Embed Size (px)
Citation preview

Bringing the Pieces Together
A case study:Primary Biliary Cirrhosis
(PBC)
Lee HautapuBiochemistry Department, Medlab Central
2009

The patient:
Female
44 years old
Presents early September 2006

The start: Immunology
How are the ANA and TAAT performed?
ANA results.
TAAT results.

Indirect Fluorescent Assay (IFA)
Screen done first and if positive titres are then performed. A fluorescent antibody is used as a marker for a antigen-antibody binding reaction.This occurs on a substrate surface.The substrate is normally either a mono-layer of cells grown on a slide or tissue fixed to a microscope slide.

IFA- How the test is performed
ANA: screen 1:80, if positive titre 160 – 320 – 640 TAAT: screen 1:40, if positive titre 80 - 160 Auto-antibodies bind to antigens in/on the substrate. Wash the slide to remove all excess serum.Fluorescein conjugated antiserum (FITC) is added to the substrate.The FITC binds to the bound auto-antibodies.
Wash the slide to remove the excess conjugate.

IFA- Indirect Fluorescent Assay
The slide is cover-slipped.
The slide is viewed using a fluorescent microscope.
Observation of specific fluorescent pattern/s on the
substrate indicates the presence of the auto-
antibodies in the test specimen.
Further testing if required: TAAT, ENA, DNA
Patients Immunology Results
ANA: Screen 1:80Titre: 160/320/640
TAAT: Screen 1:40Titre: 80/160
Positive1:640 titrePattern – Few nuclear dots Cytoplasmic Staining- Suggestive of aMitochondrial patternPositive1:80 titrePattern - Mitochondrial

