Embed Size (px)
Citation preview

*For correspondence: gc.island@
gmail.compollybrandon@mac.
com
Competing interests: The
authors declare that no
competing interests exist.
Received: 14 August 2016
Accepted: 16 August 2016
Published: 09 January 2017
This article is Open Access:
https://
creativecommons.org/licenses/
by/4.0/)
s BJGP Open 2017;
DOI:10.3399/
bjgpopen17X100557
Primary care in the Calais JungleGerry Clare, BSc, MSc, PhD, FRCOphth
1*, Polly Nyiri, MBBChir, DTM&H, MA International Health2*
1Consultant ophthalmologist, Western Eye Hospital, London, UK; 2GP, HealthInclusion Clinic, Guy’s and St Thomas’ Hospital NHS Foundation Trust, London, UK
IntroductionLast summer our small medical team visited the Calais ’Jungle’. Since that time much has changed
and the camp is being demolished and by the time this article is read, it will probably be long gone.
Some youngsters are finally being brought to the UK under the ’Dubs’ amendment. However, once
this camp is cleared it will not solve the ongoing flight of refugees from war torn areas: other camps
are already appearing.
July 2016A young Afghan man caught his finger on a sharp point while trying to cross a barbed wire fence.
The finger was partially degloved. He attended the local hospital, where they placed a few sutures,
but now, 2 weeks later, the skin is necrotic and the underlying tissue looks infected. He is in danger
of losing his finger.
A middle-aged Sudanese man has been having rigors and is generally unwell. He says it is similar
to when he last had malaria.
A young Ukrainian woman complains of lower back pain and urinary frequency.
The paths of these three people may never have crossed; yet here they are, denizens of the Calais
Jungle. They turn up to a makeshift primary care ‘clinic’ that we set up in the heart of the unofficial
refugee camp one weekend in July 2016.
With only basic medical supplies, we are immediately challenged by what we see. How can we
arrange secondary care for the young Afghan in danger of losing his finger? We try to persuade him
to return to the original local hospital, but he is reluctant. It was not a good experience for him the
first time round.
With the other two patients, it is easier. They can attend the Salam clinic run by a local association
during weekdays. Later, we receive word that malaria has been confirmed in our Sudanese patient.
More people arrive, presenting with scabies, rat bites, tinea, chest infections, and wheezing from
inhaling smoke from fires lit to cook and keep warm in their tents at night. We examine a severely
malnourished 2-year-old boy. We meet several of the camp’s 600 unaccompanied children, at grave
risk of sexual exploitation. We learn that there is inadequate safeguarding in place to protect them.
A young Eritrean man comes in worried about his eye. He has sustained direct ocular trauma from a
rubber bullet, and will never see normally again out of that eye. We see haematomas from police
batons, and hear about children being exposed to tear gas again and again (Figure 1).
The realityThese are no ordinary patients. They have travelled far from home to escape war, poverty, and mis-
ery. They have endured personal odysseys to get here, experienced untold hardships, and suffered
unimaginable privations. Many have survived the loss of their families, torture, and rape. Their jour-
neys over, for the moment at least, they must make their homes in the Calais Jungle. Their new shel-
ters are in many cases mere tarpaulin covers, and their new beds just rugs on the ground. They own
next to nothing. There is little for them to do, besides use their ingenuity to cross the English Chan-
nel in search of a better life. They are vulnerable to exploitation, crime, injury, and disease. Poten-
tially violent clashes with local police, with other ethnic groups resident in the Jungle, or local far
Clare G and Nyiri P. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100557 1 of 5
PRACTICE & POLICY
CC BY license (
*For correspondence: egalam@
hotmail.com
Competing interests: The
authors declare that no
competing interests exist.
26 November 2016
Accepted: 29 November 2016
Author Keywords: burnout,
trainees, general practice,
empathy, coping
DOI:10.3399/
bjgpopen17X100773
’Intern life’: a longitudinal study ofburnout, empathy, and coping strategiesused by French GPs in trainingEric Galam, PhD1*, Camille Vauloup Soupault, MD2, Lucie Bunge, MD3,Celine Buffel du Vaure, MD2, Emilie Boujut4, Philippe Jaury, PhD2,5
1GP, Departement de Medecine Generale, Faculte de Medecine, Universite ParisDiderot, Sorbonne Paris Cite, Paris, France; 2GP, Departement de MedecineGenerale, Universite Paris Descartes, Sorbonne Paris Cite, Faculte de Medecine,Paris, France; 3GP, Departement de Medecine Generale, Universite Paris Diderot,Sorbonne Paris Cite, Faculte de Medecine, Paris, France; 4Psychologist, Institute ofPsychology, Paris Descartes University, Paris, France; 5GP, Institut of Psychology,Paris Descartes University, Paris, France
AbstractBackground: More than half of French medical GP trainees (GPTs) suffer from burnout.
Aim: To define and follow the evolution of risk factors, such as empathy and coping strategies,
associated with burnout in this population.
Design & setting: Prospective longitudinal study involving volunteers of 577 Parisian university
GPTs in 2012.
Method: Self-reported anonymous online questionnaires were sent three times every 6 months to
all participants. Stress was measured using the Intern-Life scale and burnout using the Maslach
Inventory, and anxiety and depression measured using the Hospital Anxiety and Depression Scale
(HADS). Sociodemographic, professional, and personal data, including coping strategies and
measures of empathy were also collected.
Results: In total 343 questionnaires were fully completed at baseline (T0): 304 were usable at
baseline, 169 were usable at 6 months (T1) and 174 at 1 year (T2). Stress rates decreased sharply
between T1 (scores 42.96) and T2 (17.08), while scores for burnout remained relatively stable: more
than 13% of GPTs had high scores in all three dimensions of burnout. Depersonalisation increased
from 61% (T1) to 66% (T2). One hundred and four paired samples were analysed between T0 and
T1, and between T1 and T2. Emotion-centred coping was associated with emotional exhaustion
(P<0.05), while professional support reduced it. Experiences of aggression increased
depersonalisation (P<0.05). Social support, problem-centred coping, perspective-taking empathy,
and professional support improved the sense of personal accomplishment (P<0.05).
