Embed Size (px)
Citation preview

Building Public/Private Partnership for Health System Strengthening
Contracting: Overview
Peter BermanThe World Bank
Bali Hyatt Hotel, Sanur, Bali21-25 June 2010

Outline
Separating the financing and delivery functions in government programs
Contracting is the use of contracts to achieve objectives. So…what is a “contract”?
Advantages and disadvantages of contracting Some examples Some “conditional guidance” on how to do
contracting

The key innovation in contracting is for government to separate
the financing and delivery functions
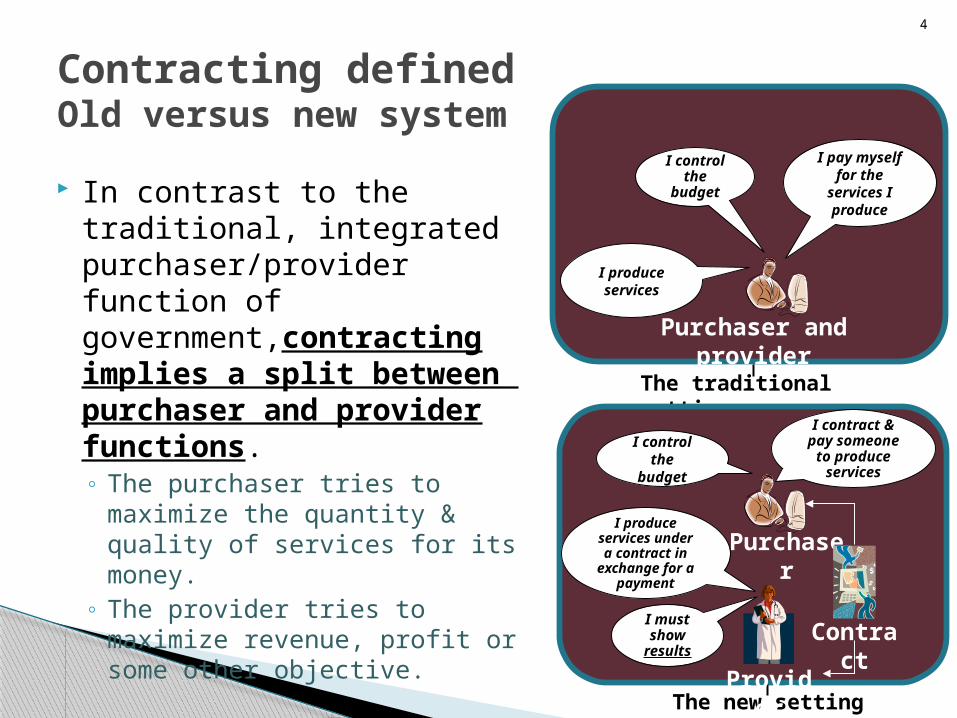
Contracting definedOld versus new system
In contrast to the traditional, integrated purchaser/provider function of government,contracting implies a split between purchaser and provider functions.◦ The purchaser tries to
maximize the quantity & quality of services for its money.
◦ The provider tries to maximize revenue, profit or some other objective.
4
I control the
budget
I produce services
I pay myself for the
services I produce
The traditional setting
Purchaser and provider
I control the
budget
I produce services under a contract in
exchange for a payment
I contract & pay someone
to produce services
The new setting
Purchaser
Provider
Contract
I must show
results
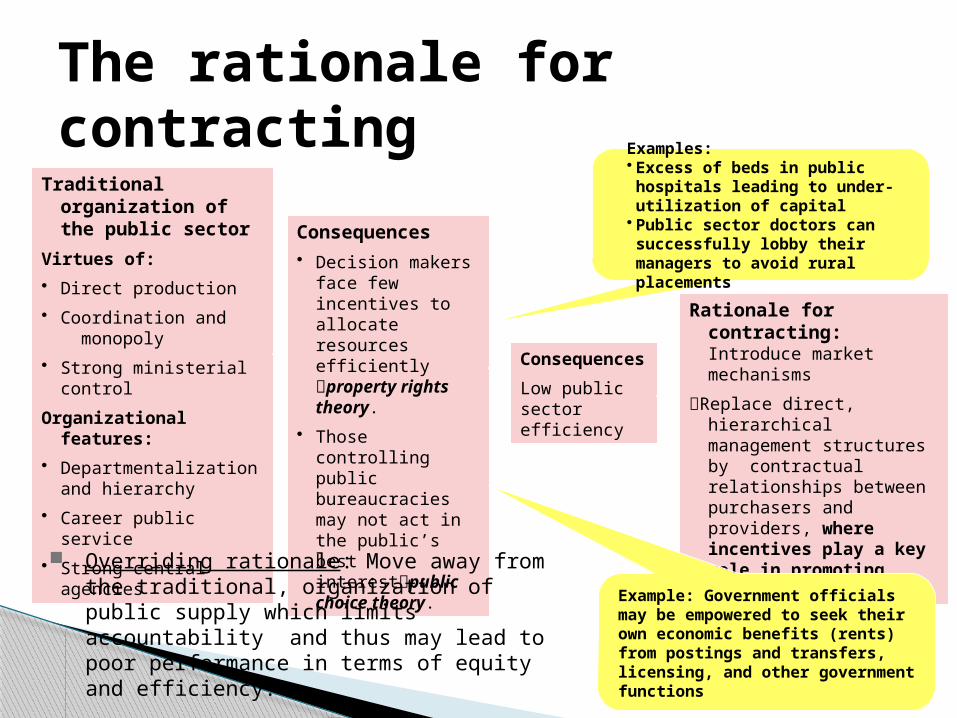
The rationale for contracting
5
Consequences
Low public sector efficiency
Traditional organization of the public sector
Virtues of:
• Direct production
• Coordination and monopoly
• Strong ministerial control
Organizational features:
• Departmentalization and hierarchy
• Career public service
• Strong central agencies
Consequences• Decision makers
face few incentives to allocate resources efficiently property rights theory.
• Those controlling public bureaucracies may not act in the public’s best interestpublic choice theory.
Rationale for contracting: Introduce market mechanisms
Replace direct, hierarchical management structures by contractual relationships between purchasers and providers, where incentives play a key role in promoting better performance.
Examples:• Excess of beds in public hospitals leading to under-utilization of capital
• Public sector doctors can successfully lobby their managers to avoid rural placements
Example: Government officials may be empowered to seek their own economic benefits (rents) from postings and transfers, licensing, and other government functions
Overriding rationale: Move away from the traditional, organization of public supply which limits accountability and thus may lead to poor performance in terms of equity and efficiency.

