Embed Size (px)
Citation preview
Institute for Public Policy Research
The progressive policy think tank
BUILDING BACK CANCER SERVICES IN ENGLAND Parth Patel and Chris Thomas
September 2021
IPPR Building back cancer services in England 2
About the authors
Dr Parth Patel is a research fellow at IPPR
Chris Thomas is a senior research fellow at IPPR
Charitable purpose
This research fulfils IPPR’s charitable purpose of advancing health and public services
Acknowledgements
Lilly provided financial support to IPPR that made this work possible. IPPR retained full editorial control.
This paper forms part of IPPR’s Better Health and Care Programme. IPPR would like to thank the founding sponsors of the programme: Gilead, AbbVie, GSK, AstraZeneca, Carnall Farrar and Siemens Healthineers. The authors would like to thank Nour Mohanna, Matt Ware, Scott Bentley, Ben Richardson from CF for the quantitative analysis and modelling in this paper and Harry Quilter-Pinner, Clare McNeil, David Wastell and Robin Harvey from IPPR for their contributions to this paper.

IPPR Building back cancer services in England 3
THE STATE OF CANCER SERVICES IN ENGLAND
The pandemic has severely disrupted cancer services in England. While Covid-19 might not have caused our health service to ‘collapse’ rapidly, it has forced us to take previously unthinkable steps like cancelling cancer treatments.
There have been widespread disruptions across the cancer care pathway – screening, referrals, diagnostic and treatment services have all seen reductions in activity. Unmitigated, the consequences will be severe. Delays in cancer referrals during the first wave of the pandemic are estimated to have undone two, six and eight years of improvements in five-year survival rates from lung, breast and colorectal cancer (Patel, Thomas and Quilter-Pinner 2021).
Fortunately, cancer services have been considerably more resilient to subsequent Covid-19 waves (figures 1 and 2), which is testament to the planning and measures put in place by NHS institutions across the country. But national progress on ‘missing patient backlogs’ across the cancer care pathway has been slow and there is considerable catch up to be done in diagnostic and treatment services. The ‘missing patient backlogs’ in cancer care are perhaps the most urgent in the NHS – for every four week delay in diagnosis and treatment of cancer, estimates suggest between a 6-13% loss in cancer survival (Hanna et al 2020).