ANA: A Few Nuclear Dots
This pattern is found in patients with Autoimmune and Viral liver diseases (eg Primary Biliary Cirrhosis, Chronic active hepatitis).
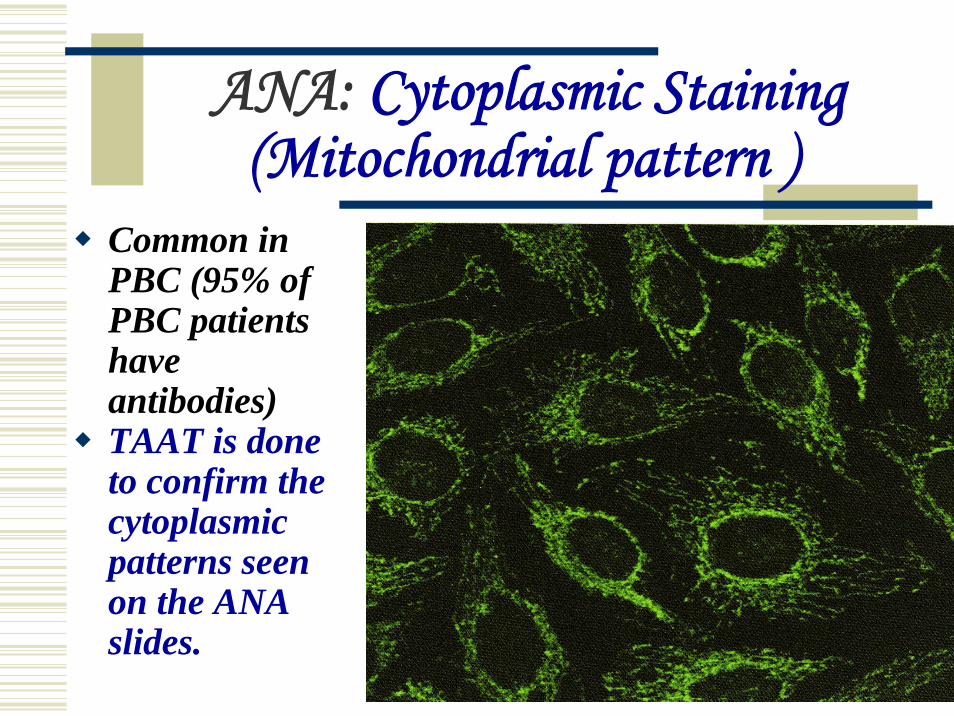
ANA: Cytoplasmic Staining (Mitochondrial pattern )
Common in PBC (95% of PBC patients have antibodies) TAAT is done to confirm the cytoplasmic patterns seen on the ANA slides.
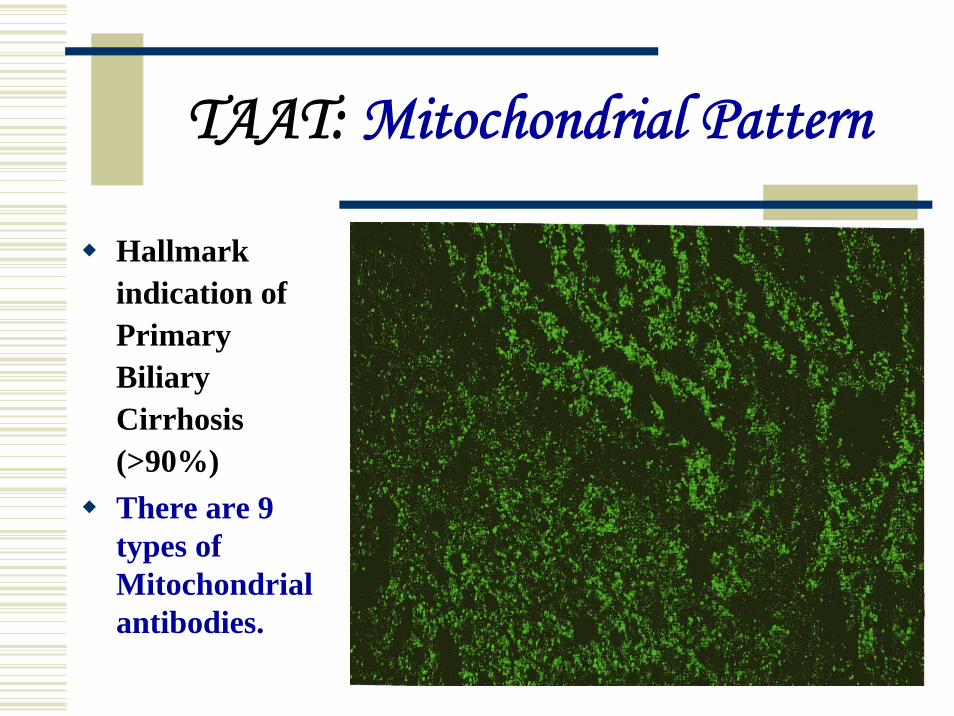
TAAT: Mitochondrial Pattern
Hallmark indication of Primary Biliary Cirrhosis (>90%)There are 9 types of Mitochondrial antibodies.

What does it all mean?
ANA
Autoimmune liver
disease - PBC
Viral liver disease -
Hepatitis
TAAT
Autoimmune disease -Primary Biliary CirrhosisOccasionally CREST syndrome and other autoimmune diseases

