-
Br. J. Cancer (1974) 29, 232
FIBROSIS AS AN INDICATION OF TIME IN INFILTRATINGBREAST CANCER
AND ITS IMPORTANCE IN PROGNOSIS
0. TH. ANASTASSIADES* AND D. M. PRYCEt*Front the Departmtent of
I'athology, State General Hospital, Athens (Cholargos), Greece,
and thetDepartmient of Mlorbid Anatomy, University of London, St
MUary's Hospital, London, England
Receive(d 5 April 1973. Accepted 28 November 1973
Summary.-The histological grading of tumours according to their
intrinsicmalignancy is very important in the prognosis of breast
cancer but within eachgrade the ultimate prognosis depends mainly
on the age of the tumours.
We have shown that tumour fibrosis is an indication of this time
factor, increasingwith the age of the tumour. Within each grade the
metastatic ratio is higher andthe 5 year and 10 year survival less
with the scirrhous than with the non-scirrhoustumours. The
establishment of axillary metastases is closely connected with
boththe degree of malignancy and the time available, the
unfavourable effect upon survivalbeing greater in the scirrhous
than in the non-scirrhous tumours.
Another consequence of the passage of time, as indicated by
fibrosis, is thegradual diminution of lymphoid infiltration (LI)
which is mostly present in youngtumours, especially those of high
grades. The favourable effect of LI upon survivalis demonstrated in
the non-scirrhous tumours of grade III, possibly because of
itsgreat intensity, but this influence upon survival is lost as
fibrosis increases and theintensity of the reaction diminishes.
REACTIVE fibrosis is a phrase oftenused in pathological reports.
It is alsocommonly used by investigators of breastcancer. Gallager
and Martin (1969) haveillustrated diagrammatically the
centralfibrous reaction in infiltrating breastcarcinomata,
referring to it as " reparativefibrosis ". Although the fibrosis in
cancerappears to be truly reactive, this term isapt to convey the
impression that fibrosisis a favourable feature. Evidence to
thecontrary is, however, accumulating. Ina study of the connective
tissue stroma ofbreast carcinomata Smolak, Kolodziejskaand Urban
(1968) found that the 5 yearmortality was greatest with the
poorlydifferentiated carcinomata with abundantand compact
connective tissue stroma.Furthermore, Hamlin (1968) and
Alderson,Hamlin and Staunton (1971) expressedsurprise at the high
mortality score obtainedwith tumour fibrosis.
We have been interested in this matterfor several years. In a
previous paper(Anastassiades and Pryce, 1966), in whichtumour size
was used as an indication oftime, we realized that scirrhous
tumoursrequired a separate scale because, beingshrunken, they
corresponded with non-scirrhous tumours which were larger. Itseems
probable therefore that on averagewithin each grade they would be
olderand have a poorer prognosis. To put thismatter to the test, a
new series of caseswas investigated. From the histologicalstudy of
these cases we came to regardthe fibrous reaction as a continuous
processtaking place during the evolution of br-eastcancer and we
decided to evaluate itsinfluence on metastases and
post-operativesurvival of the patients. We also decidedto assess
the intensity of the lymphoidinfiltration (LI) of the tumours,
thepresence of which has been proved
-
FIBROSIS AND ITS IMPORTANCE IN PROGNOSIS
beneficial by several authors (Moore andFoote, 1949; Black,
Speer and Opler,1956; Richardson, 1956; Berg, 1959;McDivitt,
Stewart and Berg, 1968; Cutleret al., 1969; Bloom, Richardson and
Field,1970; Bloom, 1971) and to evaluate itspossible relationship
to the degree ofmalignancy and fibrosis of the tumours andto the
survival of the patients.
MATERIALS AND MIETHODS
The study was based on a series of 206consecutive cases of
breast cancer operated onbetween the years 1945 and 1950 in St
Mary'sHospital, London. Patients who had re-ceived preoperative
radiotherapy were notincluded. The material for this study wastaken
from the files of the Pathology Depart-ment of St Mary's Hospital
and the survivaldata were obtained independently from thefollow-up
files of the Department ofRadiology.
