Embed Size (px)
Citation preview
Thorax (1963), 18, 45
Bronchial polypsD. J. B. ASHLEY, E. A. DANINO, AND H. D. DAVIES
From Morriston Hospital, Swansea
Carcinoma of the bronchus is by far the mostcommon intrabronchial lesion causing obstructionof the respiratory passages. Benign tumours andmalignant neoplasms originating in connectivetissue are much less frequently seen and, whenthey occur, present difficult problems of diagnosisand of management often solved only at thoraco-tomy. The patients reported here presented withsymptoms due to bronchial obstruction causedby intrabronchial polyps which were not neoplastic.The symptoms were treated by endoscopic removalof the lesions without thoracic exploration.
CASE REPORTS
CASE 1 A labourer, aged 62 years, attended thechest clinic complaining of dyspnoea on effort, whichhad been present for one month. He had had a minordegree of cough without sputum for some years, butin the three weeks preceding admission he expec-torated a good deal of yellow-green sputum. Duringthis period he had also had pain in the right sideof the chest and had occasionally felt cold andshivery. He gave no relevant history of previousillnesses either in himself or his family. He smokeda pipe and had never worked underground in thecoal-mines. His general condition was good, althoughhe had lost some weight; there was no clubbingof the fingers. The trachea was deviated to the leftand there was complete dullness to percussion at theright lung base. A radiograph of the chest showeddense uniform shadowing of the lower part of theright lung. A small amount of amber fluid wasremoved from the right pleural cavity by paracentesis.Malignant cells were not identified in this material.Bronchoscopy was carried out (E. A. D.) two weeks
after this initial attendance at the clinic. The presump-tive diagnosis was carcinoma of the bronchus. Therewas a foetor in the bronchial tree and a large amountof pus was seen coming from the right main bronchus.This was sucked out and the mucosa of the rightmiddle and lower bronchi was seen to be intenselycongested. A granulomatous mass, 2 cm. in length,was seen protruding from the lower lobe bronchuswhich it was obstructing in a ball-valve manner. Thislesion was removed and more pus was seen in thelower lobe bronchus.
Histology Section of this lesion showed it to be apolyp of the bronchial tree. The core consisted of
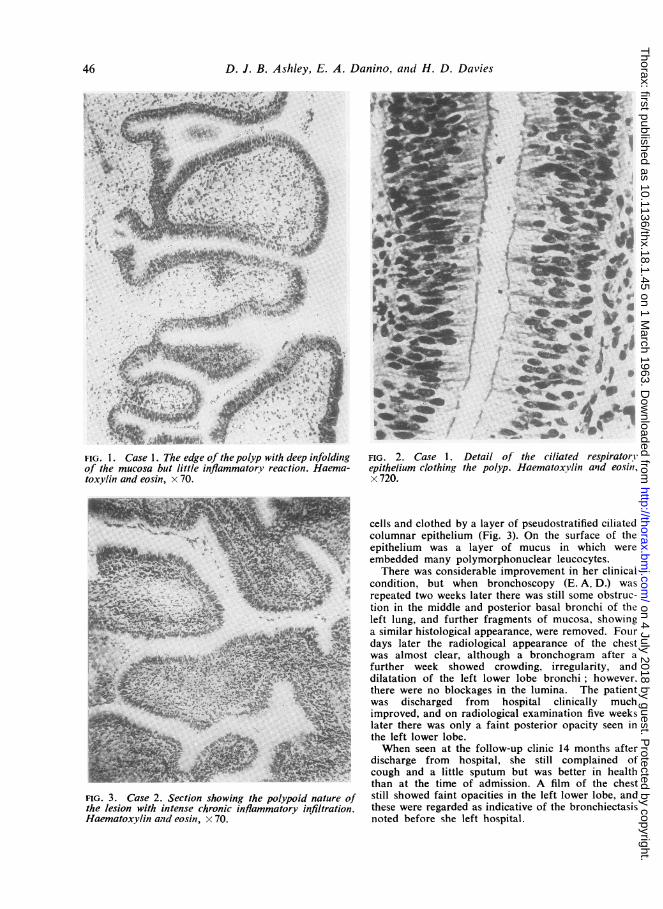
vascular oedematous fibrous tissue in which were afew foci of acute and chronic inflammatory infiltra-tion. The whole of the polyp was clothed bycolumnar ciliated epithelium of respiratory typewhich descended into clefts on the surface of themass (Figs. 1 and 2). No epithelial atypia was seenand there was no squamous metaplasia. There wasno evidence of malignancy in the connective tissuecore of the polyp.A large amount of purulent sputum was drained
from the chest in the week after the bronchoscopy,and clearing of the radiological lesions was seen tobegin on the day after operation. Three weeks laterthe patient felt very well and was producing verylittle sputum, although on examination there werestill diminished resonance and breath sounds at thebase of the right lung. A second bronchoscopy(E. A. D.) was carried out three weeks after the first.There was no odour in the bronchial tree and no puswas seen. The mucosa of the right lower lobebronchus was still thickened and the interbronchialsepta were wide and fleshy. A radiograph taken atthis time showed almost complete clearing of thebasal shadow.The patient was discharged from hospital 34 days