The patient: Presented in early September 2006
Clinical details:
General fatigue
Legs itchy
Jaundice
Hepatitis?
History of arthritis
Tests requested:
CBCB12 & FolateLFTFasting LipidsImmunoglobulinsHepatitis B & A & CCMV EBV ANATAAT
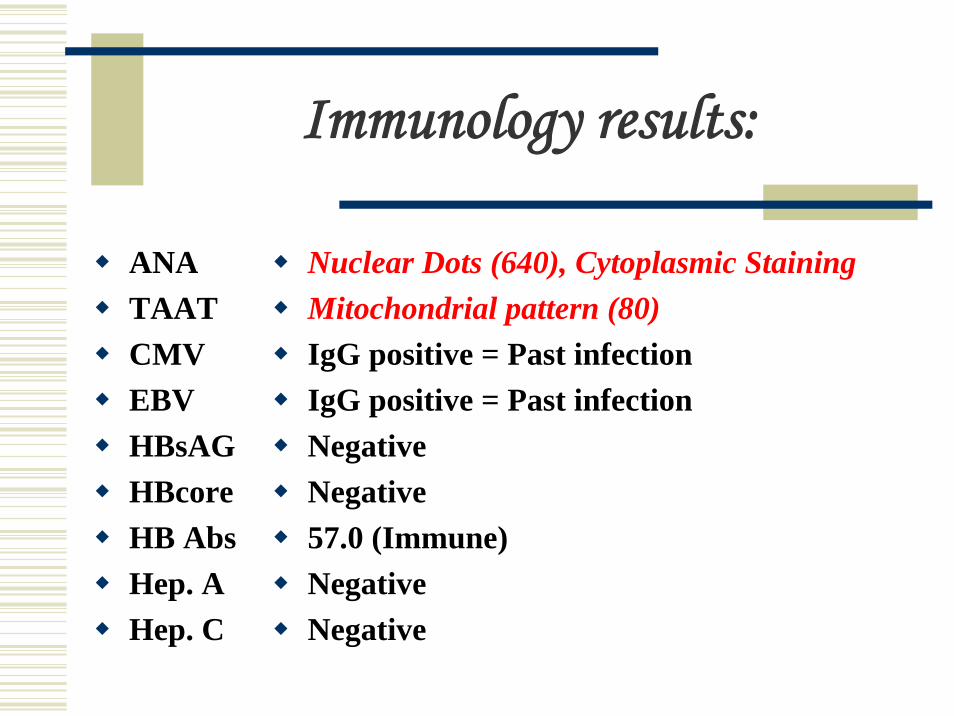
Immunology results:
ANATAATCMVEBVHBsAGHBcoreHB AbsHep. AHep. C
Nuclear Dots (640), Cytoplasmic StainingMitochondrial pattern (80) IgG positive = Past infection IgG positive = Past infectionNegativeNegative57.0 (Immune) NegativeNegative