The original sections were examinedtogether with newr sections
stained withhaematoxylin and eosin, Van Gieson stain andWeigert's
elastin stain. In 8 cases noblocks could be found and in 3 others
thefixation was too poor. As the purpose of thestudy wvas to make a
straight comparisonbetween infiltrating scirrhous and non-scirrhous
tumours, it was considered neces-sary to exclude 12 patients w%ith
mucoidtumours and a similar number with muchintraductal growth but
the minimum ofinfiltration Also discarded were 5 patientswith
multiple tumours, a patient whosetumour had mutated and another in
whom ithad spontaneously regressed. Three couldnot be used because
there was no follow-upand 20 additional ones were discardedbecause
the death of the patients was eitherunrelated to cancer or was due
to an un-known cause.
The 141 cases used had a measurable massof infiltrating growth
ranging from 0-5 to9-0 cm in greatest diameter. The number oflymph
nodes in each case varied from 2 to 19.In 61 cases there were 2 to
5 lymph nodes; in42 the lymph nodes available were
completelyreplaced by growth. The overall metastaticratio of the
initially collected 206 cases was56% and of the 141 cases used
62%.
Grading of tumours was made accordingto Bloom and Richardson
(1957). The
tumours were originally divided according tothe quantity of
their fibre content into 4groups, but due to the paucity of numbers
thefinal comparison was made betw%een thecombined two less, and the
combined twNomore, fibrous groups. The combined lessfibrous group
contained tumours with slightor little connective tissue stroma
wAhich wrasfibroblastic and more or less evenly distri-buted
throughout the wrhole tumour. Thecombined more fibrous group
containedtumours with moderate or marked centralfibrosis with
hvalinization, and correspondedto the well known scirrhous
tumours.
The lymphoid infiltration (LI) at thecentre as well as at the
periphery of thetumours was also estimated in each individualcase.
In some tumours it w^as moderate ormarked whereas in others it was
slight orabsent. The former two groups were regardedas positive and
the latter two groups asnegative.
RESULTS
The collection comprised 30 tumours ingrade I, 60 tumours in
grade II and 51tumours in grade III. The characteristicsof each
individual tumour can be seen inthe scatter diagrams.
The metastatic ratio of the tumours inthe three grades was
rather similar: 66%in grade I, 63% in grade II and 59% ingrade III.
The overal 5 year and 10 yearsurvival, however, decreased with
increas-ing grade, as can be seen in Table I.The decrease was even
greater in themetastatic cases, as can be seen in TableII. These
figures show that although themetastatic ratio is similar in all
threegrades, prognosis is affected mainly bytumour grade and
particularly whenmetastases are present, the greater en-hancement
being in grade III.
The series contains 53 cases in thenon-scirrhous group and 88 in
the scirr-hous group. It appears from the scatterdiagrams that the
scirrhous tumotirs aremore frequent in grades I and II (70%o
and710% respectively) and less frequent ingrade III (470%). They
are also morefrequent among the metastatic cases (750o)compared
with the non-metastatic cases(41 %)
233
-
0. TH. ANASTASSIADES AND D. M. PRYCE
SCI RRHOUS
0O 1 0 NON SCIRRHOUS
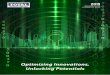
FIG. 1.-Thirty tumours of grade I are distributed according to
their size and according to theirdegree of fibrosis on 2 cm scales.
The tumours above each line are metastatic, and the tuinoursbelow
the lines are non-metastatic.
0.
@0* 1 1 SCIRRHCUS
00 000V0i W 0'n
NON SCIRRHOUS
O&Gf OV i.)0O 0
FIG. 2.-Sixty tumours of grade II are distributed according to
their size and according to theirdegree of fibrosis on 2 cm scales.
The tumours above each line are metastatic and the tumoursbelow the
lines are non-metastatic. Two tumours on the line have only minute
metastases.
0 @*f4 0 0
I f * * * SCIRRHOUSM1 ~o or0~~~~
@ _ 0*:~ NON SCIRRHOUS
ocooVFIG. 3.-Fifty-one tumours of grade III are distributed
according to their size and according to their
degree of fibrosis on 2 cm scales. The tumours above each line
are metastatic and the tumoursbelow the lines are
non-metastatic.
* SUCCUMBED WITHIN 5 YEARS5 YEAR SURVIVORS
o 10 YEARS SURVIVORS0 MODERATE LICr MARKED LI
234
-
FIBROSIS AND ITS IMPORTANCE IN PROGNOSIS
TABLE I.-Metastatic Ratio and Prognostic Outlook of the Whole
Series, andScirrhous and Non-scirrhous Groups
Metastatic ratioGrade I 5 year survival
10 year survivalMetastatic ratio
Grade II 5 year survival10 year survivalMetastatic ratio
Grade III 5 year survival10 year survival
TABLE II. Prognostic Outlook of the Metastatic Cases of the
Whole Series, andScirrhous and Non-scirrhous Groups
Grade I 5 year survival10 year survival
Grade II 5 year survival10 year survival
Grade III 5 year survival10 year survival
In each grade the prognostic outlookwas greatly worsened with
increase offibre content. As can be seen in Table I,the metastatic
ratio was greater, and the5 year and 10 year survival less, in
thescirrhous than in the non-scirrhous group.It is therefore
evident that the metastaticratio and the survival of the patients
varyconsiderably among tumours of the samegrade according to their
degree of fibrosis.