What is a “contract”? Contracting is the use of contracts to achieve
objectives
Contracting defined Contracting is a purchasing mechanism
used to acquire:◦ from a specific provider◦ a specified service◦ for an explicit quantity◦ of a known quality◦ at an agreed-on price◦ for a given period of time
In contrast to a one-off exchange, the term contracting implies an on-going relationship, supported by a contractual agreement.
7
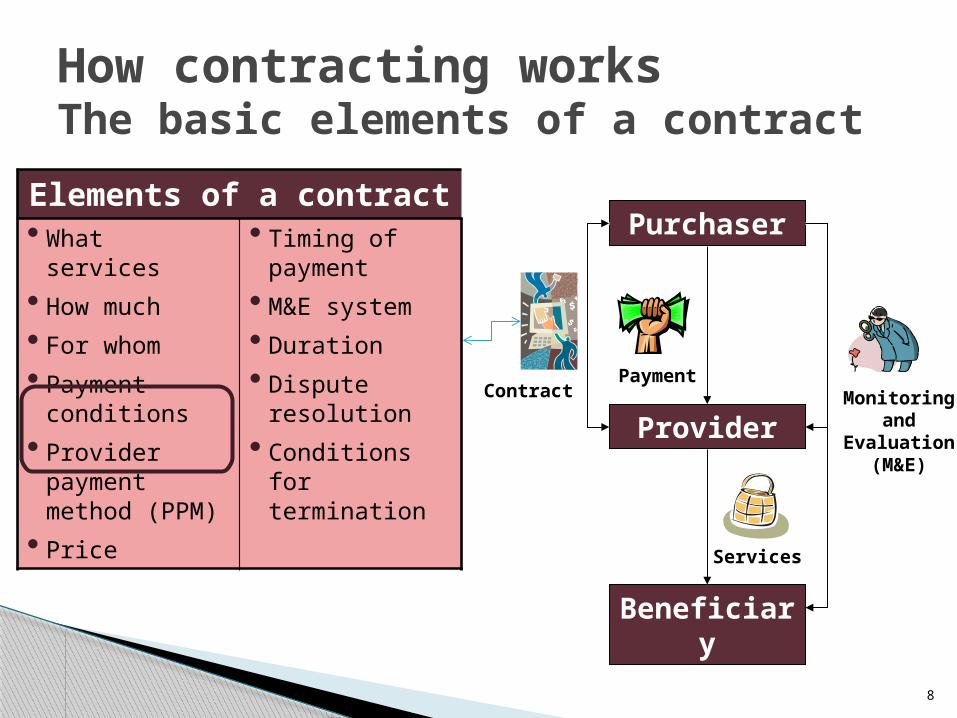
How contracting worksThe basic elements of a contract
8
Elements of a contract• What services
• How much
• For whom
• Payment conditions
• Provider payment method (PPM)
• Price
• Timing of payment
• M&E system
• Duration
• Dispute resolution
• Conditions for termination
Purchaser
Provider
Beneficiary
Contract Monitoring and
Evaluation (M&E)
Payment
Services
Different contracting arrangements Contracting in
◦ Bring outside private management to operate an internal government service (e.g., hire a private firm to run cleaning or catering services inside a public hospital).
Contracting out◦ Purchase services from a private source that provides
the service using external workforce and resource.
Contracting can be done with public or private providers◦ Governments can contract with public autonomous
institutions or with private providers.
9