Conclusion: Tools to help GPTs are available but are underused. More training in doctor–patient
relationships and understanding of medical hidden curricula are necessary to decrease burnout
among GPTs and improve their wellbeing and patient care.
How this fits inBurnout is described with increasing frequency among French doctors and trainees, especially
among GPs.
The links between empathy and professional characteristics have been studied in France among
GPs and GPTs but no longitudinal study has ever been conducted.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 1 of 12
RESEARCH
*For correspondence: egalam@
hotmail.com
Competing interests: The
authors declare that no
competing interests exist.
Accepted: 29 November 2016
14 June 2017
Author Keywords: burnout,
trainees, general practice,
empathy, coping
s BJGP Open 2017;
DOI:10.3399/
bjgpopen17X100773
’Intern life’: a longitudinal study ofburnout, empathy, and coping strategiesused by French GPs in trainingEric Galam, PhD1*, Camille Vauloup Soupault, MD2, Lucie Bunge, MD3,Celine Buffel du Vaure, MD2, Emilie Boujut4, Philippe Jaury, PhD2,5
1GP, Departement de Medecine Generale, Faculte de Medecine, Universite ParisDiderot, Sorbonne Paris Cite, Paris, France; 2GP, Departement de MedecineGenerale, Universite Paris Descartes, Sorbonne Paris Cite, Faculte de Medecine,Paris, France; 3GP, Departement de Medecine Generale, Universite Paris Diderot,Sorbonne Paris Cite, Faculte de Medecine, Paris, France; 4Psychologist, Institute ofPsychology, Paris Descartes University, Paris, France; 5GP, Institut of Psychology,Paris Descartes University, Paris, France
AbstractBackground: More than half of French medical GP trainees (GPTs) suffer from burnout.
Aim: To define and follow the evolution of risk factors, such as empathy and coping strategies,
associated with burnout in this population.
Design & setting: Prospective longitudinal study involving volunteers of 577 Parisian university
GPTs in 2012.
Method: Self-reported anonymous online questionnaires were sent three times every 6 months to
all participants. Stress was measured using the Intern-Life scale and burnout using the Maslach
Inventory, and anxiety and depression measured using the Hospital Anxiety and Depression Scale
(HADS). Sociodemographic, professional, and personal data, including coping strategies and
measures of empathy were also collected.
Results: In total 343 questionnaires were fully completed at baseline (T0): 304 were usable at
baseline, 169 were usable at 6 months (T1) and 174 at 1 year (T2). Stress rates decreased sharply
between T1 (scores 42.96) and T2 (17.08), while scores for burnout remained relatively stable: more
than 13% of GPTs had high scores in all three dimensions of burnout. Depersonalisation increased
from 61% (T1) to 66% (T2). One hundred and four paired samples were analysed between T0 and
T1, and between T1 and T2. Emotion-centred coping was associated with emotional exhaustion
(P<0.05), while professional support reduced it. Experiences of aggression increased
depersonalisation (P<0.05). Social support, problem-centred coping, perspective-taking empathy,
and professional support improved the sense of personal accomplishment (P<0.05).
Conclusion: Tools to help GPTs are available but are underused. More training in doctor–patient
relationships and understanding of medical hidden curricula are necessary to decrease burnout
among GPTs and improve their wellbeing and patient care.
How this fits inBurnout is described with increasing frequency among French doctors and trainees, especially
among GPs.
The links between empathy and professional characteristics have been studied in France among
GPs and GPTs but no longitudinal study has ever been conducted.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 1 of 12
RESEARCH
*For correspondence: egalam@
hotmail.com
Competing interests: The
authors declare that no
competing interests exist.
Accepted: 29 November 2016
14 June 2017
Author Keywords: burnout,
trainees, general practice,
empathy, coping
s BJGP Open 2017;
DOI:10.3399/
bjgpopen17X100773
’Intern life’: a longitudinal study ofburnout, empathy, and coping strategiesused by French GPs in trainingEric Galam, PhD1*, Camille Vauloup Soupault, MD2, Lucie Bunge, MD3,Celine Buffel du Vaure, MD2, Emilie Boujut4, Philippe Jaury, PhD2,5
1GP, Departement de Medecine Generale, Faculte de Medecine, Universite ParisDiderot, Sorbonne Paris Cite, Paris, France; 2GP, Departement de MedecineGenerale, Universite Paris Descartes, Sorbonne Paris Cite, Faculte de Medecine,Paris, France; 3GP, Departement de Medecine Generale, Universite Paris Diderot,Sorbonne Paris Cite, Faculte de Medecine, Paris, France; 4Psychologist, Institute ofPsychology, Paris Descartes University, Paris, France; 5GP, Institut of Psychology,Paris Descartes University, Paris, France
AbstractBackground: More than half of French medical GP trainees (GPTs) suffer from burnout.
Aim: To define and follow the evolution of risk factors, such as empathy and coping strategies,
associated with burnout in this population.
Design & setting: Prospective longitudinal study involving volunteers of 577 Parisian university
GPTs in 2012.
Method: Self-reported anonymous online questionnaires were sent three times every 6 months to
all participants. Stress was measured using the Intern-Life scale and burnout using the Maslach
Inventory, and anxiety and depression measured using the Hospital Anxiety and Depression Scale
(HADS). Sociodemographic, professional, and personal data, including coping strategies and
measures of empathy were also collected.
Results: In total 343 questionnaires were fully completed at baseline (T0): 304 were usable at
baseline, 169 were usable at 6 months (T1) and 174 at 1 year (T2). Stress rates decreased sharply
between T1 (scores 42.96) and T2 (17.08), while scores for burnout remained relatively stable: more
than 13% of GPTs had high scores in all three dimensions of burnout. Depersonalisation increased
from 61% (T1) to 66% (T2). One hundred and four paired samples were analysed between T0 and
T1, and between T1 and T2. Emotion-centred coping was associated with emotional exhaustion
(P<0.05), while professional support reduced it. Experiences of aggression increased
depersonalisation (P<0.05). Social support, problem-centred coping, perspective-taking empathy,
and professional support improved the sense of personal accomplishment (P<0.05).
Conclusion: Tools to help GPTs are available but are underused. More training in doctor–patient
relationships and understanding of medical hidden curricula are necessary to decrease burnout
among GPTs and improve their wellbeing and patient care.