FIGURE 1:
Cancer referrals fell dramatically when the dramatically and have been slow to recover
Per cent service activity by compared to 2019 levels
Source: CF analysis of NHS England datasets 2021
IPPR Building back cancer services in England 4
FIGURE 2
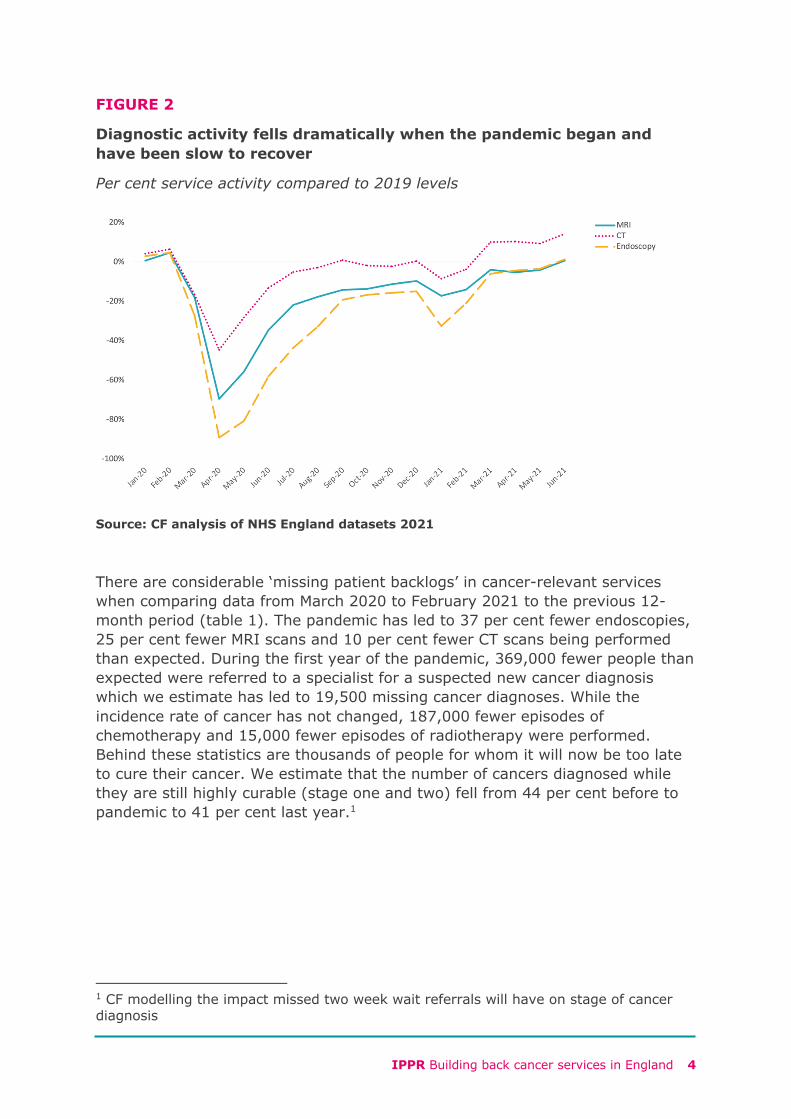
Diagnostic activity fells dramatically when the pandemic began and have been slow to recover
Per cent service activity compared to 2019 levels
Source: CF analysis of NHS England datasets 2021
There are considerable ‘missing patient backlogs’ in cancer-relevant services when comparing data from March 2020 to February 2021 to the previous 12-month period (table 1). The pandemic has led to 37 per cent fewer endoscopies, 25 per cent fewer MRI scans and 10 per cent fewer CT scans being performed than expected. During the first year of the pandemic, 369,000 fewer people than expected were referred to a specialist for a suspected new cancer diagnosis which we estimate has led to 19,500 missing cancer diagnoses. While the incidence rate of cancer has not changed, 187,000 fewer episodes of chemotherapy and 15,000 fewer episodes of radiotherapy were performed. Behind these statistics are thousands of people for whom it will now be too late to cure their cancer. We estimate that the number of cancers diagnosed while they are still highly curable (stage one and two) fell from 44 per cent before to pandemic to 41 per cent last year.1
1 CF modelling the impact missed two week wait referrals will have on stage of cancer diagnosis
IPPR Building back cancer services in England 5
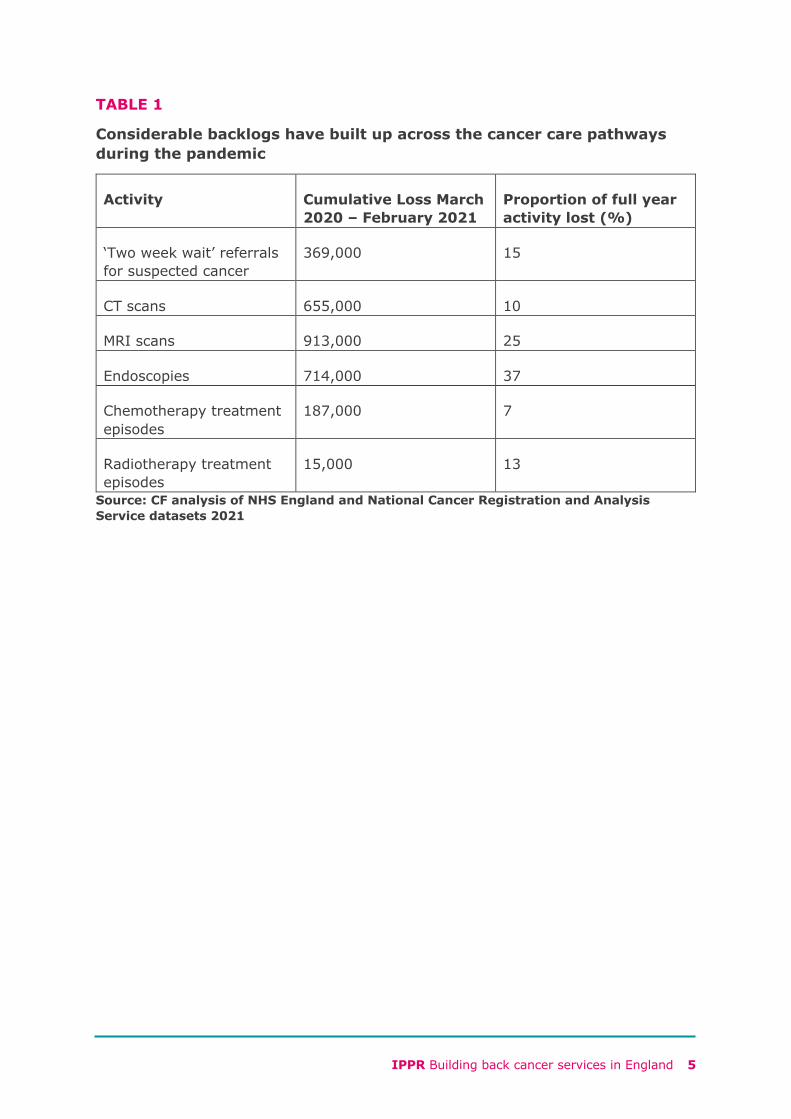
TABLE 1
Considerable backlogs have built up across the cancer care pathways during the pandemic
Activity Cumulative Loss March 2020 – February 2021
Proportion of full year activity lost (%)
‘Two week wait’ referrals for suspected cancer
369,000 15
CT scans 655,000 10
MRI scans 913,000 25
Endoscopies 714,000 37
Chemotherapy treatment episodes
187,000 7
Radiotherapy treatment episodes
15,000 13
Source: CF analysis of NHS England and National Cancer Registration and Analysis Service datasets 2021
IPPR Building back cancer services in England 6
CHARTING THE RECOVERY
Different parts of the cancer care pathway are experiencing different magnitudes of challenge. Working with CF, the health consultancy and data analytics company, we have modelled how long it will take to address these care backlogs under different activity level scenarios.
