Embed Size (px)
DESCRIPTION
Bringing Evidence to the Bedside in Critical Care. Allan S. Detsky Physician-in-Chief Mount Sinai Hospital. We need information. If asked: We need it twice a week We get it from textbooks, journals and our colleagues. We really need information. If shadowed: - PowerPoint PPT Presentation
Citation preview
Bringing Evidence to the Bedside in Critical Care
Allan S. Detsky
Physician-in-Chief
Mount Sinai Hospital
We need information
If asked:
• We need it twice a week
• We get it from textbooks, journals and our colleagues
We really need informationIf shadowed:
• We need it twice for every 3 outpatients and 5 times for every patient
• But we rarely get what we need from the resources that we use– Colleagues– Textbooks– Journals
Ann Intern Med 1991;114:576-81
Evidence of Care Gaps
• Beta blockers in post MI patients
• Statins in post MI patients
• ACE-I in patients with CHF
• Antithrombotic therapy in patients with nonvalvular atrial fibrillation
HOW CAN WE BRIDGE THIS GAP?
Bringing evidence to the point of care• Need it within seconds if it is to be incorporated into
busy clinical rounds• Focus on users’ needs and important clinical outcomes• Our initial attempts to bring the best evidence to a busy
clinical team caring for over 200 patients per month
JAMA 1998;280:1336-8.
Kinds of Questions
1. Therapeutic Effectiveness
2. Diagnostic Accuracy
3. Prognostic Information
Therapeutic Effectiveness
For patients with health state X,
does Rx A do more good than
harm (compared to Rx B)?
Diagnostic Accuracy
Does test A help us separate those with disease from those without for patients that look like X?
Prognostic Information
For patients with health state X, was the risk of an adverse outcome over a specified period of time?
What do clinicians want on PDAs?
• Clinical bottom line from preappraised resources
• Management algorithms
• Drug dosages and interactions
• Numerical summaries of risks and benefits
• They don’t want traditional clinical practice
guidelines
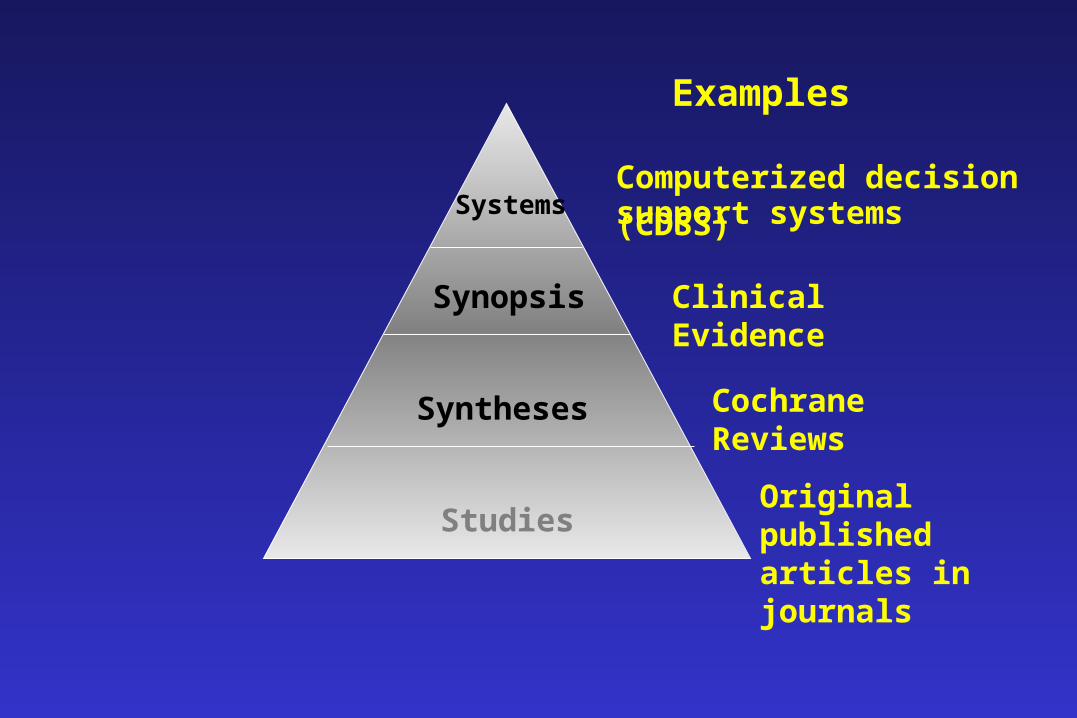
Examples
Computerized decisionsupport systems (CDSS)Systems
Synopsis
Syntheses
Studies
Clinical Evidence
Cochrane Reviews
Original published articles in journals
Internet Available Resources
www.cebm.utoronto.ca
www.eboncall.co.uk
How To design 1. Learn how to recognize questions.
2. Learn how to quantify answers.
Therapeutic Effectiveness
Pc = event rate in control group
Pt = event rate in experimental group
Pc - Pt = ARD
(Pc - Pt)/Pc = PRD
Pt/Pc = RR
1 = NNT
Pc - Pt
10% - 5% = 5% = ARD
(10% - 5%)/10% = 50% = RRD
5%/10% = .5 = RR
1
10% - 5% = 20 = NNT
DIAGNOSTIC TESTS
• Sensitivity
• Specificity
• Likelihood ratios
LR > 1
LR = 1
LR < 1
Read and appraise individual
studies, systematic reviews
Then go to websites to see how
results are presented.
Next - start a simple research
project.
Medical Consults
What is the validity of a
cardiac risk index in
our patients?
• Start slowly
• Progress will take time
• It’s harder than you think





