How this fits inBurnout is described with increasing frequency among French doctors and trainees, especially
among GPs.
The links between empathy and professional characteristics have been studied in France among
GPs and GPTs but no longitudinal study has ever been conducted.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 1 of 12
RESEARCH
*For correspondence: egalam@
hotmail.com
Competing interests: The
authors declare that no
competing interests exist.
Accepted: 29 November 2016
Author Keywords: burnout,
trainees, general practice,
empathy, coping
s BJGP Open 2017;
DOI:10.3399/
bjgpopen17X100773
’Intern life’: a longitudinal study ofburnout, empathy, and coping strategiesused by French GPs in trainingEric Galam, PhD1*, Camille Vauloup Soupault, MD2, Lucie Bunge, MD3,Celine Buffel du Vaure, MD2, Emilie Boujut4, Philippe Jaury, PhD2,5
1GP, Departement de Medecine Generale, Faculte de Medecine, Universite ParisDiderot, Sorbonne Paris Cite, Paris, France; 2GP, Departement de MedecineGenerale, Universite Paris Descartes, Sorbonne Paris Cite, Faculte de Medecine,Paris, France; 3GP, Departement de Medecine Generale, Universite Paris Diderot,Sorbonne Paris Cite, Faculte de Medecine, Paris, France; 4Psychologist, Institute ofPsychology, Paris Descartes University, Paris, France; 5GP, Institut of Psychology,Paris Descartes University, Paris, France
AbstractBackground: More than half of French medical GP trainees (GPTs) suffer from burnout.
Aim: To define and follow the evolution of risk factors, such as empathy and coping strategies,
associated with burnout in this population.
Design & setting: Prospective longitudinal study involving volunteers of 577 Parisian university
GPTs in 2012.
Method: Self-reported anonymous online questionnaires were sent three times every 6 months to
all participants. Stress was measured using the Intern-Life scale and burnout using the Maslach
Inventory, and anxiety and depression measured using the Hospital Anxiety and Depression Scale
(HADS). Sociodemographic, professional, and personal data, including coping strategies and
measures of empathy were also collected.
Results: In total 343 questionnaires were fully completed at baseline (T0): 304 were usable at
baseline, 169 were usable at 6 months (T1) and 174 at 1 year (T2). Stress rates decreased sharply
between T1 (scores 42.96) and T2 (17.08), while scores for burnout remained relatively stable: more
than 13% of GPTs had high scores in all three dimensions of burnout. Depersonalisation increased
from 61% (T1) to 66% (T2). One hundred and four paired samples were analysed between T0 and
T1, and between T1 and T2. Emotion-centred coping was associated with emotional exhaustion
(P<0.05), while professional support reduced it. Experiences of aggression increased
depersonalisation (P<0.05). Social support, problem-centred coping, perspective-taking empathy,
and professional support improved the sense of personal accomplishment (P<0.05).
Conclusion: Tools to help GPTs are available but are underused. More training in doctor–patient
relationships and understanding of medical hidden curricula are necessary to decrease burnout
among GPTs and improve their wellbeing and patient care.
How this fits inBurnout is described with increasing frequency among French doctors and trainees, especially
among GPs.
The links between empathy and professional characteristics have been studied in France among
GPs and GPTs but no longitudinal study has ever been conducted.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 1 of 12
RESEARCH
*For correspondence: egalam@
hotmail.com
Competing interests: The
authors declare that no
competing interests exist.
Received: 26 November 2016
Accepted: 29 November 2016
Published: 14 June 2017
Author Keywords: burnout,
empathy, coping
s
DOI:10.3399/
bjgpopen17X100773
’Intern life’: a longitudinal study ofburnout, empathy, and coping strategiesused by French GPs in trainingEric Galam, PhD1*, Camille Vauloup Soupault, MD2, Lucie Bunge, MD3,Celine Buffel du Vaure, MD2, Emilie Boujut4, Philippe Jaury, PhD2,5
1GP, Departement de Medecine Generale, Faculte de Medecine, Universite ParisDiderot, Sorbonne Paris Cite, Paris, France; 2GP, Departement de MedecineGenerale, Universite Paris Descartes, Sorbonne Paris Cite, Faculte de Medecine,Paris, France; 3GP, Departement de Medecine Generale, Universite Paris Diderot,Sorbonne Paris Cite, Faculte de Medecine, Paris, France; 4Psychologist, Institute ofPsychology, Paris Descartes University, Paris, France; 5GP, Institut of Psychology,Paris Descartes University, Paris, France
AbstractBackground: More than half of French medical GP trainees (GPTs) suffer from burnout.
Aim: To define and follow the evolution of risk factors, such as empathy and coping strategies,
associated with burnout in this population.
Design & setting: Prospective longitudinal study involving volunteers of 577 Parisian university
GPTs in 2012.
Method: Self-reported anonymous online questionnaires were sent three times every 6 months to
all participants. Stress was measured using the Intern-Life scale and burnout using the Maslach
Inventory, and anxiety and depression measured using the Hospital Anxiety and Depression Scale
(HADS). Sociodemographic, professional, and personal data, including coping strategies and
measures of empathy were also collected.
Results: In total 343 questionnaires were fully completed at baseline (T0): 304 were usable at
baseline, 169 were usable at 6 months (T1) and 174 at 1 year (T2). Stress rates decreased sharply
between T1 (scores 42.96) and T2 (17.08), while scores for burnout remained relatively stable: more
than 13% of GPTs had high scores in all three dimensions of burnout. Depersonalisation increased
from 61% (T1) to 66% (T2). One hundred and four paired samples were analysed between T0 and
T1, and between T1 and T2. Emotion-centred coping was associated with emotional exhaustion
(P<0.05), while professional support reduced it. Experiences of aggression increased
depersonalisation (P<0.05). Social support, problem-centred coping, perspective-taking empathy,
and professional support improved the sense of personal accomplishment (P<0.05).
Conclusion: Tools to help GPTs are available but are underused. More training in doctor–patient
relationships and understanding of medical hidden curricula are necessary to decrease burnout
among GPTs and improve their wellbeing and patient care.
