Embed Size (px)
Citation preview

Pediatric Pulmonology 31:394±397 (2001)
Bronchiolitis Obliterans Organizing Pneumonia (BOOP)in a Child With Mild-To-Moderate Asthma:
Evidence of Mast Cell and EosinophilRecruitment in Lung Specimens
Angelo Barbato, MD,1* Cristina Panizzolo, MD,1 Emanuele S.G. D'Amore, MD,2
Mario La Rosa, MD,3 and Marina Saetta, MD4
Summary. Bronchiolitis obliterans with organizing pneumonia (BOOP) is rarely described inchildren and little is known about its pathogenesis. This paper reports on an 11-year-old patient
suffering from mild-to-moderate asthma. He presented with a retrocardiac density at chest
computed tomography scan that was slow to resolve and failed to respond to antibiotic therapy.
Open lung biopsy revealed a histological picture with buds of granulation tissue in respiratorybronchioles and alveolar ducts, with organized extensions into the alveoli. The use of monoclonal
antibodies on biopsy specimens demonstrated the presence of an in¯ammatory process affecting
not only the thickened alveolar walls, but also the remaining lung parenchyma, the pulmonary
arteries, and the bronchioles. The in¯ammatory in®ltrate consisted mainly of mast cells andeosinophils. The clinical condition improved with steroid therapy. To the best of the authors'
knowledge, this is the ®rst report of BOOP in an asthmatic child with recruitment of mast cells and
eosinophils documented by using monoclonal antibodies. Pediatr Pulmonol. 2001; 31:394±397. ß 2001 Wiley-Liss, Inc.
Key words: BOOP; asthma; mast cells; eosinophils; in¯ammation.
INTRODUCTION
Bronchiolitis obliterans organizing pneumonia (BOOP)is a relatively rare disease characterized by: 1) patchyin¯ammatory changes of the bronchoalveolar lumenand wall, with some associated peribronchial scarring;2) patchy areas of organizing pneumonia; 3) obliterationof the alveolar lumen by intraluminal polyps of looseconnective tissue, containing in¯ammatory cells and®broblasts; 4) an interstitial mononuclear cell in®ltrate ofvarying severity.1±3
The presence of numerous mast cells in the intra-alveolar spaces and septa has already been described inthe adult,3,4 whereas reports of its association with eosi-nophil activation are less common.5 This report describesa case of BOOP in an asthmatic child, diagnosed by openlung biopsy (OLB) and using monoclonal antibodies onthe biopsy specimen to identify an in¯ammatory processin which the mast cells and eosinophils were thepredominant cell types.
CASE REPORT
S.N., an 11-year-old Caucasian male with a familyhistory of atopy, had atopic dermatitis from the age of 3months to 3 years. After spontaneous clinical regressionof his eczema, he developed persistent mild-to-moderateasthma, with 3±4 episodes a year, treated during the
winter season with nebulized beta2-agonists and inhaledsteroids. He also suffered from exertion-induced asthma.Prick tests for allergies at age 6 years revealed reactionsto house dust mites, grasses, and olive. As of March 1997,he had mild episodes of asthma (twice a month) and wastreated with beta2-agonist nebulizers, inhaled steroids,and cyclic antibiotics. In the intervals between bronch-ospastic attacks, he had a productive cough that persistedeven at night. In August 1997, the child was seen by apediatrician because of a persistent productive cough andreduced air exchange in the lower left lobe was detected.The child was hospitalized.
His clinical status was generally satisfactory. Heweighed 43 kg (90±97th %ile) and was 146 cm tall
1Department of Pediatrics, University of Padova, Padova, Italy.
2Institute of Pathology, University of Padova, Padova, Italy.
3Department of Pediatrics, University of Catania, Catania, Italy.
4Institute of Industrial Medicine, University of Padova, Padova, Italy.
*Correspondence to: Prof. Angelo Barbato, Dipartimento di Pediatria,
Universit�a di Padova, Via Giustiniani 3, 35128 Padova, Italy.