Advantages and disadvantages of contracting
Potential benefits of contracting Competitive forces:
◦ Contracting can generate pressure on providers to improve performance in both price and quality (but this benefit hinges on the actual competitive forces at work).
Planning and policy development:◦ Contracting requires and may promote better planning & policy
development by improving the flow of information about volumes of goods, services, costs, quality, responsiveness, population served, health needs, and other issues.
Price stability:◦ Contracting provides government with a mechanism for purchasing
needed health services at an agreed-on and, therefore, predicable price.
Improve equity:◦ Contracting can focus on delivering services to targeted population
groups.
11

Potential drawbacks of contracting Transaction costs:
◦ If significant costs in designing, M&E, and managing CO government may not capture efficiency gains from CO.
Government capacity:◦ Government limitations to design & manage contracts may limit
potential gains from CO. Provider capacity:
◦ Weak private sector limited number and capacity of bidders low quality.
Setting the price right is difficult:◦ If government over- or under-estimates price, this may waste resources
or threaten providers’ financial equilibrium. Monitoring and evaluation:
◦ If few resources allocated to M&E of providers, government may be unable to effectively enforce contracts & achieve strategic outcomes.
Quality may be a casualty of CO: ◦ Even if contracts specify quality, providers may save on non-verifiable
aspects of care, especially if purchasers have limited ability to scrutinize & enforce contracts.
12

One ExampleNGO Contracting in
CambodiaLarge Scale
Detailed Impact Evaluation
Methodology Used to Evaluate Contracting in Cambodia
12 districts (100,000-180,000 pop’n each) randomly assigned to CO, CI, or GS
3 districts were not contracted G
Baseline household surveys carried out by 3rd party in 1997
Follow-on survey carried out in mid-2001, 2.5 years after start of the contracts and in 2003, 4 years into the contracts
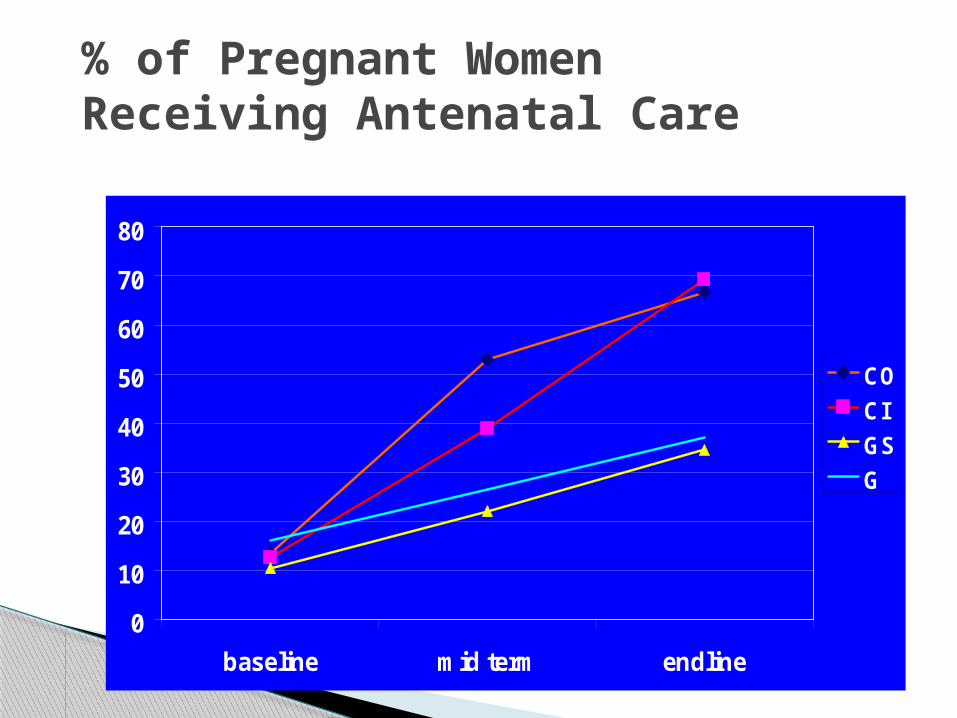
% of Pregnant Women Receiving Antenatal Care
0
10
20
30
40
50
60
70
80
baseline mid term endline
CO
CI
GS
G