How this fits inBurnout is described with increasing frequency among French doctors and trainees, especially
among GPs.
The links between empathy and professional characteristics have been studied in France among
GPs and GPTs but no longitudinal study has ever been conducted.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 1 of 12
RESEARCH
Copyright © The Authors 2017;

This is the first French longitudinal study of GPTs over their first year in training, and confirms a
high prevalence of burnout, as well as the increasing depersonalisation of doctors and the impor-
tance of some risk factors including ways of coping as a caregiver and of being empathic to patients,
and the impact of the hidden medical curriculum.
IntroductionAccording to Maslach and Leiter:1
’... burnout is a psychological syndrome emerging as a prolonged response to chronic
interpersonal stressors on the job. The three key dimensions of this response are an
overwhelming exhaustion, feelings of cynicism and detachment from the job, accompanied by a
sense of ineffectiveness and lack of accomplishment. The significance of this three-dimensional
model is that it clearly places the individual stress experience within a social context and
involves the person’s conception of both self and others.’
Widely described in the medical world, burnout is frequent among French GPs, and other doc-
tors.2–5 It is also frequent among medical trainees in general practices (GPTs).6–9 Its consequences
can be dramatic10 and its causes complex.11–16 Several multifactorial explanations have been pro-
posed, including links with stress,17–20 depression,21 sleep deprivation,22 and medical error.2,23
Three aspects of this problem are particularly important. First, ways of understanding others
through empathy,24–27 which reflects the ability of the caregiver to understand the point of view of
his or her client. Secondly, managing one’s own problems by coping,17,28–29 which is the ability to
overcome the impact of an event perceived as threatening. It can be based on three categories of
strategy centred on a) the problem, b) the seeking of social support, and c) the emotions entailed.
Third, the ’hidden curriculum’,30 which acknowledges that medical education is more than the simple
transmission of knowledge and skills; it is also a process of ’socialisation’, including norms and values
about how to be a good doctor. The main objective of this study was to explore possible predictors
in the evolution of burnout among Parisian GPTs during their first year internship, and to assess their
correlation to empathy and coping, and to highlight the role of the hidden curriculum (Box 1).31
Method
Participants and settingThis work is a part of the ’Intern life study’, a 3-year follow-up study of a cohort of Parisian GPTs,
which started in October 2012.
Box 1. French GP training course
After 6 years of medical studies, each French medical trainee has to choose a specialisation. A
French medical student studies 3 years to specialise as a GP. This includes, at least:
. 200 hours of theoretical coursework.
. Six practical courses of 6 months in medical settings including one in an outpatient generalmedicine setting, one in emergency, one in internal medicine and one in gynecology orpaediatrics, and two other specialties of the trainee’s choice. GPTs have a biannual meetingto choose their next 6-month placement. GP trainees were offered participation in thisstudy at these meetings.
. Proof of learning as evidenced by written stories anecdotes of an experience as apractitioner including their analysis of authentic clinical situations.
. Thesis on a topic for a GP.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 2 of 12
Research

Participants were all general practice residents in their first year training. There were no exclusion
criteria. The study was presented by GPTs during their first meeting where residents-in-training
choose the topic and location of internship every 6 months. Five gifts were drawn (free cinema tick-
ets) to encourage participation. Anonymous online questionnaires were sent with reminders to par-
ticipants at three different times: at baseline (T0), after 6 months (T1), and after 1 year (T2). A free
telephone number was provided to help GPTs seeking help for themselves if necessary.
MeasuresThis study collected extensive longitudinal data on the GPTs, some of which is reported else-
where.32–34 The results presented here are about burnout and empathy, at the T0 timepoint (base-
line), T1 (6 months) and T2 (October 2013).
Before use, the questionnaire (available from authors on request) was tested on three GPTs. It
contained 53 questions and took 20 minutes to complete. In addition to demographic, work, envi-
ronmental, and behavioural data, it explored levels of burnout, depression, stress, and transactional
variables such as coping strategies and clinical empathy toward patients.
The following validated questionnaires were used:
. burnout measured by the Maslach Burn-out Inventory (MBI);1
. empathy by the Jefferson Physician Empathy Scale (JSPE scale);35
. coping strategies by the Ways of Coping Checklist-Revised Questionnaire (WCC-R);36
. stress by a specific stress questionnaire for GPTs developed and validated by the qualitativepart of the ’Intern-life’ study;37
. anxiety and depression by the HADS;38 and
. other variables: doctor–patient training, professional support, current training, workload,aggression towards the doctor and conscientiousness.
Statistical analysisDescriptive univariate analyses were complemented by bivariate analysis using Spearman and Pear-
son tests between burnout dimensions and quantitative variables. Qualitative variables were
explored using Student t tests. The variables associated in the first part of the study with P<0.01
were selected for multivariate analysis by logistic regression.
Analyses on paired samples were conducted, averaging the scores by a same participant at T0
and T1, and then at T1 and T2. Student t tests were used to compare the average of repeated meas-
urements to track the evolution over time of burnout and other variables. The effect of variables on
the three dimensions of burnout were compared by analysis of variance for repeated measures
(ANOVA). A P-value of <0.05 was considered significant. Statistical tests were performed with the
SPSS 17.0 software.
Results
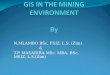
Population characteristicsAmong all 577 Parisian GPTs starting their internship, 304 questionnaires were complete and usable
at T0 (response rate: 52.6%), 169 (29.3%) at T1, and 174 (30.2%) at T2. At the three time points, an
average of 76.1% of GPTs were female, with an average age of 25.4 years (range 22–43 years). See
Table 1 and Figure 1.
Univariate analysis at T1 and T2Burnout scoresAt T1, 61% had at least one dimension of high burnout and more than 13% had high scores in the
three dimensions. At T2, these figures remained almost stable at 66% (one dimension) and 13%
(three high dimensions). Emotional exhaustion rates were 46% at T1 and 47% at T2. Depersonalisa-
tion rate was 61% at T1 and 66% at T2; and low personal accomplishment rates were 34% at T1 and
35% at T2 (Table 2).
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 3 of 12
Research

EmpathyA T1 and T2, the three dimensions of empathy were distributed similarly across the study population
(Table 3).