This model assumes that 75 per cent of the ‘missing suspected cancer patients’ will eventually present to some form of NHS service for a suspected cancer referral or investigation. It also assumes that 90 per cent of those with cancer who have missed chemotherapy or radiotherapy treatment since the pandemic began will eventually present for treatment (including palliative chemotherapy and radiotherapy). We made these assumptions after discussion with clinical oncologists. The model also assumes demographic change will lead to a 4 per cent increase in demand on services over time. Based on these assumptions, CF have modelled how long it will take to address backlogs across the cancer care pathway (table 2).
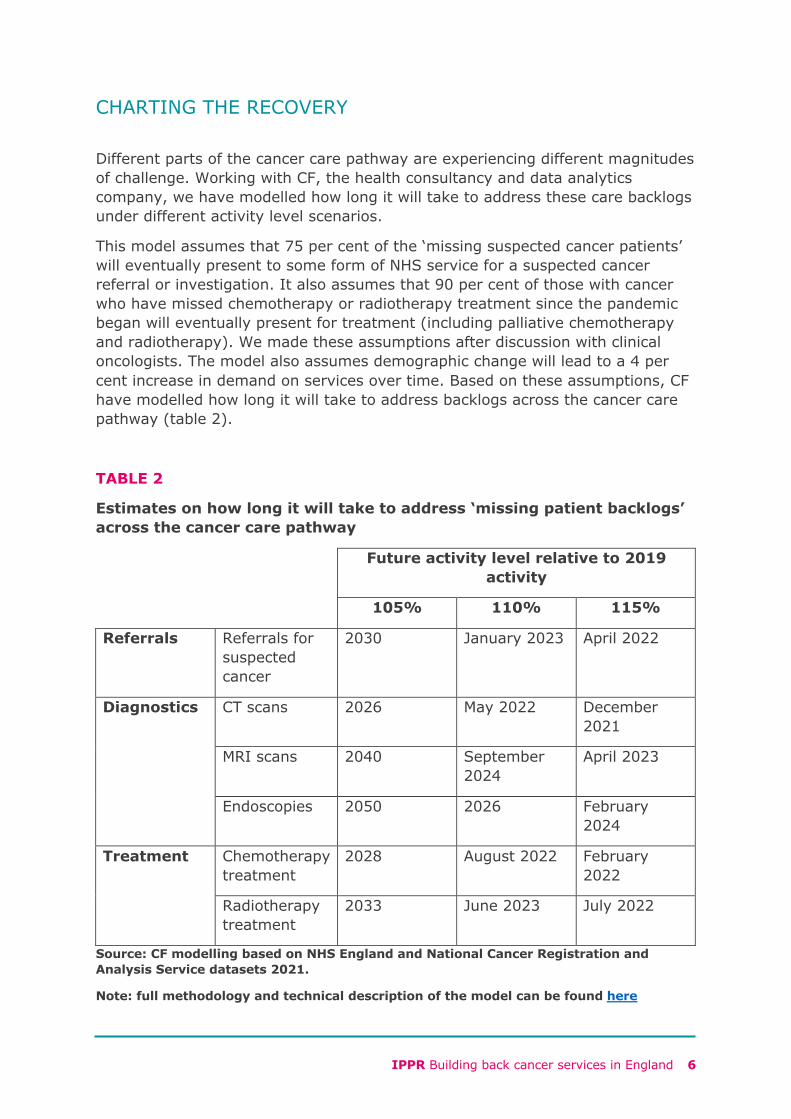
TABLE 2
Estimates on how long it will take to address ‘missing patient backlogs’ across the cancer care pathway
Future activity level relative to 2019 activity
105% 110% 115%
Referrals Referrals for suspected cancer
2030 January 2023 April 2022
Diagnostics CT scans 2026 May 2022 December 2021
MRI scans 2040 September 2024
April 2023
Endoscopies 2050 2026 February 2024
Treatment Chemotherapy treatment
2028 August 2022 February 2022
Radiotherapy treatment
2033 June 2023 July 2022
Source: CF modelling based on NHS England and National Cancer Registration and Analysis Service datasets 2021.
Note: full methodology and technical description of the model can be found here
IPPR Building back cancer services in England 7
Even if stretched hospitals can maintain national services at 105 per cent of pre-pandemic activity levels, it will take until 2028 and 2033 to make up for missed chemotherapy and radiotherapy treatment. It would take considerably longer to recover missed diagnostic investigations. This slow recovery is because at 105 per cent of pre-pandemic activity is to a great extent cancelled out by demographic pressures on service demand.