Health Center Utilization in the Last Month (%)
0
10
20
30
40
baseline mid term endline
CO
CI
GS
G

% of Deliveries Taking Place in Health Facility
0
5
10
15
20
25
baseline mid term endline
CO
CI
GS
G
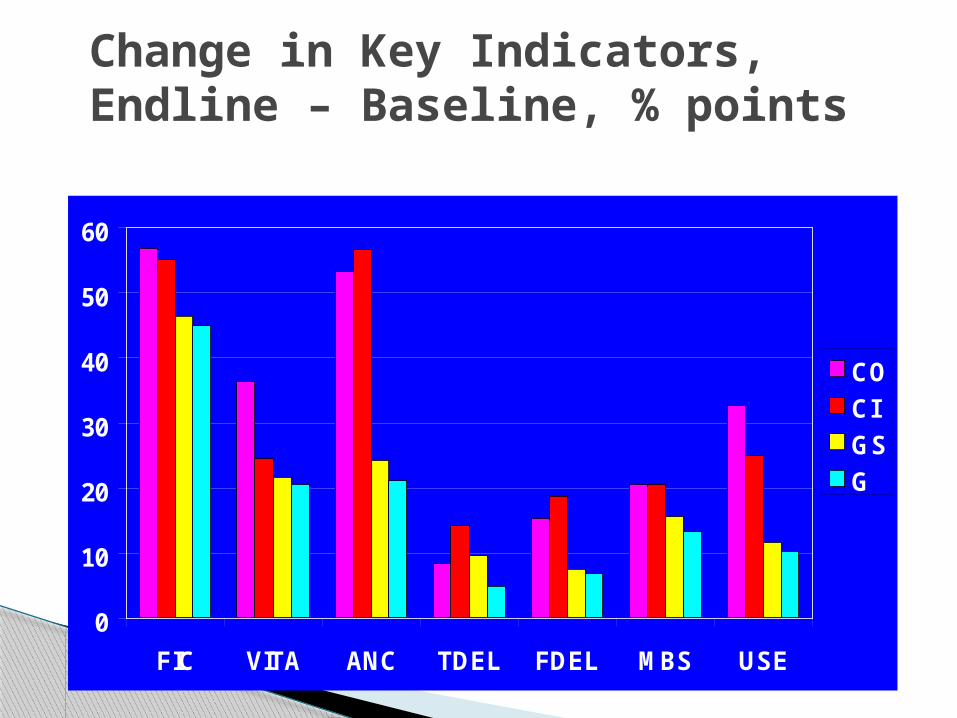
Change in Key Indicators,Endline – Baseline, % points
0
10
20
30
40
50
60
FIC VITA ANC TDEL FDEL MBS USE
CO
CI
GS
G