AnxietyAt T1, the average anxiety score was 11.21 (standard deviation [SD] 2.38) showing anxiety for more
than 50% of GPTs (197 responders). It remained stable at T2 with a score of 11.02 (SD 2.183).
Table 1. Population at the three study times
T0 (n = 304) beforestarting course
T1 (n = 169) after6 months
T2 (n = 174) after12 months
n (%) n (%) n (%)
Demographics
Female 258 (75.2) 166 (77.2) 158 (76.0)
Male 85 (24.8) 49 (22.8) 50 (24.0)
Living alone 167 (48.7) 99 (46.0) 79 (38.0)
Location of rotation
Accident & Emergency 87 (40.5) 97 (46.6)
Internal medicine 102 (47.4) 88 (42.3)
Paediatrics 9 (4.2) 8 (3.8)
Gynaecology 3 (1.4) 2 (1.0)
Private GP practice 1 (0.5) 8 (3.8)
Free course 13 (6.0) 5 (2.4)
Job characteristics
Satisfaction rating course, 1–10 7 (1.9) 7 (1.7)
Working hours per week, n 56 (16.9) 59 (38.4)
Duty nights per month, n 3 (2.0) 3 (2.2)
Free weekends per month, n 2 (1.1) 2 (0.8)
Free weeks per 6 month course, n 2 (0.9) 4 (0.9)
Transport time per day, minutes 88 (51.5) 84 (45.2)
Professional experiences
Moral harrassment 11 (5.1) 16 (7.7)
Sexual harrassment 3 (1.4) 5 (2.4)
Conscientiousness-hitting 138 (64.2) 128 (61.5)
Aggression 74 (34.4) 89 (42.8)
Clinical part of work 169 (64.2) 174 (64.5)
Administrative part of work 169 (27.7) 174 (28.3)
Professional support 176 (81.6) 177 (85.1)
Doctor–patient relationship training 151 (70.2) 75 (36.1)
Predominance of informal trainingcompared to formal training
191 (91.0) 189 (94.0)
Positive scientific role-modeling doctors 196 (93.3) 193 (96.0)
Compassionate role-modeling doctors 199 (94.8) 184 (91.5)
Negative scientific role-modeling doctors 147 (70.0) 146 (72.6)
Non-compassionate role-modelingdoctors
159 (75.7) 145 (72.1)
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 4 of 12
Research

DepressionAt T1, the average depression score was 8.18 (SD
1.649): most GPTs had no evidence of depression
scores. It remained stable at T2 with 8.39 (SD
1.684).
Coping strategiesAt T1 and T2, the three coping strategies were
distributed similarly across the population
(Table 3).
StressA T1, GPTs had an average stress score of 42.96
with a median of 44 and an SD of 9.58 for 169
responders. At T2, the stress rate was much
lower at 17.08 (SD = 4.05) for 174 responders.
Bivariate cross-sectional analysisA T1, emotion-centred coping strategies
appeared to be positively associated with the
three burnout dimensions.
At T1 and T2, being assaulted had a significant
impact on emotional exhaustion and depersonali-
sation (P<0.01). Conscientiousness was correlated
with depersonalisation at T1 and with emotional
exhausation at T2.
At T1 and T2, GPTs who had received training on doctor–patient relationships were less likely to
experience emotional exhaustion (Box 2).
Multivariate cross-sectional analysisFactors associated with emotional exhaustionStress at T1 (odds ratio [OR] 1.07; 95% confidence interval [CI] = 1.02 to 1.13) and at T2 (OR 1.2;
95% CI = 1.03 to 1.32), emotion-centred coping (OR 1.1; 95% CI =1.01 to 1.22) at T1 and at T2 (OR
1.14; 95% CI = 1.05 to 1.23) were statistically associated with emotional exhaustion.
At T1, there was also an association with anxiety (OR 1.3; 95% CI = 1.15 to 1.41) and at T2 with
’conscientiousness-hitting’ — that is, being unable to live up to one’s personal values — (OR 1.34;
95% CI = 1.15 to 1.79).
At T1 and T2, no significant impact was found with the number of working hours, satisfaction with
the course, professional support, doctor–patient training, and aggression towards the doctor.
Figure 1. Flowchart of the study.
Number of GPTs at each time.
n = number of answers.
u = number of utilisable questionnaires.
Table 2. Burnout scores
T1, % T2, %
Three high scores 14 13
Two high scores 17 13
One high score 30 40
No high score 39 34
High emotional exhaustion 46 47
High depersonalisation 61 66
Low personal accomplishment 34 35
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 5 of 12
Research

Factors associated with depersonalisationNo variable was significantly associated with depersonalisation at T1 or T2.
Factors associated with low personal accomplishmentStrong emotion-centred coping rate was associated with low personal accomplishment (OR 1.11;
95% CI = 1.01 to 1.22) at T1 and at T2. Conversely, a high problem-centred coping rate (OR 0.86;
95% CI = 0.77 to 0.96) and taking perspective empathy (OR 0.92; 95% CI = 0.86 to 0.98) were asso-
ciated with a high rate of personal accomplishment).
Table 3. Empathy and coping strategies at T1 and T2
Mean Median Standard Deviation
T1 T2 T1 T2 T1 T2
Empathy n = 197 n = 197
Taking perspective 50.3 51.9 50 52 7.9 7.9
Compassionnate care 43.7 43.5 44 44 5.8 6.1
Put in the patient’s place(seeing things from the patient’s point of view)
9.8 10.1 10 10 2.4 2.3
Coping n = 172 n = 179
Problem centred 26.7 27.6 27 28 6.4 6.4
Support centred 20.8 21.7 21 22 4.6 4.4
Emotion centred 21.7 21.9 22 22 6.4 5.8
Box 2. Main results on paired samples n = 104 (for the same persons at two different points)
Transversal analysis Longitudinal analysis
Positive correlations Negative correlations Positivecorrelations
Negative correlations
Emotional empathy No correlation . Stress (T1 and T2). Emotion-centred copinga (T1,
T2). Anxiety (T1). Moral harrassment (T2). Conscience-hitting (T2)
Professionalsupport
. Stress
. Emotion-centredcopinga
Depersonalisation No correlation No correlation No correlation Aggression
Low personalaccomplishment
Emotion-centred coping(T1, T2)
. Problem-centred copinga (T1,T2)
. Taking perspective empathy(T1, T2)a
. Dining out (T1 and T2)
. Social-support centredcoping
. Problem-centredcopinga
. Taking perspectiveempathya
. Professional support
aCorrelations found in all study analysis.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 6 of 12
Research

Longitudinal analysis of paired samplesAverage comparison testAmong the 104 analysed subjects, significant changes for a particular person across two time points
(T0 and T1, and T1 and T2) were:
. three dimensions of burnout increased significantly (P<0.01);
. taking perspective empathy decreased (P = 0.06);
. leisure and clinical (compassionate) empathy decreased significantly P = 0.027 (leisure) P =0.016 (empathy); and
. anxiety increased (P<0.01)
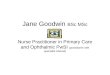
Analysis of variance of repeated measures (ANOVA)An increase in emotional exhaustion (Figure 2) was associated with emotion-centred coping
(P<0.01) and stress (P = 0.02). A decrease in emotional exhaustion was associated with professional
support (P<0.01). An increase in depersonalisation was associated with being assaulted (P = 0.02).