after admission. Eighteen months after discharge hewas still well and free of respiratory symptoms.
CASE 2 A woman of 34 was admitted to hospitalcomplaining of tiredness and the loss of 40 lb. (18 kg.)in weight over the preceding seven months. She wasdyspnoeic on effort. She gave a history of havinghad a chronic cough with sputum since childhood.There was a family history of tuberculosis but tuberclebacilli had never been detected in her sputum andthere was no radiological evidence of tuberculosis.A radiograph of the chest showed streaking in theleft lower lobe. There was no improvement in hercondition after a course of chloramphenicol and nochange in the radiological appearances. A radiographtaken two weeks later showed a diffuse opacity at thebase of the left lung, and a bronchogram showedobstruction to the left lower lobe bronchus.
Bronchoscopy was carried out (E. A. D.) and thefloor of the left lower lobe bronchus was seen to beheaped up and granular and the bronchial lumenwas obstructed. The mucosa was removed piecemeal.
Histology The mucosa was of polypoid type.There was a core of vascular oedematous connectivetissue heavily infiltrated by lymphocytes and plasma
45
on 4 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.18.1.45 on 1 March 1963. D
ownloaded from
D. J. B. Ashley, E. A. Danino, and H. D. Davies
FIG. 1. Case 1. The edge of thepolyp with deep infoldingof the mucosa but little inflammatorY reaction. Haema-toxylin and eosin, x 70.
FIG. 3. Case 2. Section showing the polypoid nature ofthe lesion with intense chronic inflammatory infiltration.Haematoxylin and eosin, x 70.
Aft. 9
FIG. 2. Case 1. Detail of the ciliated respiratorYepithelium clothing the polyp. Haematoxylin and eosini,x 720.
cells and clothed by a layer of pseudostratified ciliatedcolumnar epithelium (Fig. 3). On the surface of theepithelium was a layer of mucus in which wereembedded many polymorphonuclear leucocytes.
There was considerable improvement in her clinicalcondition, but when bronchoscopy (E. A. D.) wasrepeated two weeks later there was still some obstruc-tion in the middle and posterior basal bronchi of theleft lung, and further fragments of mucosa, showinga similar histological appearance, were removed. Fourdays later the radiological appearance of the chestwas almost clear, although a bronchogram after afurther week showed crowding, irregularity, anddilatation of the left lower lobe bronchi; however.there were no blockages in the lumina. The patientwas discharged from hospital clinically muchimproved, and on radiological examination five weekslater there was only a faint posterior opacity seen inthe left lower lobe.When seen at the follow-up clinic 14 months after
discharge from hospital, she still complained ofcough and a little sputum but was better in healththan at the time of admission. A film of the cheststill showed faint opacities in the left lower lobe, andthese were regarded as indicative of the bronchiectasisnoted before she left hospital.