Among the metastatic tumours of thethree grades the prognostic
outlook waseven worse in the scirrhous than in thenon-scirrhous
tumours, as can be seen inTable II. The 5 year survival was less
inthe scirrhous than in the non-scirrhoustumours in all three
grades. The 10 yearsurvival data are not as convincing as faras
grade II is concerned (possibly becauseof the small number of
cases) as all the 6metastatic cases in the non-scirrhousgroup died
within 10 years. However, ingrade I the 10 year survival was much
lessin the scirrhous than in the non-scirrhousgroup and in grade
III there were nosurvivors in the scirrhous group.
Lymphoid infiltration of the tumours(LI) was more frequent in
the moremalignant grades. It was present in 10%
Overall60%35%,31%16%20%13%
Scirrhous53%290o28%18%0%
-Non-scirrhous100%660o50%0%46%30%
in grade I, 26% in grade II and 53%0 ingrade III. It seems
therefore that themore malignant tumours evoke more LI.It was also
more frequent in the non-scirrhous group in all three grades, as
canbe seen in Table III. Although morecommon in the non-scirrhous
tumours, itseems important to note its existence in aconsiderable
proportion of the scirrhoustumours in the two more malignantgrades,
especially in grade III. But as canbe seen in the scatter diagram
for thescirrhous tumours of this grade, LI waspresent predominantly
in moderate degreecompared with the non-scirrhous tumoursof the
same grade, where it was presentpredominantly in marked degree.
TABLE III. Incidence of LI in the WholeSeries, and in Scirrhous
and Non-scirrhous Groups
Overall Scirrhous Non-scirrhouisGrade I 10% 0% 33%Grade II 26%
19% 47%Grade III 53% 42% 63%
The influence of LI on metastases andsurvival of the patients is
particularlyevident in the non-scirrhous tumours of
Overall66%66%46%63%43%30%59%39%31%
Scirrhous80%57%33%74%37%28%70%20%16%
Non-scirrhous33%89%77%35%58%35%48%55%44%
235
-
0. TH. ANASTASSIADES AND D. M. PRYCE
grade III, as can be seen in the scatterdiagram for this grade.
Eleven out of 17(64%) LI positive cases were non metas-tatic. Also,
12 out of 17 (70%0) LI positivecases survived a years and 9 cases
(53%0)survived 10 years. The influence of LI ingrade I cannot be
considered because of thesmall number of LI positive cases. Ingrade
II the results are irregular and noinfluence of LI can be
demonstrated.
DISCUSSION
The close relationship between gradeand prognosis has been
repeatedly reportedby many authors (Black and Speer, 1957;Bloom and
Richardson, 1957; Bloom,1962, 1965, 1971; Cutler et al., 1966;
Wolf,1966; Hamlin, 1968; Tough et al. 1969,Alderson et al., 1971).
Accordingly, thedata from this series of cases show that the5 year
and 10 year survival decreases withincreasing grade.
Although the histological grading oftumours (Bloom and
Richardson, 1957;Black and Speer, 1957) is an artificial
andsubjective procedure, it appears to be ofgreat clinical value
because it roughlyreflects the rate of growth of the
neoplasticcells and consequently the rapidity withwhich the disease
progresses.
Nevertheless, the tumours of the threegrades in our series of
cases exhibitsimilar metastatic ratios (grade I 66%,grade II 63%,
grade III 59%0). Compar-able results have also been reported
byBell, Friedell and Goldenberg (1969).Kreyberg and Christiansen
(1953) have alsopointed out that the metastatic ratio ofgrade I
tumours is as high as that of themore malignant grades. The fact
that, in agiven series of cases, slow growing andrapidly growing
neoplasms exhibit asimilar metastatic ratio, shows that
theestablishment of the regional lymph nodemetastases is a result
of the competitiveinterplay of more than one factor. Amongthese the
chronological age of the tumoursand the reactivity of the host have
beenconsidered of potentially great importancetogether with the
rate of growth of theneoplastic cells.