An increase in personal accomplishment was associated with problem-centred coping (P = 0.05),
social-support centred coping (P<0.001), empathy (P<0.0041), and professional support (P<0.0304).
Discussion
SummaryThis is the first major longitudinal study to define and follow the evolution of risk factors, inclusion
empathy and coping strategies, associated with burnout in French GP trainees. Positive findings
included stress rates decreasing sharply during the study period and overall low scores for anxiety
and depression on the HADS. However, levels of burnout, particularly depersonalisation, were high.
In paired, within-subject analyses, emotion-centred coping strategies contributed to, and profes-
sional support protected against, emotional exhaustion. Aggressiveness towards doctors increased
feelings of depersonalisation. Trainees’ sense of personal accomplishment improved through social
support, problem-centred coping, empathy and professional support.
Strengths and limitationsThere have been no other longitudinal studies on burnout in French GPTs. The entire questionnaire
used validated tools and in addition to individual and professional risk factors, interpersonal factors
were explored.
This study has a few limitations. There was a selection bias: the average age and personal status
of GPTs in the current study are similar to other French studies,6,9,39 and the participants are all liv-
ing in the Paris region. Therefore, it is difficult to generalise these findings to all French GPTs. Also,
the questionnaire was self-completed via the internet, and did not allow for the control of the
amount of time for completion or the assurance that only one questionnaire was filled out per
participant.
There was also a measurement bias: there are many definitions of burnout and although the MBI
is validated and widely used, allowing for comparisons with other findings, it does not distinguish
between formal, potential, or obvious burnout. This study looked for factors associated with the
severe stages of each of the three dimensions of burnout and did not integrate moderate scores,
which are regarded as pathological by some authors. The method of self-questionnaire necessarily
produced subjective responses and may be influenced by social desirability bias or modesty. Finally,
grids, whatever their validity criteria, are all reductive, especially when they explore experience in a
declarative way.
Comparison with existing literatureAlmost 32% of all GPTs participated in this study at T1 and T2. It decreased from the beginning rate
(T0) but it is of note that participants at T0 had not yet begun their training. This rate is lower than
comparable studies on GP or GPT burnout where rates are >60%.6,8 However, it is important to
note that the questionnaire took 20 minutes to complete and was required to be repeated three
times.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 7 of 12
Research

Figure 2. Evolution of correlations during the study for 104 paired samples.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 8 of 12
Research

The burnout scores were much higher than in the literature. Results showed a medium emotional
exhaustion score of 27.6 versus 19.5 in subsequent thesis work.3 The depersonalisation scores were
19.9 versus 10 and low personal accomplishment at 36 versus 37.4 in the literature.6 This can be
explained by the fact that this study population concerned young interns in their first or second
semester. This assumption confirms Barbarin’s work,40 showing that 70% of first year GPTs meet at
least one of the high burnout criteria (versus 64% in the current study).
Concerning social life and leisure, this study found similar results to those in the literature.7–8,41
The time devoted to private life seemed to be protective for burnout, as well as increasing personal
accomplishment
At T1 and T2, no significant association was found with the number of working hours, satisfaction
with the training course, professional support, doctor–patient training, and aggression. This is hard
to believe, but confirms other studies7 that found other risk factors including a poorly defined role,
lack of support, difficulties in expressing one’s doubts, disproportionate responsibilities, discrimina-
tion, harassment, the gap between business expectations and reality field, or violence. This study
confirms this direction by finding that professional support as protective for burnout and ’conscien-
tiousness hitting’ — being unable to live up to one’s professional values — the experience of
aggression, and stress are risk factors for burnout.
The study showed that ’taking perspective’ empathy is protective for burnout at T1 and T2 and in
the longitudinal analysis. As in the literature,42 clinical (compassionate) empathy decreased over the
course of the GP internship in the current study.
A multicentre study conducted in 2004 with all medical students of Minnesota correlated the pro-
gressive loss of empathy with emotionally difficult experiences of the student during their course of
hospital work, and poor quality of life, unlike feelings of wellbeing that were correlated with a high
degree of empathy.18
If empathy proves to be a powerful help in the understanding of patient needs, it is altered dur-
ing the internship. Emotion-centred coping is associated with emotional exhaustion and a decrease
in personal accomplishment. Active coping strategies (problem-centred and social support-centred
strategies) decreased burnout. Emotion-centred coping was found to be an avoidance strategy that
does not solve the problem and can cause stress.
Implications for research and practiceA number of interventions have been introduced in France to treat burnout in GPs and GPTs within
hospital services.43
Like other doctors, GPTs are often overloaded and continue working despite blatant warning
signs.44 They need to be able to accept their weaknesses and to ask for help if necessary.
Here, organisational aspects join cultural expectations. Like any other social activity, basic rules
should be respected within medical practice. For example, the compensatory rest45 after being on
call (as detailed in a recently proposed law46 limiting GPs working time to 48 hours per week), is far
from being fully implemented. External stressors could be studied to see how systemic/policy
change can be implemented to minimise their contribution to burnout. Qualitative studies can also
help to understand and take the necessary actions for the development of medical education and
GPTs development.
