Embed Size (px)
Citation preview

David LukeCoordinator, ATPC16 July, 2020
Economic Commission for Africa
Building competitive and resilient African pharmaceutical value chains through the African
Continental Free Trade Area

PHARMACEUTICAL TRENDS IN AFRICA

Trade in goods: trends
Africa’s trade in pharmaceuticals (medicines and equipment combined) increased steadily over the past two decades• Africa’s total exports increased from US$ 0.2 billion in 1998 to US$ 1.4 billion in 2018• Africa’s total imports jumped from $4.2 billion in 1998 to over $20 billion in 2018• Africa’s trade deficit in pharmaceuticals has increased significantly
Almost all Africa’s pharmaceuticals imports originate from outside the continent• 97% of Africa’s total imports (average period 2016-2018) originate from outside Africa• About 51% of which is sourced from the EU alone
In contrast, a substantial share of Africa’s pharmaceuticals exports are directed towards the continent itself• Intra-African pharmaceuticals exports account for 40.6% of Africa’s total pharmaceutical exports• Senegal, Tanzania, Zimbabwe, Zambia, Sudan and Uganda are important main destinations, each
receiving at least 5% of Africa’s pharmaceutical exports to Africa• South Africa, Kenya, Ghana and Egypt are the main exporters, supplying 26.6%, 18.7%, 12.7%
and 10.9% of Africa’s total exports to Africa, respectively• Outside the continent, EU remains the leading destination for African exports (43.4% of African
exports to the rest of the world)

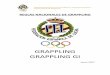
Trade in goods: composition
• Medicines (including antibiotics) represent the bulk of Africa’s total pharmaceuticals trade:
o Imports: the shares of medicines vs. equipment are relatively comparable between intra-African imports (82.6% for medicines vs. 17.4% for equip.) and Africa’s imports from the ROW (81.4% vs. 18.6%)
o Exports: there is a more pronounced difference in the shares of medicines vs. equipment between intra-African exports (82.6% for medicines vs. 17.4% for equip.) and Africa’s exports to the ROW (65.1% vs. 34.9%)
• Pharmaceutical equipment, which accounts for a higher share of Africa’s exports to rest of world vs. within Africa, typically embeds higher value added content than medicines
82.62%
65.14%
17.38%
34.86%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Africa Rest-of-the-world
Export composition
82.62% 81.36%
17.38% 18.64%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Africa Rest-of-the-world
Import composition
Optical,Medical,SurgicalInstruments
Antibiotics andPharmaceuticalproducts
Source: ECA’s calculations based on BACI dataset

Trade in goods: SNA end uses
• According to the system of national accounts (SNA), Africa largely imports pharmaceuticals for final consumption (60.6%), followed by intermediates (27.7%) and capital goods (11.7%)
• The proportion of intermediates (vs. consumption vs. capital goods) is relatively lower in intra-African imports (19.1% vs. 69.8% vs. 11.1%) compared to Africa’s imports from the rest of the world (28.0% vs. 60.3% vs. 11.7%)
• This indicates a reliance of Africa on outside partners for intermediates, which are subsequently used in the production of pharmaceuticals
• The composition of exports of pharmaceuticals in terms of intermediates vs. consumption goods vs. capital goods is relatively similar to that of imports
11.16%20.00% 16.42%
69.84% 51.56% 58.97%
19.00%28.44% 24.61%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Africa Rest-of-the-world TOTAL
SNA category exports (2016-2018)
11.15% 11.68% 11.66%
69.80%60.32% 60.62%
19.05%28.00% 27.72%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Africa Rest-of-the-world TOTAL
SNA category imports (2016-2018)
IntermediategoodsConsumptiongoodsCapital goods
Source: ECA’s calculations based on BACI dataset

Tariffs – pharmaceutical industry
Africa’s annual
imports (US$ 2016-18 average)
Africa’s annual
exports (US$ 2016-18 average)
Average MFN tariff
imposed by Africa on its imports from
Average MFN tariff faced by
Africa on its exports to
World 19.80 billion 1.37 billion 3.9% 2.6%
Intra-Africa 0.53 billion 3.7% 3.02%
Rest of the world 19.27 billion 0.84 billion 3.9% 2.5%
• Average tariffs on pharmaceuticals imposed and faced by Africa are relatively low, regardless of the origin or destination
• However, in terms of import tariffs (only), those tend to be higher (regardless of the origin) and requiring greater attention (including in AfCFTA context) for:o A few countries (e.g. Djibouti, Ghana, Algeria, DRC, Ethiopia, Sudan);o A few products (e.g. optical equipment and medical instruments such as thermometers and
hydrometers).
Source: ECA’s calculations based on MacMap-hs6 tariffs data (trade weighted)