The rate of growth of the neoplasticcells, differing
considerably among thevarious tumours (Slack et al., 1969;Kusama et
al., 1972), can be roughlyevaluated histologically by the
variousgrading systems, but the chronological ageof any given
tumour cannot be assessedby any of the known procedures. Thedelay
of the patients in seeking treatmenthas been used as indirect
evidence byBloom (1965), who has demonstrated thatit exerts an
influence on survival when thegrade of the tumours is taken into
accountand the delay refers to tumours of similarrate of growth. It
is obvious that whenindolent, slow growing tumours are dis-covered
they should be smaller and presentfor longer time than rapidly
growingaggressive tumours.
In our series of cases, grade I tumoursare as a whole of smaller
size than those ofgrade III tumours, 76% of grade I and53% of grade
III being 3 cm or less at theirgreatest diameter. Grade II is the
mostartificial group of tumours, sharing charac-teristics of both
borderline grades, theproportion of small tumours in thisgrade
being 65%.
The preponderance of small tumours ingrade I (76%) is indicative
of their slowrate of growth compared with the tumoursof the other
grades. But the metastaticratio of these small tumours, in spite
oftheir low malignancy, is very high (60%),probably because of
their long existence.It is even higher than the metastatic ratioof
the most aggressive grade III tumours ofthe same size (510%). It
appears, there-fore, that the age of the tumours interfereswith
aggressiveness, with the result that thethree grades exhibit a
similar metastaticratio. But in spite of the fact that gradeI
tumours are older their overall r5 yearand 10 year survival is
greater than in theother grades (5 year survival 66% com-pared with
43%0 and 39%0 in grades II andIII, and 10 year survival 46%
comparedwith 30 and 31% in grades II and IIIrespectively). This
emphasizes the enor-mous prognostic importance of the degreeof
malignancy of the tumours, which
236
-
FIBROSIS AND ITS IMPORTANCE IN PROGNOSIS
constitutes a dominant feature in breastcancer, predetermining
the rapidity withwhich the evolution of the disease will
takeplace.The time factoor
From the study of our series of cases,we came to the conclusion
that someevidence of tumour age could be suggestedby histological
changes found in thetumours themselves. The various appear-ances in
breast cancer are still described intextbooks of pathology as
immutable andno consideration appears to have beengiven to the
possibility that histologicalchanges occurring with the passage of
timecould be evaluated and used for prognosis.Such changes are
taking place in alltumours and are more or less constant.In some
infiltrating breast cancers theconnective tissue stroma is sparse
andfibroblastic. in others more abundant andin still others there
is an enormousincrease of the connective tissue stromawith distinct
phenomena of maturationand scarring. The increase and sclerosisof
the connective tissue stroma whichhistologically are undoubtedly
ageingprocesses are found as one proceeds fromthe periphery to the
centre of the tumour,going from the more recent to the olderparts
of it. The sclerotic centre varies inextent in the various tumours.
It iswell developed in tumours of low degree ofmalignancy probably
because of their longduration. Although less extensive, it isalso
found in tumours of intermediate andhigh degrees of malignancy,
reflecting theirlonger duration compared with tun4ours ofthe same
degree of malignancy with scantyand fibroblastic stroma.
In our series of cases we found thatthere is a significant
difference in themetastatic ratio and the survival ofthe patients
between the scirrhous andthe non-scirrhous tumours in all
threegrades (Table I).
Although the separation of tumoursaccording to their degree of
fibrosis in twogroups is an artificial division as thedevelopment
of fibrosis is a continuous
process, the greater metastatic ratio of thetumours and the less
survival ofthe patientsof the scirrhous groups compared with
thenon-scirrhous groups in all three grades,reveal the prognostic
significance of thetime factor among tumours of similar rateof
growth. It is also clear that tumours ofthe same grade cannot be
taken as ahomogeneous group because of the widespectrum of ages
among the population ofeach grade. The preponderance of
thescirrhous tumours in grade I (70%0) andthe high (80%)0 indeed
the highest,metastatic ratio of these tumours (al-though they are
slow growing) indicatethat they are the oldest group of tumoursand
that they have the greatest timescale. But the prognostic
significance ofthe time factor, as evidenced by fibrosis,
isgreatest for the most malignant gradeIII tumours although they
have a shortertime scale. The scirrhous tumours of thisgrade have
the least 5 year and 10 yearsurvival (20%0 and 16oo
respectively).