Haematology results: CBC
RBC = 3.8* (3.9-5.5) Hb = 130 (115- 155) PCV = 0.38 (0.36-0.47) MCV = 108* (80-100) MCH = 30 (27-32) MCHC = 342 (315-355) RDW = 14.6* (11.5-14.5) Film comment: MACRO++ RBC morphology not diagnostic but possible causes include B12/Folate deficiency, liver disease, hypothyroidism, renal disease or malignancy.
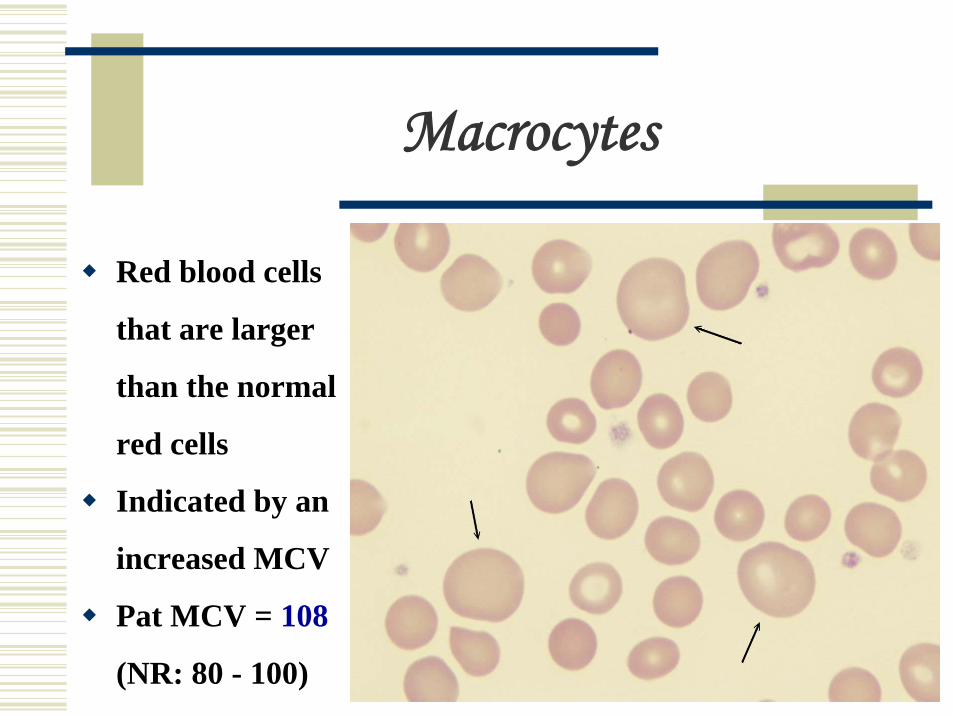
Macrocytes
Red blood cells
that are larger
than the normal
red cells
Indicated by an
increased MCV
Pat MCV = 108
(NR: 80 - 100)
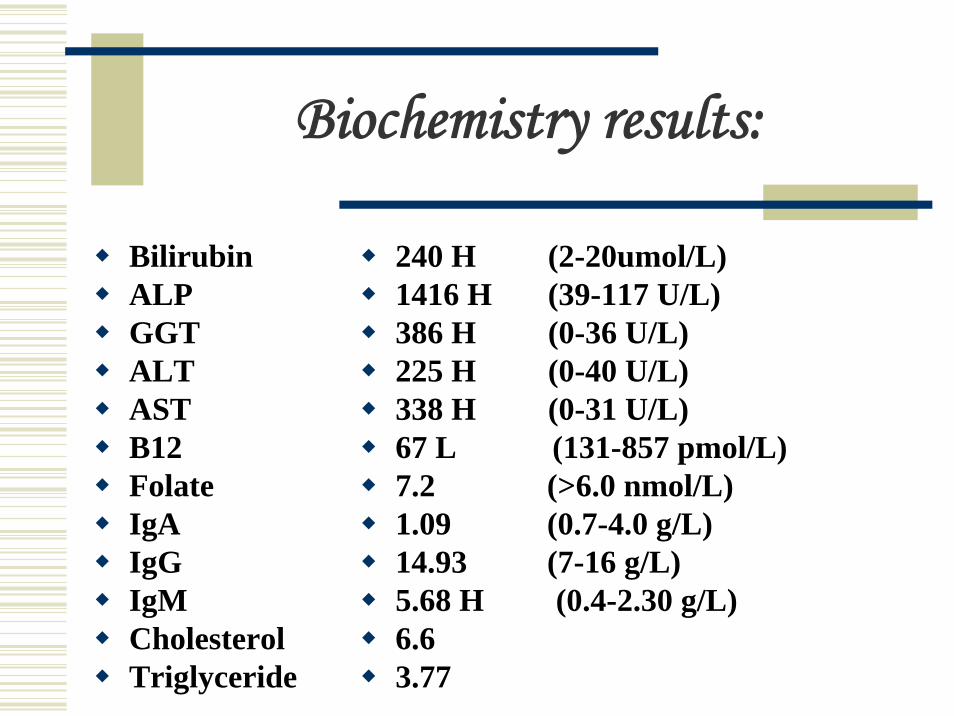
Biochemistry results:
Bilirubin ALPGGTALTASTB12FolateIgAIgGIgMCholesterolTriglyceride
240 H (2-20umol/L) 1416 H (39-117 U/L) 386 H (0-36 U/L) 225 H (0-40 U/L) 338 H (0-31 U/L) 67 L (131-857 pmol/L) 7.2 (>6.0 nmol/L) 1.09 (0.7-4.0 g/L) 14.93 (7-16 g/L) 5.68 H (0.4-2.30 g/L) 6.6 3.77
How does it all tie in?
ANA/TAAT - Strong indication of Primary Biliary Cirrhosis – are the liver function tests abnormal?Liver function – Abnormal(Bio & Immuno)Macrocytosis - Due to a B12 deficiency or liver disease – what are the B12 levels (Bio & Haem)B12 deficiency - Due to liver disease(Bio & Haem & Immuno)
Patient presented : late Sept. 06, April 2007, June 2007
Clinical details
General fatigueJaundicePalpable liverUnusual spots around eyesMonitor Primary Biliary Cirrhosis (June)
Tests requested
CBCB12 & FolateLFTANATAAT