However, if activity levels across the cancer care pathway could be increased and maintained at 115 per cent of 2019 levels, most backlogs across the cancer care pathway could be addressed by next year. That would prevent many cancer-related deaths. Achieving this relies first and foremost on a larger workforce, more diagnostic and treatment equipment, and more physical space to provide care in.
Recovering cancer services will take a concerted and sustained effort. This is unlikely to be doable in the NHS as currently resourced and staffed. The health service was running hot before the pandemic began (Thomas 2020), and the solution cannot be to simply run it hotter. This would have consequences for workforce retention, service access and quality, and patient outcomes.
THE SEPTEMBER 2021 FUNDING SETTLEMENT
In September 2021, the government announced it will invest £30.3 billion in health and care services in England over the next three years. Of this, £15.8 billion will go to the NHS. This amounts to approximately £1 billion more by 2024/25 than would be expected if NHS funding continued at the same rate of growth as the settlement that came with the NHS Long Term Plan.
That means trade-offs between COVID-19 services, recovering backlogs across specialties and transforming the health service to deliver Long Term Plan targets are inevitable. The funding for the NHS is approximately half of what NHS Providers and NHS Confederation have estimated the service requires to avoid such trade-offs.
The government’s three-year funding plans for health and care services, announced in September 2021, states the additional funding it is providing means the “NHS in England can aim to deliver around 30 per cent more elective activity by 2024/25 than it was before the pandemic”. It is difficult to see how the level of funding announced will enable such dramatic activity increases, which is also limited by the size of the workforce and the amount of equipment and physical space in the health service.
IPPR Building back cancer services in England 8
IS RECOVERY ENOUGH?
Even if it is possible to maintain higher activity levels in cancer services, we should question whether a return to 2019 quality and outcomes constitutes the right level of ambition. Before the pandemic, the UK had lower one-year survival rates for stomach, colon, rectal and lung cancer than Australia, Canada, Denmark, Ireland, New Zealand and Norway (Arnold et al 2019).
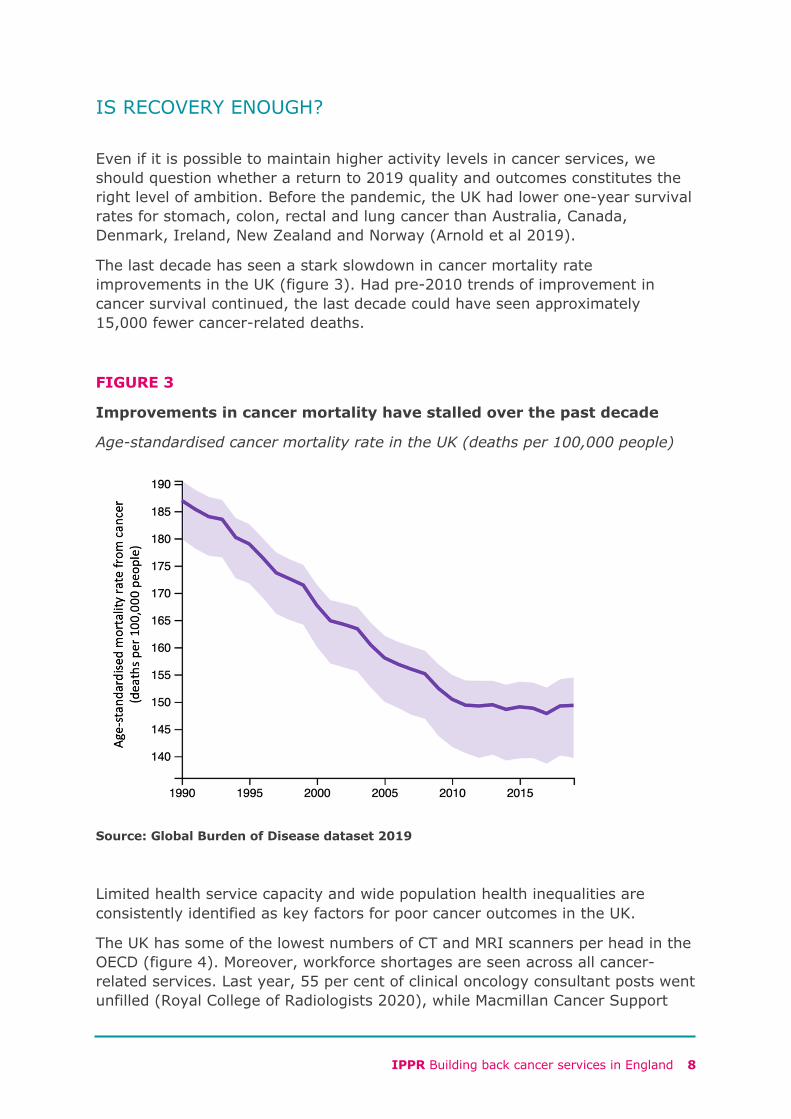
The last decade has seen a stark slowdown in cancer mortality rate improvements in the UK (figure 3). Had pre-2010 trends of improvement in cancer survival continued, the last decade could have seen approximately 15,000 fewer cancer-related deaths.