These findings show that the degree ofmalignancy in breast
cancer constituteswhat Bloom (1971) precisely characterizedas the
inherited " tempo " of the diseaseand that the time available, as
indicatedby the degree of fibrosis, permits theinherited
aggressiveness to kill the patientsin an increasing rate with
increasingmalignancy.
The influence of the age, together withthe malignancy of the
tumours, uponsurvival is most in evidence in cases inwhich
metastases have already developedand both factors are decisively
active(Table II). In these cases the survival ofthe patients is
even worse compared withthe whole series. The metastatic gradeIII
tumours with much fibrosis are, aswould be expected, the tumours
with theworst prognosis. All the patients of thisgroup died within
5 years.The host reactivity
There is already a large amount ofevidence of host resistance of
an im-munological nature in breast cancer,including reaction in the
tumours them-
-37
-
238 0. TH. ANASTASSIADES AND D. M. PRYCE
selves and in the regional lymph nodes.The presence of LI in the
primary tumourshas been repeatedly reported as accom-panied by
better prognosis. The relation-ship of this type of host reactivity
to thedegree of malignancy and fibrosis of thetumours requires
further consideration.
The data from our series of cases showthat LI is very common in
breast cancer,particularly in the more malignant gradeswhich may be
more antigenic, as hasalready been pointed out by Bloom et
al.(1970). However, it appears that thisreactivity is more
characteristic of tumourswhich are relatively young and have
lessfibrosis in all three grades (Table III).There is therefore a
decrease in theincidence of LI as fibrosis progresses,which is
accompanied by its gradualdisappearance from the centre of
thetumours. Otherwise the disappearance oflymphocytes and plasma
cells is a normalphenomenon when maturation and sclero-sis of
connective tissue is taking place.
The influence of LI on survival is mostin evidence in the
non-scirrhous tumoursof Grade III, in which it is found in
itshigher incidence and intensity.
With the highly malignant non-scirr-hous tumours of grade III
the results arein agreement with the previous authorswho have shown
that medullary tumourswith LI have a good prognosis in spite
oftheir high intrinsic malignancy.
As can be seen in the scatter diagramfor the non-scirrhous
tumours of grade III,12 out of 17 LI positive cases (70%/)survived
5 years and 9 cases (52%/)survived 10 years. From the 10 LInegative
cases only 3 (300%) survived, thesurvival exceeding 10 years. This
differ-ence in prognosis between the LI positiveand LI negative
non-scirrhous tumours ofgrade III must be due to host
reactivity.But with increasing fibrosis of the tumourshost
reactivity, as expressed by LI,lessens and finally ceases and its
influenceon prognosis is completely lost in thescirrhous grade III
tumours, although LIstill persists in moderate degree in some
ofthese tumours. As can be seen in the
scatter diagram for the scirrhous tumoursof grade III, only one
of the 10 LI positivecases survived.
This probably means that the passageof time gradually
neutralizes the exertedbeneficial effect of host resistance of
thistype. If the non-scirrhous LI positivetumours of grade III were
not excised atthis comparatively early stage of theirevolution they
would become examples ofthe scirrhous group of the same grade
andhave high mortality. Fortunately, how-ever, these tumours in
spite of theirtendency to be large are young, and evenyounger than
the non-scirrhous tumoursof grade II, just as these are younger
thanthe non-scirrhous tumours of grade I.Furthermore, the rapid
increase in size ofthese tumours makes the clinical
diagnosispossible at this earlier stage of theirdevelopment with
the reactivity of thehost to the tumour, as expressed by LI,still
being active.
We are indebted to the PathologyDepartment of St Mary's Hospital
forproviding the material for this study andfor the technical
assistance and to Mr P.Lagogiannis for his help in the
preparationof the diagrams.
REFERENCESALDERSON, M. R., HAMLIN, I. M. E. & STAUNTON,
M. D. (1971) The Relative Significance of Prog-nostic Factors in
Breast Carcinomas. Br. J.Caancer, 25, 646.
ANASTASSIADAS, 0. TH. & PRY(E, D. M. (1966)Immunological
Significance of the MorphologicalChanges in Lymph Nodes Draining
Breast Cancer.Br. J. Cancer, 20, 239.
BELL, J. R., FRIEDELL, G. H. & GOLDENBERG, I. S.(1969)
Prognostic Significance of PathologicalFindings in Human Breast
Carcinoma. SurgeryGynec. Obstet., 129, 258.
