Embed Size (px)
Citation preview
J. Endocrinol. Invest. 19: 186-189 ,1996
CASE REPORT
Bronchial carcinoid tumor presenting as athyroid nodule:An unusual clinical manifestationA. Chico*, M.C. Pallares'" , X. Matfas-Guiu***, L. Cipres" ". M. Puig-Domingo*, andS.M. Webb*Departments of Endocrinology*, Oncology** and Pathology ***, Hospital de la Santa Creu i Sant Pau,Autonomous University of Barce lona, Barcelona; Section of Endocr inology****, Hosp ital Obispo Polanco ,Teruel, Spain
ABSTRACT. Although rare, carcinoid tumors maypresent as thyroid metastatic nodules. We describetwo patients with an undiagnosed bronchial carcinoid tumor, who presented as a thyroid nodule.Pathological examination of these nodules was diagnostic. Chemotherapy was indicated despite thedisseminatio n of the tumors. The patients have an
INTRODUCTION
Carc inoid tumors are infrequent neoplasms, predominantly located in the gastro intestinal tract, andmost frequently in the append ix, but also in the lung(10 %) (1) . These tumors originate in the APUD(amine precursor uptake and decarboxylation) system, and have the capacity to produce many pep tides and amines with different biological actions(1). Characteristically, these tumors produce serotonin , which may be detected by an increased urinary excretion of 5-hydroxyindoleacetic acid (5-HIAA), and the typical clinical manifestation is knownas the "carc inoid syndrome" (flushing , diarrhea,asthma and right-side valvular heart disease) (2);however , the carcinoid syndrome is absent in themajority of carci noid tumors, being mostly confinedto carcinoid tumors of the small bowel metastatizingto the liver. In general, bronchial carcinoids have agood prognosis and only 5% produce distantmetastases (3).We describe two cases of und iagnosed bronchialcarcinoids who presented as a metastatic thyroidnodule . The pathological findings of these nodules
Key-words: Bronchial carcinoid, thyroid metastasis. thyroid nodule.
Correspondence: Dr. S.M. Webb , Dept. Endocrinology, Hospital de laSanta Creu i Sant Pau, Av. San Antonio Marfa Clare t, 16708025,Barcelona, Spain.
Acce pted December 11, 1995.
186
excellent quality of life. They are asymptomatic andalive , 18 and 24 month s afte r diagnosis, respectively. In one case , chemotherapy obtained an important reduction in the size of the tumoral lesionsbut the other case showed no regression. Octreotide(SMS 201-995) was used in the case with carcinoidsyndrome, with an excellent response.
were diagnostic, One of them had cl inical man ifestat ions of the carcinoid syndrome .
CASE REPORTS