E-mail: [email protected]
Received 11 March 1999; Accepted 11 November 1999.
ß 2001 Wiley-Liss, Inc.

(75th %ile). He had no chest deformities, and breathsounds were normal. Cardiac ®ndings were normal.
Blood test results were normal: white blood cell count(WBC) was 9,870/mm3 (neutrophils 64%, lymphocytes24%, monocytes 5%, eosinophils 4%, and basophils 3%).Erythrocyte sedimentation rate was 16 mm/hr, C-reactiveprotein was 3.2 mg/L; intradermal tuberculosis skin testwas negative, with 5 U of PPD. Blood testing for preci-pitins for Thermopolyspora polyspora were negative.
The sweat test showed 38 mEq/L of Clÿ . Immuno-globins G, M, and A were normal. IgE was 578 IU/L.Prick test results showed 4� reactions for grasses andolive, and 3� for house dust mites. No antibodies toadenovirus, in¯uenza virus, and Mycoplasma pneumo-niae were found. Chest X-ray revealed a retrocardiacdensity.
Spirometry indicated a mild, restrictive ventilatorydisorder: forced vital capacity (FVC)� 2.59 L (89%);forced expired volume in 1 sec (FEV1)� 2.14 L (82%);maximal expiratory ¯ow when 75% of FVC remains to beexhaled (MEF 75)� 3.68 L/sec (103%); MEF 50� 3.04L/sec (129%); and MEF 25� 1.56 L/sec (141%).
Computed tomography (CT) scan of the chest showeda retrocardiac density close to the hilum. Lung scinti-graphy showed no gallium accumulation in the lungs.The child was given antibiotic therapy that resulted in noclinical improvement.
Bronchoscopy demonstrated in¯ammatory stenosis ofthe left lower lobe airways associated with the presenceof thick secretions (culture was negative).
A thoracotomy for OLB revealed normal gross lungmorphology. Multiple biopsies were taken from the lowerleft lobe. Open lung biopsy revealed a histological picturewith buds of granulation tissue in respiratory bronchiolesand alveolar ducts, with extension of the organizedin¯ammatory process into the alveoli.
The child was initially treated with oral steroids, andthen for 6 months with beclomethasone dipropionateinhalation 500 mg three times a day. Follow-up CT scan1 month after surgery showed that the parenchymalstructure still presented areas of micro-atelactasis in the
posterior segment of the left lower lobe. More than 18months after the biopsy, the child is well, with no clinicalevidence of pulmonary disease and normal spirometricvalues.
MICROSCOPIC PATHOLOGY
Specimens obtained from the lung were ®xed in 10%formaldehyde and embedded in paraf®n. Five-micron-thick serial sections were prepared immunohistochemicalprocessing as described elsewhere.6 Mouse monoclonalantibodies were used to identify neutrophils (anti-elastase, M792 Dako Ltd., High Wycombe, UK),eosinophils (anti-EG-2, Pharmacia Diagnostic, Fair®eld,NJ), mast cells (anti-tryptase, M7052 Dako), macro-phages (anti-CD68, M814 Dako), and CD4 � cells (anti-CD4, M834 Dako). Monoclonal antibody binding wasdetected with the alkaline phosphatase anti-alkalinephosphatase method (APAAP kit system K 670 Dako)and fast-red substrate. To expose the immunoreactiveepitopes of cell markers, the sections to be stained formacrophages, eosinophils, and mast cells were pretreatedwith an aqueous solution of 0.1% trypsin (SigmaChemical) in 0.1% calcium chloride at pH 7.8 and at37�C for 20 min. Control slides were included in eachstaining run, using human tonsil as a positive control andmouse monoclonal anticytokeratin antibody (M717Dako) as a negative control.