COVID-19 IMPACTS ON PHARMA VALUE CHAINS

Access
Border disruptionsLockdowns
Key players in pharma VCs (e.g. China and India) put in place containment measures which adversely impacts supply globally Social distancing Travel bans Factory closures
This puts “import-dependent” Africa in a perilous position Supplies of global pharma
factories operating in Africa have also been adversely impacted by lockdown measures
To tackle domestic shortages, 95 countries have introduced COVID-19 related export bans 14 of these are in Africa Most of these bans are
concentrated on medical supplies (other than food) E.g. India banned export
of alcohol based hand sanitizers, and certain kinds of masks, ventilators and textile raw materials for masks and coveralls
38 African countries have announced land border closures and 17 have announced maritime border closures Most regions introduced
guidelines to prioritize and facilitate interstate flow of essential goods, including medicines, fuel and food Yet, COVID-19 border
regulations have led to border disruptions which also slow down the flow of pharma supplies Green lanes for “super-
fast” clearance can help
Export restrictions

Price
Pharma ingredients
Prices of pharma ingredients manufactured in China are rising Global spill over effects: since 70% of APIs
used in Indian drug production originate from China, and India is responsible for 20% of pharmaceuticals production in volume terms globally
Cost of importing APIs has increased further due to rising price of air freight
Logistics providers and pharma companies are grappling with capacity constraints Most pharma cargo is transported on
passenger flights, which have been cancelled due to travel bans
Yet, demand for air cargo to transport pharmaceuticals has increased by 100%
Air freight
Share of China and India in African imports of intermediate pharmaceutical products
Intermediate pharmaceutical productGlands
and other organs
Human or
animal blood
Medicaments consisting of two or more constituents
Wadding, gauze and bandages
Pharmac-euticalgoods n.e.s.
Ghana China 2.13 1.60 64.62 10.08India 58.34 45.93 56.07 10.88 8.57
Kenya China 10.65 1.08 15.90 70.95 27.15India 25.81 11.41 4.37 5.47
Nigeria China 9.88 3.55 12.67 96.02 57.89India 33.49 30.81 0.14 1.78
Tanzania China 1.83 0.28 78.82 60.47India 95.17 18.54 91.76 4.75 13.79
Uganda China 0.21 0.01 76.62 4.45India 14.15 47.22 3.52 9.04
South Africa
China 20.10 0.12 18.97 32.47 7.36India 0.08 0.27 34.85 2.96 0.34
Source: ECA-ODI calculations using Comtrade

• As African countries struggle to procure medical products from global suppliers, there has been a positive shift from global supply chains towards more regionalized and local supply chains
• This demonstrates that there is potential for African industries to respond to demand
• ECA-AFREXIMBANK are supporting the scaling up of manufacturing of medical supplies that can be produced in Africa and sent across borders
• Regional approach based on comparative advantage and economies of scale
Supply
EXAMPLESSouth Africa
U-Mask redirected production from protective masks for mining and agricultural companies to medical respirator masks
Nigeria National Agency for Science and Engineering Infrastructure produced first made in Nigeria ventilator
Senegal In collaboration with the UK and France, is prototyping a pocket-sized kit which will cost less than 1 USD
Ghana Diagnostic firm in cooperation with a local university developed a test that delivers results in 20 minutes
Continental AU Africa Task Force for COVID-19 is working to connect Member States that have medical supply shortages, with those that have surplus supplies

Case Study: Impact of COVID-19 on firms in AfricaATPC-IEC online firms survey
80% of respondents indicated being significantly affected by COVID-19
MSMEs were particularly concerned by the cash flow outlook, while large companies noted challenges on the need to adapt their business model to the crisis
The rate of capacity utilization ranged from 30-40% (for small-sized enterprises) to 50-60% (for large-sized enterprises)
Logistical contingencies due to covid-19 have pushed companies to build-up high stocks
This structurally costly strategy has typically proved effective during the crisis to make up for unforeseen events
the crisis has forced companies to adapt their operations, and integrate digital working methods that are likely to remain after the crisis
Cash flow was raised as a major concern, with some interviewees noting that they preferred to keep goods rather than sell without the certainty of timely payment
ATPC-AFD pharma industry interviews
Top 3 challenges faced by company, by size
Source: ECA & IEC (2020). Insights on African businesses’ reactions and outlook to COVID-19