Immunology results: Sept 06, May 07, June 07
TAAT
ANA
Positive - Mitochondrial
Titre >160 (prev. 1:80)
Positive – Few Nuclear Dots
Cytoplasmic Staining
Titre >640 (prev. 1:640)
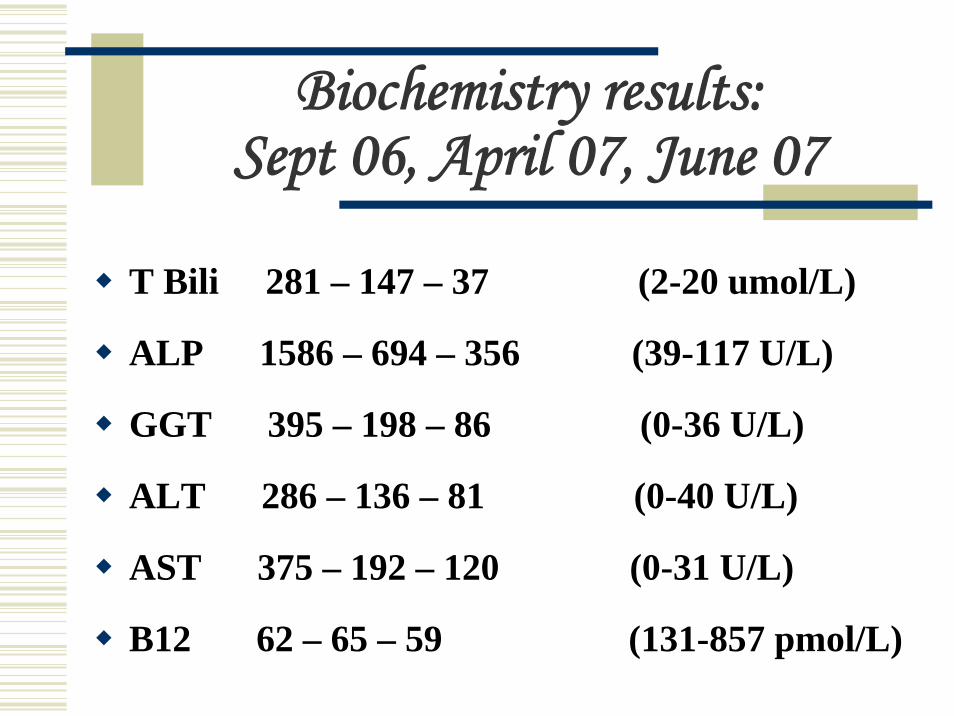
Biochemistry results: Sept 06, April 07, June 07
T Bili 281 – 147 – 37 (2-20 umol/L)
ALP 1586 – 694 – 356 (39-117 U/L)
GGT 395 – 198 – 86 (0-36 U/L)
ALT 286 – 136 – 81 (0-40 U/L)
AST 375 – 192 – 120 (0-31 U/L)