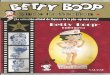
Microscopy showed thickening of the alveolar walls inthe areas surrounding the pulmonary arteries andbronchioles. This feature was associated with thepresence of an in¯ammatory process that involved notonly the thickened alveolar walls, but also the remaininglung parenchyma, bronchioles, and periarteriolar areas(Fig. 1). This in¯ammatory process consisted mainly ofmast cells (Fig. 2) and eosinophils (Fig. 3), whileneutrophils were only occasionally detected, and thein®ltration of macrophages and CD4� T-lymphocyteswas moderate.
DISCUSSION
The diagnosis of BOOP was suspected on the basis ofclinical and radiological ®ndings (retrocardiac density onCT scan, failure to respond to antibiotic treatment, andfavorable response to steroid therapy), and was con®rmedby histological ®ndings in the OLB. In the recentliterature, there have been several reports of pediatriccases of BOOP, though their number remains verylimited, possibly because lung biopsy is essential tocon®rm such a diagnosis, and this diagnostic practice isonly applied to children with severe disease.
Some pediatric case reports have suggested a link withetiological factors such as medication,7 infections,8 orimmunological processes,9,10 while in other cases theetiology has remained unclear and BOOP was considered
ABBREVIATIONS
BOOP Bronchiolitis obliterans with organizing pneumonia
CT Computed tomography
FVC Forced vital capacity
FEV1 Forced expiratory volume in 1 sec
MEF 75 Maximal expiratory ¯ow when 75% of FVC remains to be
exhaled
MEF 50 Maximal expiratory ¯ow when 50% of FVC remains to be
exhaled
MEF 25 Maximal expiratory ¯ow when 25% of FVC remains to be
exhaled
OLB Open lung biopsy
BOOP in Asthma 395

idiopathic.11 In our patient, the cause of BOOP remainsunproven, though we cannot rule out that the child'sallergic asthma played an etiologic role; in fact, acorrelation between hypersensitivity to inhalants andBOOP has been demonstrated in the adult.5
As in the adult, pediatric BOOP is a ®brosing lungdisease characterized histologically by a proliferationof ®broblasts in the distal bronchioles, alveolar ducts,and alveoli.1,2 Although the ®brosis is of rapid onsetand involves the proliferation of ®broblastic cells, theprognosis is generally good and steroid treatment canlead, as in our case, to a complete clinical regressionof the disease, suggesting reversibility of the ®broticprocess.12 The presence of mast cells in the septa andintra-alveolar spaces has already been reported in adultBOOP13 and was emphasized recently.4 In the reportfrom Pesci et al.,4 a mutual relationship between mastcells and ®broblasts was suggested in the pathogenesis ofthis disease. Mast cell clones cannot induce ®brosis, butthe interaction between mast cells and ®broblasts14
suggests a primary role for mast cells in the developmentof ®brosis, even in reversible ®brotic disorders such asBOOP.
In our case, the presence of numerous mast cells in thelung parenchyma, bronchioles, and periarteriolar areasseems consistent with ®ndings in the adult.4 It is moredif®cult to interpret the eosinophils in the biopsy materialof our case. Their presence could be due to the child'sasthma, or to other causes. Numerous eosinophils andBOOP were found in several adults with hypersensitivityto inhalants5 and also in patients affected by in¯amma-tory bowel disease and sulfalazine-induced BOOP.15 Anincrease in eosinophils in the bronchoalveolar lavage¯uid of patients with BOOP and evolving ®brosis hasbeen described in adults who had a poor response totreatment.12 The presence of mast cells and eosinophils inour biopsy specimens might be a demonstration of a trendtoward ®brosis and a sign of the advisability of initiatingan adequete therapy early. In our case, the etiologyremains idiopathic, though it is possible that allergicenvironmental factors may have stimulated the observedrecruitment of eosinophils and mast cells. To ourknowledge, this is the ®rst reported case of BOOP in achild with a recent history of intermittently active asthma,with histological ®ndings documenting an importantrecruitment of mast cells and eosinophils.
REFERENCES
1. Epler GR, Colby TV, McLoud TC, Carrington C, Gaensler E.Bronchiolitis obliterans organizing pneumonia. N Engl J Med1985;312:152±158.