Cultural aspects converge, explain, and strengthen social aspects. Becoming a doctor is not only
founded on knowledge and practice, but also on acculturation to a more or less dogmatic concep-
tion of medical practice. This ’hidden curriculum’47 requires the trainee doctor to absorb and bend
to the implicit, yet pervasive, standards of the medical community: no complaints or even criticism
from their superiors, no emotional or personal disease states, especially if they are related to the
practice of medicine. As such, burnout, even more than non-psychological diseases such as heart fail-
ure or cancer, is marked as a transgression, or of infamy and treason for the medical establishment.
Managing uncertainty and difficulties, dealing with medical errors when they occur, overcoming the
loss of meaning and negotiating ethical dilemmas, treating relatives and one’s own diseases, treating
other sick doctors ... all these situations are, with few exceptions,48 not formally addressed in the
medical curriculum, as if they did not exist or as if everyone should manage them alone, as a per-
sonal problem to be hidden.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 9 of 12
Research

This amplifies the fact that training for managing in patient–doctor relationships is still considered
as implicit and comprises only a very small part of the formal curriculum. In addition to the overwork-
ing,49 medical practice sometimes leads to humiliation and a lack of sensitisation for GPs.50
Beyond the organisation and resources of the healthcare system and those of each caregiver, tak-
ing care of oneself and protecting one’s social life is essential,14 since it has been shown that individ-
uals who have many resources, as they are often less sensitive to stress perception, use active
coping, and have less risk of burnout.15
Funding
The authors received no funding for this research.
Ethical approval
Ethical approval was given by the Parisian Ethical Comittee on 8 July 2013 by the Comite de Protec-
tion des Personnes Ile de France 2.
Authorisation
Authorisation was given by the French National Commission for Data Security (CNIL).
Provenance
Freely submitted; externally peer reviewed.
Acknowledgements
The authors thank all ’Intern-life’ contributors as well as Parisian GPTs who responded to the
questionnaire.
References1. Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for
psychiatry. World Psychiatry 2016; 15(2): 103–111.2. Galam E. L’erreur medicale, le burn out et le soignant (Medical error, burnout and the caregiver). Paris:
Springer, 2012.3. Soler JK, Yaman H, Esteva M, et al. Burnout in European family doctors: the EGPRN study. Fam Pract 2008;
25(4): 245–265. doi: 10.1093/fampra/cmn0384. Truchot D. Epuisement professionnel et burn out: concepts, modeles, interventions. (Professional exhaustion
and burn out: concepts, models, interventions). Paris: Dunod, 2004.5. Galam E. L’epuisement professionnel des medecins franciliens: temoignages, analyses et perspectives.
Commission prevention et sante publique (Parisian physician burnout: testimonies, analysis, and prospects).Union Regionale des Medecins Liberaux d’Ile de France. 2007.
6. Galam E, Komly V, Le Tourneur A, et al. Burnout among French GPs in training: a cross-sectional study. Br JGen Pract 2013; 63(608): e217–e224. doi: 10.3399/bjgp13X664270
7. Ernst M. Le syndrome de Burn out des internes en medecine generale a la faculte de medecine deStrasbourg: prevalence et analyse d’entretiens (Strasbourg GPTs burnout syndrome: prevalence and analysisof interviews). These d’exercice en medecine. Strasbourg: Universite de Strasbourg, 2009.
8. Guinaud M. Evaluation du burn out chez les internes de medecine generale et etude des facteurs associes(Evaluation of GPT’s burnout and associated factors study). These d’exercice en medecine. Creteil:Universite de Creteil, 2006.
9. Thevenet M. Analyse du burn out chez les internes de medecine generale sur la base d’une etudecomparative entre l’Ile de France et le Languedoc-Roussillon (Analysis of GPT’s burnout: comparativeanalysis between two French regions). These d’exercice en medecine. Paris: Universite de Paris 6, 2011.
10. Chocard AS, Gohier B, Juan F, et al. Le suicide des medecins (physician’s suicide) revue francaise depsychiatrie et de psychologie medicale. 2003; 65: 23–29.
11. Cherniss C. Beyond burnout: helping teachers, nurses, therapists and lawyers recover from stress anddisillusionment. New York, NY: Routledge, 1995.
12. Karasek R, Theorell T. Healthy work: stress, productivity and the reconstruction of working life. New York,NY: Basic Books, 1990.
13. Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol 1996; 1(1):27–41. doi: 10.1037/1076-8998.1.1.27
14. Freudenberger HJ. Staff burn-out. J Soc Issues 1974; 30(1): 159–165. doi: 10.1111/j.1540-4560.1974.tb00706.x
15. Hobfoll SE. Conservation of resources. A new attempt at conceptualizing stress. Am Psychol 1989; 44(3):513–524. doi: 10.1037/0003-066X.44.3.513
16. Prins JT, Gazendam-Donofrio SM, Dillingh GS, et al. The relationship between reciprocity and burnout inDutch medical residents. Med Educ 2008; 42(7): 721–728. doi: 10.1111/j.1365-2923.2008.03041.x
17. Lazarus RS, Folkman S. Stress, appraisal and coping. New York, NY: Springer, 1984.
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 10 of 12
Research

18. Thomas MR, Dyrbye LN, Huntington JL, et al. How do distress and wellbeing relate to medical studentempathy? A multicenter study. J Gen Intern Med 2007; 22(2): 177–183. doi: 10.1007/s11606-006-0039-6
19. Iacovides A, Fountoulakis KN, Kaprinis S, et al. The relationship between job stress, burnout and clinicaldepression. J Affect Disord 2003; 75(3): 209–221. doi: 10.1016/S0165-0327(02)00101-5
20. Biaggi P, Peter S, Ulich E. Stressors, emotional exhaustion and aversion to patients in residents and chiefresidents — what can be done? Swiss Med Wkly 2003; 133(23-24): 339–346. doi: 2003/23/smw-10134
21. West CP, Tan AD, Habermann TM, et al. Association of resident fatigue and distress. with perceivedmedical errors. JAMA 2004; 302: 12.