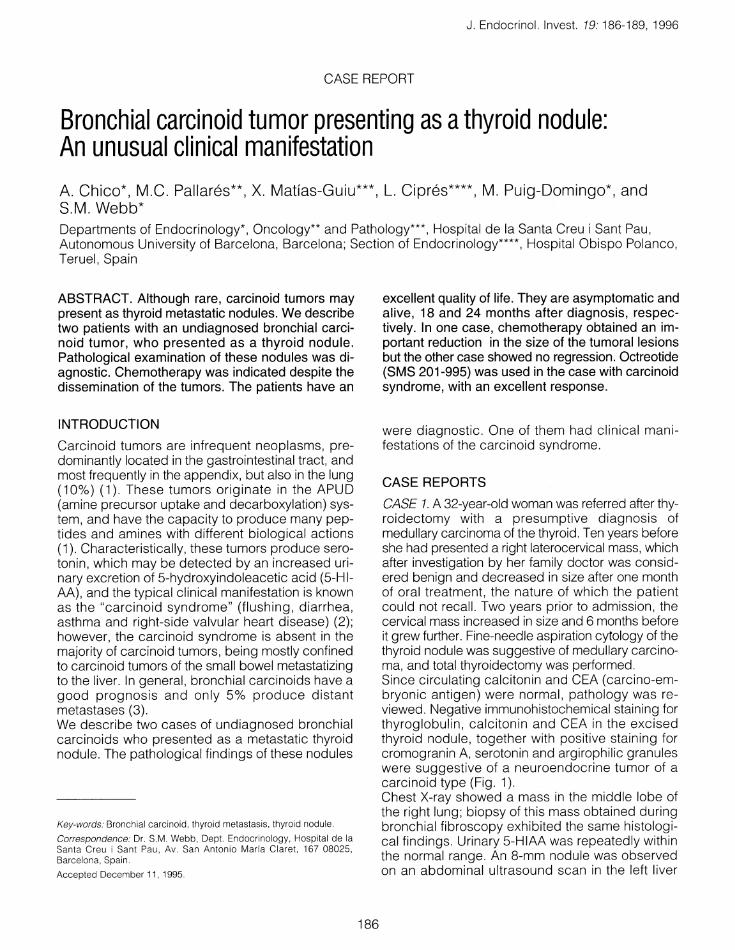
CASE 1. A 32-year-old woman was referred after thyroidectomy with a presumptive diagnosis ofmedullary carcinoma of the thyroid. Ten years beforeshe had presented a right laterocervical mass, whichafter investigation by her family doctor was consid ered benign and decreased in size after one monthof oral treatment , the nature of which the patientcould not recall. Two years prior to admission, thecervical mass increased in size and 6 months beforeit grew further. Fine-needle aspiration cytology of thethyroid nodule was suggestive of medullary carc inoma, and total thyroidectomy was performed.Since circu lating calcitonin and CEA (carcino-embryonic antigen) were normal , patho logy was reviewed . Negative immunohistochemical staining forthyroglobulin , calciton in and CEA in the exc isedthyroid nodule , together with positive staining forcromogranin A, serotonin and argirophilic granuleswere suggestive of a neuroendocrine tumor of acarcinoid type (Fig. 1).Chest X-ray showed a mass in the middle lobe ofthe right lung; biopsy of this mass obtained duringbronchial fibroscopy exhibited the same histological findings. Urinary 5-HIAA was repeatedly withinthe normal range . An 8-mm nodule was observedon an abdominal ultrasound scan in the left liver
A. Chico, M.C . Pal/ares, X. Matfas-Guiu, et al.
Fig. 1 - Microscopical view of the thyroid nodule obtained afterthyroidectomy, illustrating the regular growth pa ttern and theuniform round-ce ll nuclei, characteristic of carcinoid tumors(Hematoxylin and eosin, X400).
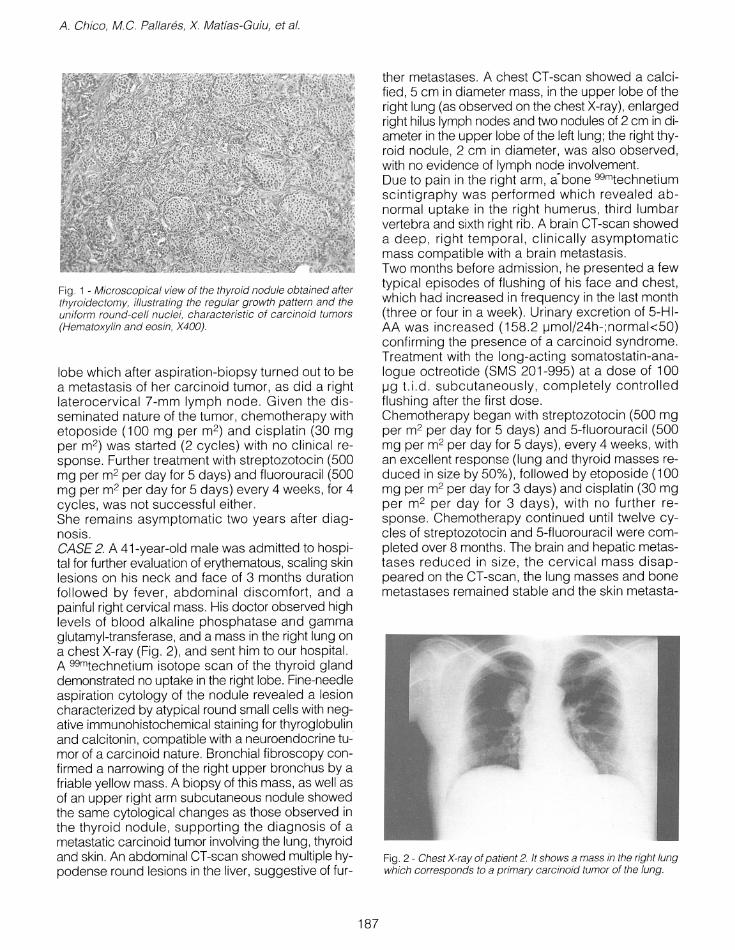
lobe which after aspiration-biopsy turned out to bea metastasis of her carcinoid tumor , as did a rightlaterocervical 7-mm lymph node . Given the disseminated nature of the tumor , chemotherapy withetoposide (100 mg per m2) and cisplatin (30 mgper m2) was started (2 cycles) with no clin ical response. Further treatment with streptozotocin (500mg per m2 per day for 5 days) and fluorouracil (500mg per m2 per day for 5 days) every 4 weeks , for 4cycles, was not successful either.She remain s asymptomatic two years after diagnosis.CASE2. A 41-year-old male was admitted to hospital for further evaluation of erythematous, scaling skinlesions on his neck and face of 3 months durationfollowed by fever , abdominal discomfort, and apainful right cervical mass. His doctor observed highlevels of blood alkaline phosphatase and gammaglutamyl-transferase, and a mass in the right lung ona chest X-ray (Fig. 2), and sent him to our hospital.A 99mtechnetium isotope scan of the thyroid glanddemonstrated