46
on 4 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.18.1.45 on 1 March 1963. D
ownloaded from
Bronchial polyps
DISCUSSION
Both of these patients presented with respiratorysymptoms attributable to blockage of a bronchus,and each was relieved by the bronchoscopicremoval of polypoid material from a lower lobebronchus. These lesions are extremely rare, andnone of us could remember having seen one atany time previously. Fried (1959), in his mono-
graph on intrathoracic neoplasms, made no
mention of polyps, and Holinger (1960), in a
similar monograph, described them as uncommon
lesions, frequently associated with suppuration,and analogous to nasal polyps, a view shared bySalek, Pazderka, and Zdk (1958), who describedtwo cases seen in 10 years' experience at thesurgical clinic of Charles University in Prague.Our two patients presented different clinical
pictures, which could be correlated with thedifferent types of polypoid hyperplasia of thebronchial mucosa seen on histological examina-tion. In the first patient there had been nosymptoms referable to the respiratory tract untilthe episode that led to his admission, and a
presumptive clinical and radiological diagnosis ofbronchial carcinoma was made. The polyp wasapparently solitary and was attached to the wallof the bronchus only by a thin peduncle at oneend. It was easily removed in toto at a singleoperation which was followed by a clinical andradiological improvement. In the second patientthere was a long history of bronchial infectionextending back to childhood, and the polypoidtissue causing bronchial obstruction was moreclearly related to a persistent inflammatory statein the bronchial wall. She showed considerablerelief of her acute symptoms but it is unlikely thatmore permanent relief will be experienced. Thesetwo lesions, the solitary bronchial polyp seen incase 1 and the polypoid chronic bronchitis ofcase 2, are to some extent separable.
Pollak, Cohen, and Gnassi (1938) described a
man of 55, who complained of cough and was
found radiologically to have an opacity in the rightupper lobe. An irregular mass of tissue was seen
at bronchoscopy in the right upper lobe bronchus,but he died of respiratory infection before anyattempt at surgical treatment could be made. Atnecropsy a pedunculated growth arising from andobstructing the right upper lobe bronchus was
found. On section this proved to comprise fibroustissue with inflammatory infiltration and oedema.It was covered by a transitional type of epitheliumsuch as is often seen in the infected bronchial tree.Bjork (1952) described a patient whose history,course, and anatomical features were very similar
to those in our case 1. A man of 50 hadcomplained of cough for several months. Threeweeks before admission he had had fever and anintense exacerbation of his cough, both of whichhad subsided on treatment with sulphonamides.He was free from dyspnoea and had a goodappetite. Radiological examination of the chestshowed atelectasis of the left upper lobe, and atbronchoscopy a polyp, 2-5 x 1-5 x 1 cm., was foundattached by a narrow stalk to the wall of thebronchus. On section this lesion was shown to becovered by respiratory epithelium which dippeddeeply into many clefts and ducts in theoedematous fibrous core. There was moderatesubepithelial inflammatory infiltration. Radio-graphs of the chest six days after operation showedthe affected area to be clearing; three monthslater clearing was complete. Three years after-wards he was very well and a further broncho-scopy showed the anatomy of the bronchial treeto be normal. The two Czechoslovakian patients(Salek et al., 1958) were also men, and in each thelesion was removed at thoracotomy. The first wasa man aged 61 who had had a cough for 10 years.Radiographs of the chest showed collapse of themiddle and upper lobes of the right lung, and atbronchoscopy a mobile tumour the size of a cherrywas seen in the main bronchus. Thoracotomy wasperformed and the two affected lobes wereremoved. Section of