FIGURE 3
Improvements in cancer mortality have stalled over the past decade
Age-standardised cancer mortality rate in the UK (deaths per 100,000 people)
Source: Global Burden of Disease dataset 2019
Limited health service capacity and wide population health inequalities are consistently identified as key factors for poor cancer outcomes in the UK.
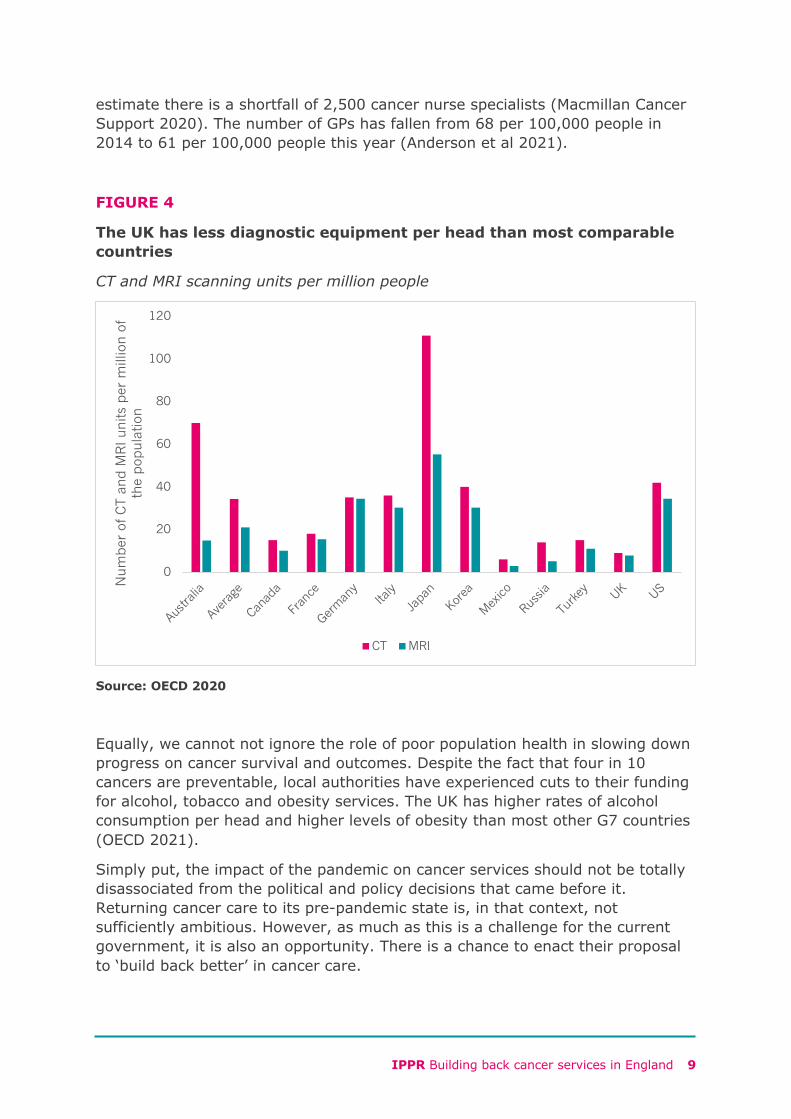
The UK has some of the lowest numbers of CT and MRI scanners per head in the OECD (figure 4). Moreover, workforce shortages are seen across all cancer-related services. Last year, 55 per cent of clinical oncology consultant posts went unfilled (Royal College of Radiologists 2020), while Macmillan Cancer Support
IPPR Building back cancer services in England 9
estimate there is a shortfall of 2,500 cancer nurse specialists (Macmillan Cancer Support 2020). The number of GPs has fallen from 68 per 100,000 people in 2014 to 61 per 100,000 people this year (Anderson et al 2021).
FIGURE 4
The UK has less diagnostic equipment per head than most comparable countries
CT and MRI scanning units per million people
Source: OECD 2020
Equally, we cannot not ignore the role of poor population health in slowing down progress on cancer survival and outcomes. Despite the fact that four in 10 cancers are preventable, local authorities have experienced cuts to their funding for alcohol, tobacco and obesity services. The UK has higher rates of alcohol consumption per head and higher levels of obesity than most other G7 countries (OECD 2021).
Simply put, the impact of the pandemic on cancer services should not be totally disassociated from the political and policy decisions that came before it. Returning cancer care to its pre-pandemic state is, in that context, not sufficiently ambitious. However, as much as this is a challenge for the current government, it is also an opportunity. There is a chance to enact their proposal to ‘build back better’ in cancer care.