Change in Concentration Index Endline - Baseline
-0.25
-0.15
-0.05
0.05
0.15
0.25
FIC VITA ANC TDEL FDEL MBS USE
CO
CI
GS
G
More Pro-Poor
Less Pro-Poor
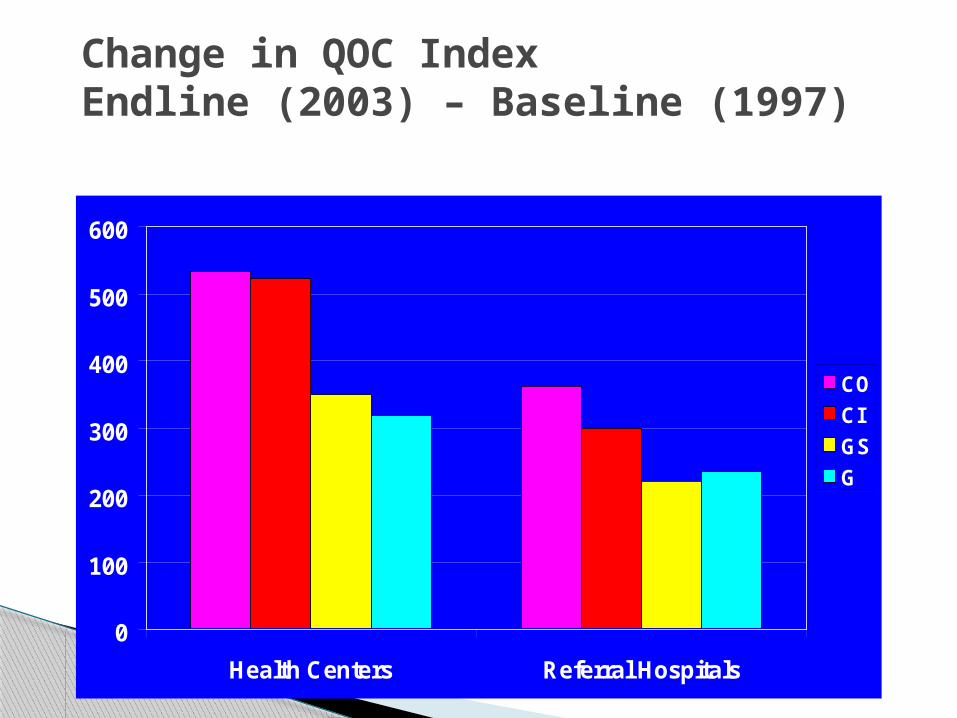
Change in QOC Index Endline (2003) – Baseline (1997)
0
100
200
300
400
500
600
Health Centers Referral Hospitals
CO
CI
GS
G

Total Per Capita Health Expenditures - 2003
1.71.743.474.83
19.9919.8616.7214.29
0
5
10
15
20
25
CO CI GS G
OOP
Public
19.12 20.1921.60 21.69

Discussion Questions
1. What do you think about contracting with NGOs as a way of improving delivery of PHC?
2. What do you think would be the likely impediments or difficulties in introducing contracting in the context in which you work?
3. Besides changes in coverage of services, how else would you evaluate the performance of the NGOs and contracting in general?
Discussion Questions
4) What do you think would be the obstacles to sustainability of contracting in your context in which you work?
5)What would be the advantages and
disadvantages of increasing the scale of each contract to cover 2 or 3 operational districts?