the polyp showed a vascularfibrous core with a few fat cells and a little chronicinflammatory infiltration; the polyp was coveredby ciliated columnar epithelium which dipped intothe clefts in the core. Four years afterwards hewas alive and free from symptoms. The secondpatient was a man aged 36 who had complainedof cough for five years. A polyp, 4 x 1 x 1-2 cm.,was removed from the left main bronchus atbronchotomy. Section of this lesion showed itto have a sparse fibrous stroma covered partlyby ciliated columnar epithelium and partly bysquamous epithelium. Cords of squamous cellsand 'cysto-papillary' formations extended into thestroma.These four patients and our own patient form a
group in which the principal cause of the respiratorydisease was a solitary polypoid lesion causingbronchial obstruction not associated with evidenceof extensive chronic bronchial inflammation. Thenature of these lesions is uncertain. Histologicallythey do not appear to be neoplastic and aredistinguishable from benign tumours of thebronchus, adenoma and fibroma, that may presentin a similar manner (Powers, Godwin, andLangston, 1956). It is unlikely that they are ofinflammatory origin although apparently solitary
47
on 4 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.18.1.45 on 1 March 1963. D
ownloaded from
D. J. B. Ashley, E. A. Danino, and H. D. Davies
polypoid lesions of the bronchial mucosa mayoccur in chronically inflamed bronchi (Citroni anddi Guglielmo, 1955) and may be recurrent (Peroni,1934). It is more probable that an analogy maybe drawn with the polypoid lesions of the skinand mucous membranes, of unknown aetiology,which consist of a fibrous core surrounded by athin layer of stratified squamous epithelium, orwith the very common polyps of the cervix andcorpus uteri, and that a localized overgrowth ofthe epithelium is perpetuated by being drawn awayfrom its base so that a core of oedematous con-nective tissue can form. Clinically, the importanceof these lesions is that they mimic carcinoma ofthe bronchus. It is difficult to suggest any clinicaldiagnostic criterion that may be used except thatthey are benign in character and can be removed,with clinical cure, by endoscopic means. This isan indication for bronchoscopy in the routineinvestigation of patients clinically thought to beexamples of carcinoma of the bronchus; somemay be benign lesions which, because of theirmechanical effects, are capable of causing deathif untreated (Pollak et al., 1938).Our second case is an example of a more
common lesion that we would like to termpolypoid chronic bronchitis. In these patients thereis a long-standing history of chronic respiratoryinfection (Jackson and Jackson, 1932; Citroni anddi Guglielmo, 1955), and the polypoid mucosa,although it may reach major dimensions and, if ina suitable situation, cause bronchial obstruction,is heavily infiltrated with chronic inflammatorycells. Peroni (1934) distinguished two types ofchronic inflammatory reaction in the bronchialtree, one more superficial and the other involvingthe connective tissues deep to the mucousmembrane. It is this second type of deep inflamma-tion that is likely to cause elevation of thebronchial epithelium and the formation of multiplepolyps. Alteration of the chronically inflamedbronchial epithelium in such a manner is notuncommon although, as we have pointed out, itrarely reaches such proportions as to causemechanical obstruction of the bronchial lumen.We made a survey of 275 bronchial biopsies,mostly taken in the investigation of suspectedcarcinoma of the lung, which were seen in thelaboratory of this hospital between 1956 and 1961.In 172 of these cases a diagnosis of carcinoma ofthe bronchus was confirmed histologically. In ninecases, six of carcinoma of the lung, two subse-quently shown to be simple chronic inflammatorylesions, and one of chronic pulmonary tuberculosis,the bronchial epithelium showed the beginnings ofpolypoid change. The alterations in the micro-
1-*
C,,,',
.
.' ', .-
t..'d.
$.