0
20
40
60
80
100
120
Australia
Average
Canada
France
Germany
Italy
Japan
Korea
Mexico
Russia
Turkey UK US
Num
ber
of C
T an
d M
RI u
nits
per
mill
ion o
f th
e pop
ula
tion
CT MRI
IPPR Building back cancer services in England 10
POLICY RECOMMENDATIONS
The government recently announced a three-year funding plan for the health service. They have said the funding will allow the NHS to aim for highly ambitious activity increases. The new funding means the NHS budget will continue to grow at a rate similar to that in the NHS Long Term Plan settlement and is only around one half of the amount NHS Providers and NHS Confederation say is required to recover from the pandemic (NHS Confederation 2021). It is difficult to see how the level of funding announced will enable such dramatic activity increases, which is also limited by the size of the workforce and the amount of equipment and physical space in the health service.
There is more to be done to ‘build back batter’ cancer care. To that end, we recommend a new three-part cancer pledge for the country.
1. Build capacity: the government should explore ways to build the right level of capacity in the system in the immediate and medium term to enable increases in service activity. This must include plans to expand the workforce and diagnostic capacity.
2. Harness innovation: without innovation, productivity gains the government is better and aspirations set out in the NHS Long Term Plan will difficult to deliver. Improving uptake of technological advances and re-thinking service design will improve survival outcomes and improve productivity.
3. Better prevention: the government should scale its ambitions on prevention and reduce demands on the health service. This should include new tobacco levy, a junk food tax and a fruit and vegetable subsidy.
The sections below provide constructive proposals enact this plan as the government look to take their next steps.
1. Capacity to recover
Grow and sustain the cancer workforce
Cancer Research UK found that nearly three in four staff surveyed in non-surgical oncology services see staff shortages as a barrier to providing excellent patient experience (Cancer Research UK 2020). In 2018 Health Education England (HEE) set out that, to provide a world-class service for NHS cancer patients, the workforce in seven priority cancer-related professions would likely need to increase by 45 per cent by 2029. Cancer Research UK estimate this will require an additional £142 million to £260 million funding for HEE, which should be taken into account at this year’s comprehensive spending review (ibid).
It will take time to grow the cancer-related workforce, from histopathologists to surgeons, to an adequate level. There are however immediate-term options to expand capacity to accelerate the speed at which backlogs are addressed. A survey by the Royal College of Radiologists estimates the NHS in England is currently short of 189 clinical oncologists, a figure which is set to grow if nothing
IPPR Building back cancer services in England 11
is done. A shortage of oncology consultants is one of the biggest barriers to getting through cancer treatment backlogs. The current pension tax rules perversely discourage some NHS consultants from working additional hours, despite many wanting to. Indeed, some have chosen to retire as a result. The government should review the pension rules to ensure consultants are not being discouraged from working more to help meet cancer backlogs.
In addition to retaining and increasing the number of oncology consultants, the government can take further measures to ensure the broader workforce is retained and supported. IPPR have previously set out recommended the following to maximise NHS workforce retention as Covid-19 fades from pandemic to endemic (Patel and Thomas 2021).
• Recover: it would be unwise to push staff, who are often already working stretched rotas, to increase activity levels. Government and NHS England should instead prioritise staff wellbeing and productivity. This means ensuring staff have access to rest facilities and can take their full annual leave allocations. We recommend annual leave entitlements are guaranteed for the next five years and made transferrable across NHS organisations. We also recommend staff are compensated when annual leave requests are rejected.
• Reward: in line with perception among both the public and the workforce, we previously recommended a 5 per cent average pay rise for NHS staff, tilted in favour of the lower paid.
• Renew: we recommend Health Education England provide a new ‘skills passports’ that would allow skills and abilities to be recognised across the country, increasing the chance workers remain within the NHS if looking for new roles or moving town.
Making diagnostics more resilient
Even before the pandemic, rising waiting times for diagnostic imaging were revealing that diagnostic capacity in the NHS had reached tipping point. This is despite the headline target of the NHS Long Term Plan to improve cancer survival by radically increasing early diagnosis rates. The pandemic has accentuated the diagnostics shortage as infection control procedures have made procedures take longer. It is likely these additional infection control procedures will remain for several years as Covid-19 becomes an endemic disease.
We welcome that last year’s spending review committed £325 million to upgrade outdated diagnostic machinery. But considerably more investment is needed to create the capacity that both Covid-19 and population growth demand. Sir Mike Richards has recommended that CT scanning capacity should be doubled over the next five years. He also recommends that MRI, X-ray and ultrasound scanning equipment should, as a minimum, be expanded in line with growth rates prior to the pandemic. We support these recommendations.