B12 62 – 65 – 59 (131-857 pmol/L)
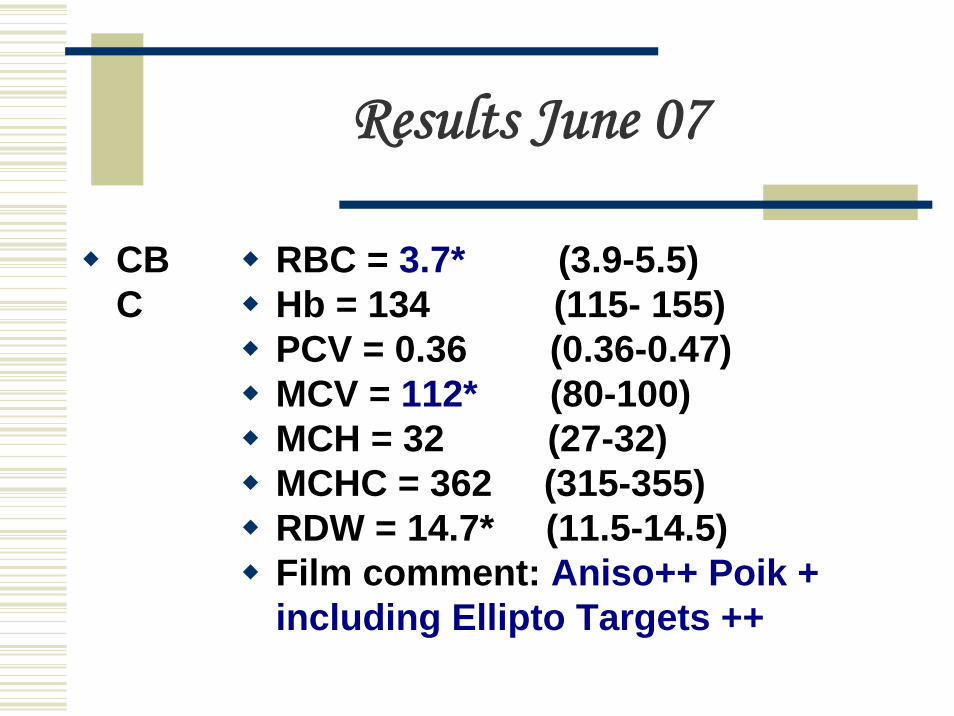
Results June 07
CBC
RBC = 3.7* (3.9-5.5)Hb = 134 (115- 155)PCV = 0.36 (0.36-0.47)MCV = 112* (80-100)MCH = 32 (27-32)MCHC = 362 (315-355)RDW = 14.7* (11.5-14.5)Film comment: Aniso++ Poik + including Ellipto Targets ++
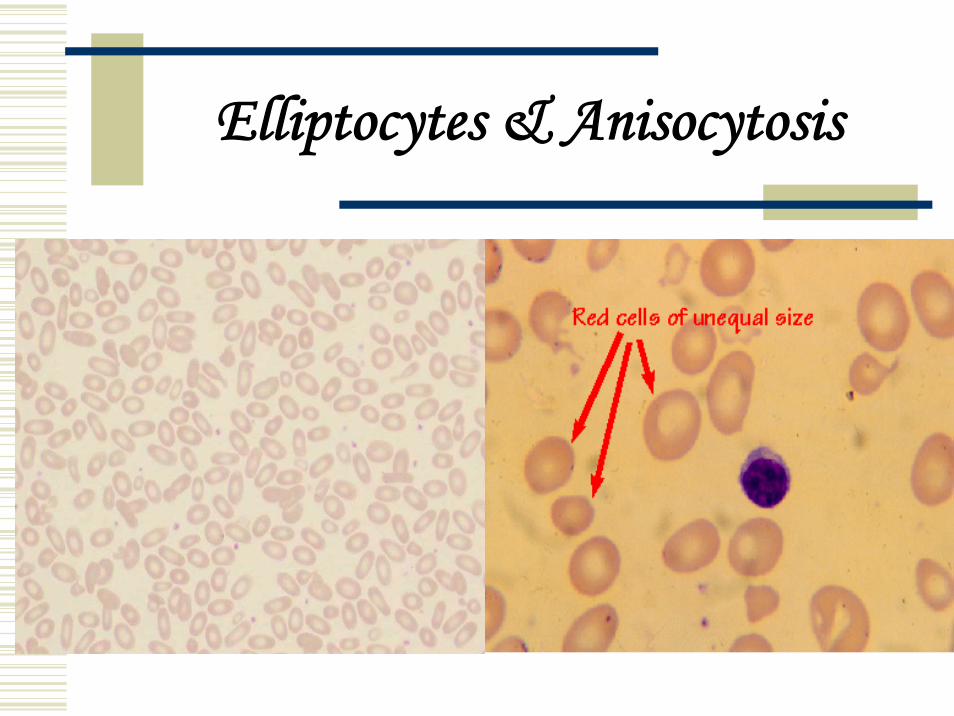
Elliptocytes & Anisocytosis
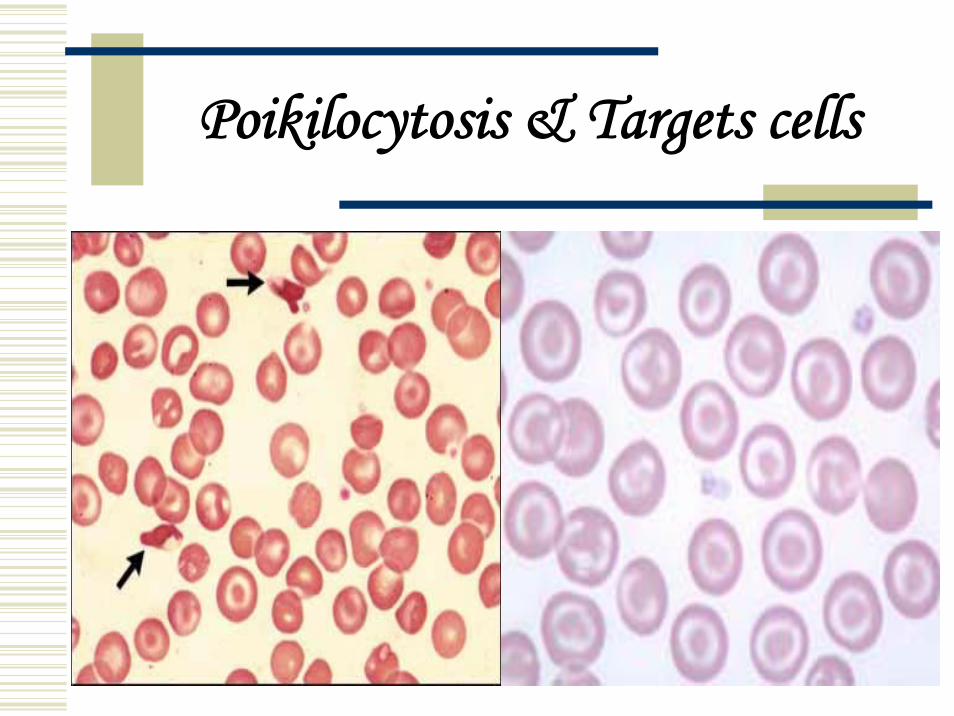
Poikilocytosis & Targets cells