no uptake in the right lobe. Fine-needleaspiration cytology of the nodule revealed a lesioncharacterized by atypical round small cells with negative immunohistochemical staining for thyroglobulinand calcitonin, compatib le with a neuroendoc rine tumor of a carcino id nature. Bronchial fibroscopy confirmed a narrowing of the right upper bronchus by afriable yellow mass. A biopsy of this mass, as well asof an upper right arm subcutaneous nodule showedthe same cytological changes as those observed inthe thyroid nodule, supporting the diagnosis of ametastatic carcinoid tumor involving the lung, thyroidand skin. An abdominal CT-scan showed multiple hypodense round lesions in the liver, suggestive of fur-
187
ther metastases. A chest CT-scan showed a calc ified, 5 cm in diameter mass, in the upper lobe of theright lung (as observed on the chest X-ray), enlargedright hilus lymph nodes and two nodules of 2 cm in diameter in the upper lobe of the left lung; the right thyroid nodule , 2 cm in diameter, was also observed ,with no evidence of lymph node involvement.Due to pain in the right arm , a-bone 99mtechnetiumsc intigraphy was performed which revealed abnormal uptake in the right humerus, third lumbarvertebra and sixth right rib. A brain CT-scan showeda deep, right temporal, c linically asymptomaticmass compatible with a bra in metastasis.Two months before admission, he presented a fewtypical episodes of flushing of his face and chest,which had increased in frequency in the last month(three or four in a week) . Urinary excretion of 5-HIAA was increased (158 .2 ~mol/24h-;normak50)
confirming the presence of a carc inoid syndrome.Treatm ent with the long -acting somatostatin-analogue octreotide (SMS 201-995) at a dose of 100~g t .i.d . subcutaneously , completely controlledflushing after the first dose .Chemothe rapy began with streptozotocin (500 mgper m2 per day for 5 days) and 5-fluorouracil (500mg per m2 per day for 5 days), every 4 weeks , withan excellent response (lung and thyroid masses reduced in size by 50%), followed by etoposide (100mg per m2 per day for 3 days) and cisplatin (30 mgper m2 pe r day for 3 days), with no further response. Chemotherapy continued until twelve cycles of streptozotocin and 5-fluorouracil were completed over 8 months. The brain and hepatic metastases redu ced in size, the cervical mass disappeared on the CT-scan , the lung masses and bonemetastases remained stable and the skin metasta-
Fig . 2 - Chest X-ray of pat ient 2. It shows a mass in the right lungwhich corresp onds to a primary carcinoid tumor of the lung.