We also recommend Integrated Care Systems (ICSs) consider commissioning mobile diagnostics to expand short-term diagnostic capacity in places with
IPPR Building back cancer services in England 12
especially long backlogs. The most deprived regions of England experienced the greatest number of cancellations and should now receive the greatest investment in recovery (Propper, Stockton and Stoye 2020), otherwise place-based inequalities will be further entrenched. Indeed, while commissioning independent sector diagnostic capacity is likely to be helpful, this is hugely concentrated in the South East of England, and ICSs outside of this region will need to think more creatively. 2. Harnessing innovation to build back better
Making the most of new technologies that improve cancer outcomes and boost productivity
There have been a host of technological innovations in cancer diagnostics and treatment over recent years, from the fast-growing field of genomics, technologies like capsule endoscopy and new therapeutics. Discovery of new cancer therapies have accelerated with technological advances in cancer biology. It remains variable how quickly these become available to patients in England, and policy will need change pace to keep up with the speed of advance. While the UK is a world-leader in genomics research, it remains slow to translate these advances into clinical genomics. There is a considerable gap between the government’s rhetoric on genomics revolutionising health care, and service level implementation that will take time, training and investment to resolve. For cancer care, genomic sequencing can drive big improvements in survival chances by better tailoring treatment regimes to individual tumours. However, at current rates, it can take weeks for oncological samples to be genomically sequenced, leading to delays in patient care. Greater investment across the clinical genomics pathway, including in local hospitals where staff prepare samples to send to genomics laboratory hubs, is needed to make the promise of genomics revolution a reality.
Developments like capsule endoscopy and quantitative faecal immunochemical testing are likely to not only improve gastrointestinal cancer diagnostics but are likely to lead to considerable improvements in service efficiency. Although traditional endoscopy will remain the gold-standard diagnostic test for gastrointestinal cancers, such as stomach and colon cancer, these newer diagnostics could more confidently help rule out cancer in some patients without needing oesophageal or colonic endoscopic procedures. This is pertinent given the pandemic has led to endoscopy backlogs that could take decades to address. Local and national clinical guidelines for suspected gastroenterological cancer
Recommendation: At this year’s comprehensive spending review, we recommend the government provide funding for Health Education England and revise pension tax rules to optimise the size of the oncology consultant workforce. We also recommend significant increases to the Department of Health and Social Care’s capital budget such that Sir Mike Richards’ recommendations to increase diagnostic capacity are afforded.
IPPR Building back cancer services in England 13
should consider incorporating such technologies, when safe and appropriate, to reduce the demand for endoscopy services.
These are disruptive innovations, which will inevitably impact service configurations and patient pathways. IPPR have previously outlined the rationale for better funding the clinical implementation of new technologies and innovations and to support their roll out across the NHS. There are now several such initiatives including the Accelerated Access Collaborative and the Innovative Medicines Fund. We advise the scope of such initiatives is expanded to improve the clinical translation of diagnostic innovations and improve clinical genomics services. Bringing existing initiatives together into a healthcare innovation fund, backed by £2 billion of funding, will create a platform to ‘build back better’ cancer care.
Innovating service pathways
Expanding diagnostic capacity should come alongside re-imagining cancer service delivery. We strongly welcome NHS England’s plan to introduce ‘one stop shop’ community diagnostic hubs, as recommended by Sir Mike Richards. Delivering this lies at the heart of achieving the NHS Long Term Plan’s ambition to diagnose three quarters of all cancers while they are still highly curable by 2028.
As further outlined by NHS Confederation, there are immediate opportunities for the NHS to more directly harness the health on the high street agenda. For example, many high streets around the country have vacant retail space, as competition from online retailers and the continued consequence of Covid-19 on consumer behaviour takes its toll on physical shops. There is a very real opportunity for the NHS to work with local authorities and other partners, in the context of the integrated care agenda, to use this space to set up and deliver community diagnostics. As well as a health benefit, this would benefit the local economy, in line with wider principles of community wealth building.
3. Prevent unnecessary cancers
A ‘polluter pays’ levy on tobacco companies
Tobacco is the leading cause of preventable cancer. The government has ambitiously committed to bring an end to the smoking epidemic by 2030.
Recommendation: Genomics and diagnostic innovations are vital to efforts to ‘build back better’. We recommend this year’s comprehensive spending review announces a healthcare innovation fund for the NHS, to accelerate the implementation of new technologies in healthcare. We also recommend that community diagnostic hubs become bedrock to future healthcare and welcome the NHS’s plans to make this a reality. The community setting should be the mainstay of non-emergency diagnostic investigations.

IPPR Building back cancer services in England 14
To help it achieve that, it should take a ‘polluter pays’ approach that requires tobacco companies to pay the cost of tobacco control. Learning from France and the United States, an annual levy set in legislation could be raised from tobacco companies to fund all tobacco-related regulation activity and smoking services. We support the sector-wide call for a £270 million levy in England on tobacco companies to fund local, regional and national smoking cessation and prevention services.