BERG, J. W. (1959) Inflammation and Prognosis inBreast Cancer. A
Search for Host Resistance.Cancer, N. Y., 12, 714.
BLACK, M. Al. (1970) Human Breast Carcinoma.Part II. Research
Potential. N.Y. St. J. Med.,15, 962.
BLACK, M. M., SPEER, F. D. & OPLER, S. R. (1956)Structural
Representation of Tumor-Host Rela-tionship in Mammary Carcinoma.
Am. J. clin.Path., 26, 250.
BLACK, M. M. & SPEER, F. D. (1957) NuclearStructure in
Cancer Tissues. Surgery Gynec.Obstet., 105, 97.
-
FIBROSIS AND ITS IMPORTANCE IN PROGNOSIS 239
BLOOM, H. J. G. & RICHARDSON, W. W. (1957)Histological
Grading and Prognosis in BreastCancer. Br. J. Cancer, 11, 359.
BLOOM, H. J. G. (1962) The Roles of HistologicalGrading in the
Study of Breast Cancer. Sym-posium on the Prognosis of the
Malignant Tumoursof the Breast. Ed. P. Denoix and C.
Rouquette.Basel: Karger. p. 51.
BLOOM, H. J. G. (1965) The Influence of Delay onthe Natural
History of Breast Cancer. Br. J.Cancer, 19, 228.
BLOOM, H. J. G., RICHARDSON, W. W. & FIELD, J. R.(1970) Host
Resistance and Survival in Carcinomaof the Breast. A Study of 104
Cases of MedullaryCarcinomas in a Series of 1411 Cases of
BreastCancer Followed for 20 years. Br. med. J., ii,181.
BLOOM, H. J. G. (1971) Impact of Tumor Grade andHost Resistance.
Cancer, N. Y., 28, 1580.
CUTLER, S. J., BLACK, M. M., FRIEDELL, G. H.,VIDORE, R. A. &
GOLDENBERG, I. S. (1966)Prognostic Factors in Cancer of the
FemaleBreast. II Reproducibility of HistologicalClassification.
Cancer., N. Y., 19, 75.
CITTLER, S. J., BLACK, M. M., MORK, T., HARVEI, S.&
FREEDMAN, C. (1969) Further Observations onPrognostic Factors in
Cancer of the FemaleBreast, Cancer, N. Y., 24, 653.
GALLAGER, H. S. & MARTIN, J. E. (1969) EarlyPhases in the
Development of Breast Cancer.Cancer, N. Y., 24, 1170.
HAMLIN, I. M. E. (1968) Possible Host Resistance inCarcinoma of
the Breast. A Histological Study.Br. J. Cancer, 22, 383.
KREYBERG, L. & CHRISTIANSEN, T. (1953) The Prog-nostic
Significance of Small Size in Breast Cancer.Br. J. Cancer, 7,
37.
KuSAMA, S., SPRATT, J. S., DONEGAN, W. L.,WATSON, F. R. &
CUNNINGHAM, C. (1972) TheGross Rates of Growth of Human
MammaryCarcinoma. Cancer, N. Y., 30, 594.
McDIVITT, R., STEWART, F. & BERG, J. W. (1968)Tumors of the
Breast. Atlas ofTumour Pathology.Armed Forces Institute of
Pathology.
MOORE, 0. S. & FOOTE, F. W. (1949) The RelativeFavourable
Prognosis of Medullary Carcinoma ofthe Breast. Cancer, N. Y., 2,
635.
RICHARDSON, W. W. (1956) Medullary Carcinoma ofthe Breast. Br.
J. Cancer, 10, 415.
SLACK, N. H., BLUMENSON, L. E. & BROSS, I. D. J.(1969)
Therapeutic Implication from a Mathe-matical Model Characterizing
the Couirse ofBreast Cancer. Cancer, N. Y., 24, 960.
SMOLAK, K., KOLODZIEJSKA, H. & URBAN, A. (1968)Investigation
on the Relationship Between theClinical Course of Mammary Carcinoma
and theMorphological Features of the Stroma. Pol.med. J., 7, 162.
(Translated from NowotworyXVII, No. 2/1967.)
TOUGH, I. C. K., CARTER, D. C., FRAZER, J. &BRUCE, J. (1969)
Histological Grading of BreastCancer. Br. J. Cancer, 23, 294.
WOLFF, B. (1966) Histological Grading in Carcinomaof the Breast.
Br. J. Cancer, 20, 36.