LEVERAGING AFCFTA TO DEVELOP AFRICA’S PHARMACEUTICAL INDUSTRY

Bringing the pharma sector to the heart of the AfCFTA
• Business opportunities in Africa’s healthcare and wellness sector are estimated tobe worth US$259 billion by the year 2030, with potential to create 16 million jobs
• 14 per cent of all business opportunities in the healthcare and wellness sectorglobally are estimated to be in Africa
• There are numerous opportunities for the private sector to invest in laboratory anddiagnostics, pharmaceuticals, skills development, research and capacity building,and digital health innovations
• AfCFTA offers the perfect platform for businesses to tap into these opportunities• The Agreement will create an environment conducive for establishing regional value
chains and champions in the pharmaceutical sector, which can be leveraged as aspringboard for nurturing African multinationals
• Yet it will not provide a panacea to Africa’s over-reliance on pharmaceuticals withouta targeted framework that integrates an awareness of the multiple ways in whichtrade can impact on health systems
• Delay to start of trading (brought about by COVID-19) offers a window ofopportunity
• Creative thinking is now required on how the AfCFTA can be reconfigured to elevatethe pharmaceutical sector as the heart of the AfCFTA Agreement

Priority ‘pharma’ actions for the AfCFTA
• Pharmaceutical and medical products should not be included in the sensitive item or exclusion lists of State Parties’ tariff schedules
• The timeframe of 5 years for liberalization of pharmaceutical goods should be reduced in order to speed up the development of African value chains in anticipation of future shocks
• An AU directive would help to support compliance with these proposals
• The finalization of rules of origin should be prioritized for pharma products and textile and apparel covering PPE and masks
• Fast track digitization of systems of origin certification
Trade in goods Trade in services
• Member states should consider adding health and education services to the priority list of services sectors for the first round of services negotiations
• Alternatively, the liberalization of professional services under the overall business services sector, could extend to cover medical services personnel
• Complementary efforts needed to facilitate international movement of critical health and technical experts in a safe manner
• Ensuring equivalency of accreditation for health-related degrees and programmes is crucial to facilitate quick health responses, including movement of workers

Priority ‘pharma’ actions for the AfCFTA
• Implementation of the already finalized NTB Mechanism and AfCFTA trade facilitation, customs cooperation and transit trade annexes should be fast-tracked
• These annexes must be implemented in a manner that is cognizant of the risks of unregulated movements of pathogens and hazardous goods
• State Parties should prioritize the harmonization of standards for medical and pharmaceutical products
• The AfCFTA should be used as a platform for African standards bodies to pool and share resources to provide expedited testing and safety approval for new production of medical equipment in Africa.
Non-tariff Measures Intellectual Property Rights
• The pharmaceutical sector should be central to the second phase AfCFTAintellectual property rights negotiations
• Through supporting Africa to negotiate as a coherent bloc, AfCFTA should be used to strengthen the continent’s ability to ensure TRIPS flexibilities are fully utilized in efforts to enable local production and access to essential medicines
• When a COVID-19 vaccine becomes available, a coordinated African notification to the WTO of the use of TRIPS flexibilities will be crucial

ECA’s AfCFTA-anchored pharma initiative
To overcome Africa’s reliance on imported pharmaceuticals, ECA has launched an initiative toensure access to efficacious, safe, and affordable medicines and supplies• The initiative is expected to support intra-African trade in pharmaceuticals under the AfCFTA, and
operationalization of the African Medicines Agency (AMA)• The AfCFTA-anchored pharma project will be piloted in ten African countries (with support from IGAD):
Comoros, Djibouti, Eritrea, Ethiopia, Kenya, Madagascar, Mauritius, Rwanda, Seychelles, and Sudan• Priority area: reproductive health
The initiative adopts a three-pronged approach:• Localized production• Pooled procurement• Harmonized regulatory and quality frameworks
Progress has already been made to support African pharmaceutical production:• Continental based pharmaceutical manufacturers have been identified and shortlisted• Quality standards for scaling-up production have been ascertained
As part of the initiative, ECA is supporting African countries to respond to COVID-19• ECA is collaborating with AFREXIMBANK, Africa CDC and ECONET to strengthen capacities and
capabilities of local manufacturers (including agriculture companies) to scale-up or repurpose theirproduction facilities to respond to COVID-19 needs
• This includes PPE, equipment such as ventilators, and food supplies to cater for forecasted gaps

THANK YOU!