22. Weinger MB, Ancoli-Israel S. Sleep deprivation and clinical performance. JAMA 2002; 287(8): 955–957. doi:10.1001/jama.287.8.955
23. West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress andempathy: a prospective longitudinal study. JAMA 2006; 296(9): 1071–1078. doi: 10.1001/jama.296.9.1071
24. Rogers CR. Le developpement de la personne (On becoming a person). Malakoff: Dunod. 2005; 270.25. Hojat M. Empathy in patient care: antecedents, development, measurement, and outcomes. 1st edition.
New York, NY: Springer-Verlag, 2006.26. Buffel du Vaure C. Determinants de l’empathie clinique des medecins generalistes et de leur pratique
(Determinants of GP’s practice and clinical empathy). These d’exercice en medecine. Paris: Universite Paris5. 2012.
27. Lamothe M, Boujut E, Zenasni F, et al. To be or not to be empathic: the combined role of empathic concernand perspective taking in understanding burnout in general practice. BMC Fam Pract 2014; 15: 15. doi: 10.1186/1471-2296-15-15
28. Pronost AM, Tap P. La prevention du burn out et ses incidences sur les strategies de coping (Burnoutprevention and implications on coping strategies). Psychologie De La Sante, Psychologie Francaise 1996; 41(2): 165–172.
29. Kolecj M, Bruchon-Schweitze M, Thiebaut E, et al. Job stress, coping and burn out among French generalpractitioners. Eur Rev of Appl Psychol 2000; 50: 309–314.
30. Mahood SC. Medical education beware the hidden curriculum. Can Fam Physician 2011; 57(9): 983–985.31. Galam E. [Becoming doctor: highlight the hidden curriculum. Medical error as an example]. Presse Med
2014; 43(4 Pt 1): 358–362.32. Vauloup-Soupault C. Facteurs predictifs du burnout chez les internes de medecine generale d’Ile de France
(Predictive burnout factors among parisians GPTs). These d’exercice de medecine generale. Paris: UniversiteParis 5; 2014.
33. Bazin L. Evolution et lien entre burnout et empathie au cours des deux premieres annees d’internat demedecine generale (Evolution and correlations between burnout and empathy during two first years ofgeneral practice course). These d’exercice en medecine. Paris: Universite Paris 5, 2015.
34. Marot ML. Facteurs predictifs d’empathie chez les internes de medecine generale. (Predictive factors ofburnout among GPTs). These d’exercice en medecine. Paris: Universite Paris 5, 2015.
35. Tavakol S, Dennick R, Tavakol M. Psychometric properties and confirmatory factor analysis of the JeffersonScale of Physician Empathy. BMC Med Educ 2011; 11: 54. doi: 10.1186/1472-6920-11-54
36. Skinner EA, Edge K, Altman J, et al. Searching for the structure of coping: a review and critique of categorysystems for classifying ways of coping. Psychol Bull 2003; 129(2): 216–269. doi: 10.1037/0033-2909.129.2.216
37. Myszkowski N, Villoing B, Zenasni F, et al. Monitoring stress among internal medicine residents: anexperience-driven, practical and short measure. Psychol Health Med 2016. 1–8. doi: 10.1080/13548506.2016.1220599
38. Zigmond AS, Snaith RP.Hospital anxiety and depression scale. http://www.scalesandmeasures.net/files/files/HADS.pdf (accessed 7 Apr 2017).
39. Cauchard L. De l’evaluation du burn out a la promotion du bien-etre des internes en Languedoc-Roussillon(From burnout evaluation to the promotion of wellbeing of the residents in Languedoc-Roussillon) Thesed’exercice en medecine. Montpellier: Universite de Montpellier, 2009.
40. Barbarin B, Goronflot L. Syndrome d’epuisement professionnel chez les internes de medecine generale(Burnout in residents among general practice. A cross sectionnal study). Exercer 2012; 101: 72–78.
41. Pittaco M. Les internes sont-ils en burnout? (Are residents burnt out ?) These d’exercice en medecine. Paris:Universite de Paris, 2009.
42. Airagnes G, Consoli SM, De Morlhon O, et al. Appropriate training based on Balint groups can improve theempathic abilities of medical students: a preliminary study. J Psychosom Res 2014; 76(5): 426–429. doi: 10.1016/j.jpsychores.2014.03.005
43. Revue MEDECINE. Numero special: soigner les soignants. (Special issue: caring for caregivers). 2015. http://www.jle.com/fr/revues/med/sommaire.phtml?cle_parution=4265. (accessed 8 Jun 2017).
44. Szymczak JE, Smathers S, Hoegg C, et al. Reasons why physicians and advanced practice clinicians workwhile sick: a mixed-methods analysis. JAMA Pediatr 2015; 169(9): 815–821. doi: 10.1001/jamapediatrics.2015.0684
45. Ministere de l’Education Nationale Superieure et de la Recherche. Les etudes de sante. http://www.enseignementsup-recherche.gouv.fr/cid102950/temps-de-travail-des-internes-et-respect-du-repos-de-securite.html (accessed 7 Apr 2017)
46. Legifrance.gouv.fr. Decret n˚2015-225 du 26 fevrier. 2015. https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000030295642&categorieLien=idchangement (accessed 7 Apr 2017).
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 11 of 12
Research

47. Galam E. Soigner les soignants. La formation implicite des medecins et leurs fragilites (Caring for cargivers.Medical hidden curriculum and doctors’ fragilities). Medecine 2015; 11: 388–389. doi: 10.1684/med.2015.1284
48. Galam E. De l’erreur medicale a la securite du patient. Un enseignement moderne et sensible (From medicalerror to patient safety. A modern and sensitive course). Medecine 2015; 11: 418–423. doi: 10.1684/med.2015.1293
49. Maranda M-F, Gilbert M-A, Saint-Arnaud L, et al. La detresse des medecins : un appel au changement(Doctor’s distress. A call for change). Laval: Les Presses de l’Universite de Laval. 2006; 152.
50. Cook AF, Arora VM, Rasinski KA, et al. The prevalence of medical student mistreatment and its associationwith burnout. Acad Med 2014; 89(5): 749–754. doi: 10.1097/ACM.0000000000000204
Galam E et al. BJGP Open 2017; DOI: 10.3399/bjgpopen17X100773 12 of 12
Research