2. Katzenstein AL, Myers JL, Prophet WD, Corley L, Shin M.Bronchiolitis obliterans and usual interstitial pneumonia: acomparative clinicopathologic study. Am J Surg Pathol1986;10:373±381.
Fig. 2. Detail of Figure 1, showing mast-cell in®ltration in lungparenchyma, bronchioles, and periarteriolar areas. Immunos-taining with monoclonal antitryptase antibody (magni®cation� 200).
Fig. 3. Photomicrograph showing eosinophilic in®ltration intolung parenchyma, bronchioles, and periarteriolar areas. Immu-nostaining with monoclonal anti-EG-2 antibody (magni®cation� 200).
Fig. 1. Photomicrograph showing thickening of alveolar wallsin areas surrounding pulmonary arterioles and bronchioles.Immunostaining with monoclonal antitryptase antibody(magni®cation�80).
396 Barbato et al.

3. Colby TV. Pathologic aspects of bronchiolitis obliterans organiz-ing pneumonia. Chest 1992;102:38±43.
4. Pesci A, Majori M, Piccoli ML, Casalini A, Curti A, Franchini D,Gabrielli M. Mast cells in bronchiolitis obliterans organizingpneumonia. Mast cell hyperplasia and evidence for extracellularrelease of tryptase. Chest 1996;110:383±391.
5. Cohen AJ, King TE, Downey GP. Rapidly progressive bronch-iolitis obliterans with organizing pneumonia. Am J Respir CritCare Med 1994;149:1670±1675.
6. Saetta M, Turato G, Facchini FM, Corbino L, Lucchini RE,Casoni G, Maestrelli P, Mappa CE, Ciaccia A, Fabbri LM.In¯ammatory cells in the bronchial glands of smokers withchronic bronchitis. Am J Respir Crit Care Med 1997;156:1633±1639.
7. Battistini E, Dini G, Savioli C, Morando A, Gandolfo A, KotitsaZ, Garaventa A, Rossi GA. Bronchiolitis obliterans organizingpneumonia in three children with acute leukemias treated withcytosine arabinoside and anthracyclines. Eur Respir J 1997;10:1187±1190.
8. Zahraa J, Herold B, Abrahams C, Johnson D. Bronchiolitisobliterans organizing pneumonia in a child with acquiredimmunode®ciency syndrome. Pediatr Infect Dis J 1996;15:448±451.
9. Mahajan L, Kay M, Wyllie R, Steffen R, Goldfarb J. Ulcerativecolitis presenting with bronchiolitis obliterans organizing pneu-monia in a pediatric patient. Am J Gastroenterol 1997;92:2123±2124.
10. Kleinau I, Perez-Canto A, Shmid HG, Grassot A, Staab D, RenzH, Henze G, Wahn U, Paul K. Bronchiolitis obliterans organizingpneumonia and chronic graft-versus-host disease in a child afterallogenic bone-marrow transplantation. Bone Marrow Transplant1997;19:841±844.
11. Inoue T, Toyoshima K, Kikui M. Idiopathic bronchiolitisobliterans organizing pneumonia (idiopathic BOOP) in child-hood. Pediatr Pulmonol 1996;22:67±72.
12. Cordier JF, Loire R, Brune J. Idiopathic bronchiolitis obliteransorganizing pneumonia: de®nition of characteristic clinical pro®lesin a series of 16 patients. Chest 1989;96:999±1004.
13. Peyrol S, Cordier JF, Grimaud JA. Intra-alveolar ®brosis ofidiopathic bronchiolitis obliterans organizing pneumonia: cellmatrix patterns. Am J Pathol 1990;137:155±170.
14. Levi-Shaffer F, Rubinichik E. Mast-cell/®broblast intereactions.Clin Exp Allergy 1994;24:1016±1021.
15. Scully R, Mark EJ, McNeely WF, McNeely BU. Case recordsof the Massachussets General Hospital, case 12Ð1993. N EnglJ Med 1993;328:869±876.
BOOP in Asthma 397