Some Guidance on Implementation
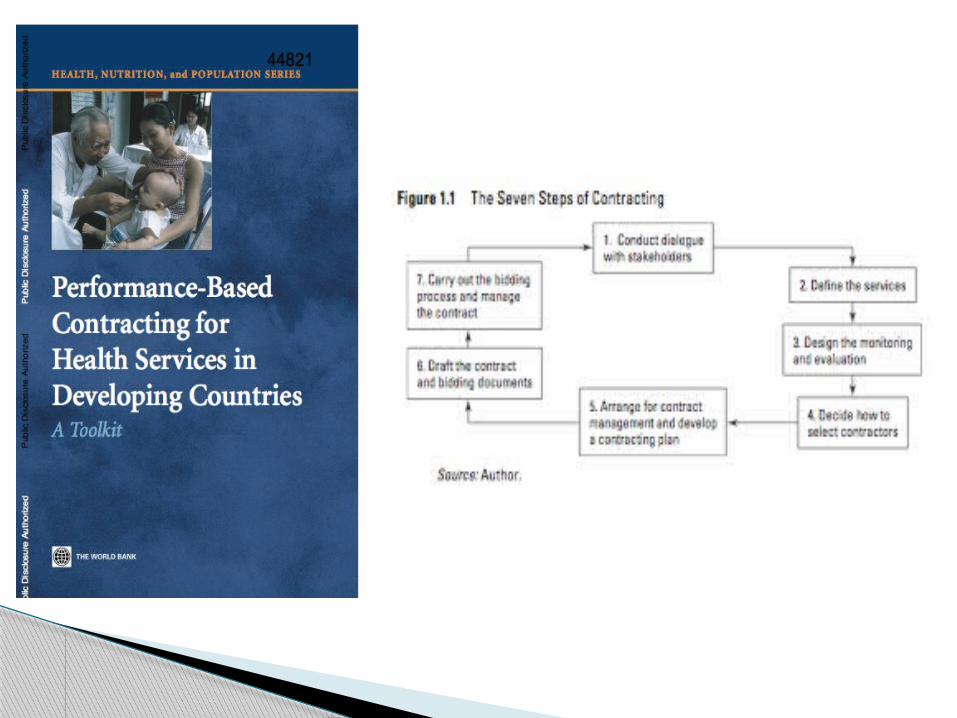
Design of Agreements/Contracts1. Defining Objectives
2. Maximizing Managerial Autonomy
3. Size of Individual Contracts
4. Other important aspects of contracts
Defining Objectives Big advantage of contracting is results focus
so concentrate on outputs not inputs
The clientshould objectively define:◦Quantity of services (e.g. % DTP3
coverage)◦Quality of care (national technical
guidelines) ◦Equity (ensuring the poor receive services)◦Catchment area and population
Stating Objectives They need to address the most important
outputs/outcomes
There can’t be too many – indicator inflation
They need to be measurable and actually intend to be measured
Targets need to be realistic and plausible, not aspirational

How to ensuring focus on results Use performance bonuses
Provide baseline data to contractors
Regular discussion of indicators
Use and improvement of HMIS data
Credible threat of being fired for non-performance
Use and review the contract

Ensuring Managerial Autonomy Decentralize management to people who
are closest to the ground reality
Accountability for results is easier when managers have responsibility and autonomy
Encourage innovation
Take advantage of private sector’s flexibility
Impediments to Managerial Autonomy Telling contractors “how” they should deliver
services (define objectives, “what”)
Too specific line item budgets ( is it possible to use lump-sum contracts with performance benchmarks?)
Government procures important inputs (allow contractors to do procurement)
Require following Government procedures for staff hiring, firing, transfer, and pay
Unclear authority of government officials

Scale – Size of “Packages”
Economies of scale affects the cost (price) per beneficiary◦Distributing management and admin costs
Large packages facilitate contract management
Easier and cheaper to monitor and evaluate contractor performance with fewer packages
◦ Hence packages should cover millions or hundreds of thousands
Need to balance against concerns regarding contractor capacity

Other Important Aspects
Duration: 3-5 years is minimum, takes time to build relationships, no advantage to yearly “renewal”, but can use performance reviews
Termination/Sanctions: Clearly spelled out procedures. Embarrassment works!!
Payments: Mobilization payment often needed, 6 monthly payment thereafter (less frequent payment may increase timeliness of payment)
Reporting Requirements: Clear, not onerous.

Other Important Aspects Procurement:contractor should be
responsible for procurement, generally. Standards needed for drug quality
User Charges: should contractor be able to implement user charges (if they want to) within guidelines and conditions to assure protection of poor?
Training/Capacity Building:may include contractor obligations in terms of training and capacity building, access to training courses should be specified if coming from government.

Relationships & Responsibilities Contract type: For services already being
delivered by government, “contracting-in” is often easier◦need to define relations with existing
staff
All contracts need to define authority of government officials
Infrastructure: – who owns it? contractor pays for maintenance & repair
Concluding Thoughts

Challenges and potentials Many of the posited difficulties of contracting
can be managed or are exaggerated – need to compare with the alternative of government provision:◦ Not only small scale◦ Not necessarily more expensive◦ Government can manage (if capacity developed)◦ Trust can be developed◦ Equity may be improved◦ As sustainable as government will to finance
There is ample evidence of potential – one of a set of possible strategies to improve outcomes





