The diagnosis: PBC
The patient had been referred to a specialist.The patient had a Liver Biopsy performed.The diagnosis was confirmed as being Primary Biliary Cirrhosis: Stage Two. Patient also currently has Xanthoma present around both eyes.Treatment:Cholestyramine Ursodeoxycholic Acid Non-steroid anti-inflammatory

Xanthoma
Characterised by the presence of plaques of a yellow colour in the skin, due to deposits of lipidsXanthelasma palpebrarum

PBC: what is it?
PBC is an chronic auto-immune disease.PBC has 4 stages:
Inflammation (Portal)Scarring (Periportal)Fibrosis (Septal)Cirrhosis.
Marked by the progressive destruction of small bile ducts.
PBC: what is it? (continued)
This disease presently has no known cure.
Occurs between 40 – 60 years of age.
Female to male ratio = 9:1
1:4000 people will have this disease.
PBC can lead to a host of other health problems.
Treatment:
Currently there is NO cure.
Current medications can only be used
to SLOW the progression of the
disease.

Some symptoms:
Fatigue 65%
Itchy skin 55%
Jaundice 35%
Right upper quadrant pain 17 - 25%
Extra-hepatic autoimmune disorder 50 – 70%
Xanthoma 10%
Definitive diagnosis:
A patient who shows all three of the following is diagnosed as having PBC:
Cholestatic liver tests (ALP/GGT elevated more than ALT/AST)TAAT: Mitochondrial = positive.With a titre equal or greater than 1:40Diagnostic or compatible liver biopsy

Some complications:
Osteoporosis (440%)
Portal hypertension
Esophageal varices and gastropathy
Splenomegaly (15%)
Edema and ascites
Maldigestion and malabsorption
Bruising and bleeding disorders
Cause of Primary Biliary Cirrhosis:
The true cause is unknown.
It is called an autoimmune disorder because of the
presence of auto-antibodies (ANA,TAAT).
Most patients have anti-mitochondrial antibodies
(M2)

The End
Thank you to staff from the: Haematology Department
Immunology DepartmentBiochemistry Department
Thank you to the audience for your time and attention.
Q&A time













![General Intelligence through playing games? · define powerful universal learning agents that have provabl yoptimalperformance[Hut05]. Bringing all these pieces together, we can](https://img.pdfslide.us/doc/110x75/5f1b75c2834882611401a39e/general-intelligence-through-playing-games-deine-powerful-universal-learning.jpg)