sis disappeared . Eighteen months after diagnosishe sti ll remains in partial remission , clinicallyasymptomatic, working, and leading a normal active life, with octreot ide 300 IJg per day sc.
DISCUSSIONThyroid metastases present ing as a thyroid masswhile the original source remains occu lt are extremely rare, simulating a primary thyroid tumor ornodular thyroiditis , thereby increasing the diagnostic challenge for the clinician . Among thyroidmetastases, the most common are renal cell carcinoma, large bowel adenocarcinoma, and malignantmelanoma (4). Bronchopulmonary carcinoids, arising from the Kulchitzsky cells of the bronchus, constitute less than 5% of lung tumors (3). Carcinoidswere mistakenly called "bronchial adenomas" in thepast ; additionally, the name carcinoid is inappropriate, as these neoplasms are true carcinomas (5).Most pulmonary carcinoids have a good prognosis with a low incidence of metastases , but someof them run a rapid course with metastatic spread(6) . Extrabronch ial extension occurs in approximately 10% of patients, especially to regional lymphnodes (3), but distant metastases can appear (liver, bone and adrenal gland are the most frequent).Berge et al. (7), found 201 carcinoid tumours in aseries of 16,296 autops ies, and only two metastatic to the thyroid gland ; none of them originated asa bronchial carcino id. Furthermore, Lerprasertsukeet al. (8), describe a patient with a rectal carcinoidmetastatic to the thyroid.The distinction between pulmonary carcinoidsmetastatic to the thyroid and medullary carcinomaof the thyroid is difficult (9). Rosai (4) and Neslandet al. (10), have described carcinoid tumors of thelung metastat izing to the thyroid and simulating amedullary carcinoma. In the second case (10), thethyroid metastasis appeared 13 years after surgicalexcission of a primary pulmonary carcinoid tumor.111In-DTPA-octreotide scintigraphy can be usefulto localize carcinoid tumor tissue, since this tumorscontain somatostatin receptors (11); however, thisisotope was unavailable at the time our patientspresented .Pulmonary carcinoids cause the carcinoid syndromeonly rarely, in less than 5% of patients (3), which explains why the serotonin metabolite 5-HIAA is usually within the normal range , as in our first case.Given the immediate symptomatic control which octreotidecan attain on flushing and accompanyingclinical characteristics of the carcinoid syndrome, itsuse is appropriate as early therapy in these patients.The described associated reduct ion in 5-HIAA ex-
188
Carcinoid as a thyroid nodule
cretion suggests that the clinical effectivenessof thissomatostatin analog is not due simply to an end-organ effect, but is also related to inhibition of the synthesis or release of serotonin and perhaps of otherbiogenic amines (12-14). A further therapeutic approach with recombinant interferon-alpha-2ahas also been reported to effectively control carcinoidsymptoms, but not tumor growth, and is well tolerated; it constitutes, therefore, a further alternative forthe medical treatment of these patients (15).Surgical removal of the tumor is mandatory whenpossible; if this is not possible,.due to extension ofthe disease, as in our two patients, the second stepis chemotherapy, although most tumors respondpoorly . The most frequently used cytostatic treatment regimens are a combination of streptozotocinand 5-fluorouracil (1). Etoposide and cisplatin canbe effective when the tumor shows atypical histological features (16, 17).The prognos is of pulmonary carcinoids in terms ofsurvival is relatively benign , altough different degrees of malignancy, have been described . Amongthe tumor features, initial clin ical extension and tumor diameter are the most consistent prognosticfactors (18). A 5-year surv ival rate has been observed in approximately 88% of patients with bronchopulmonary carcinoids, but experience variesdepending on the series. In metastatic disease thisrate decreases to 11% (19).In conclusion , metastases to the thyroid of pulmonary carcinoid tumors are except ional , butshould be considered in the differential diagnosis ofpatients presenting thyroid nodules, since specificand potentially successful treatment can be offered.
