DLCO, despite the considerable extent of DE.
Gould and coworkers showed that in patientswith BE the major determinant of the respiratoryfunction impairment is the severity of the emphy-sema in non-bullous lung.10 In accordance with thisstudy, we observed poor correlations between theextent of BE and the functional measurements. Onthe other hand, our findings partially contrast withthat study, as we did not observed any correlationbetween the extent of DE and PFTs. The differencein the results is probably due to the heterogeneitybetween the populations studied: in study of Gouldand coworkers the mean extent of BE was 27% oftotal lung volume, therefore the correlation be-tween DLCO and DE was conserved. In our popula-tion the extent of BE was more limitedð15:2� 8:2%Þ; though the presence of bullae inGroup I resulted in significantly lower TLCHE incomparison with Group II (Table 2).
In the density histogram of CTwe describe a signassociated with severe BE: the presence of abimodal distribution of the lung density, in therange between �910 and �1024HU; correspondingto the density of emphysema (Fig. 2). In ourexperience this finding was never observed in DEand is therefore specific for severe BE, and it wasassociated with the presence of a single large bulla(occupying 450% of a lung).
The main limit of this study is that a visual scorewas used to identify the BE, while an automaticscore was used to assess the overall extent ofemphysema. However, previous studies have shownthat the visual score is as reliable as the densitymask program in the quantification of emphysema,with no significant difference between the twotechniques, when the CT scan is performed by anexperienced radiologist.27
In conclusion, BE complicating DE substantiallycontributes to the functional deterioration andcauses significant confounding effects on thefunctional assessment. These results give a ratio-nale for the opportunity of bullectomy interventionin patients with both bullous and non-bullousemphysema at advanced stage. Furthermore, they
suggest that HRCT scan and helical quantitative CTscan are very useful in the work-up of BE, allowinga correct diagnosis of bullous disease, when thechest X-ray is only suggestive or negative, andclarifying the functional findings, that may beconfounding.
References
1. Fraser RS, Muller NL, Colman N, Pare PD. Chronic obstructivedisease. in: Fraser RS, Muller NL, Colman N, Pare PD,editors. Diagnosis of diseases of the chest. Philadelphia: WBSaunders Company; 2000.
2. Murphy DM, Fishman AP. Bullous diseases of the lung. in:Fishman AP, editor. Pulmonary diseases. New York: McGraw-Hill; 1998.
3. Morgan MDL, Edwards CW, Morris J, Matthews HR. Origin andbehaviour of emphysematous bullae. Thorax 1989;44:533–8.
4. Laurenzi GA, Turino GM, Fishman AP. Bullous disease of thelung. Am J Med 1962;32:361–78.
5. Zompatori M, Fasano L, Battista G, Canini R. Diagnosticimaging of bullous pulmonary disease. Radiol Med1998;96:161–7.
6. Venuta F, Rendina EA, Pescarmona EO, et al. Occult lungcancer in patients with bullous emphysema. Thorax1997;52:289–90.
7. Pride NB, Hugh-Jones P, O’Brien EN, Smith LA. Changes inlung function following the surgical treatment of bullousemphysema. Q J Med 1970;39:49–69.
8. Baldi S, Palla A, Mussi A, et al. Influence of bulla volume onpostbullectomy outcome. Can Respir J 2001;8:233–8.
9. Pride NB. Breathing in patients with bullous emphysema:why lung volume reduction may work. Monaldi Arch ChestDis 1998;53:483–5.
10. Gould GA, Redpath AT, Ryan M, et al. Parenchymalemphysema measured by CT lung density correlates withlung function in patients with bullous disease. Eur Resp J1993;6:698–704.
11. Pauwels RA, Buist AS, Ma P, et al. Global strategy for thediagnosis, management, and prevention of chronic obstruc-tive pulmonary disease: National Heart, Lung, and BloodInstitute and World Health Organization Global Initiative forChronic Obstructive Lung Disease (GOLD): executive sum-mary. Respir Care 2001;46:798–825.
12. Piquette AC, Rennard SI, Snider GL. Chronic bronchitis andemphysema. in: Murray JF, Nadel AJ, editors. Textbook ofrespiratory medicine. Philadelphia: WB Saunders Company;2000.
13. Kauczor H, Wolcke B, Fisher B, et al. Three-dimensionalhelical CT of the tracheobronchial tree: evaluation ofimaging protocols and assessment of suspected stenoseswith bronchoscopic correlation. Am J Roentgenol1996;167:419–24.
14. Zompatori M, Fasano L, Mazzoli M, et al. Spiral CTevaluationof pulmonary emphysema using a low-dose technique.Radiol Med 2002;104:13–24.
15. Zompatori M, Fasano L, Fabbri M, et al. Assessment of theseverity of pulmonary emphysema by computer tomography.Monaldi Arch Chest Dis 1997;52:147–54.
16. American Thoracic Society. Standardization of Spirometry,1994 Update. Am J Respir Crit Care Med 1995;152:1107–36.
17. D’Angelo E, Prandi E, Milic-Emili J. Dependence of maximalflow-volume curves on time corse of preceding inspiration. JAppl Physiol 1993;75:1155–9.

ARTICLE IN PRESS
M. Mura et al.178
18. Melissinos CG, Mead J. Maximum expiratory flow changesinduced by longitudinal tension of trachea in normalsubjects. J Appl Physiol 1977;43:537–44.
19. Quanier PH. Standardized lung function testing. ReportWorking Party ‘‘Standardization of Lung Function Tests’’,European community for Coal and Steel. Eur Respir J1993;6:1–100.
20. Eltayara L, Becklake MR, Volta CA, Milic-Emili J. Relationshipbetween chronic dyspnoea and expiratory flow-limitation inpatients with chronic obstructive pulmonary disease. Am JRespir Crit Care Med 1996;154:1726–34.
21. Mahler DA, Harver A. Dyspnea. in: Fishman AP, editor.Pulmonary rehabilitation. New York: Marcel Dekker;1996.
22. Mahler DA, Guyatt GH, Jones PW. Clinical measurement ofdyspnea. in: Mahler D, editor. Dyspnea. New York: MarcelDekker; 1998.
23. Meyers BF, Patterson GA. Chronic obstructive pulmonarydisease. 10: Bullectomy, lung volume reduction surgery, andtransplantation for patients with chronic obstructive pul-monary disease. Thorax 2003;58:634–8.
24. Gelb AF, Gold WM, Nadel AJ. Mechanism limiting airflow inbullous lung disease. Am Rev Respir Dis 1973;107:571–8.
25. De Giacomo T, Rendina EA, Venuta F, et al. Bullectomy iscomparable to lung volume reduction surgery in patientswith end-stage emphysema. Eur J Cardiothor Surg2002;22:357–62.
26. Snider GL. Reduction pneumoplasty for giant bullousemphysema. Chest 1996;109:540–8.
27. Zompatori M, Battaglia M, Rimondi R, et al. Pulmonaryemphysema quantitation with Computed Tomography. Com-parison between the visual score with high resolution CT,expiratory density mask with spiral CT and lung functionstudies. Radiol Med 1997;93:374–81.