/'
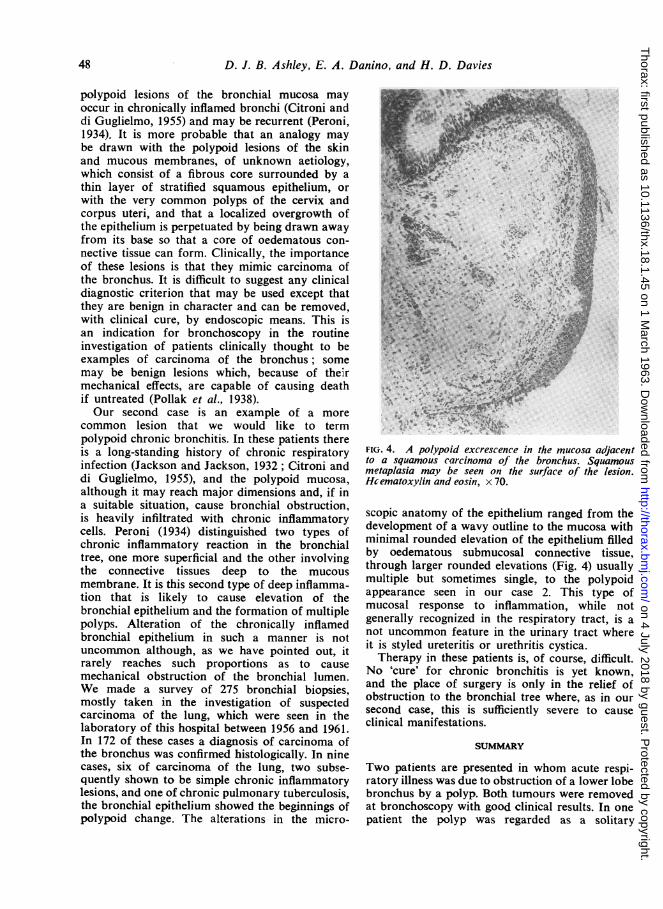
FIG. 4. A polypoid excrescence in the mucosa adjacentto a squamous carcinoma of the bronchus. Squamousmetaplasia may be seen on the surface of the lesion.Hcematoxylin and eosin, x 70.
scopic anatomy of the epithelium ranged from thedevelopment of a wavy outline to the mucosa withminimal rounded elevation of the epithelium filledby oedematous submucosal connective tissue,through larger rounded elevations (Fig. 4) usuallymultiple but sometimes single, to the polypoidappearance seen in our case 2. This type ofmucosal response to inflammation, while notgenerally recognized in the respiratory tract, is anot uncommon feature in the urinary tract whereit is styled ureteritis or urethritis cystica.Therapy in these patients is, of course, difficult.
No 'cure' for chronic bronchitis is yet known,and the place of surgery is only in the relief ofobstruction to the bronchial tree where, as in oursecond case, this is sufficiently severe to causeclinical manifestations.
SUMMARY
Two patients are presented in whom acute respi-ratory illness was due to obstruction of a lower lobebronchus by a polyp. Both tumours were removedat bronchoscopy with good clinical results. In onepatient the polyp was regarded as a solitary
48
7..X-.ov'A * O" k .71. .
JOC,i , % . 1". 4.1 -4. 15.. CIA,. ".. -, '.
" * "k
.. ::i:
11 ., I
x
..O
on 4 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.18.1.45 on 1 March 1963. D
ownloaded from

Bronchial polyps
phenomenon of unknown aetiology and theprognosis was assessed as good. In the other, thelesion was regarded as an unusual manifestationof chronic inflammatory disease of the bronchialtree and, while there was marked improvementin the acute condition, no hope of relief of theunderlying chronic bronchitis could be held out.
We are indebted to Dr. T. W. Davies and Dr. J. M.O'Kane for the provision of clinical data in case 1.
REFERENCES
Bj'rk,[H. (1952). Acta oto-laryng. (Stockh.), 42, 329.Citroni, G. A., and di Guglielmo, L. (1955). Minerva med. (Parte
sci.), 46(2), 686.Fried, B. M. (1959). Tumors of the Lung and Mediastinum. Kimpton,
London.Holinger, P. H. (1960). In Tumors of the Chest, ed. D. M. Spain,
p. 143. Grune and Stratton, New York.Jackson, C., and Jackson, C. L. (1932). J. Amer. med. Ass., 99, 1747.Peroni, A. (1934). Arch. Otolaryng., 19, 1.Pollak, B. S., Cohen, S., and Gnassi, A. M. (1938). Ibid., 27, 426.Powers, R. C., Godwin, M. C., and Langston, H. T. (1956). A.M.A.
Arch. Surg., 72, 984.Salek, J., Pazderka, S., and Zhk, F. (1958). J. thorac. Surg., 35, 807.
49
on 4 July 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.18.1.45 on 1 March 1963. D
ownloaded from