REFERENCES
1. Creutzfeldt W., Stbckmann F.Carcinoids and carcinoid syndrome.Am. J. Med . 82: 4, 1987.
2. Feldman J.M.Carc inoid tumors and syndrome.Sem.Oncol. 14: 237,1987.
3. Davila D.G., Dunn W.F., Tazelaar HD., Pairolero P.C.Bronchial carcinoid tumors.Mayo. Clin. Proc. 68: 795, 1993.
4. Rosai J., Carcangiu M.L., deLellis RATumors of the thyroid gland.In: Atlas of tumor pathology.AFIP, Bethesda , Maryland , 1992, p. 291.
5. Paladugu R.R., Benfield J.R., Pak H.Y., Ross R.K.,Tepl itz R.L.Bronchopulmonary Kulchit zsky cell carcinomas .Cancer 55: 1303, 1985.
6. Goodwin J.D., Brown C.C.
A. Chico, M. C. Palla res, X. Matias-Guiu, et al.
Comparative epidemiology of carcinoid and oat-celltumors of the lung.Cancer 40: 1671, 1977.
7. Berge T.B., Linell F.Carcinoid tumours.Acta Pathol. Microbiol. Scand . 84: 322, 1976.
8. Lertprasertsuke N., Kakudo K., Satoh S., Tada N.,OsamuraY.Rectal carcinoid tumor metastasizing to the thyroidand pancreas.Acta Pathol. Jpn . 40: 352, 1990.
9. Dunn E.L., Nishiyama R.H., Thompson NW.Medulla ry carcinoma of the thyroid gland .Surgery 73: 848, 1973.
10. Nesland J.M. , Sobrinho-Simoes MA, Holm R.,Johannessen J.V.Organoid tumor in the thyroid gland .Ultrastruct. Pathol. 9: 65, 1985.
11. Krenning E.P., Bakker W.M., Breemar WAP.Localization of endocrine related tumours with a radioiodinated analogue of somatostatin.Lancet 1: 242, 1989.
12. Kvols L., Moertel C., Schutt A , Rubin J.Treatment of the malignant carcinoid syndrome.Evaluation of the long-acting somatostatin analogue.N. Engl. J. Med. 315: 663, 1986.
13. Lamberts SW.J., Krenning E., Reubi J.C.The role of somatostatin and its analogs in the diagnosis and treatment of tumors.Endocr . Rev. 12: 450, 1986.
189
14. Moertel C.G., Johnson C.M., McKusicc k M.A., MartinJ.K., Nagorney D.M., Kvols L.K., RubinJ., KunselmanS.The management of patients with advanced carci noid tumors and islet cell carcinomas.Ann. Intern. Med. 120: 302,1994.
15. Bajetta E., Zilembo N., Di Bartolomeo M., Di Leo A ,Pilotti S., Bochicchio AM. , Castellani R., Buzzoni R.,Celio L., Dogliotti L., Pinotti G., Aitini E., Labianca R.,Fornasiero A, RivaP., SchiepattiG., NelliP., Mariani L.Treatment of metastatic carcinoids and other neuroendocrine tumors with recombinant interferon-alpha-2a.Cancer 72: 3099, 1993.
16. Moertel C.G., Kvols L.K., O'Connell M.J., Rubin J.Treatment of neuroendocrine carcinomas with combined etoposide and cisplatin .Cancer 68: 227, 1991.
17. Grote T.H., Macon W.R., Davis B., Greco FA,Johnson D.H.Atypical carcinoid of the lung.Chest 93: 370, 1988.
18. EI-Naggar AK. , Ballance W., Abdul Karim FW.,Ordonez N.G., McLemore D., Giaco G.G., BatsakisJ.G.Typical and atypical bronchopulmonary carcinoids.Am. J. Clin. Pathol. 95: 828, 1991.
19. Goodwin J.D.Carcinoid tumors: An analysis of 2,837 cases .Cancer 36: 560,1975.