A fruit and vegetable subsidy and junk food tax
Obesity is a leading cause of many cancers. Many of the policies in the government’s July 2020 obesity strategy will prove helpful in reducing obesity and improving diet. It is fiscal policy, however, that is particularly effective in reducing population obesity levels (Blakely et al 2020). Evidence from the UK’s soft drinks industry levy have revealed the population-wide and progressive health impacts of such policy without it causing harm to industry (Pell et al 2021). Taxing broader food groups, such as the levy on non-essential energy dense foods in Mexico, would lead to more radical population health benefits. That is why the government-commissioned National Food Strategy has recommended a taxing on salt and sugar, which will encourage healthier reformulation of food products, and using some of the revenue generated to subsidise fruit and vegetables. We support this recommendation, which mirrors previous IPPR calls to tax non-essential foods and subsidise the cost of healthy foods for low-income families.
Recommendation: We recommend the government makes better use of fiscal policy to improve population health, reduce inequalities and prevent common diseases like cancer. We recommend a broadening the base of food taxes and a ‘polluter pays’ tobacco levy, with proceeds subsidising healthy foods and funding tobacco control services.

IPPR Building back cancer services in England 15
REFERENCES
Anderson, M. et al. (2021) ‘Securing a sustainable and fit-for-purpose UK health and care workforce’, The Lancet, 397(10288), pp. 1992–2011. doi:10.1016/S0140-6736(21)00231-2.
Arnold, M. et al. (2019) ‘Progress in cancer survival, mortality, and incidence in seven high-income countries 1995–2014 (ICBP SURVMARK-2): a population-based study’, The Lancet Oncology, 20(11), pp. 1493–1505. doi:10.1016/S1470-2045(19)30456-5.
Blakely, T. et al. (2020) ‘The effect of food taxes and subsidies on population health and health costs: a modelling study’, The Lancet Public Health, 5(7), pp. e404–e413. doi:10.1016/S2468-2667(20)30116-X.
Cancer Research UK (2020) Estimating the cost of growing the NHS cancer workforce in England by 2029. Available at: https://www.rand.org/randeurope/research/projects/estimating-the-cost-of-growing-the-nhs-cancer-workforce-in-engla.html (Accessed: 2 September 2021).
Hanna, T.P. et al. (2020) ‘Mortality due to cancer treatment delay: systematic review and meta-analysis’, BMJ, 371, p. m4087. doi:10.1136/bmj.m4087.
Macmillan Cancer Support (2020) Addressing the gap. Available at: https://www.macmillan.org.uk/about-us/what-we-do/we-make-change-happen/we-shape-policy/workforce.html (Accessed: 2 September 2021).
NHS Confederation (2021) Patients in peril as NHS future funding finalised | NHS Confederation. Available at: https://www.nhsconfed.org/news/patients-peril-nhs-future-funding-finalised (Accessed: 22 September 2021).
Patel, P. and Thomas, C. (2021) Recover, Reward, Renew: A post-pandemic plan for the healthcare workforce, IPPR. Available at: https://www.ippr.org/research/publications/recover-reward-renew (Accessed: 10 August 2021).
Patel, P., Thomas, C. and Quilter-Pinner, H. (2021) State of health and care: The NHS Long Term Plan after Covid-19. Available at: https://www.ippr.org/research/publications/state-of-health-and-care (Accessed: 24 March 2021).
Pell, D. et al. (2021) ‘Changes in soft drinks purchased by British households associated with the UK soft drinks industry levy: controlled interrupted time series analysis’, BMJ, 372, p. n254. doi:10.1136/bmj.n254.
The Royal College of Radiologists (2020) Oncology workforce census. Available at: https://www.rcr.ac.uk/press-and-policy/policy-priorities/workforce/oncology-workforce-census (Accessed: 2 September 2021).
IPPR Building back cancer services in England 16
Thomas, C. (2020) Resilient health and care: Learning the lessons of Covid-19, IPPR. Available at: https://www.ippr.org/research/publications/resilient-health-and-care (Accessed: 24 January 2021).
ABOUT IPPR IPPR, the Institute for Public Policy Research, is the UK’s leading progressive think tank. We are an independent charitable organisation with our main office in London. IPPR North, IPPR’s dedicated think tank for the north of England, operates out of offices in Manchester and Newcastle, and IPPR Scotland, our dedicated think tank for Scotland, is based in Edinburgh.
Our primary purpose is to conduct and promote research into, and the education of the public in, the economic, social and political sciences, science and technology, the voluntary sector and social enterprise, public services, and industry and commerce. Other purposes include to advance physical and mental health, the efficiency of public services and environmental protection or improvement; and to relieve poverty, unemployment, or those in need by reason of youth, age, ill-health, disability, financial hardship, or other disadvantage.
Registered charity no: 800065 (England and Wales), SC046557 (Scotland)
This paper was first published in September 2021. © IPPR 2021
The contents and opinions expressed in this paper are those of the authors only.